
Abstract
Background:
Premature infants are at higher risk of developing congenital hypothyroidism (CH) but the neonatal screening strategy for this population is still debatable. The purpose of this retrospective study is to describe the results of a screening program for CH in a preterm infant cohort.
Materials and Methods:
All preterm newborns who underwent neonatal screening in the Italian region of Piedmont in the period January 2019–December 2021, were included in this retrospective cohort study. The first thyrotropin (TSH) measurement was performed at 72 hours, whereas the second at 15 days of life. Infants with TSH >20 mUI/L at first detection and >6 mUI/L at second were recalled for a full evaluation of thyroid function.
Results:
During the study period, 5930 preterm newborns were screened. Based on birthweight (BW), the mean TSH was 2.08 ± 0.15 for BW <1000 g, 2.01 ± 0.02 for BW 1001–1500 g, 2.28 ± 0.03 for BW 1501–2499 g, and 2.41 ± 0.03 mUI/L in normal-weight newborns (p < 0.005) at the first detection, with a significant difference observed at the second measurement (p < 0.005). Based on gestational age, the mean TSH at first detection was 1.71 ± 0.09 mUI/L for extremely preterm babies and 1.87 ± 0.06, 1.94 ± 0.05, and 2.42 ± 0.02 mUI/L for very preterm, moderately, and late preterm infants (p < 0.005), respectively. Significant between-group differences of TSH measurements were also at the second and third detections (p < 0.005 and p = 0.01). The 99% reference range in this cohort overlapped with the recommended TSH cutoffs for screening recall (8 mUI/L for first detection and 6 mUI/L for second detection). CH incidence was 1:156. Of the 38 patients diagnosed with CH, a eutopic gland was present in 30 (87.9%), with CH transient in 29 (76.8%).
Conclusions:
We observed no significant difference in the recall rate between preterm and at term infants screened in this study. Our current screening strategy therefore appears effective in avoiding misdiagnosis. CH screening approaches vary among countries. Development and testing of a uniform multinational screening strategy is needed.
Introduction
Preterm birth is defined as delivery before 37 completed weeks of gestation. The consequent system immaturity involves the hypothalamus–hypophysis–peripheral endocrine glands axis, including the thyroid gland. 1,2 Thyroid hormones play an essential role in neuro-psychomotor development and growth, but are also known to have a significant role in cardiac and pulmonary maturation. 3
The pattern of postnatal thyroid function in preterm newborns differs from that of full-term infants, with the timing of the changes being different and slower, especially for very-low-birthweight (VLBW) infants (birthweight [BW] <1500 g) and extremely premature infants (23–27 weeks). 4 –7 In the latter, free thyroxine (fT4) levels decrease during the 1st week of life and then progressively increase. In infants born at 28–30 weeks, fT4 levels remain in a steady state in the 1st week and within the first 3–6 weeks of life reach the lower end of the reference range for full-term babies. Only in infants born at 30–35 weeks' gestation, fT4 increases during the 1st week, before decreasing again. Regarding thyrotropin (TSH), levels rise very slowly during the 1st week in extremely preterm infants and then gradually decrease until the 10th week. In very preterm infants (28–31 weeks of gestation), TSH levels decrease until the nadir in the first 4–5 weeks of life and then progressively increase. 2,8
Primary congenital hypothyroidism (CH) is the most common endocrine congenital disorder in children, presenting with elevated TSH and low/normal levels of fT4. CH can be classified into thyroid dysgenesis—athyreosis, ectopia, hypoplasia in situ, and dyshormonogenesis, in which there is a synthetic defect of thyroid hormones. 9 CH can also be classified as permanent or transient, almost all transient CH being associated with an in situ (eutopic) gland. 10 In recent years, the incidence of CH has increased due to many factors, such as the progressive lowering of the TSH detection cutoff in neonatal screening strategies and the increase in categories of newborns at risk of developing CH, such as small for gestational age (SGA) and preterm newborns. 11 –21 The latter category has a risk of developing CH compared with infants born at term due to multiple factors. Previous studies have shown that low birthweight (LBW), maternal thyroid disorders, pregnancy complications, genetic factors, drug use during the pregnancy, advanced maternal age, hypothalamus–pituitary–thyroid axis immaturity, and decreased liver-synthetized binding proteins are among the main factors associated with CH in this category. 22 –36
Many nonthyroidal disorders, such as respiratory distress syndrome and retinopathy of prematurity, which are very common in this category of infants, can also influence thyroid hormone synthesis and lead to false positive or false negative results in the newborn screening program. 37 –39
In addition to CH, preterm infants display other patterns of thyroid function tests (TFTs) that can be considered unique in this category. Transient hypothyroxinemia of the prematurity is a condition with low levels of thyroxine (T4) and fT4 and normal levels of TSH 1,2,40 –42 ; in this disorder, treatment is not currently recommended, unless an increase in TSH is also observed. Delayed TSH elevation is another characteristic pattern of preterm newborns, up to a maximum age of 56 days of life, with most cases showing a transient TSH elevation, especially when TSH levels are slightly elevated. 1,2
Most reports of neonatal screening programs show a higher incidence of CH in preterm infants. 2,43 –45 However, the reported incidence rates vary among studies, due to the heterogenous screening strategies with different TSH detection cutoffs, different timing in TSH detection, and different follow-up periods after referral to pediatric endocrinologists. Most newborn screening programs include a second detection at 2–4 weeks of age; in extremely preterm infants, many centers carry out a third detection at 6–8 weeks of age. These strategies enable detection of delayed TSH elevation but are associated with a higher risk of false positive testing, and higher costs. 46 –66
The purpose of this study is to describe the data from the screening program in preterm infants in the Italian Region of Piedmont with attention to the biochemical features of infants diagnosed with CH in this cohort.
Materials and Methods
All preterm newborns who underwent neonatal screening in the Piedmont region of Italy in the period January 2019–December 2021 were included in this retrospective cohort study. All TSH detection tests on dried blood spot (DBS) were performed at a single center, the regional reference center for Neonatal Screening at Regina Margherita Children's Hospital in Torino, Italy. All TSH blood spot detections were performed using the two-site immunofluorometric assay GSP© DELFIA Neonatal hTSH (normal range 9–18 mUI/L, coefficient of variability 10.6%). TSH, fT4, and free triiodothyronine (fT3) on blood were detected using DiaSorin Liaison©. Normal range at birth and at 2 years of age for fT4 was 9.2–24.4 and 9.2–18.6 pmol/L, respectively, whereas fT3 normal range were 3.37–9.98 and 3.37–6.91 pmol/L, respectively.
Infants with suspected central hypothyroidism due to lower-than-normal TSH levels, specific syndromes, or other diagnosed chromosomal abnormalities were excluded.
Demographic and clinical data were collected from the digital platform of the regional reference center for Neonatal Screening. Newborns were classified, according to gestational age, as extremely preterm (<28 weeks), very preterm (28 to <32 weeks), moderately preterm (32 to <34 weeks), and late preterm (34 to <37 weeks). Based on BW, the categories considered were extremely low birthweight (ELBW, BW <1000 g,), VLBW (BW 1000–1499 g), LBW (BW 1500–2500 g), and normal weight (BW >2500 g). Newborn infants were considered SGA when BW or length fell below the 10th percentile.
All the newborns performed the first TSH detection at 72 hours of age, the second at 15 days of age. In infants treated with drugs that interfere with TSH detection or fed with total parenteral nutrition, further measurements were performed every 15 days.
All infants with capillary TSH >20 mUI/L at the first detection and with TSH >6 mUI/L at the second were referred to the Department of Pediatric Endocrinology for a complete assessment of venous TFTs and clinical evaluation. Newborns displaying TSH values of 8–20 mUI/L after the first detection were recalled if the TSH was higher than 6 mUI/L at the second detection. From the third detection onward, the newborns were referred when the TSH was above 6 mUI/L.
CH was diagnosed when serum TSH levels were above 20 mUI/L and when serum TSH was 10–20 mUI/L with fT4 below the reference range and treatment with liquid formulation of L-T4 was promptly started. Newborns with mildly elevated TSH (5–20 mUI/L) and normal levels of fT4 underwent periodic follow-up until TFTs normalized or were considered to have CH after a persistent (>3 months) increase in TSH (>10 mUI/L) or when fT4 levels were below normal ranges. Newborns with hypothyroxinemia of prematurity were excluded.
Radiological assessment was initially performed with ultrasound evaluation 67 to determine the site and position of the thyroid gland. Dyshormonogenesis was diagnosed when a gland in situ was considered to be enlarged. Thyroid hypoplasia owing to dysgenesis was diagnosed if the gland was considered small. Thyroid volume was determined as the sum of each lobe using the prolate ellipsoid formula (length × width × depth × 0.52). 68 In case of absence of thyroid tissue on ultrasound imaging or uncertain reports, 99Tc-scintiscan was performed to confirm thyroid dysgenesis from ectopia or athyreosis.
The diagnostic re-evaluation was performed at 2 years of age, after 1 month of withdrawal of the previous therapy. Children with TSH >10 mUI/L or fT4 below normal were considered to have permanent CH, whereas children with TSH was 5–10 mUI/L and normal fT4 were classified as having persistent isolated hyperthyrotropinemia (transient CH).
The study was conducted according to the guidelines of the Declaration of Helsinki and received the approval of the City of Health and Science University Hospital of Turin Ethics Committee (number of approval 13899/A1). Parental informed consent was obtained in all cases.
We performed Student's t-test to compare means and the chi-square test to compare differences between groups. Statistical significance of differences was assumed if p < 0.05. The 95% confidence intervals (CIs) were reported. Statistical analyses and graphs were performed through GraphPad 7 software (GraphPad Software, La Jolla, CA).
Results
During the study period (Fig. 1), 5930 preterm newborns (2794 females and 3136 males) were screened. The mean gestational age was 34 ± 2.35 [CI: 34.2–34.3] weeks, and 190 (3.2%) subjects were born extremely preterm, 464 (7.8%) very preterm, 723 (12.2%) moderately preterm, and 4553 (76.8%) late preterm. The mean neonatal weight was 2302.6 ± 623 [CI 2287–2318] g, with 213 (3.6%) ELBW, 490 (6.9%) VLBW, 2922 (49.3%) LBW, and 2386 normal-weight newborns. Regarding gestational age and neonatal weight, 165 (2.8%) were SGA.
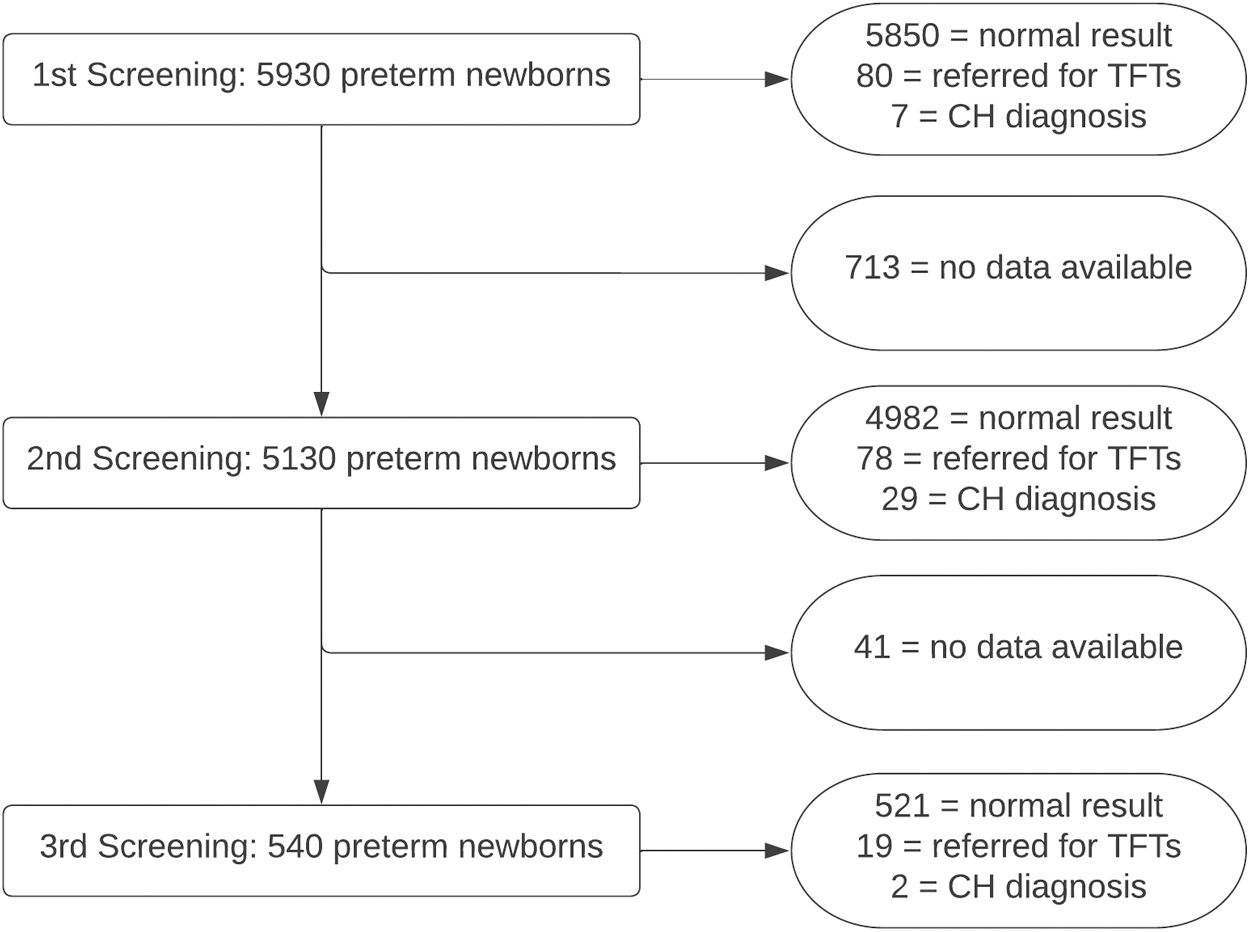
Participant flow diagram. CH, congenital hypothyroidism; TFTs, thyroid function tests.
Table 1 shows the mean TSH levels according to centiles in the whole cohort at first, second, and third detection. The first TSH detection was performed at 3.3 ± 1.45 [CI 3.2–3.47] days of life in 5930 infants, the second at 15 ± 1.4 [CI 14.9–15.2] days of life in 5130 subjects, and the third at 26.8 ± 15.4 [CI 25.5–28.1] days of life in 540 infants.
Mean (Standard Deviation) Capillary Thyrotropin Levels and Centiles at First, Second, and Third Detection in 5930 Preterm Infants Screened in the Piedmont Region of Italy During a 3-Year Period
TSH, thyrotropin.
The mean TSH level was 2.3 ± 0.02 [CI 2.3–2.5] mUI/L at the first detection, 1.77 ± 0.02 [CI 1.65–1.98] mUI/L at the second, and 1.56 ± 0.02 [CI 1.48–2.2] mUI/L at the third.
Figure 2 and Table 2 show the mean capillary TSH values according to BW category. The mean TSH at first detection was 2.08 ± 0.15 [CI 1.78–2.38] mUI/L in ELBW, 2.01 ± 0.08 [CI 1.86–2.18] mUI/L in VLBW, 2.28 ± 0.03 [CI 2.22–2.34] mUI/L in LBW, and 2.41 ± 0.03 [CI 2.31–2.45] mUI/L in normal-weight newborns (p < 0.005). At second detection the mean TSH level was 2.13 ± 0.11 [CI 1.86–2.36], 2.26 ± 0.23 [CI 1.79–2.72], 2.1 ± 0.04 [CI 2–2.19], and 1.62 ± 0.02 [CI 1.57–1.67] mUI/L, respectively (p < 0.005). No differences were observed between the different categories at third detection (2.07 ± 0.05 [CI 1.83–2.3], 2.2 ± 0.17 [CI 1.92–2.47], 2.07 ± 0.28 [CI 1.74–2.4], 1.62 ± 0.08 [CI 1.43–1.82] mUI/L, respectively).
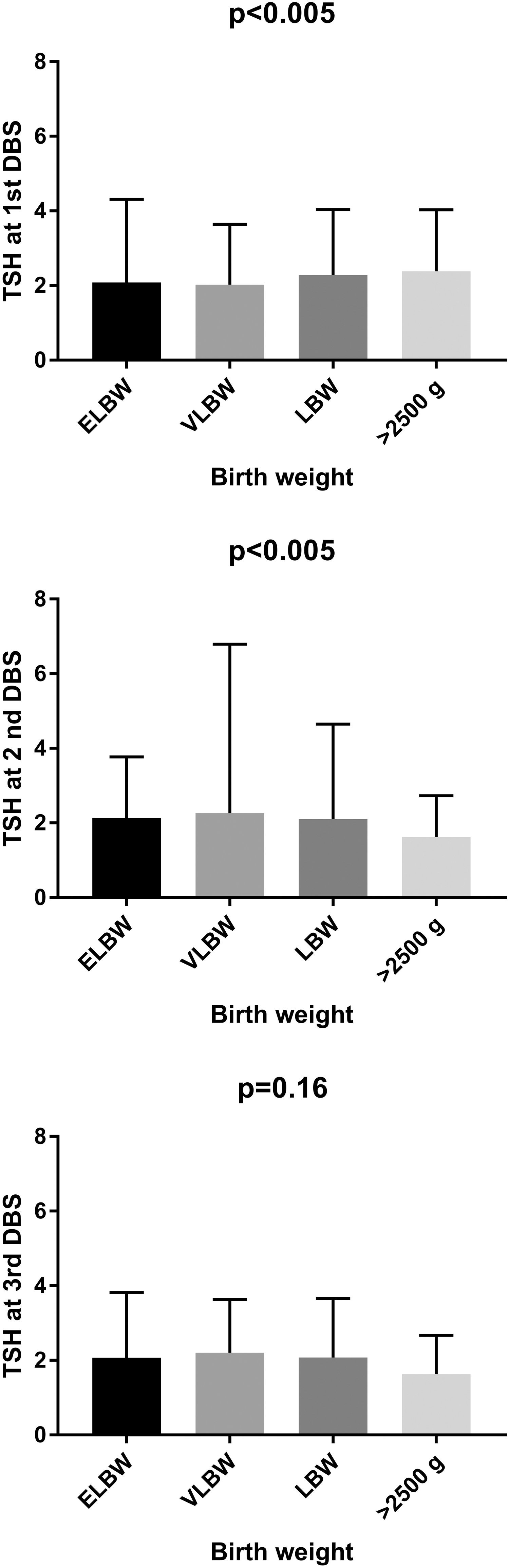
Box and whisker SDs showing mean capillary TSH levels (mUI/L) according to birthweight in a cohort of preterm infants. DBS, dried blood spot; ELBW, extremely low birthweight; LBW, low birthweight; SDs, standard deviations; TSH, thyrotropin; VLBW, very low birthweight.
Capillary Thyrotropin Centiles According to Birthweight Categories in a Cohort of Preterm Infants
BW, birthweight; ELBW, extremely low birthweight; LBW, low birthweight; TSH, thyrotropin; VLBW, very low birthweight.
Figure 3 and Table 3 show the mean capillary TSH values according to gestational age. The mean TSH level at first detection was 1.71 ± 0.09 [CI 1.53–1.9] mUI/L for extremely preterm babies and 1.87 ± 0.06 [CI 1.73–2], 1.94 ± 0.05 [CI 1.83–2.1], and 2.42 ± 0.02 [CI 2.37–2.47] mUI/L for very, moderately, and late preterm infants, respectively (p < 0.005). A statistically significant difference was also observed at second and third detection (1.89 ± 0.11 [CI 1.67–2.12], 2.15 ± 0.21 [CI 1.72–2.58], 2.2 ± 0.16 [CI 1.88–2.52], 1.75 ± 0.02 [CI 1.71–1.79] mUI/L and 1.75 ± 0.14 [CI 1.46–2.03], 2.11 ± 0.13 [CI 1.84–2.38], 2.62 ± 0.24 [CI 2.14–3.1], 1.94 ± 0.14 [CI 1.66–2.21], respectively [p < 0.005 and p = 0.01]).
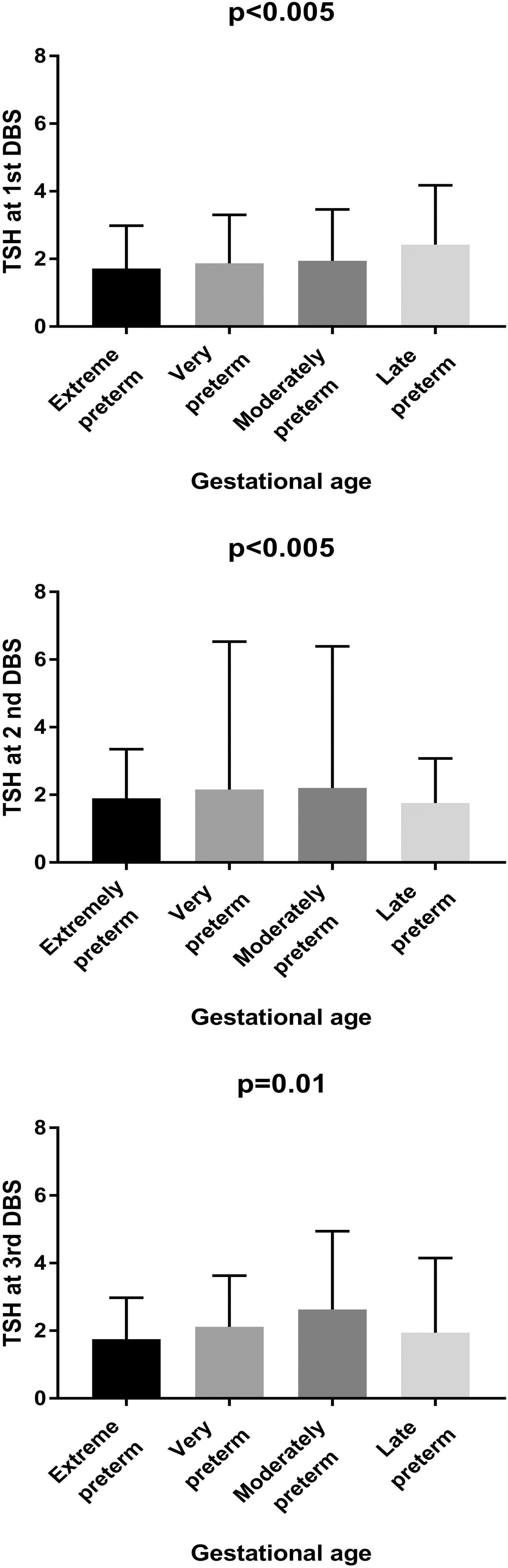
Box and whisker SDs showing mean capillary TSH levels (mUI/L) according to gestational age in a cohort of preterm infants.
Capillary Thyrotropin Centiles According to Gestational Age in a Cohort of Preterm Infants
At first detection 5850 (98.7%) newborns displayed normal capillary TSH, while 80 subjects were referred for venous TSH and fT4 measurement of whom 7 were diagnosed with CH. At the second detection, 4982 newborns showed normal TSH (97.1%), whereas 78 infants were referred for a full TFT evaluation and 29 of them had diagnosis of CH. At the third detection, 521 (96.5%) newborns had a normal TSH level, 19 were referred for TSTs, and 2 of them received diagnosis of CH. Sensitivity and specificity of the first detection were 81.6 and 99.5%, 100% and 97.1% at the second detection, respectively.
The incidence of CH in the studied cohort was 1:156 (38/5930). Based on BW, the incidence of CH was 1:71, 1:102, 1:112, and 1:477 for ELBW, VLBW, LBW, and newborns with BW >2500 g, respectively. Considering the gestational age, the incidence was 1:190 for extremely preterm newborns and 1:58, 1:103, and 1:207 for very, moderately, and late preterm infants, respectively.
Of the 38 patients diagnosed with CH, eutopic gland was found in 34 (89.5%) subjects, with dyshormonogenesis (enlarged gland) in 5 newborns, thyroid hypoplasia in 4 subjects, and normal-size gland in 25 subjects. Athyreosis was diagnosed in 2 subjects and thyroid ectopia in another two. Transient CH was present in 29 of the 38 (76.8%) cases of whom all had eutopic thyroid with dyshormonogenesis in one case and thyroid hypoplasia in 4 subjects.
All newborns with final diagnosis after first detection had TSH levels above 20 mUI/L. Of the 29 infants diagnosed after second detection, 15 had normal TSH at first detection, 14 had levels of 8 to 20 mUI/L, whereas all had TSH >20 mUI/L at second detection. The 2 newborns diagnosed after third detection had normal results at first detection and a slight increase in TSH at second detection (17 and 21 mUI/L, respectively). Both should have been referred after the second screening, but in this case a decision was made for further detection.
Discussion
Preterm newborns exhibit a unique pattern in TFTs compared with full-term infants, 1,2 including changes in TSH within normal stabilization of thyroid function.
BW is considered the main factor that can influence postnatal change in TSH. 1,2,65 In our study, we observed a significant difference in TSH level at first and second detection between the different categories. Percentiles based on BW showed a 99th percentile of TSH above the cutoff used in our neonatal screening center for referral to second and third detection (Table 2), demonstrating that where BW is concerned, no further targeted strategies appear necessary.
Gestational age has also been described as critical for postnatal TSH changes. Significant differences were observed between extremely preterm, very preterm, moderately preterm, and late preterm infants in all detections. The earlier the delivery occurred, the earlier was the increase in TSH (Table 3) confirming current literature data. 1,2,4,22,62,63 Analyzing the percentiles based on gestational age, we observed that it is not necessary to change the current TSH cutoff based on the time of delivery. Sensitivity and specificity at first detection were 81.6 and 99.5%, and 100% and 97.1% at the second detection, respectively.
A total of 38 infants (0.64%) were diagnosed with CH, mostly at the second detection of TSH, as described in previous studies. The referral rate after the first and second detection was similar to a previous work. 18 The incidence rates of CH reported in the literature are very heterogeneous, owing to the differences in neonatal screening strategies between centers 24 and the combining of infants with permanent and transient CH. In a previous Italian study from the Lombardy region, the reported incidence was 1:142, which is very similar to that observed in the present study. 18 We also found a similarly high rate of in situ thyroid gland among preterm newborns diagnosed with CH (89.5%). This latter finding may explain the high number of patients with transient CH (76.8%).
The strengths of this study are the large size of the cohort and the consistent management, as all TSH detections were analyzed by the same neonatal screening center and the referral was conducted at the same pediatric endocrinology department. The major limitations of the work are the retrospective nature of the data and the lack of comprehensive clinical information, as the data were collected from the neonatal screening center's digital platform. Another limitation is that no data were available from 713 preterm infants, who needed to be excluded from the study (Fig. 1).
The key question is, what is the best screening strategy for preterm infants? The optimal capillary TSH cutoff required to trigger referral for venous TFTs is unresolved. Furthermore, it remains unclear whether the third detection at 30 days of life is required for all preterm infants. Some authors recommend lowering the TSH cutoff and using gestational age-specific cutoffs. 6,24,46 –50 The need to lower the cutoff below 20 mUI/L, to avoid missing the diagnosis, is beyond dispute. A cutoff of 10 mUI/L will improve the sensitivity, whereas lower cutoffs than this will increase the false positive rate. 51
Cutoff levels of 10–12 mUI/L have been reported to reduce false negative rate of cases and the diagnosis of CH in unsuspected case. 17 A cutoff of 6 mUI/L was considered to be sufficient for one-test strategy, without the risk of missing any diagnosis. 24,52 –54 Other authors reported a higher risk of false positive using the 6 mUI/L cutoff, while some diagnoses were missed, and pointed out that the delayed TSH increase is an essential factor for retesting. 47 In view of this, a widely recommended approach includes retesting, which can lead to the diagnosis of CH in the missed cases after the first detection. However, the timing of the second test is not universally agreed and ranges from the second to 4th week of life, 24,51,54 –57 although some authors have reported that preterm infants achieve the same pattern of TFTs as full-term infants at 4–6 weeks of life. 24,58,59 Hashemipour et al. after a systematic review of the literature recommend performing the second screening at 2 weeks of life. 24 The screening strategy in our center includes the use of the same cutoff for preterm and full-term infants.
The referral cutoff after the first detection is above 20 mUI/L, whereas infants with TSH between 8 and 20 mUI/L undergo a recall for the second detection. To summarize, we recommend initial screen at 48–72 hours and using a cutoff TSH of 8 mU/L, a second screening at 2 weeks of life regardless of the first test result using a cutoff TSH of 6 mUI/L. In this study, we did not observe significant difference in the recall rate between preterm and full-term infants. The false positive rate after the first detection was 1.37% for preterm infants and 1% for full-term infants. After the second detection, the rate was 0.98% and 0.7%, respectively. Our current screening strategy also appears to avoid also missed diagnosis, as the only two diagnoses detected at the third analysis on DBS, should have been referred to the pediatric endocrinology center after the second detection on DBS. The observed incidence of CH in this study was similar to that reported in another Italian study conducted in the Region of Lombardy, thus confirming that the double screening program with different cutoffs at first and second detections seems to be an efficient screening strategy.
In conclusion, prompt thyroid hormone replacement of CH is mandatory due to the pivotal role of the thyroid in neural maturation and growth. Neonatal screening strategies and clinical management in case of altered TFTs need to be more uniform. International multicenter studies are needed to determine the best screening strategy in the growing population of fragile infants, particularly preterm newborns.
Footnotes
Authors' Contributions
G.T. contributed to the study design, statistical analysis, writing of the first article draft and clinical management of all referred newborns. J.M. contributed to the data collection, literature check, and clinical management of all referred newborns. K.T. contributed to the data collection and literature check. E.P. contributed to the data collection and management of all screened newborns. L.d.S. contributed to the study design and revision of the final version of the article.
Author Disclosure Statement
All authors have nothing to disclose.
Funding Information
No funding was received for this article.