
Abstract
Background:
The incidence of differentiated thyroid cancer in Mainland China has increased rapidly in recent years, yet the number of studies focusing on health-related quality of life (HR-QOL) is still limited. Additionally, some of the quality-of-life (QOL) issues specific to thyroid cancer have not been adequately described. The aims of this study were to assess the generic and disease-specific HR-QOL of differentiated thyroid cancer survivors and to identify the associated factors.
Methods:
A cross-sectional survey including 373 patients was conducted in Mainland China. Participants completed the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30), the Thyroid Cancer-Specific Quality of Life Questionnaire (THYCA-QOL), and a questionnaire on patient demographics and clinical characteristics.
Results:
The QLQ-C30 global mean score was 73.12 (standard deviation [SD] = 11.95), while the THYCA-QOL summary mean score was 34.50 (SD = 12.68). The two QLQ-C30 functional subscales with the lowest scores were the social functioning and role functioning subscales. The five symptom subscales of the THYCA-QOL with the highest scores were the subscales regarding less interest in sex, problems with scar, psychological problems, voice problems, and sympathetic problems. Factors associated with worse global QOL on the QLQ-C30 included a shorter time since completing primary treatment (≤6 months), a history of lateral neck dissection, and a lower current thyrotropin (TSH) level (≤0.5 mIU/L). Higher cumulative activities of radioiodine (RAI; >100 mCi), gender (women), postoperative hypoparathyroidism, and a history of lateral neck dissection were associated with worse thyroid cancer-specific QOL. In contrast, higher monthly household income (>5000¥) and a history of minimally invasive thyroid surgery were associated with better thyroid cancer-specific QOL.
Conclusions:
Thyroid cancer patients experience multiple health-related problems and disease-specific symptoms after completing primary treatment. Patients with a duration ≤6 months from the completion of primary treatment, those with a history of lateral neck dissection, and a current TSH level ≤0.5 mIU/L may be more likely to have impaired generic QOL. More thyroid cancer-specific symptoms may be associated with higher cumulative activities of RAI, gender (women), postoperative hypoparathyroidism, a history of lateral neck dissection, lower monthly household income, and conventional surgery.
Introduction
The incidence of thyroid cancer in Mainland China has increased rapidly in recent years. According to the latest report from the National Cancer Center of China, 1 thyroid cancer has the fastest growing incidence among all cancer types, with an average annual increase of 20.6% during 2007–2016. It is estimated that 221,093 new cases of thyroid cancer occurred in China in 2020. 2 Differentiated thyroid cancer treatment generally involves surgery and, if indicated, radioiodine (RAI) ablation. With the efficacy of primary treatment, the prognosis is usually very good. 3 However, patients may experience complications or discomfort during or after treatments, such as changes in voice, changes in physical appearance, and employment disruption. These can negatively impact patients' physical, psychological, and social well-being, leading to decreased health-related quality of life (HR-QOL). HR-QOL has become an important consideration when assessing patients' subjective symptoms associated with the cancer itself or the effects of treatment. 4
The number of studies concerning the HR-QOL of thyroid cancer patients is increasing annually. 5 However, these existing studies have shown mixed results. The majority of these studies demonstrated impaired HR-QOL in thyroid cancer survivors compared with the reference population, whereas other studies reported a similar HR-QOL. 6 In the studies that have shown worse HR-QOL in thyroid cancer survivors, specific impaired aspects of quality of life (QOL) or its associated factors have also varied. The survey instruments that are currently used are mainly generic tools. 7 Some of the QOL issues specific to differentiated thyroid cancer have not been adequately described. Studies conducted in Mainland China have explored the HR-QOL of thyroid cancer survivors and the correlates defining HR-QOL, 8,9 yet the number of studies is limited. There is still an overall lack of literature on how thyroid cancer itself and its treatment impact patients' QOL, especially QOL issues that are specific to differentiated thyroid cancer patients in Mainland China. Further research with large samples using specific questionnaires in China is necessary.
Therefore, this study was designed to investigate the generic and disease-specific HR-QOL in a large sample of differentiated thyroid cancer survivors in Mainland China, using a generic tool combined with a thyroid cancer-specific QOL questionnaire, and to identify the sociodemographic and clinical factors that impair general HR-QOL and thyroid cancer-specific QOL.
Materials and Methods
Study design and participants
This study involved a one-time cross-sectional survey performed through an online thyroid cancer surveillance system, which stores the health information of patients who receive thyroid cancer treatment and provides information about thyroid cancer to patients registered at a university cancer center in China. Thyroid cancer patients who complete oncological treatment have been encouraged to register in the surveillance system since August 2019. We delivered the survey from August 17, 2021, to November 6, 2021, using convenience sampling. The inclusion criteria were as follows: an age ≥18 years; a diagnosis of differentiated thyroid cancer; the completion of thyroid cancer treatment; the ability to read and write; and the willingness to participate in this study.
Patients with other malignancies, distant metastasis, or cognitive disorders were excluded. The potential response rate was estimated according to a previous survey conducted in the same center among a different group of thyroid cancer patients with a response rate of 89.8%. 10 Eligible patients were invited to participate in the study and provided with a detailed explanation about the purpose of the study and an electronic link to a secure website. Patients who volunteered to participate in the study provided informed consent and completed the assessment via the electronic link online. Informed consent was obtained from each patient who participated in this survey. This study was approved by the Ethics Committee of Tianjin Medical University Cancer Institute and Hospital (No. bc2020152).
Measures
Patient demographic and clinical variables
A specific form was designed to collect patient demographic data as well as cancer-related information from patients, including gender, current age, monthly household income, and primary treatment. Clinical variables such as cancer stage, lateral neck dissection, and cumulative activities of RAI were collected from the surveillance system by two members of the research team with permission of the patient and the approval of the institutional ethics board. Data on the variables (e.g., primary treatment) provided by patients were verified by the two members. Postoperative hypoparathyroidism was defined as a low level of calcium and an inappropriately normal or low level of parathormone, or the need for active vitamin D and/or calcium treatment after thyroid cancer surgery. 11,12 Comorbidities diagnosed by a physician included the following diseases: hypertension, diabetes, previous stroke, asthma, or any other specific chronic disease.
HR-QOL questionnaires
General HR-QOL was assessed by the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30), which was developed as a general questionnaire for all patients with cancer 13 (Supplementary Text S1). The Chinese version of the EORTC QLQ-C30 was demonstrated to have good validity and reliability in Chinese cancer patients. 13
Thyroid cancer-specific QOL was assessed by the Thyroid Cancer-Specific Quality of Life Questionnaire (THYCA-QOL). 14 This instrument was developed to assess thyroid cancer-specific symptoms 14 (Supplementary Text S1). The Chinese version of the THYCA-QOL has been demonstrated to have satisfactory reliability and validity in combination with the EORTC QLQ-C30 for the assessment of QOL in Chinese thyroid cancer patients. 15
Statistical analyses
All statistical analyses were performed using SPSS version 22.0 (IBM Corporation, Armonk, NY), and a p value of <0.05 was considered to be statistically significant. Categorical variables are presented in the form of frequencies and percentages, while continuous variables are presented in the form of means ± standard deviations (SDs) or medians (25th–75th percentile). Patients with missing data were excluded from the statistical analyses. The effects of participant characteristics on the general QOL score of the EORTC QLQ-C30 and the THYCA-QOL summary score were examined using independent sample t tests and one-way analysis of variance with Bonferroni post hoc tests for normally distributed data. Variables with a p value <0.05 in univariate analysis were selected for the subsequent stepwise multivariable linear regression analysis to identify factors associated with worse HR-QOL. A variance inflation factor (VIF) of <5 was considered acceptable when identifying possible multicollinearity.
Results
Patient characteristics
A total of 425 thyroid cancer survivors were invited to participate in the survey (Fig. 1). Among these survivors, 29 refused to participate (93.2% response rate), 19 were excluded due to incomplete questionnaires or contradictory answers, and 4 were excluded for medullary thyroid cancer diagnoses, leaving 373 patients with valid data (valid rate = 94.20%). Reasons for not participating in the survey included a lack of interest in research and a lack of time. Patient characteristics are described in Table 1. The majority of participants were women (76.9%) and middle-aged adults (64.9%). The most common pathology in our sample was papillary cancer (95.7%). Of all participants, 47.5% (177) underwent total thyroidectomy and 38.3% (143) underwent lateral neck dissection. All patients underwent surgery, and RAI treatment was administered in addition to surgery in 25.7% (96) of the participants with cumulative activities of 80–430 mCi. Twenty-eight patients (7.5%) had postoperative hypoparathyroidism as defined for the study. The median and interquartile range for the time since primary treatment was 12 (5, 19) months.
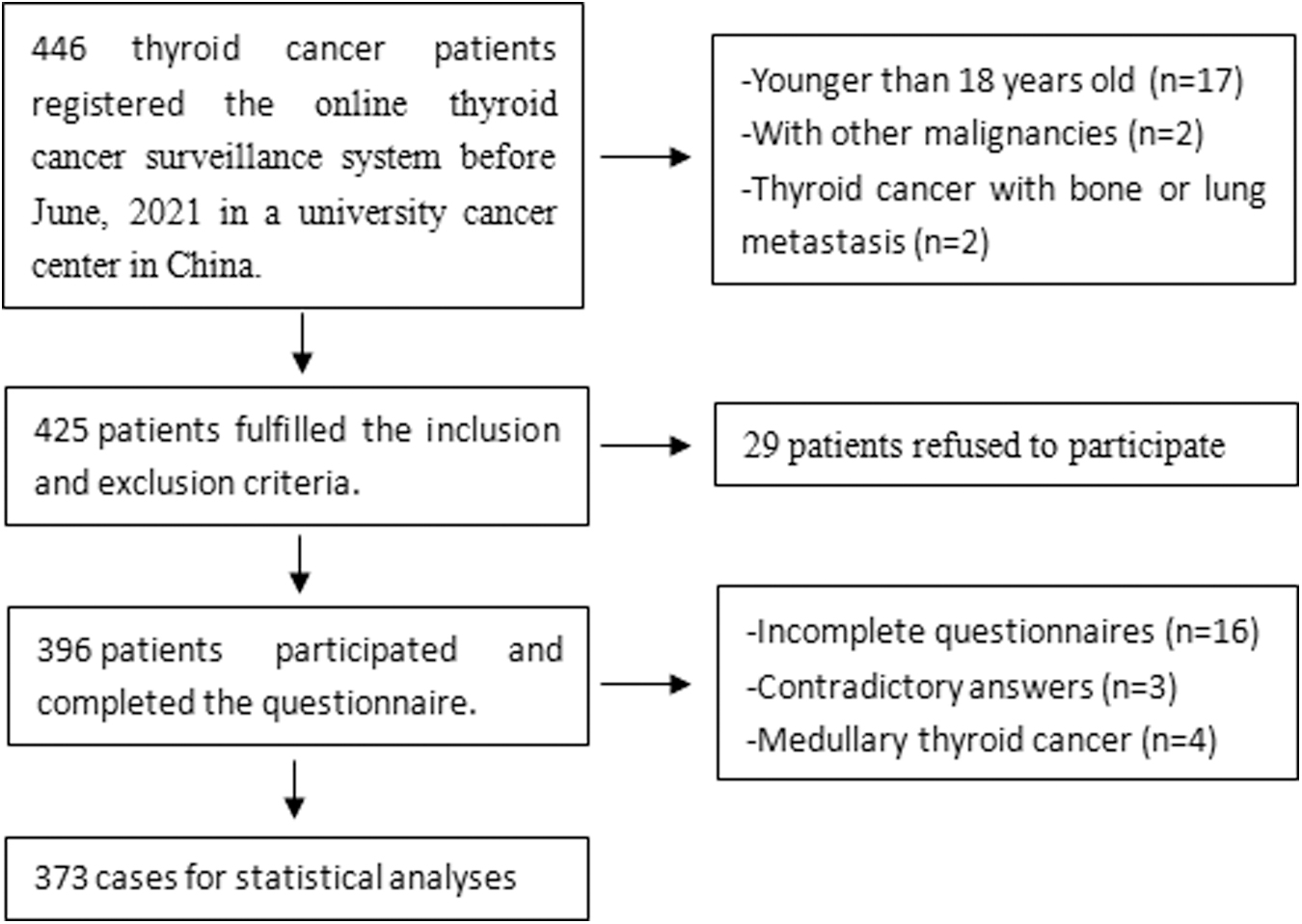
Flowchart of the data collection process.
Patient Characteristics
Minimally invasive surgery involves the removal of a thyroid tumor through a very small incision (e.g., endoscopic thyroidectomy and robotic thyroidectomy).
AJCC, American Joint Committee on Cancer; fT3, free triiodothyronine; fT4, free thyroxine; IQR, interquartile range; LT4, levothyroxine; RAI, radioiodine; SD, standard deviation; T3, triiodothyronine; T4, thyroxine; TSH, thyrotropin.
General HR-QOL
The general HR-QOL scores are presented in Table 2. The mean global QOL score of the EORTC QLQ-C30 was 73.12 (SD = 11.95). For the functional subscales, the two subscales with the lowest scores were the social functioning (mean: 69.17, SD = 19.70) and role functioning subscales (mean: 70.55, SD = 16.99). The three symptom subscales with the highest scores were the insomnia (mean: 36.91, SD = 28.80), financial difficulties (mean: 35.03, SD = 28.51), and fatigue subscales (mean: 34.61, SD = 18.24). When stratified by gender, men reported better emotional functioning, cognitive functioning and less insomnia, and constipation problems compared with women (Supplementary Table S1).
Summary Scores and Subscales Scores of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire and Thyroid Cancer-Specific Quality of Life Questionnaire
N = 373.
EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire; QOL, quality of life; THYCA-QOL, Thyroid Cancer-Specific Quality of Life Questionnaire.
The associations of global QOL with patient characteristics are shown in Table 3. Employment status, cancer stage, lateral neck dissection, the type of thyroidectomy, primary treatment, the use of RAI and its activities, current free triiodothyronine (fT3) level, current free thyroxine (fT4) level, current thyrotropin (TSH) level, thyroid cancer type, and the time since the completion of primary treatment were found to be significantly associated with the global QOL score (p < 0.05).
Associations Between Patient Characteristics and the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Global Scores and Thyroid Cancer-Specific Quality of Life Questionnaire Summary Scores
N = 373. Minimally invasive surgery involves the removal of a thyroid tumor through a very small incision (e.g., endoscopic thyroidectomy and robotic thyroidectomy).
Thyroid cancer-specific QOL
The thyroid cancer-specific QOL scores are reported in Table 2. The mean summary score of the THYCA-QOL was 34.50 (SD = 12.68). Less interest in sex (mean: 67.02, SD = 25.40), problems with scar (mean: 39.77, SD = 31.21), psychological problems (mean: 36.64, SD = 20.40), voice problems (mean: 35.03, SD = 23.63), and sympathetic problems (mean: 34.50, SD = 22.50) were the five subscales with the highest scores. When stratified by gender, men reported better total scores on the THYCA-QOL and less concentration, scar, chilly, headache, and sex problems compared with women (Supplementary Table S1). The associations of thyroid cancer-specific QOL with patient characteristics are shown in Table 3. Gender, educational level, employment status, monthly household income, cancer stage, lateral neck dissection, the type of thyroidectomy, primary treatment, postoperative hypoparathyroidism, the use of RAI and its activities, current TSH level, and the type of surgical procedure were found to be significantly associated with thyroid cancer-specific QOL (p < 0.05).
Multivariable analysis of factors associated with general HR-QOL
The results from multivariable stepwise analysis between global QOL and the selected statistical variables showed that patients with a duration of 6 months or less since the completion of primary treatment, lateral neck dissection, and a lower TSH level (≤0.5 mIU/L) had worse general HR-QOL (p < 0.05; Table 4). Together, these variables explained 41.8% of the variance in general HR-QOL. The VIFs ranged from1.029 to 1.339, indicating that multicollinearity was acceptable in this multivariable model.
Multivariable Linear Regression Analysis of Factors Associated with the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Quality of Life Score
R 2 = 0.426, adjusted R 2 = 0.418, F = 54.497, p = 0.000. N = 373.
CI, confidence interval; SE, standard error.
Multivariable analysis of factors associated with thyroid cancer-specific QOL
The results from multivariable stepwise analysis between thyroid cancer-specific QOL and the selected statistical variables showed that patients with higher cumulative activities of RAI (>100 mCi), women, postoperative hypoparathyroidism, and lateral neck dissection had worse thyroid cancer-specific QOL, while patients with a higher monthly household income (>5000¥) and those who underwent minimally invasive surgery had better thyroid cancer-specific QOL (p < 0.05; Table 5). Together, these variables explained 23.5% of the variance in thyroid cancer-specific QOL. The VIFs ranged from 1.012 to 2.036, indicating that multicollinearity was acceptable in this multivariable model.
Multivariable Linear Regression Analysis of Factors Associated with Thyroid Cancer-Specific Quality of Life Questionnaire Summary Score
R 2 = 0.256, adjusted R 2 = 0.235, F = 12.442, p = 0.000, N = 373. Minimally invasive surgery involves the removal of a thyroid tumor through a very small incision (e.g., endoscopic thyroidectomy and robotic thyroidectomy).
Discussion
This study examined general HR-QOL and thyroid cancer-specific QOL and relevant factors in Chinese patients who had undergone differentiated thyroid cancer treatments. To the best of our knowledge, this study represents one of a few studies that have assessed general and disease-specific QOL using a thyroid cancer-specific QOL questionnaire in patients with differentiated thyroid cancer in Mainland China. Herein, the results from this study revealed that patients experienced impaired general QOL after completing thyroid cancer treatment, which was in accordance with results reported in previous studies. 8,16
Among the 14 domains of the general HR-QOL scale, social functioning and role functioning were most affected, and insomnia, financial difficulties, and fatigue were the three most severe symptoms in the present study. Some of these domains have also been identified by the current literature as the worst aspects of general HR-QOL. 8,17,18 Insomnia and fatigue are the most common symptoms among thyroid cancer patients across cultures. 17,19,20 In addition, our study also identified financial burden as one of the most severe symptoms in thyroid cancer patients, which was in line with the report by a study that specifically focused on financial burden among thyroid cancer survivors. 21
With further multivariable analysis, a shorter time since completing primary treatment (≤6 months), lateral neck dissection, and a lower current TSH level (≤0.5 mIU/L) were found to be significantly associated with decreased general HR-QOL. Studies have shown that better HR-QOL is associated with a follow-up duration of more than 1 or 2 years. 22,23 However, in this study, patients with more than 6 months of time since the completion of primary treatment had already reported better general HR-QOL. Lubitz et al. 24 also reported that at 6 months after initial treatment, QOL was comparable to baseline in thyroid cancer patients. The difference may be caused by the different grouping methods according to the duration after primary treatment. Cancer patients usually perceive improved HR-QOL after months or years of recovery.
In our study, patients who underwent lateral neck dissection reported worse general QOL than patients who did not undergo lateral neck dissection. Similar findings were reported by Nickel et al. 25 and Wang et al. 8 Lateral neck dissection might affect QOL from multiple aspects, such as the major surgery itself, voice alteration, and shoulder stiffness after surgery. In addition, our study showed that patients with serum TSH level below 0.5 mIU/L reported worse HR-QOL, which was in line with previous research. 26 Adverse effects of thyrotoxicosis such as arrhythmia, anxiety, and insomnia increased significantly with lower TSH level, which might lead to worse HR-QOL. 26
In the present study, the mean THYCA-total score was 34.50 (SD = 12.68), which was lower than that reported by Chan et al., 17 indicating that patients in this study may have better thyroid cancer-specific QOL than those who were included in the study by Chan et al. Differences in the participants might be one possible explanation. In our study, 47.5% of the patients had undergone total thyroidectomy, while the proportion in Chan et al.'s study was 91.4%. Moreover, most participants (70.8%) in the study by Chan et al. had received RAI therapy, whereas the proportion in our study was 25.7%. Among the 13 domains, less interest in sex, problems with scar, psychological problems, voice problems, and sympathetic problems were the 5 most severe disease-specific symptoms in the present study.
An important finding was that the mean score of the less interest in sex domain was distinctly high in our study. Impaired sex life was also reported by a third of the patients in a study by Sawicka-Gutaj et al. 27 However, scores on this domain reported in other studies were relatively good. 17,28,29 Considering the conservative attitude toward sex in Mainland China and the natural decline in interest in sex as people age, our data could not clearly indicate that the diagnosis and treatment of thyroid cancer were the major reasons for the low interest in sex, and further research is needed. Sympathetic problems were also reported by Rogers et al. 30 and Husson et al. 31 as one of the most common symptoms in thyroid cancer patients. Recurrent injury to the laryngeal nerve is recognized as a common complication, and patients may experience voice change after thyroidectomy.
Regarding the factors associated with thyroid cancer-specific QOL, patients with a monthly household income of more than ¥5000 was associated with better thyroid cancer-specific QOL. Mongelli et al. 21 also reported that negative financial events were associated with poorer QOL. A study conducted by Yu et al. 32 investigated the economic burden among patients with inflammatory bowel disease in China and reported that nearly 98.0% (2954/3000) of the patients worried about their financial situation. 32 They also reported that, although 96.5% of the patients were covered by health insurance, the average reimbursement ratios were <50%. Although that study only focused on inflammatory bowel disease patients, it provided insight into the economic issues that Chinese patients might face.
In terms of the cumulative activities of RAI, patients who received activities higher than 200 mCi were reported to be at risk for poor QOL. 33 However, our results suggested that cumulative activities higher than 100 mCi could be associated with impairment in thyroid cancer-specific QOL. The use of RAI and its cumulative activities should be carefully individualized. We observed that women had worse thyroid cancer-specific QOL, which confirmed the findings of Rogers et al. 30 In this study, participants with postoperative hypoparathyroidism perceived worse thyroid cancer-specific QOL. Büttner et al. 16 also reported that thyroid cancer patients with hypoparathyroidism reported impaired QOL. Patients treated with lateral neck dissection reported higher thyroid cancer-specific symptoms, which was consistent with the report by Nickel et al. 25 Lateral neck dissection is a necessary treatment for those who have lymph node metastasis, which could possibly lead to more adverse effects and psychological concerns. We also observed that patients treated with minimally invasive surgery reported better disease-specific QOL compared with those treated with conventional surgery.
Limitations
Our study had several limitations. First, the present study was conducted in a single center, which may not represent the overall QOL of differentiated thyroid cancer patients in Mainland China. Second, most of our participants were in the early stage and were diagnosed with papillary cancer. Third, this was a one-time cross-sectional survey. Changes in QOL over time were not analyzed. Furthermore, as this was a convenience sample, the study may not have been adequately powered to fully explore all the reported variables in the multivariable analysis. There may also be selection bias, with respect to some of the surgeries that were offered (e.g., minimally invasive surgery). These limitations may contribute to bias. However, considering that the participants recruited from the institution came from a wide geographical area of China, our findings provide general insight into the current status of general QOL and thyroid cancer-specific QOL and their related factors in thyroid cancer patients from Mainland China. Further research is warranted to address these limitations in the future.
Conclusions
The present study indicated that differentiated thyroid cancer patients in Mainland China experienced impaired general and thyroid cancer-specific QOL. Patients with shorter time since completing primary treatment (≤6 months), a history of lateral neck dissection, and a lower TSH level (≤0.5 mIU/L) perceived worse general QOL. Higher cumulative activities of RAI (>100 mCi), gender (women), postoperative hypoparathyroidism, and a history of lateral neck dissection were associated with worse thyroid cancer-specific QOL, while a higher monthly household income (>5000¥) and minimally invasive surgery were associated with better thyroid cancer-specific QOL. Our findings have important implications for clinical care of thyroid cancer patients in China. Health professionals should be aware of the factors associated with QOL impairment and provide supportive care, with the intention of improving the general QOL and thyroid cancer-specific QOL of thyroid cancer survivors.
Footnotes
Authors' Contributions
C.C. contributed to conceptualization, investigation, formal analysis, writing—original draft, visualization, writing—review and editing, and project administration. J.C. took charge of conceptualization, investigation, and writing—review and editing. Y.W. was involved in conceptualization, investigation, data curation, and formal analysis. X.H. contributed to conceptualization, investigation, data curation, and writing—review and editing. Y.Z. was involved in conceptualization and investigation. S.Z. was in charge of conceptualization, supervision, writing—review and editing, and project administration.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was funded by Tianjin Key Medical Discipline (Specialty) Construction Project (No. TJYXZDXK-011A).
Supplementary Material
Supplementary Text S1
Supplementary Table S1