
Abstract
Background:
Macro-thyrotropin (macro-TSH) is a large molecular weight TSH that causes elevated serum TSH concentrations due to its slow clearance. It is primarily a complex of TSH and anti-TSH autoantibodies. The aims of this study were to examine the prevalence and nature of macro-TSH in neonates and to determine how to cope with macro-TSH in neonates suspected to have congenital hypothyroidism through neonatal mass screening.
Methods:
The presence of macro-TSH was examined using polyethylene glycol (PEG), gel filtration chromatography (GFC), and 125I-TSH binding studies in 939 umbilical cord blood samples from neonates and their mothers.
Results:
Among 138 serum samples with a PEG precipitation ratio of TSH >68.9% (mean + standard deviation), human anti-mouse antibodies were found in nine samples. The presence of macro-TSH was examined in the remaining 129 serum samples using a 125I-TSH binding study and GFC. The 125I-TSH binding study revealed that four babies (0.43%) had significantly high ratios of 125I-TSH binding to their sera. Two of the babies were siblings, and their mother and the other two mothers also showed significantly high binding ratios. The 125I-TSH binding was displaced by a large amount (1 μg) of unlabeled human TSH in a similar way between babies and their mothers in all cases, suggesting the presence of anti-TSH autoantibodies in their sera. Further characterization of the autoantibodies in one baby and its mother showed a low affinity and high specificity to human TSH, and the nature was very similar between them. These findings may indicate that the anti-TSH autoantibodies that developed in the mother were transferred to the baby through the placenta and formed macro-TSH by binding to neonatal TSH. GFC revealed macro-TSH in only one baby and its mother, probably because of the dissociation of TSH from autoantibodies during the analytical procedure.
Conclusions:
Macro-TSH was found in 0.43% of neonates, and their mothers all had macro-TSH as well. We recommend that if a baby's serum TSH concentration is high enough to consider levothyroxine treatment suspecting congenital hypothyroidism but the free thyroxine level is normal, their mother's macro-TSH should be checked.
Introduction
Congenital hypothyroidism causes severe physical and mental retardation and can be generated by endemic, genetic, or sporadic causes. 1 The incidence is between 1 in 3000 and 1 in 2000 neonates and it is one of the congenital diseases that are screened for in newborn mass-screening schemes. Congenital hypothyroidism is suspected if thyrotropin (TSH) concentrations in the heel pad blood of neonates are abnormally high and is confirmed by low serum free thyroxine (fT4) and high serum TSH concentrations. Thyroid hormone replacement therapy is initiated upon diagnosis.
Macro-TSH has a molecular mass >150 kDa, and several case reports have been published. 2 –5 The prevalence was reportedly 0.6% in 495 patients having TSH >10 mU/L, 6 0.79% in 1901 patients with subclinical hypothyroidism, 7 and 3.1% in 97 patients with thyroid tumor. 8 Patients with macro-TSH have elevated serum TSH concentrations because of slower clearance from circulation. 9 Serum thyroid hormone levels are normal, mimicking subclinical hypothyroidism in terms of laboratory data. 10 However, thyroid hormone replacement therapy is unnecessary in patients with macro-TSH because the bioactivity of macro-TSH is low and thyroid function is normal. 2,11 If macro-TSH exists in neonates and those with macro-TSH are misdiagnosed as having congenital hypothyroidism, unnecessary replacement therapy may be administered over a long period. Macro-TSH is primarily a complex comprising TSH and anti-TSH autoantibodies. However, it may be a heterogeneous entity, and a congenital origin may coexist. A comparison of the prevalence and nature of macro-TSH in babies and their mothers might provide useful information about its origin.
This study aimed to examine the prevalence and nature of macro-TSH in neonates and to determine how to cope with macro-TSH in neonates who are suspected to have congenital hypothyroidism during mass screening.
Materials and Methods
Subjects
Umbilical cord blood samples were collected from 939 babies born at the Hamada Obstetrics and Gynecology Hospital from January 2019 to December 2021. Blood was also collected from the babies' mothers at the time of their birth. The average age of the mothers at delivery was 34.0 ± 4.1 years. Thirty-six mothers delivered babies twice during the study period.
TSH assays
The concentration of TSH was measured with an enzyme immunoassay that was established in our laboratory. 11 A human TSH-β monoclonal antibody (10-T25C; Fitzgerald Industries International, Acton, MA) was used as the capture antibody, and a human TSH-β monoclonal antibody (10-T25B; Fitzgerald) was used as the detection antibody. The reference preparation (hTSH-RP-2) was highly purified human TSH (AFP3959A) from the human pituitary (National Hormone and Peptide Program [NHPP], Harbor-UCLA Medical Center, Torrance, CA). The analytic limit of detection was 0.0075 mIU/L (conversion factor from ng/mL to mIU/L was 7.54).
Based on a serum sample with a total TSH concentration of 4.5 mIU/L, the intra- and inter-assay coefficients of variation were 3.5% and 5.2%, respectively. The reference ranges (95% confidential interval) of TSH in the cord blood of neonates and their mothers were 2.16–23.88 and 0.87–4.36 mU/L, respectively. Log-transformed data were used to determine the mean ± 1.96 standard deviation (SD) and converted back to the ordinary number. The highest TSH data in neonates were judged to be an outliner using Smirnov-Grubbs test and excluded to determine the reference range. The reference range of fT4 was 0.89–1.76 ng/dL according to the instruction of ADVIA Centaur Chemiluminescent Kit (Siemens, Munich, Germany).
Polyethylene glycol precipitation
Polyethylene glycol (PEG) was used to precipitate γ-globulin associated with TSH as previously reported. 11 In brief, 50 μL serum samples were treated with either 50 μL of 25% PEG (the final concentration of PEG was 12.5%) to precipitate γ-globulin fractions leaving the non-PEG-precipitable TSH in the supernatant or with 50 μL of water instead as a control (serum TSH). The percentage of PEG-precipitable TSH, which may be increased in sera containing macro-TSH, was calculated as follows: (serum TSH – non-PEG-precipitable TSH)/serum TSH × 100.
Gel filtration chromatography
Gel filtration chromatography (GFC) was performed with a 1 × 20 cm mini-column of Ultrogel AcA 44 (IBF, La Garenne, France) that was equilibrated with 0.01 mol/L sodium phosphate buffer (pH 7.0) containing 0.1 mol/L NaCl, 0.1% (w/v) bovine serum albumin, and 0.05% (w/v) NaN3. Serum samples (50–500 μL) were applied to the column, and 1-mL fractions were collected for TSH measurements. Serum samples suspected to contain macro-TSH were analyzed using a longer column (1 × 65 cm). The column was calibrated using various molecular weight markers (Sigma-Aldrich).
Human anti-mouse antibodies
Human anti-mouse antibodies (HAMAs) can produce spuriously high TSH values in sandwich-type immunoassay systems employing two mouse monoclonal antibodies, 12,13 because HAMAs bridge the capture antibody and detection antibody in the absence of TSH. Three HAMA blockers were used to counteract the effects of HAMAs: mouse whole serum (MP Biomedicals, Santa Ana, CA), mouse IgG (THBR1), and mouse IgM (THBR2; the latter two were from Cosmobio Co., Tokyo, Japan). The ratio of TSH in the presence of HAMA blockers to that in the absence of HAMA blockers in 138 cord serum samples with a PEG precipitation ratio of TSH >68.9% (mean + SD) was 101.5 ± 6.9%. HAMAs were suspected when the ratio was <87.7% (mean – 2 SDs).
125I-hTSH binding study
125I-hTSH binding study was performed as previously described. 14 Highly purified human TSH (hTSH; National Institute of Diabetes and Digestive and Kidney Diseases [NIDDK] hTSH-SIAFPI-8, AFP-3959A), rat TSH (rTSH, NIDDK rTSH-I-9, AFP-11542B), human luteinizing hormone (hLH, NHPP hLH, AFP6780C), human follicle-stimulating hormone (hFSH, NHPP hFSH, AFP7298A), human chorionic gonadotropin-α (hCG-α, NHPP hCG-α, AFP8492A), and hCG-β (NHPP hCG-β, AFP8494A) were provided by Dr. A. F. Parlow. To determine the binding characteristics of anti-TSH autoantibodies, binding data using various amounts of unlabeled hTSH were analyzed by nonlinear regression using GraphPad Prism version 9 (GraphPad Software Inc., La Jolla, CA).
Statistical analyses
All measurements are expressed as means ± SDs. Values ±2 SDs away from the mean were considered significantly different. Statistical analyses were performed using GraphPad Prism version 9. Wilcoxon rank-sum test was used to compare TSH concentrations between neonates and their mothers. Student's t test was used to compare 125I-TSH binding to the sera between neonates and their mothers. Nonlinear regression (one-site) model was applied to the displacement curve of 125I-hTSH by various amounts of unlabeled hTSH.
This study was approved by the Clinical Research Review Board of the Hamada Obstetrics and Gynecology Hospital (HMH 2018-01). Informed consent was obtained from all participants. This research was completed in accordance with the Declaration of Helsinki. All relevant data are within the article, and this is a cross-sectional observational study.
Results
Concentrations and PEG precipitation ratios of TSH in umbilical cord serum
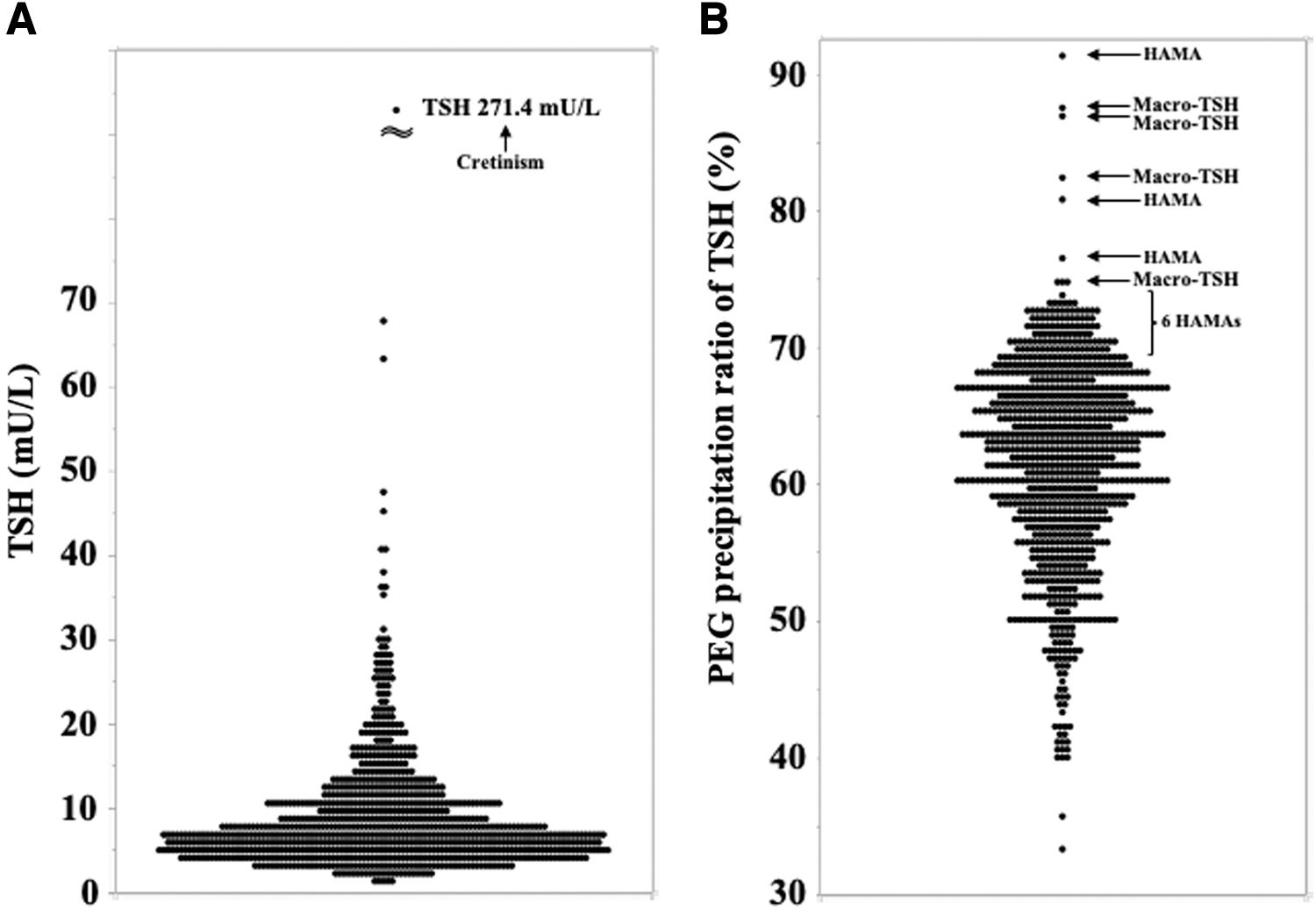
Figure 1 A shows the serum TSH concentrations in umbilical cord blood samples from 939 neonates. TSH concentration ranged from 0.9 to 271.4 mU/L, and the median value was 6.9 mU/L, which was significantly (p < 0.0001) higher than that in their mothers (median 1.9 mU/L, range 0.6–11.3 mU/L). A baby whose cord serum TSH concentration was 271.4 mU/L had been diagnosed with congenital hypothyroidism by newborn mass screening for congenital metabolic disorders and was already receiving thyroid hormone replacement therapy at the time this result was obtained.
Concentrations and PEG precipitation ratios of TSH in umbilical cord serum.
Figure 1B shows the PEG precipitation ratios of TSH in umbilical cord serum from 939 neonates. It ranged from 33.3% to 91.3% (mean ± SD: 61.5 ± 7.4%). HAMAs interfere with the assay platform and produce a spuriously high PEG-precipitation ratio. Therefore, HAMAs were examined in 138 serum samples with a PEG precipitation ratio of TSH >68.9% (mean + SD). The ratio of TSH in the presence of HAMA blockers to that in the absence of HAMA blockers in 138 cord serum samples was 101.5 ± 6.9%. If HAMAs are present, TSH concentrations in the samples that are added HAMA blockers decrease. Nine serum samples had a ratio of <87.7% (mean – 2 SDs) and were judged as having HAMAs.
125I-TSH binding studies in sera from neonates and their mothers
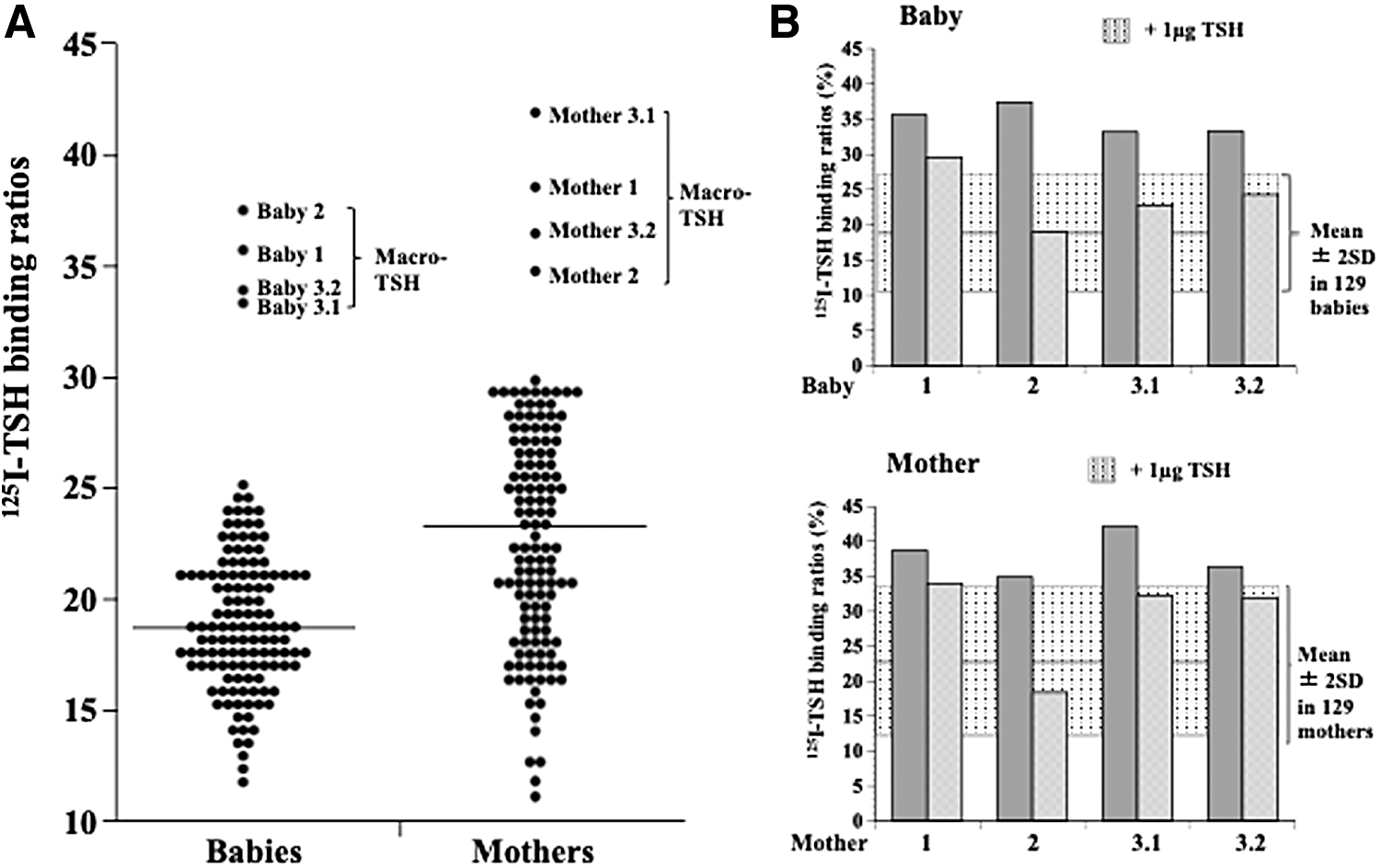
It is highly possible that macro-TSH is present in sera with a high PEG precipitation ratio of TSH. A 125I-TSH binding study was conducted in all 129 HAMA-negative serum samples with a PEG precipitation ratio of >68.9% (mean + SD) of babies and their mothers (Fig. 2A). The nonspecific binding of 125I-TSH in babies (19.0 ± 4.1%) was significantly lower (p < 0.0001) than that in their mothers (22.9 ± 5.4%). Four babies showed significantly high 125I-TSH binding ratios, and their mothers' blood samples also showed significantly high 125I-TSH binding ratios. Two babies (baby 3.1 and baby 3.2) were found to be siblings born to mother 3, and the deliveries were 22 months apart (mother 3.1 and mother 3.2 serum samples).
125I-TSH binding studies in sera from neonates and their mothers.
To examine whether the binding was specific to TSH, a large amount of unlabeled human TSH (1 μg) was added to the reaction mixture in the binding study. The 125I-TSH binding ratios were lowered to the normal range in babies 2, 3.1, and 3.2 and their mothers and were slightly lowered in baby 1 and its mother by excess unlabeled human TSH, suggesting that anti-TSH autoantibodies were responsible for the binding (Fig. 2B).
Table 1 shows laboratory data for the four babies and their mothers having macro-TSH. These four neonates did not show any clinical characteristics at all, and the TSH concentrations were within the reference range of the cord blood of neonates.
Laboratory Data for the Included Babies and Their Mothers
The reference range of fT4 was 0.89–1.76 ng/dL.
The reference ranges of TSH in the cord blood of neonates and their mothers were 2.16–23.88 mU/L and 0.87–4.36 mU/L, respectively.
Free TSH: TSH concentrations in the supernatant after the treatment of sera with 12.5% PEG.
PEG: The TSH precipitation ratios by PEG were calculated as (TSH concentrations – free TSH concentrations)/TSH concentrations × 100 (%).
I-TSH binding: The 125I-TSH binding ratios were calculated as the radioactivity (cpm) in the PEG precipitate/the total radioactivity (cpm) × 100 (%).
HAMA: TSH concentration in the presence of HAMA blockers/TSH concentration in the absence of HAMA blockers × 100 (%). A percentage <87.7% (mean – 2 SD) indicates that the serum contained HAMA.
>Mean +2 SD.
Mean ± SD.
cpm, count per minute; fT4, free thyroxine; HAMA, human anti-mouse antibody; ND, not determined due to the lack of serum sample; PEG, polyethylene glycol; SD, standard deviation; TSH, thyrotropin.
125I-TSH binding characteristics in a neonate and its mother
We further characterized the anti-TSH autoantibodies in baby 2 and its mother (mother 2), whose displacement rate of binding by excess unlabeled TSH was the largest (Fig. 3). Excess unlabeled human TSH almost completely displaced its specific binding in baby 2 and its mother 2. Excess unlabeled rat TSH partially displaced the binding, whereas human luteinizing hormone (LH), follicle-stimulating hormone (FSH), hCGβ, and hCGα did not displace the binding, suggesting that the autoantibodies were directed to the TSH-β subunit, mainly the human TSH-β subunit. The one-site competition model revealed the low-affinity nature of anti-TSH autoantibodies (Kd = 10−6.26 M and 10−6.00 M in baby 2 and mother 2, respectively).

125I-TSH binding characteristics in a neonate and its mother.
Gel filtration chromatography
GFC did not reveal macro-TSH in the babies and their mothers, except for in baby 1 and its mother (mother 1) (Fig. 4). There was a large molecular-sized TSH in addition to the 23 kDa TSH, but the separation of the peaks was very poor, suggesting that macro-TSH might have been dissociated during GFC.

GFC of TSH. GFC of TSH in umbilical cord serum in baby 1 and mother 1. There was a large molecular-sized TSH in addition to the 23 kDa TSH, but the separation of the peaks was very poor. GFC, gel filtration chromatography.
Discussion
We demonstrated that the prevalence of macro-TSH in neonates was 0.43% and that all mothers whose babies had macro-TSH had macro-TSH as well. The results are summarized in Figure 5. The pathogenesis of macro-TSH in neonates is likely to be a complex of neonatal TSH with anti-TSH autoantibodies that are transferred from the mothers to their babies through the placenta.
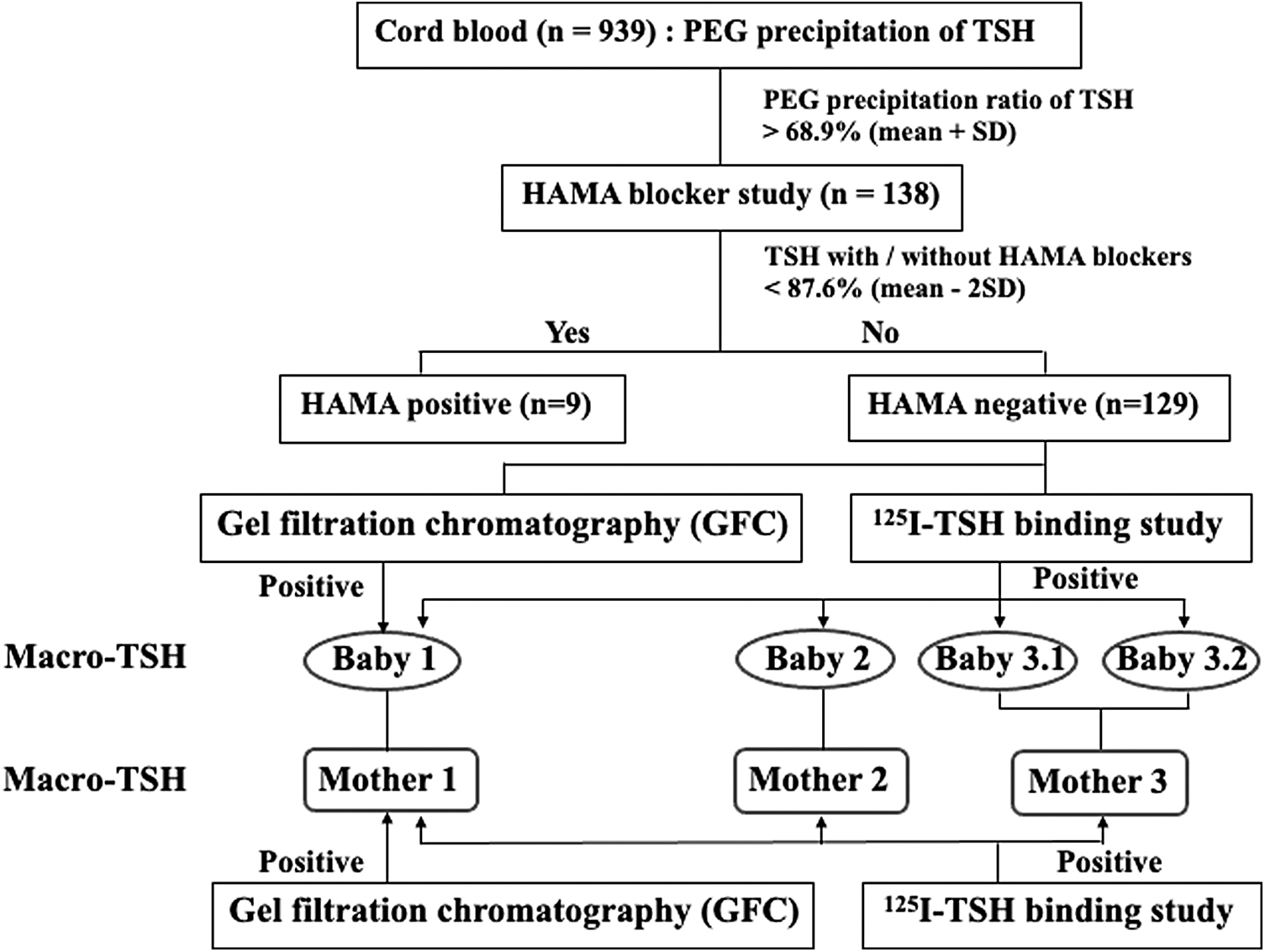
Summary of the results of this study. Four babies (0.43%; 4/939) were diagnosed with macro-TSH based on the results of the 125I-TSH binding study, but macro-TSH was only proven in one of the four babies by GFC. Two of the four neonates were born to the same mother. The three mothers of these four babies with macro-TSH also had macro-TSH with characteristics similar to those of their babies.
Several case reports have described the presence of macro-TSH in neonates. Halsall et al 15 reported a patient with a blood spot TSH level of 213 mIU/L. The neonate was euthyroid, and the mother showed increased serum TSH and normal fT4 concentrations. The authors demonstrated macro-TSH using PEG precipitation and GFC. Rix et al 16 reported a newborn whose blood spots showed an elevated TSH concentration (103 mIU/L), but normal thyroxine (T4) and triiodothyronine (T3) levels. The mother also had elevated serum TSH concentrations, with normal T4 and T3 levels. They demonstrated macro-TSH in both the newborn and the mother using PEG precipitation and GFC. The baby's TSH decreased to a normal level within 8 months in accordance with a normal rate of elimination of maternal IgG, while the TSH level in the mother remained high. Donadio-Andrei et al 17 reported a woman with high serum TSH concentrations that were highly variable on different assay platforms. She had a daughter with an elevated TSH concentration (222 mIU/L) on a dried blood spot. Levothyroxine treatment resulted in hyperthyroidism in the infancy. Her second child also presented with an elevated TSH concentration (296 mIU/L) and normal fT4 levels. Macro-TSH was demonstrated in the mother and her two babies using GFC. Serum TSH levels in the two babies returned to normal within seven months, while those in the mother remained high.
In the present study, we assayed macro-TSH in a large population of newborns. As blood sampling from a newborn is difficult, we used umbilical cord blood sampling instead. Cord blood TSH assessment is a useful screening method for congenital hypothyroidism and is used in some countries but has high false-positive rates. 18,19 Perinatal stress may be involved in higher TSH concentrations in cord blood.
In this study, we confirmed that serum TSH concentrations in umbilical cord blood samples of neonates were significantly higher than those of their mothers. Four of the 939 neonates had macro-TSH (0.43%) based on the 125I-TSH binding study, and all their mothers had macro-TSH as well. In other words, there were no macro-TSH cases in which the mother did not have macro-TSH. Two of the four neonates were siblings born to the same mother. These findings strongly suggest that macro-TSH is not of congenital origin but of maternal one.
In physiology, is the transplacental passage of macro-TSH per se possible? Heinrichs et al 20 reported that TSH was undetectable in cord plasma obtained at birth from two infants with congenital absence of the anterior pituitary gland, suggesting that TSH cannot be transferred from mothers to their fetuses through the placenta. Bajoria and Fisk 21 examined the permeability of human placenta to TSH using a perfusion system of isolated placenta and concluded that the poor transplacental passage of TSH was not due to the degradation of TSH by the placenta but to the slow passive diffusion because of its relatively high molecular weight. Taken together with these previous reports and our present finding that macro-TSH in neonates was of maternal origin, we hypothesize that anti-TSH autoantibodies developed in mothers were transferred to their babies through the placenta and formed macro-TSH by binding to neonatal TSH.
HAMAs interfere with sandwich-type immunoassays and may produce spuriously high TSH concentrations by bridging capture and detection antibodies without TSH. 12,13 Since HAMAs are γ-globulins, PEG treatment of the serum samples containing HAMAs removes them, resulting in high PEG precipitation ratios of TSH. We used a 125I-TSH binding assay, which would not be affected by HAMAs. The sera from the four babies showed a high binding ratio of 125I-TSH, which was suppressed by a large amount of unlabeled human TSH, indicating the presence of anti-TSH autoantibodies.
We further investigated the characteristics of the autoantibodies in one baby and its mother. Autoantibodies were more reactive specifically to human TSH than to rat TSH. Other hormones, such as human LH, FSH, and hCGα, which share the same α subunit, 22 did not displace 125I-TSH from the autoantibodies, suggesting that the autoantibodies were directed to the human TSH-β subunit. Human TSH-β consists of 118 amino acids and exhibits 90.6% homology with the amino acid sequence of rat TSH-β. 23 The epitopes on TSH that are shared, in part, among humans and rats may have been antigenic and led to the production of anti-human TSH-β autoantibodies that partially cross-reacted with rat TSH-β. The Kd was 10−6.26 M in one baby and 10−6.00 M in its mother, which showed a similar low binding affinity, also supporting the idea that anti-TSH autoantibodies in neonates are derived from their mothers.
The results of the GFC appear puzzling. No macro-TSH was detected on GFC except for baby 1 and its mother 1 among the four babies and their mothers, in whom the presence of anti-TSH autoantibodies was identified by 125I-TSH binding study. Because of the low affinity of the autoantibodies, the complex of TSH and anti-TSH autoantibodies might have been dissociated during the analytical procedure and could not be detected as macro-TSH on GFC. In baby 1 and its mother 1, the binding of TSH to the autoantibodies might be relatively strong, as speculated by the least degree of displacement of 125I-TSH by an excess amount of unlabeled TSH; thus, macro-TSH was partially demonstrated on GFC in these cases.
On whom workup for macro-TSH should be conducted? If TSH level is very high and fT4 is normal as in the previous case reports, it would be easy to suspect macro-TSH. However, it would be difficult to notice it as in the present four neonates having mildly elevated TSH levels and in their mothers having normal TSH levels. In this study, we examined the presence of macro-TSH in all 939 neonates and some of their mothers irrespective of their serum TSH levels. We think that the present four neonates and their mothers with macro-TSH would never have been detected in the clinical setting. Only this kind of comprehensive analysis of all samples could have disclosed macro-TSH in them.
Elevated serum TSH levels in patients with macro-TSH are due to the slow clearance of macro-TSH from the circulation, 9 not to the compensatory TSH secretion for hypothyroidism. Thus, thyroid hormone replacement therapy is not necessary in patients with macro-TSH. Recent guideline for congenital hypothyroidism recommends that if the serum TSH concentration is >20 mU/L at confirmatory testing approximately in the 2nd week of life, treatment should be started even if fT4 is normal. 1 The screening of macro-TSH in neonates should be applied to this group. If PEG precipitation ratio of TSH determined by HAMA blocker-contained assay platform is >80%, macro-TSH is suspected. If serum TSH concentrations of their mothers are also high and the PEG precipitation ratio is >80%, the diagnosis of macro-TSH is more likely and the treatment should be withheld.
It is uncertain why serum TSH levels were mildly elevated or even normal in our macro-TSH cases. A low affinity of anti-TSH autoantibodies in the present cases might be responsible or we have found macro-TSH cases in the very early stages developing into the overt macro-TSH. Further study over a long-term observation may give us the answer.
Footnotes
Acknowledgment
The authors thank Geoff Gillespie for assistance in preparing this article.
Authors' Contributions
N.H. conceived the experiments and wrote the article in consultation with A.S. K.A. contributed to clinical sample collection and the analysis of clinical data. A.Y. and T.M. carried out the experiments.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by a grant from the Ritsumeikan University.