
Abstract
Objective:
Gestational transient thyrotoxicosis (GTT) and Graves' disease (GD) are the most common causes of hyperthyroidism during pregnancy. However, few studies have compared pregnancy outcomes of patients who had GTT with those who had GD in the first trimester of pregnancy.
Methods:
We conducted a prospective multicenter cohort study in China. Participants received questionnaires, physical examinations, and underwent measurements of thyrotropin (TSH), free thyroxine (fT4), thyroid peroxidase antibody (TPOAb), TSH receptor antibody (TRAb), and urinary iodine in the first trimester. The patients diagnosed with either GTT or GD and normal thyroid function (NTF) group were followed until delivery. The thyroid function and pregnancy outcomes were reported.
Results:
A total of 125 pregnant women with thyrotoxicosis and 246 age-matched pregnant women with NTF were included. (1) The thyroid function of the GTT group returned to normal range in the third trimester, but was consistently abnormal in the GD group. (2) The incidence of gestational diabetes mellitus (GDM) in the GTT group (11.5%, 9/78) was significantly higher than that in NTF group (4.9%, 12/246) (p = 0.037). The incidence of premature delivery in the GD untreated (30.8%, 8/26, p = 0.002) and treated groups (28.6%, 6/21, p = 0.008) was both, respectively, higher than that in the NTF group (7.7%, 19/246). Miscarriage (15.4%, 4/26 vs. 3.7%, 9/246, p = 0.026) and gestational hypertension (19.2%, 5/26 vs. 3.3%, 8/246, p = 0.004) were more prevalent in the GD untreated group than in the NTF group. (3) The presence of positive TRAb and positive TPOAb in the first trimester were independent risk factors for miscarriage (odds ratio [OR] = 5.23, confidence interval [CI] = 1.11–24.78, p = 0.037) and low birth weight infants (OR = 7.76, CI = 1.23–48.86, p = 0.029), respectively.
Conclusion:
In conclusion, pregnancy outcomes appear variable, according to the etiology of first trimester thyrotoxicosis. GTT appears to be associated with GDM. GD appears to be associated with an increased risk of premature delivery, gestational hypertension, and miscarriage. The diagnosis of GTT and GD patients during early pregnancy and appropriate treatment of GD patients may be associated with improved pregnancy outcomes.
Introduction
Thyrotoxicosis is associated with adverse pregnancy effects, such as miscarriage, premature delivery, stillbirth, low birth weight, and neonatal thyroid disease. 1 –3 Gestational transient thyrotoxicosis (GTT) and Graves' disease (GD) are the most common causes of hyperthyroidism during pregnancy. The incidence rates of GD and GTT have been reported to be 0.2–0.7% and 0.2–11%, respectively. 4 –7 GD and GTT differ in pathogenesis and duration, which directly determines the choice of treatments. 8,9 Notably, few prospective studies have focused on GTT and pregnancy outcomes, so the implications are unclear.
Antithyroid drugs are the mainstay treatment for GD, including propylthiouracil (PTU) and methimazole (MMI). Although PTU is preferred for thyrotoxicosis treatment in the first trimester of pregnancy, it can cross the placenta and can potentially cause fetal hypothyroidism and fetal malformations. 10 The risks and benefits of antithyroid drug therapy for GD hyperthyroidism during pregnancy are of interest to examine.
This study is part of a large-scale population-based study focusing on the subclinical hypothyroid during early pregnancy study (the SHEP study) in China. This prospective study aimed to assess dynamic changes in thyroid function of pregnant women with thyrotoxicosis (GTT and GD) and to examine any association of thyrotoxicosis in the first trimester of pregnancy with gestational and postpartum complications. The study also aimed to identify independent risk factors for adverse pregnancy outcomes in pregnant women with thyrotoxicosis.
Methods
Study participants
The SHEP study participants were enrolled from the departments of obstetrics, gynecology, and endocrinology across 19 hospitals in 3 cities (Shenyang, Dandong, and Dalian) of Liaoning Province in China, from June 2012 to May 2014. Of the 9245 pregnant women enrolled, 8105 pregnant women met the inclusion criteria of this study. Among them, 109 women were diagnosed with thyrotoxicosis in the first trimester of pregnancy (GTT = 73, GD = 36).
In addition, another 32 patients with newly diagnosed thyrotoxicosis (GTT = 16, GD = 16) during early pregnancy (4–8 weeks) who visited the outpatient department of endocrinology of the First Affiliated Hospital of China Medical University during the same period were also included in the subsequent follow-up study. These patients diagnosed with thyrotoxicosis were matched with 1:2 randomly selected age-matched pregnant women with normal thyroid function (NTF) from the SHEP cohort. All pregnancies were spontaneous and were followed up in the second (13–27 weeks) and third (≥28 weeks) trimesters, as well as in the puerperium phase (Fig. 1).
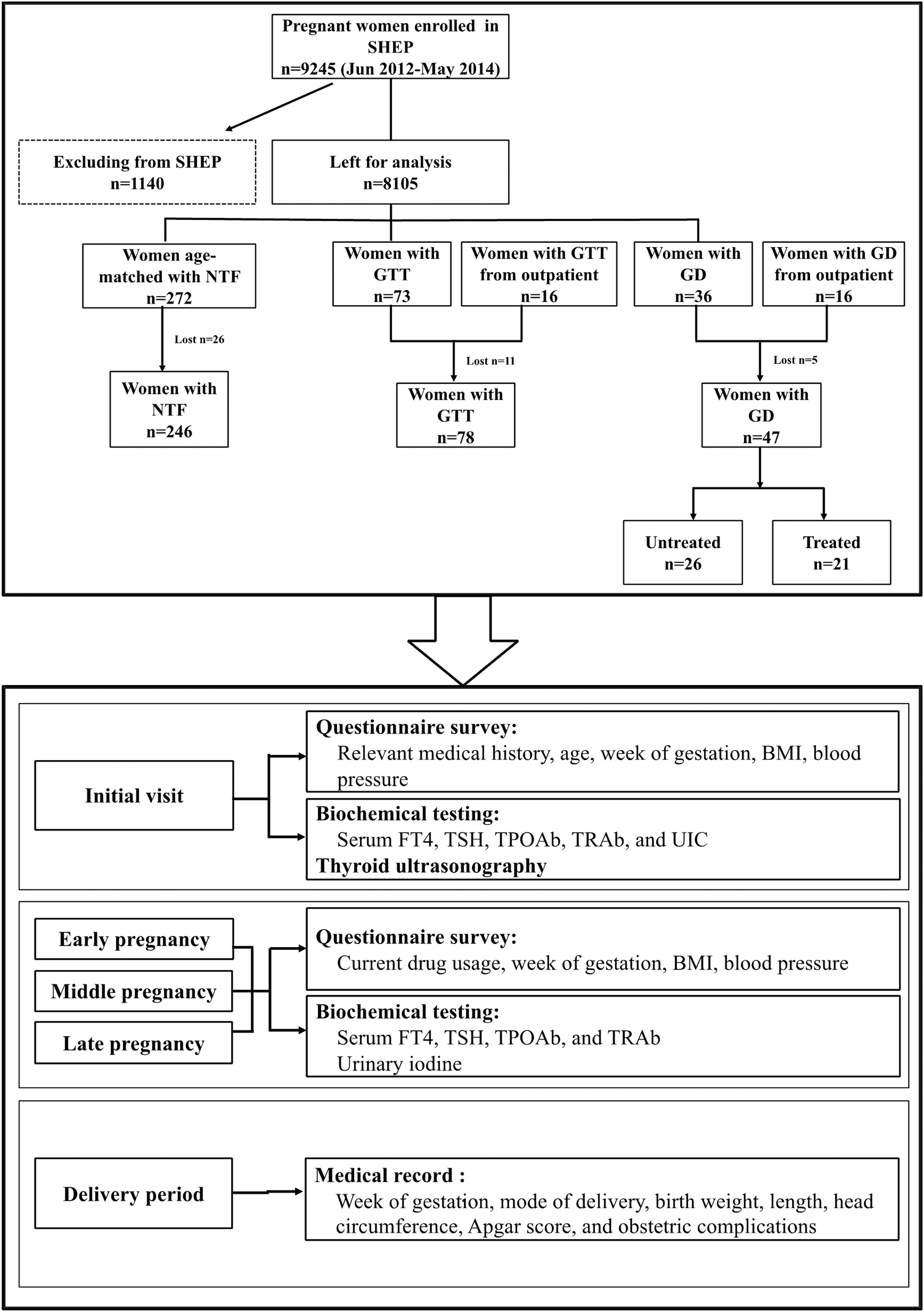
Flowchart illustrating the grouping and follow-up process of the pregnant women included in this study. BMI, body mass index; fT4, free thyroxine; GD, Graves' disease; GTT, gestational transient thyrotoxicosis; NTF, normal thyroid function; TPOAb, thyroid peroxidase antibody; TRAb, thyrotropin receptor antibody; TSH, thyrotropin; UIC, urine iodine concentration.
Pregnancy outcomes including miscarriage, premature delivery, gestational hypertension, gestational diabetes mellitus (GDM), fetal macrosomia, low birth weight infants, placental abruption, and postpartum hemorrhage were recorded. The gestational age was calculated based on the date of the last menstruation and confirmed by ultrasound examination. All adverse pregnancy outcomes were confirmed and reported by doctors in the gynecology and obstetrics clinics of these hospitals.
Some of patients with GD refused drug therapy even after being well informed of its necessity. Thus, the group of GD was further divided into treated and untreated subgroups. The participants in the GD-treated group received PTU with the intention to keep the serum free thyroxine (fT4) level near or slightly above the upper limit of the reference range.
All participants were long-term residents of Shenyang, Dandong, and Dalian cities, where the supply of dietary iodine is adequate. They responded to general questionnaires and had physical examinations. Serum thyrotropin (TSH), fT4, thyroid peroxidase antibody (TPOAb), and urine iodine concentration were measured. In addition, the participants with thyrotoxicosis were tested for TSH receptor antibody (TRAb). All the patients and controls who participated in the follow-up study underwent thyroid ultrasonography at baseline.
The study was approved by the medical ethics committee of China Medical University ([2012]2011-32-4) and was congruent with the Declaration of Helsinki. All participants signed informed consent forms before their participation in the study.
Biochemical measurements
Serum TSH, fT4, TPOAb, and TRAb levels were measured using an electrochemiluminescence immunoassay (Cobas e 601; Roche Diagnostics). Pregnancy-specific references were made by our laboratory in accordance with Guideline 22 of the National Academy of Clinical Biochemistry as previously described: 11,12 The reference ranges of TSH are first trimester: 0.14–4.87 mIU/L, second trimester: 0.27–3.80 mIU/L, and third trimester: 0.28–5.07 mIU/L. The reference ranges of fT4 are first trimester: 12.35–20.71 pmol/L, second trimester: 9.74–17.15 pmol/L, and third trimester: 9.63–18.33 pmol/L.
The TPOAb test was positive when TPOAb >34 IU/mL, and the TRAb test was positive when TRAb >1.75 IU/L. According to the American Thyroid Association guidelines for the diagnosis and management of thyroid diseases during pregnancy and postpartum, 13 the diagnostic criteria of GTT were as follows: (1) TSH <0.14 mIU/L and fT4 > 20.71 pmol/L and (2) negative serum TRAb and TPOAb tests. The diagnostic criteria of GD were as follows: (1) TSH <0.14 mIU/L and fT4 > 20.71 pmol/L and (2) positive serum TRAb test and positive or negative serum TPOAb test. Thyroid volume was estimated as the sum of volumes of both lobes, and the volume of each lobe was calculated as length × width × depth × 0.5 (cm3). 14
Definition of gestational and postpartum complications
The gestational and postpartum complications included (1) preterm delivery: live birth before 37 weeks; (2) gestational hypertension: no history of hypertension, systolic blood pressure (SBP) ≥140 mmHg or diastolic blood pressure (DBP) ≥90 mmHg during pregnancy; (3) GDM: universal testing by a 75 g OGTT at 24–28 weeks of gestation was used to diagnose GDM: 0 hour ≥5.1 mmol/L, 1 hour ≥10.0 mmol/L, 2 hours ≥8.5 mmol/L; (4) macrosomia: birth weight ≥4000 g; (5) low birth weight infants: birth weight <2500 g; (6) placental abruption; (7) postpartum hemorrhage; and (8) miscarriage: the spontaneous ending of pregnancy before 24 weeks.
Statistical analysis
Normally distributed variables are expressed as mean ± standard deviation. Student's t-test and analysis of variance were used for them to compare between or among groups, respectively. The non-normally distributed data are expressed as the median and interquartile range and compared using the Kruskal–Wallis test. Bonferroni post hoc tests were used for multiple comparisons. Chi-square test or Fisher's exact test was used to compare categorical variables presented as frequencies. Logistic regression was performed to identify variables associated with gestational and postpartum complications. All tests were two sided with a significance level defined as <0.05. All statistical analyses were conducted using SPSS version 16.0 (SPSS, Inc.).
Results
Comparison of the general characteristics of each group
There was no significant difference among the groups in terms of age, smoking, gestational age at thyroid function testing, history of miscarriage, blood pressure, and urine iodine concentration (Table 1). Body mass index (BMI) was significantly lower in the GTT group (19.57 ± 2.63 kg/m2, p = 0.02) and GD group (18.46 ± 2.47 kg/m2, p < 0.001) than that in the NTF group (20.52 ± 2.75 kg/m2). And thyroid volume was higher in both GTT group (15.86 ± 2.54 cm3, p < 0.001) and GD group (16.27 ± 2.64 cm3, p < 0.001) than that in the NTF group (10.94 ± 1.96 cm3).
Comparison of the General Characteristics of the Patient Groups
If the data obey the normal distribution, data are expressed as mean ± standard deviation and compared by ANOVA; if not, expressed as median (Q25–Q75) and compared by Kruskal–Wallis test. The chi-square test or Fisher's exact test was used to compare categorical variables. The p-value refers to the comparison among NTF, GTT, and GD (total) groups.
p < 0.05.
ANOVA, analysis of variance; BMI, body mass index; DBP, diastolic blood pressure; GD, Graves' disease; GTT, gestational transient thyrotoxicosis; NTF, normal thyroid function; SBP, systolic blood pressure; UIC, urine iodine concentration.
However, the differences in BMI (p = 0.077) and thyroid volume (p = 0.934) between GTT and GD groups were not significant. No significant difference was observed in BMI (p = 1.000) and thyroid volume (p = 0.601) between patients with GD who were untreated and those who were treated (Table 1).
Changes in thyroid function during pregnancy
The median level of TSH in the GTT group returned to the normal range in the third trimester, though the level remained lower than that of the NTF group (p < 0.001) (Table 2). The median fT4 level of the GTT group returned to normal in the second trimester, and it was significantly higher than that of the NTF group in the first and second trimesters (p < 0.001). The median TSH levels never returned to the normal range in both GD-treated and GD-untreated groups and were significantly lower than that in the NTF group at all stages of pregnancy (p < 0.001) (Table 2 and Supplementary Data).
Changes of Thyroid Function in Different Stages of Pregnancy
Data are expressed as medians and IQRs.
P < 0.05 vs. NTF.
P < 0.05 vs. GTT.
fT4, free thyroxine; IQR, interquartile range; TPOAb, thyroid peroxidase antibody; TSH, thyrotropin.
Although the fT4 level of the GD-treated group returned to normal, it was still significantly higher than the NTF group in the third trimester (p < 0.001). The TPOAb of GD-untreated group was higher than those of the NTF and GTT groups at each stage (p < 0.001) (Table 2).
Comparison of the neonatal birth weight in each group
The neonatal birth weight (NBW) was significantly lower in the GD-untreated group than that in the NTF (p = 0.021) and GTT groups (p = 0.007). However, the differences in NBW among the GD-treated group, NTF group, and GTT group were not significant (p = 0.192) (Fig. 2).
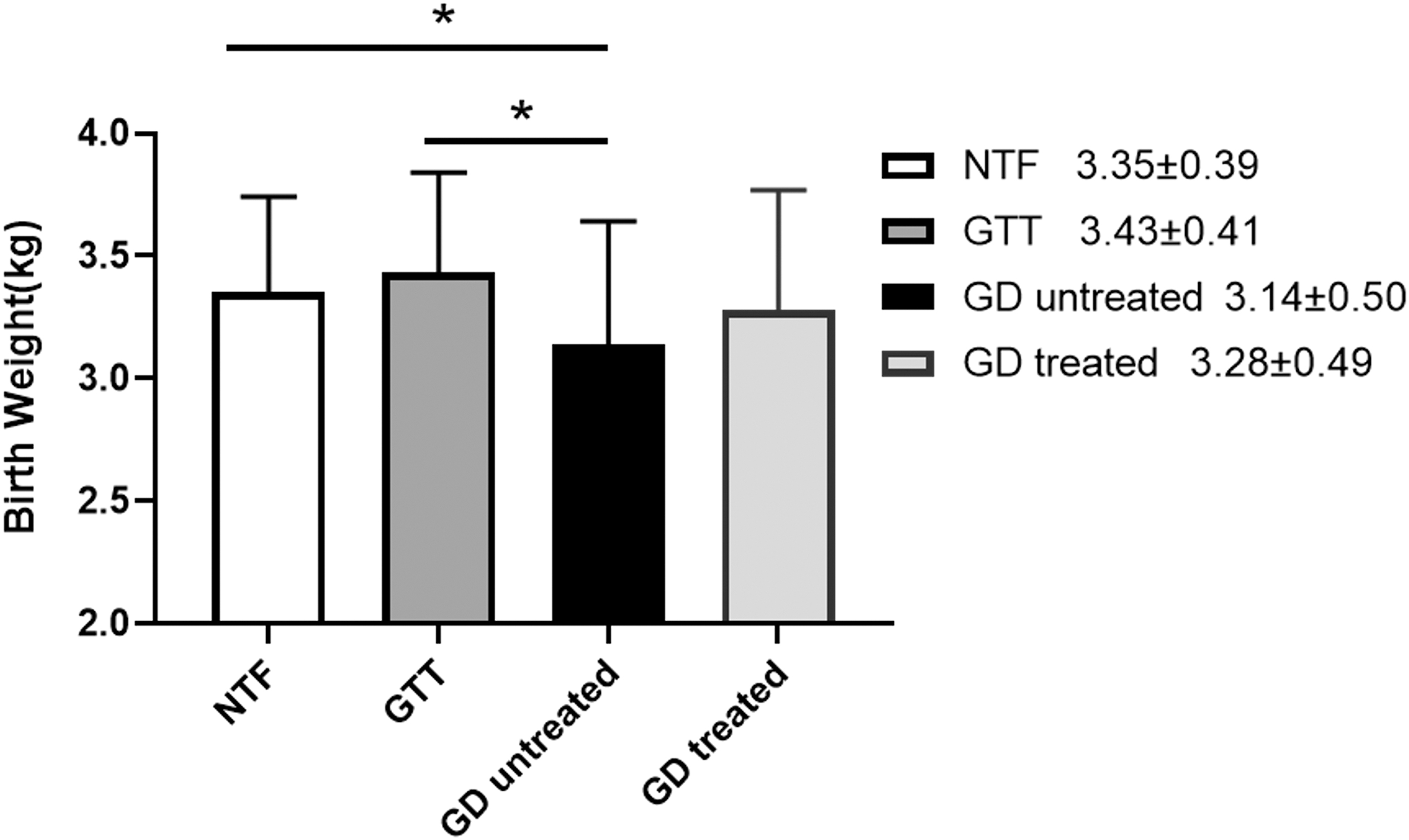
Comparison of the neonatal birth weight in each group. The data obey the normal distribution, expressed as mean ± standard deviation, and compared by ANOVA. *p < 0.05 was considered a significant difference. ANOVA, analysis of variance.
The incidence rates of the gestational and postpartum complications
As shown in forest plots for each risk factor (Fig. 4), the relative risk of GDM in the GTT group was 2.54 (risk ratio = 2.54, confidence interval [CI] = 1.03–6.29, p = 0.037). Moreover, the incidence rates of gestational hypertension (19.2%, 5/26 vs. 3.3%, 8/246, p = 0.004) and miscarriage (15.4%, 4/26 vs. 3.7%, 9/246, p = 0.026) were markedly higher in the GD-untreated group than those in the NTF group, but if patients with GD received treatment, their incidence rates did not differ significantly from those of the NTF group. The incidence rates of premature delivery were significantly higher in both GD-untreated (30.8%, 8/26, p = 0.002) and treated groups (28.6%, 6/21, p = 0.008) than that in the NTF group (7.7%, 19/246) (Figs. 3 and 4).
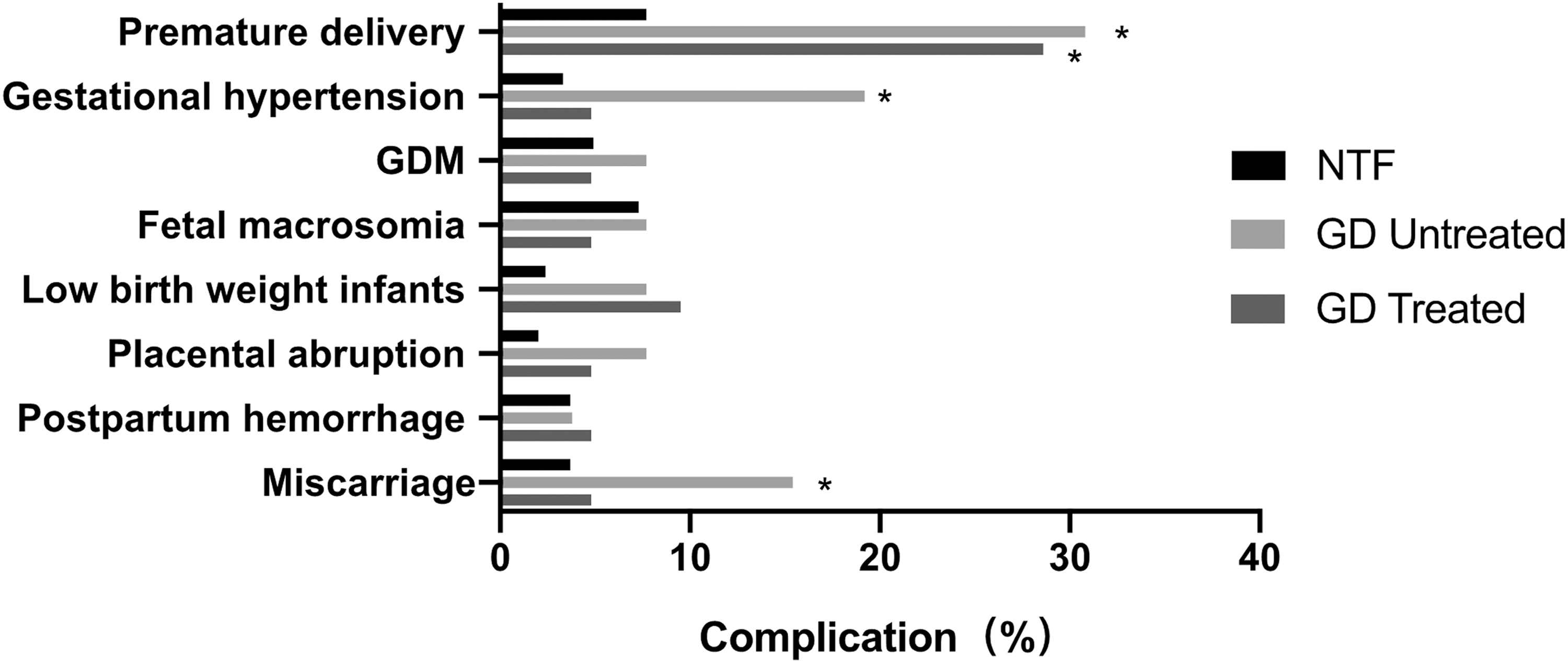
Gestational and postpartum complications in patient groups. *p < 0.05 vs. NTF. GDM, gestational diabetes mellitus.

Relative risks for gestational and postpartum complications in patient groups. Forest plots of relative risks and confidence intervals for pregnancy complications for pregnant women with GTT (
Risk factors for pregnancy gestational and postpartum complications
After adjustment for confounders (age, BMI, SBP, DBP, the levels of fT4, and TSH), positive TRAb and positive TPOAb in the first trimester were independently associated with miscarriage (odds ratio [OR] = 5.23, CI = 1.11–24.78, p = 0.037) and low birth weight of infants (OR = 7.76, CI = 1.23–48.86, p = 0.029), respectively (Table 3).
Multivariable Logistic Regression Analysis of the Risk Factors Associated with Gestational and Postpartum Complications
Bold indicates statistically significant values.
Univariate analysis was performed to determine variables associated with pregnancy complications, variables with a p-value of <0.25 were then included in a multivariable logistic regression analysis model to identify independent predictors. TSH and BMI are treated as continuous variables. TRAb and TPOAb are treated as categorical variables.
CI, confidence interval; OR, odds ratio; TRAb, TSH receptor antibody.
Discussion
This prospective cohort study evaluated the risk of gestational and postpartum complications in pregnant women with the first trimester thyrotoxicosis and revealed the different trends of thyroid function changes in GTT and GD patients. The thyroid function in all the GTT patients returned to normal by late pregnancy. Iijima reported that the TSH level of patients with GTT started to decrease at 8–14 weeks of pregnancy and dropped to the lowest level at 10–12 weeks of pregnancy. 15 Nambiar et al. revealed that the thyroid function in most GTT patients returned to normal by the end of the first trimester (at 14.4 weeks on average). 16
Consistent with our study, Niebyl also confirmed that some GTT patients may experience suppressed levels of serum TSH until the end of the second trimester. 17 Thyroid dysfunction in GD patients is more severe and lasts longer than that in patients with GTT. Moreover, we observed that the median levels of TSH in GD-treated and untreated groups never returned to the normal range in the second and third trimesters. It is consistent with American Thyroid Association guidelines that maternal thyroid function is allowed to be slightly high, which is usually associated with TSH suppression, to mitigate the risk of fetal hypothyroidism. 13
The levels of thyroid autoantibodies in GD patients in mid to late pregnancy were significantly lower than those in early pregnancy, which was consistent with the findings of previous studies. 18,19 This may be attributed to the moderate immunosuppression during pregnancy.
Thyrotoxicosis during early pregnancy impacts both maternal and fetal health. Due to differences in the baseline features of enrolled patients, the effects of thyrotoxicosis on pregnancy outcomes are subject to some uncertainty. Consistent with previous studies, the difference in NBW between GTT and NTF groups was not significant, which is related to the disease characteristics. 20,21 Goldman and Mestman demonstrated that fetal weight gain was mainly limited due to the increase of fT4 in the third trimester of pregnancy. 22
The fT4 level in the GTT group in this study returned to normal by midpregnancy and did not differ significantly from that of the NTF group at late pregnancy. Moreover, the incidence rate of GDM in the GTT group was significantly higher than that in the NTF group. The fetal weight of patients with GDM is often higher than normal. This led to the slightly higher NBW in the GTT group than that in the NTF group. Our study is consistent with previous studies showing that GTT is not associated with adverse postpartum complications. 23,24 However, we observed that GTT was associated with GDM, which was a novel finding.
An explanation for this observation is that thyroid hormones may promote intestinal absorption of glucose and increase hepatic glycogen output, thereby affecting blood glucose levels in pregnant women. 25 Oguz et al. observed that HbA1c level was negatively correlated with TSH level in patients with GTT during early pregnancy. 26 Our findings need to be confirmed and the potential mechanism by which GTT may be associated with GDM needs to be further investigated.
It is established that GD during pregnancy can have severe consequences for pregnancy outcomes. 27 –29 In this study, the NBW of the GD-untreated group was significantly lower than that of the NTF group. Consistent with previous studies, the difference between NBWs in GD-treated and NTF groups was not significant. 30 This result may be due to a negative correlation between maternal fT4 concentration and birth weight, especially in the third trimester. 31 We also observed that GD was associated with adverse pregnancy outcomes such as premature delivery and gestational hypertension. To further clarify the effect of treatment in GD patients on pregnancy outcomes, the GD patients were divided into untreated and treated subgroups.
This study revealed untreated GD is associated with an increased risk of premature delivery, gestational hypertension, and miscarriage. PTU treatment may thus effectively counteract the risks of gestational hypertension and miscarriage. Likely due to the small sample size of this study, no fetal malformations were observed.
We found that TPOAb positivity was independently associated with low birth weight. A study including 7612 pregnant women has also previously shown that TPOAb positivity is associated with low birth weight. 32 In a systematic review, maternal TSH and fT4 concentrations were, respectively, reported to be negatively associated with birth weight, where fT4 concentrations were most strongly associated with birth weight during later pregnancy, and the association of TSH with birth weight was most apparent in TPOAb-positive women. 31 Further studies are needed to clarify the specific mechanism of the effect of thyroid autoimmune disorders on birth weight.
Our study has several limitations. First, there were some group differences, including BMI and smoking rates. Second, because of the subjective choice of GD patients to receive treatments or not, there may be some differences in the group characteristics that we cannot fully appreciate. Third, some women who lost to follow-up were not enrolled in the study, which may have resulted in some selection bias. Fourth, we did not measure fT3. Fifth, due to the limited sample size, this study was not powered to observe rare adverse effects of PTU. Larger scale prospective studies may be needed to overcome these limitations and to confirm our findings.
This study revealed differences in thyroid function measurements throughout pregnancy between patients. GTT patients exhibited few gestational and postpartum complications, except for GDM. Therefore, glucose testing and GDM education could be helpful to emphasize for GTT patients. Patients newly diagnosed with GD during early pregnancy were found to have an increased risk of adverse pregnancy outcomes, including premature delivery, gestational hypertension, and miscarriage.
PTU treatment appeared to be associated with better pregnancy outcomes in patients with GD, compared with no treatment. Moreover, we also demonstrated that positive TRAb and positive TPOAb of thyrotoxicosis in the first trimester were independently associated with adverse pregnancy outcomes. Large prospective studies are needed to confirm our findings.
Footnotes
Acknowledgments
We gratefully thank the women who participated in this study. For continuous support, assistance, and cooperation, we thank Weiwei Zhou (Shenyang Women's and Children's Hospital), Chenyang Li (Shenyang Women's and Children's Hospital), Bin Xu (No. 202 Hospital of People's Liberation Army), Lihua Bi (Dalian Obstetrics and Gynecology Hospital), Tao Meng (The First Hospital of China Medical University), Jianling Du (The First Affiliated Hospital of Dalian Medical University), Shaowei Zhang (202 Hospital of People's Liberation Army), Zhengnan Gao (Dalian Municipal Central Hospital Affiliated to Dalian Medical University), Xiaomei Zhang (The First Hospital of Dandong), and Liu Yang (Shenyang Women and Children Health Care Center).
Authors' Contributions
Yu.L. and Z.S. conceived and designed the study. Y.X., C.L., W.W., X.Y., A.L., and Y.S. performed the clinical follow-up. Yo.L., X.X., and J.L. contributed to the statistical analysis. Y.X. analyzed the results and composed the article. All authors read and approved the final article.
Author Disclosure Statement
The authors declare that they have no potential conflicts of interest.
Funding Information
This study was supported by the National Science and Technology Support Program (2014BAI06B02), National Natural Science Foundation of China (81170730, 81570709, 81700697, 82204025), Foundation of Key Laboratory in the Department of Education of Liaoning Province government in China (LZ2014035), Liaoning Science public research funds (2014001001/GY2014-A-001), and the Key Platform Foundation of Science and Technology for the universities in Liaoning Province (16010).
Supplementary Material
Supplementary Data