
Abstract
Background:
Fetal overgrowth (large for gestational age, LGA) is associated with an increased risk of maternal and fetal morbidity and adverse health outcomes. Thyroid hormones are key regulators of metabolism during pregnancy and fetal development. Lower maternal free thyroxine (fT4) and higher maternal triglyceride (TG) levels during early pregnancy are associated with higher birth weight. We aimed at examining the mediating role of maternal TG in the association between maternal fT4 and birth weight.
Methods:
We performed a large prospective cohort study including pregnant Chinese women who were treated at a tertiary obstetric center during the period of January 2016 to December 2018. We included 35,914 participants with complete medical records. We performed causal mediation analysis to decompose the overall effect of fT4 on birth weight and LGA with maternal TG as the mediator.
Results:
We observed statistically significant associations between maternal fT4, TG levels, and birth weight (all p < 0.0001). Using a four-way decomposition model, we identified a controlled direct effect (coefficient [confidence interval, CI], −0.038 [−0.047 to −0.029], p < 0.0001) that accounted for 63.9% of the total effect, in addition to the other three estimated effects (reference interaction, coefficient [CI] = −0.006 [−0.009 to −0.001], p = 0.008; mediated interaction, coefficient [CI] = 0.0004 [0.000 to 0.001], p = 0.008; and pure indirect effect, coefficient [CI] = −0.009 [−0.013 to −0.005], p < 0.0001) of TG on the association between fT4 and birth weight Z score. Moreover, maternal TG accounted for 21.6% and 20.7% (via mediation) and 13.6% and 41.6% (via maternal fT4 and TG interaction) of the total effect of maternal fT4 on fetal birth weight and LGA, respectively. The proportions of the total associations that could be reduced by “eliminating” the effect of maternal TG were 36.1% for birth weight and 65.1% for LGA, respectively.
Conclusions
: High maternal TG levels may play substantial mediating roles in the relationship between low fT4 levels in early pregnancy and increased birth weight and a higher risk of LGA. Further, the occurrence of fetal overgrowth may also be influenced by possible synergistic effects between fT4 and TG.
Introduction
The intrauterine environment shapes the postnatal developmental trajectories and long-term health of the fetus. 1 Pregnancies with dysregulated metabolic and hormonal balance may be complicated by an adverse pregnancy or newborn outcomes (e.g., post-term pregnancy, C-section delivery, perinatal asphyxia, and fracture), specifically fetal overgrowth (e.g., large for gestational age [LGA]). 2,3 LGA is an important risk factor for childhood obesity 4 and type 2 diabetes in adult life. 5
We previously found that low levels of maternal free thyroxine (fT4 level, <2.5th percentile) in early pregnancy were associated with a 0.7 standard deviation higher birth weight and a 40% higher risk of LGA. 6 A recent meta-analysis also indicated that lower fT4 levels and isolated maternal hypothyroxinemia were associated with higher mean birth weight (45 and 21 g, respectively). 7 However, specific mechanisms underlying this association remain unknown.
A previous study demonstrated that a lower fT4 concentration during pregnancy was associated with adverse maternal lipid profiles. 8 Levothyroxine (LT4) may improve the lipid profile of pregnant and nonpregnant women with subclinical hypothyroidism. 9,10 Several studies have shown that even mild alterations in thyroid hormone (TH) levels may significantly affect lipid metabolism through the regulation of lipogenesis and beta-oxidation. 11 –13
A Mendelian randomization study found a causal relationship between decreased fT4 and increased lipid levels. 14 Interestingly, a higher maternal triglyceride (TG) level in early pregnancy was associated with higher birth weight and a higher risk of LGA. 15,16 It was also noted that exposure to maternal hyperlipidemic conditions induced by a high-fat diet may cause long-term disorders in offspring in mice. 17,18 Based on these observations, it is possible that some of the effects of maternal TH availability are mediated through changes in maternal TG concentrations, but the relationship among maternal thyroid function, lipid, and birth weight is complicated and remains not well defined.
In this study, we aimed at examining whether maternal TG was a mediator in the relationship between the maternal fT4 levels and birth weight or LGA.
Methods
Study participants
This was a large prospective cohort study (Chinese Clinical Trial Registry, registration No. ChiCTR1800014394) at a tertiary maternity care hospital in Shanghai, China. The participants were consecutively recruited from the International Peace Maternity and Child Health Hospital (IPMCH). A total of 43,771 pregnant women were enrolled in the study between January 2016 and December 2018. Participants were eligible if they were pregnant, could complete full antenatal visits at the IPMCH, and underwent thyroid function measurements in the first trimester.
Moreover, patients were excluded if they had a twin pregnancy, fetal loss, or in vitro fertilization; received medical treatment for thyroid dysfunction (including LT4, propylthiouracil, and methimazole) before or during pregnancy; had pre-existing hyperlipidemia, a history of thyroid disease, hepatic steatosis, diabetes, or hypertension; or had missing key values (i.e., TG). The study protocol was approved by the Medical Ethics Committee (No. GKLW2016-69) of the IPMCH. All participants signed a written informed consent form before participating in the study.
Blood samples and biochemical analyses
Fasting blood samples were drawn from each participant to test their thyroid function and lipid profile during the same period of early pregnancy (weeks 9–13). The serum was then separated from all samples by centrifugation and was sent to a clinical laboratory for analysis. fT4, thyrotropin (TSH), and antibodies against thyroperoxidase (TPO-Ab) were also quantified using the corresponding kits (Abbott, Chicago, IL) on the ARCHITECT i2000, following the manufacturer's instructions as previously described. 19
The cutoff value of TPO-Ab was 5.6 IU/mL according to the manufacturer's protocol. The pregnancy-specific references (confidence interval [CI]) for the fT4 and TSH levels in early pregnancy were 11.7–19.7 pmol/L and 0.03–3.64 mU/L, respectively, which were calculated locally as per the recommendations of the American Thyroid Association. 20 Serum TG and other maternal lipids (e.g., total cholesterol [TC], high-density lipoprotein cholesterol [HDL-C], low-density lipoprotein cholesterol [LDL-C], apolipoprotein AI [Apo AI], and apolipoprotein B [Apo B]) were determined using commercial enzymatic colorimetric assays (Roche Diagnostics, Mannheim, Germany) and were analyzed using a Cobas c702 analyzer (intra- and inter-assay coefficients of variation of <5%).
Assessments of covariates
Data were prospectively collected by nurses, residents, and gynecologists during routine pregnancy checkups. Data on maternal age, parity, last menstrual period (LMP), medical history, and educational status were obtained via face-to-face interviews during the first clinical visit. The pre-pregnancy body mass index (BMI) was calculated by dividing the self-reported pre-pregnancy body weight by the squared hospital-measured height in early pregnancy.
Women with a BMI of ≥24.0 or <24.0 kg/m2 were defined as overweight and obese (OWO) and non-OWO, respectively. 21 Gestational age was determined based on LMP and subsequently adjusted according to ultrasound results in early pregnancy. Information on birth weight, gestational duration, and fetal sex was recorded in the inpatient hospital information system. Alcohol consumption and smoking status were not analyzed, as they were rarely (<0.1%) used during pregnancy.
Diagnostic criteria
The primary outcome of this study was the standardized birth weight Z score of live-born singletons by gestational week at delivery based on the INTERGROWTH-21st newborn birth weight standards. 22 The LGA was defined as birth weight greater than the 90th standardized percentile for gestational age and neonatal sex. We defined isolated maternal hypothyroxinemia (IMH) as an fT4 level of <2.5th percentile (11.7 pmol/L) with the TSH level within the normal range (0.03–3.64 mIU/L).
The subclinical hypothyroidism (TSH level of >3.64 mIU/L with the fT4 level within the normal range [11.7–19.7 pmol/L]), overt hypothyroidism (fT4 level of <11.7 pmol/L with the TSH level of >3.64 mIU/L), overt hyperthyroidism (fT4 level of >19.7 pmol/L with the TSH level of <0.03 mIU/L), and euthyroid (fT4 level within the normal range [11.7–19.7 pmol/L] with the TSH level within the normal range [0.03–3.64 mIU/L]) groups were defined based on our previous publication. 23
Statistical analyses
Continuous and categorical variables were presented as medians (interquartile ranges [IQRs]) and frequencies (percentages), respectively. Because of a skewed distribution, maternal TG values were log-transformed for analyses. Model assumptions were assessed with residual plots, outlier exclusions, and by utilizing restricted cubic splines with three knots to assess potential nonlinearity.
Considering the potential synergistic effect of low fT4 and high TG levels on birth weight, 19 either direct or indirect effects will be biased using traditional mediation models. Therefore, we conducted casual mediation analysis using a four-way decomposition model to assess the unification of mediation and interaction. 24,25 The total effect of the maternal fT4 levels on birth weight or LGA was separated into a controlled direct effect (CDE, without TG), reference interaction (INTref, interaction without mediation by TG), mediated interaction (INTmed, both interaction and mediation), and pure indirect effect (PIE, mediation without interaction). 26
In addition, proportion eliminated indicated the proportion of the total effect of maternal fT4 that could be eliminated by eliminating the mediator (TG). Multivariate linear and logistic regression models were adjusted for maternal age, parity, education level, TPO-Ab positivity, and pre-pregnancy BMI. These potential confounders were identified considering their biological plausibility and clues from previous studies. 6,19
All statistical analyses were performed using R statistical software version 4.1.0 (R Project for Statistical Computing; packages rms, visreg, tidyverse, and CMAverse 27 ). A p-value of <0.05 was considered statistically significant.
Results
Population characteristics
The final study population consisted of 35,914 pregnant women (Supplementary Fig. S1). The median (IQR) maternal age was 30 (28–33) years, and the median pre-pregnancy BMI was 20.7 (IQR, 19.2–22.6) kg/m2. A total of 24,981 (69.5%) were primiparous, 9239 (25.7%) did not have college education, 1501 (4.2%) had pregnancy-induced hypertension, 4551 (12.7%) had gestational diabetes mellitus (GDM), and 5380 (15.0%) fetuses were born LGA.
The median TSH level was 1.17 (range, 0.65–1.80) mU/L, the median fT4 level was 14.10 (range, 13.10–15.20) pmol/L, and 3396 women (9.5%) were TPO-Ab positive (Table 1). Based on the pregnancy-specific reference range calculated locally, 20 the prevalence of IMH, subclinical hypothyroidism, overt hypothyroidism, and overt hyperthyroidism in this cohort were 3.4%, 2.3%, 0.3%, and 1.2%, respectively.
Demographic Data of the Study Population
Continuous variables are presented as median and IQR; categorical variables are presented as numbers of cases and percentage.
BMI, body mass index; fT4, free thyroxine; GDM, gestational diabetes mellitus; IMH, isolated maternal hypothyroxinemia; IQR, interquartile range; LGA, large for gestational age; TG, triglyceride; TPO-Ab, antibodies against thyroperoxidase; TSH, thyrotropin.
Association between the maternal fT4 and TG levels in early pregnancy and fetal birth weight and LGA
First, we evaluated the associations between fT4 in the full range, TG, and birth weight Z score using nonlinear models (Supplementary Fig. S2). We observed that the associations between fT4 and TG or birth weight Z scores were L-shaped, with a steep decrease in the birth weight Z score and the maternal TG, with maternal fT4 increased to 20–30 pmol/L and then stabilized. To better assume the parameters, pregnant women with hyperthyroxinemia (fT4 level of >19.7 pmol/L, according to the 97.5th percentile of the predefined reference range 23 ) were excluded from the subsequent analysis.
Associations between maternal fT4, TG, and birth weight Z scores were statistically significant (all p < 0.0001) after adjusting for potential confounders (Table 2 and Fig. 1). Maternal fT4 was inversely associated with birth weight Z score (Fig. 1A; β = −0.028; CI, −0.034 to −0.023; p < 0.0001) and maternal TG (Fig. 1C; β = −0.017; CI, −0.020 to −0.015; p < 0.0001), which was positively associated with birth weight (Fig. 1B; β = 0.208; CI, 0.182 to 0.233; p < 0.001).
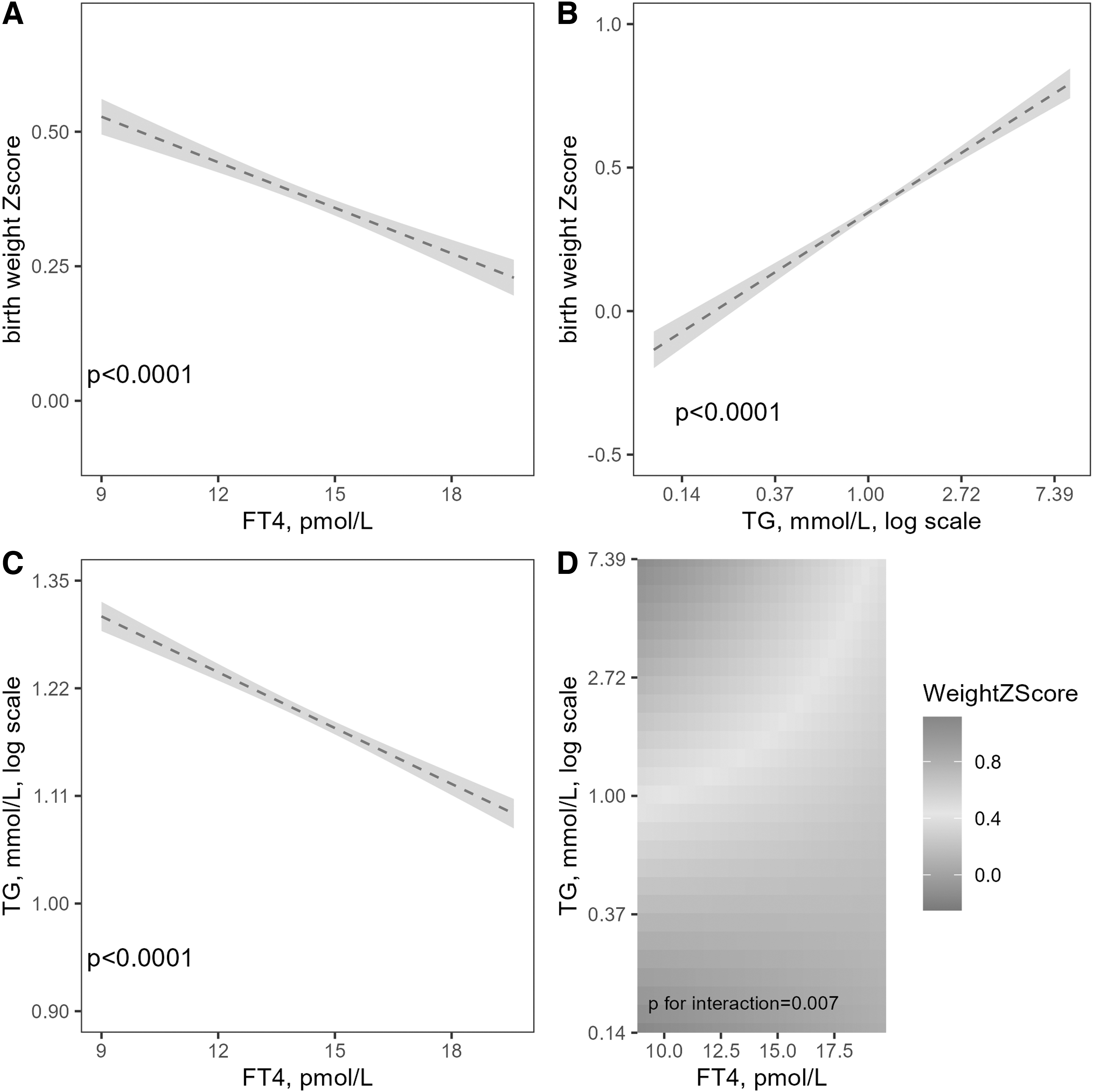
The associations between maternal fT4, maternal TGs and fetal birth weight. Linear regression models for (
Linear and Logistic Regression Models for Associations of Maternal Free Thyroxine, and Triglyceride Concentrations at Early Pregnancy with Fetal Birth Weight Z Score and Large for Gestational Age
Models 1 and Models 3 were the unadjusted models. Model 2 was adjusted for maternal age, education level, parity, TPO-Ab positivity, and pre-pregnancy BMI; Model 4 were adjusted for maternal age, education level, parity, and pre-pregnancy BMI.
p < 0.0001.
β, CI: The beta coefficients and CI derived from multivariable linear models.
CI, confidence interval; Log-TG, triglyceride, log-transformed; OR, odds ratio.
A similar association was apparent for LGA (Table 2 and Fig. 2). There was evidence of an interaction between the maternal fT4 and TG levels for the association with birth weight (Fig. 1D, p = 0.007). However, there was no association between the maternal TSH and TG levels and LGA (Supplementary Tables S1 and S2, p > 0.05).
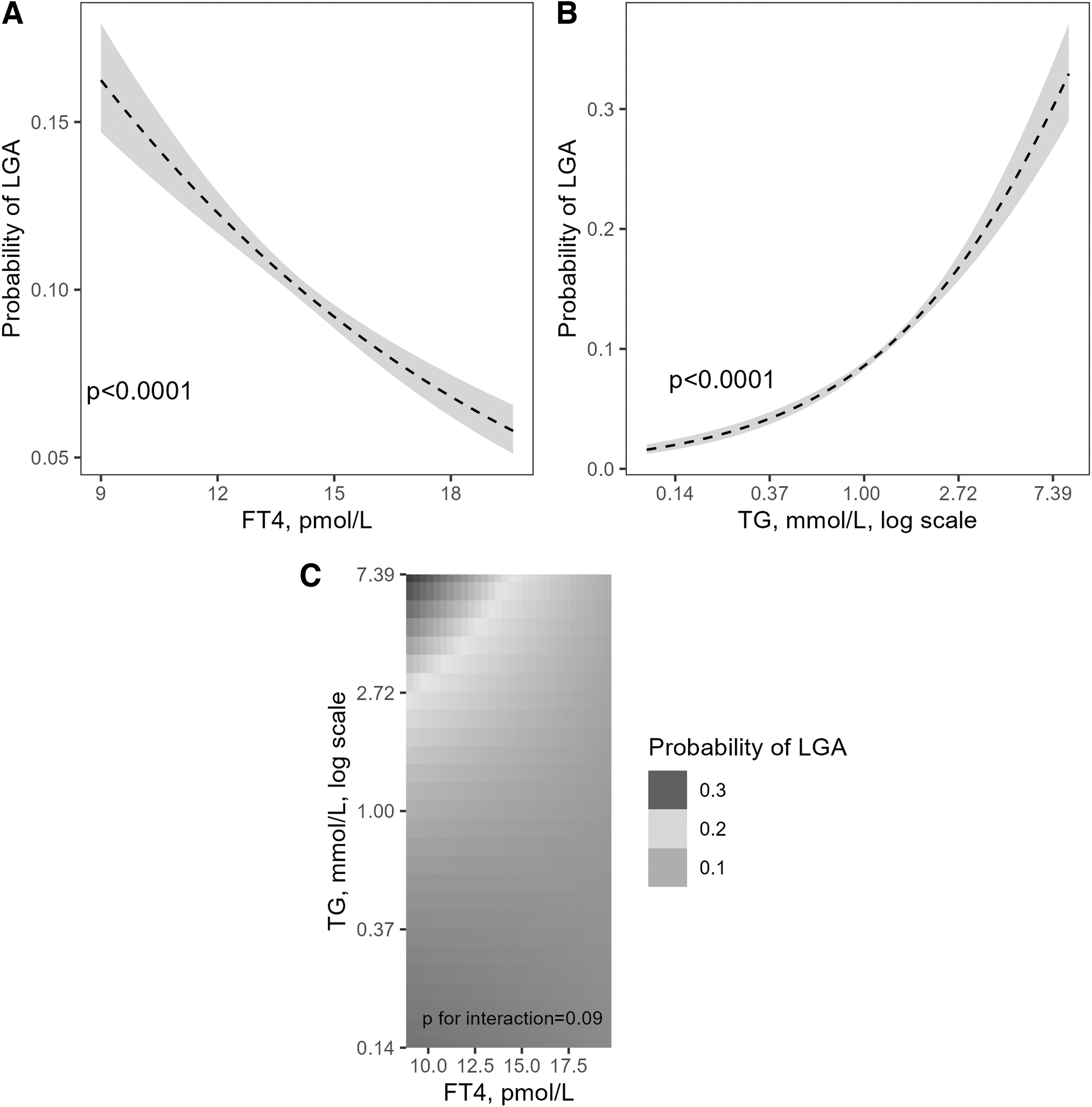
The associations between maternal fT4, maternal TG, and the risk of LGA. Logistic regression models for (
Decomposition of the estimated effect of maternal TG on the association of maternal fT4 with fetal birth weight and LGA
Subsequent causal mediation analysis demonstrated that maternal TG levels appeared to play a substantial role in explaining the association between maternal fT4 and fetal birth weight (Table 3 and Fig. 3). The total effect of maternal fT4 on birth weight (estimated coefficient, −0.038; CI, −0.047 to −0.029) could be decomposed as follows (Table 3).

Directed acyclic graphs for analyses between maternal fT4, maternal TG and fetal birth weight. These directed acyclic graphs representing the relationship between maternal fT4, maternal TGs (log-transformed) and birth weight using four-way decomposition models. The total effect of maternal fT4 on LGA was separated into (
Decomposition of the Estimated Effect of Maternal Free Thyroxine Levels on Fetal Birth Weight Z Score Altered by Maternal Triglyceride
The estimated total effect of maternal fT4 on fetal birthweight Z score was decomposed into four components (Total effect = CDE + INTref + INTmed + PIE) by multi-variable linear regression models adjusted for maternal age, education level, parity, TPO-Ab positivity, and pre-pregnancy BMI. PDE = CDE + INTref; TIE = INTmed + PIE; Proportion mediated = TIE/Total Effect; Proportion attributable to interaction: (INTref + INTmed)/Total Effect; Proportion eliminated: (INTref + INTmed + PIE)/Total Effect.
CDE, controlled direct effect; INTmed, mediated interaction; INTref, reference interaction; PDE, pure direct effect; PIE, pure indirect effect; TIE, total indirect effect.
The CDE (the direct effect of fT4 on birth weight in the absence of TG; estimated coefficient, −0.024; CI, −0.030 to −0.019; p < 0.0001) was 63.9% of the estimated total effect and was significantly larger than the other three effects, including 14.5% of INTref (the effect only due to the interaction between TG and fT4 when the TG would be high in the absence of fT4; estimated coefficient, −0.019; CI, −0.009 to −0.001; p = 0.008), −1.0% of INTmed (due to both mediation and interaction by TG; estimated coefficient, 0.0004; CI, 0.000 to 0.001; p = 0.008), and 22.6% of PIE (pure mediated effect by TG; estimated coefficient, −0.009; CI, −0.013 to −0.005; p < 0.0001) altered by maternal TG.
The proportion of the association between maternal fT4 levels and birth weight that could be reduced by “eliminating” the mediating role of TG was 36.1%.
Maternal TG levels also played an important role in mediating the relationship between maternal fT4 and the risk of LGA (Table 4). The excess relative risk for CDE was −0.033 (CI, −0.101 to 0.034; p = 0.333), which was not statistically significant, accounting for 35.0% of the estimated total effect. The proportion attributable to the INTref was 44.4% (excess risk, −0.042; CI, −0.091 to 0.007; p = 0.091), the proportion attributable to INTmed was −2.8% (excess risk, 0.003; CI, 0.0004 to 0.005; p = 0.020), and the proportion attributable to the PIE was 23.5% (excess risk, −0.022; CI, −0.036 to −0.009; p = 0.0005). The estimated proportion of the total association between maternal fT4 and LGA that could be reduced by “eliminating” the effect of the mediator was 65.1%.
Decomposition of the Estimated Effect of Maternal Free Thyroxine Levels on the Risk of Large for Gestational Age Infants Altered by Maternal Triglyceride
The estimated total effect of maternal fT4 on LGA was decomposed into four components (Total effect = CDE + INTref + INTmed + PIE) by multi-variable logistic regression for the outcome model and linear regression for the mediator model. The outcome model included an interaction term between the exposure (maternal fT4) and the mediator (maternal TG, log-transformed). Models were adjusted for adjusted for maternal age, education level, parity, TPO-Ab positivity, and pre-pregnancy BMI.
Further, the largest proportion attributable to the effect of IMH on LGA was CDE (73.7%; excess risk, 0.282, CI: 0.207 to 0.358; p < 0.0001; Table 5), and the PIE of TG accounted for 12.4% (excess risk, 0.048; CI, 0.034 to 0.06; p < 0.0001) of the total effect. No such effect was observed in the 4-way decomposition of the total effect of the association of fT4 with SGA (Supplementary Table S3; p > 0.05).
Decomposition of the Estimated Effect of Isolated Maternal Hypothyroxinemia on the Risk of Large for Gestational Age Infants Altered by Maternal Triglyceride
The estimated total effect of maternal fT4 on LGA was decomposed by 4-way decomposition (total effect = CDE + INTref + INTmed + PIE) method using a multi-variable logistic regression model for the outcome and a linear regression model for the mediator. The model for outcome included an interaction term between the exposure (IMH) and the mediator (maternal TG, log-transformed). Models were adjusted for adjusted for maternal age, education level, parity, TPO-Ab positivity, and pre-pregnancy BMI. Proportion mediated: (INTmed + PIE)/Total Effect; Proportion attributable to interaction: (INTref + INTmed)/Total Effect; Proportion eliminated: (INTref + INTmed + PIE)/Total Effect.
The mediating effect of the maternal TG remained unchanged after excluding women with GDM and hypertensive disorder of pregnancy (proportion of PIE = 20.5%, p = 0.0003, Supplementary Table S4). The PIE was still significant in euthyroid women (19.2%, p = 0.001, Supplementary Table S5). Subgroup analyses indicated that the PIE of maternal TG on the association of maternal fT4 with fetal birth weight were especially significant in pregnant women in lower fT4 category (<25th percentile [13.1 pmol/L]; proportion attributable, 45.8%; p < 0.0001; Supplementary Table S6) and non-OWO pregnant women (proportion attributable, 19.5%; p = 0.0009; Supplementary Table S7).
Effects of maternal fT4 and other maternal lipid biomarkers in early pregnancy on fetal birth weight
As shown in Supplementary Table S8, higher fT4 levels were associated with lower maternal TC, LDL-C, Apo B, and HDL-C levels during early pregnancy (all p < 0.0001), except for Apo AI (p = 0.185). The maternal TC, LDL-C, and Apo B levels were positively associated with birth weight, whereas the HDL-C and Apo AI levels were inversely correlated with birth weight (Supplementary Table S9, p < 0.0001 for all). Further analyses using the four-way decomposition model showed no significant interaction effects in TC, LDL-C, HDL-C, Apo AI, and Apo B (all p > 0.05 for INTref and INTmed).
In addition, the pure mediating effects of TC, LDL-C, HDL-C, and Apo AI (all p > 0.05), except Apo B (accounting for 11.7% of the total effect, p = 0.041), did not significantly affect the association between the maternal fT4 levels and birth weight (Supplementary Table S10).
Discussion
In this study, we demonstrated that low maternal fT4 levels were associated with higher birth weight and an increased risk of LGA in a large prospective birth cohort in China, and these associations were partially mediated through elevated maternal TG levels. The mediating effects by maternal TG were substantial in women with lower fT4 (<25th percentile) and in non-OWO women. In addition, the mediatory role of TG was greater than other lipid biomarkers, including TC, LDL-C, HDL-C, Apo AI, and Apo B, in explaining the association between lower maternal fT4 levels and higher birth weight. In addition, the potential synergistic effects of fT4 and TG may also contribute to fetal overgrowth, although not significant for LGA.
The relationship between hypothyroidism and TG on birth weight is complex. To delineate this, we conducted a causal mediation analysis by adopting a robust and flexible method (the four-way decomposition) to investigate the mediation and interaction pathways simultaneously. First, low fT4 could directly affect birth weight (CDE, 63.9%).
Second, we observed a significant contribution of the PIE (22.6%), indicating that TG was an important mediator between low fT4 levels and high birth weight. Last, a notable portion of INTref (14.5%) and very low proportion of INTmed (<1.0%) were observed, which indicated that fetal overgrowth could be partially due to the synergistic interplay between fT4- and TG-induced factors, apart from low fT4 levels. In particular, the proportions of the total associations between maternal fT4 and birth weight and LGA that could be reduced by “eliminating” the effect of TG were 36.1% and 65.1%, respectively. Thus, TG could be a meaningful mediator for the total effect of fT4 on birth weight or LGA and further studies are required to identify the exact mechanism.
Consistent with previous studies, 6,7 we verified that the maternal fT4 levels in early pregnancy were negatively associated with birth weight. Knight et al. showed that IMH is associated with an adverse maternal lipid profile. 8 It was demonstrated that maternal high TG levels were associated with increased birth weight and a higher risk of LGA in both European and Chinese populations. 15,16 Considering these evidences, there is a biological plausibility that maternal thyroid hypofunction may be attributed to an adverse maternal lipid profile, leading to uncontrolled fetal growth.
In addition to previous studies emphasizing the direct effect of TH on fetal growth by, for example, affecting fetal development, facilitating placentation, and increasing oxygen consumption, 7,28 our results provide alternative explanations for the relationship between maternal fT4 and birth weight through the mediating effect of maternal TG.
Various forms of evidence support our findings. First, the maternal TG levels are important for intrauterine development. 29,30 Lipogenesis and fat accumulation was enhanced in early pregnancy to prepare for rapid neonatal growth during later gestational stages. However, hyperlipoproteinemia may result from maladaptation to metabolic remodeling with rapid changes of hormone levels in early pregnancy. 31 –33 Second, it was found that maternal lipid levels in early gestation correlated with cord blood profile and birth weight. 34
Third, fatty acids derived from maternal plasma TG can promote the placental expression of insulin-like growth factors to promote intrauterine fetal growth. 35 Last, maternal TH could affect lipophagy in the liver and amplifies the quantity of lipid-laden autophagosomes, where TGs are broken down into fatty acids. 13,36 A recent study found that TH administration reduced the TG levels and restored autophagy in the liver. 37 Further studies are warranted to unravel the mechanism in the link between maternal hypothyroid function and fetal overgrowth with the contribution of maternal lipids.
This study has various limitations. First, this was a single-center cohort study with a single race/ethnicity. Future studies with multiple obstetric centers and other ethnic groups are needed to validate the results of our study. Second, although a series of potential confounders were adjusted in the causal mediation models, residual confounding cannot be ruled out.
Third, despite access to the maternal fT4 and lipid levels during early gestation, the potential effects of dynamic changes in the TH and lipid levels throughout pregnancy have not been studied. Finally, our results were based on an observational dataset that limits the inference of causality.
In conclusion, our results suggest that maternal TG may be an important mediating factor between low maternal fT4 levels and increased birth weight and a higher risk of LGA. Besides, potential synergistic effects of fT4 and TG might also contribute to fetal overgrowth. Future studies are required to investigate if LT4 treatment may normalize lipid profiles in women with gestational hypothyroidism or whether additional lipid altering treatments can optimize pregnancy outcomes.
Data Availability Statement
Data available on reasonable request.
Footnotes
Acknowledgments
The authors gratefully acknowledge the contributions and efforts of all pregnant women who participated in this study and the doctors and nurses involved in data collection and patient care. The authors thank Dr. Layal Chaker from Erasmus University Medical Center for statistical guidance.
Authors' Contributions
W.W.: methodology, analysis, data curation, writing original draft, and editing. Y.Z.: conceptualization, methodology, writing original draft, and editing. Y.L.: methodology, review, and editing. C.L.: data curation. J.R.: data curation, review, and editing. X.L.: methodology, review, and editing. T.I.M.K.: methodology, review, and editing. J.F.: methodology, review and editing, and supervision.
Author Disclosure Statement
All authors report no conflict of interest.
Funding Information
This work was supported by grants from the National Key Research and Development Program of China (2018YFC1004602) to J.F.; the National Natural Science Foundation of China (82261128001, 81974235) to J.F.; and the National Natural Science Foundation of China (82271706) to W.W.
Supplementary Materials
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Table S9
Supplementary Table S10
Supplementary Figure S1
Supplementary Figure S2