
Abstract
Background:
Thyroid cancer (TC) is one of the most common carcinomas in young women. Concerns have been raised regarding the impact of the disease and its treatment on reproductive function. The aim of the study was to investigate the association of TC diagnosis and radioactive iodine (RAI) treatment on infertility and pregnancy rates in women.
Methods:
The comprehensive computerized database of a health management organization in Israel was screened for all female patients who were diagnosed with TC at age ≤40 years in 2000–2020. Rates of infertility (based on a documented diagnosis or purchase of fertility medications in the patient files) and pregnancy were compared with healthy age-matched controls.
Results:
The cohort included 1164 patients with TC (median age at diagnosis 31.6 years; interquartile range [IQR]: 26.7–35.4) and 5030 controls, followed for a median period of 10 years (IQR: 5.0–15.0). The infertility rate was higher in the TC group than in the control group (23.9% vs. 20.4%, p = 0.008). Still, the postdiagnosis/referent date pregnancy rates were comparable in the whole cohort (46.9/47.7%, p = 0.625) and across all age quartiles. The median time to the first pregnancy postdiagnosis/referent date was longer in TC patients than in controls (37 vs. 31 months, p < 0.001). Within the TC group, women who received repeated radioactive iodine treatment (n = 611, 52.5%) had comparable rates of infertility and pregnancy as those who did not. However, their time to the first postdiagnosis pregnancy was longer (median 45 vs. 29 months, p = 0.020).
Conclusions:
Our study provides reassuring evidence about the reproductive characteristics of women treated for TC. Pregnancy rates in TC survivors were comparable with controls. However, a higher infertility rate and a longer time to conceive were observed in the TC group compared with the control group. These findings were consistent in women who received single or repeated RAI treatments.
Introduction
Thyroid cancer (TC) is one of the most common carcinomas diagnosed in female adolescents and young adults (AYAs), and its incidence has been rising rapidly over the past three decades. 1 –3 Surgery is the standard treatment for TC, and it may be followed by a single or repeated radioactive iodine (RAI) administration in selected patients. 4 Compared with the general population of patients with cancer, the 15- to 39-year age group is unique in terms of both the biology of their disease and the possible psychosocial impact of cancer diagnosis. 1,2,5 As this age range encompasses most of the reproductive lifespan of women, concerns have been raised regarding the impact of the diagnosis and treatment of TC on fertility.
A few population-based studies investigated the long-term effects of TC on female fertility by comparing the pregnancy/birth rate in patients with the expected rate in the general population or matched controls. 6 –8 Most reported a lower pregnancy rate in TC survivors. These findings were supported by population-based studies of the impact of various types of cancer on postdiagnosis fertility rates in AYA patients. 8 Others focused on the impact of RAI treatment in TC on different aspects of reproductive function. 9 –14 A recent meta-analysis of the effects of RAI therapy on ovarian function and fertility showed no clear association between RAI and a long-term decrease in pregnancy rate in patients with differentiated TC. 15 However, the results across studies were inconsistent, and there were no data reported on the impact of repeated RAI administration.
The aim of this study was to investigate the association of a diagnosis of TC, and RAI treatment, on infertility and pregnancy rates in a large cohort of female AYA patients in Israel.
Methods
Design and setting
A retrospective cohort study was performed using the anonymized data of ∼1.4 million residents of two districts in central Israel who were medically insured by Clalit Health Services (CHS), the largest publicly funded health management organization (HMO) in Israel. Membership in one of the four HMOs in Israel is obligatory by law. Surgical and nonsurgical treatment for TC patients is covered by the HMOs, as well as laboratory and imaging tests. In addition, medications prescribed for female infertility are covered by the HMO until the age of 45 years. CHS has a comprehensive centralized data warehouse that aggregates clinical and administrative input from health service providers, physicians, laboratories, and pharmacies and can be queried down to the level of an individual member. Data for this study were extracted from the database using the CHS sharing platform powered by MDClone.
Ethical approval
The study was approved by the Rabin Medical Center institutional ethics committee (approval no. RMC 0403–12) and the need for consent was waived owing to the retrospective retrieval of anonymized data.
Participants
The CHS database was searched for all women diagnosed with TC between January 2000 and January 2020 without restricting for specific histology. Those who were aged ≤40 years at diagnosis and ≥25 years at the time of data collection (January 2021) were identified. The control group consisted of women randomly selected from the same database who matched the study population for age (based on calendar year of birth), had no documentation of a thyroid abnormality or use of thyroid medications, and had at least one normal thyrotropin (TSH) measurement during the study period. Each patient was matched to four controls, each of whom was assigned a “referent date” that corresponded to the date of the matched survivor's TC diagnosis.
Patients and controls with a documented prior nonthyroid malignancy and/or hysterectomy before the age of 45 years were excluded from the analysis. Figure 1 provides the participant flow chart.
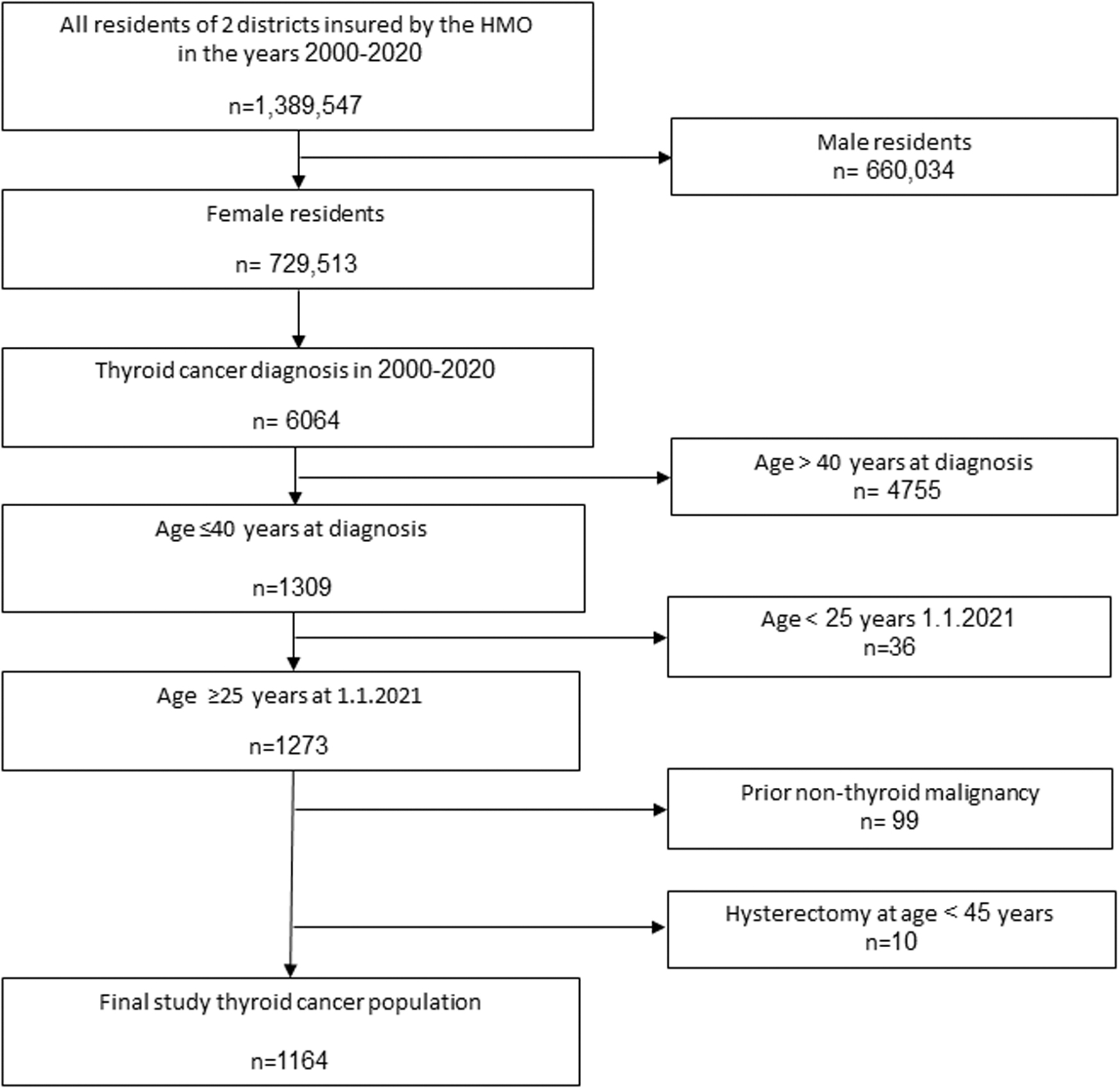
Participant flow chart.
Data retrieval
The data retrieved from the computerized files for each patient with TC included: date of TC diagnosis, serum TSH levels at diagnosis and thereafter, purchase of levothyroxine after TC diagnosis, and dates of RAI administration. The data retrieved for the healthy control group included repeated serum TSH levels. For all study participants, the files were reviewed for: date of birth, country of birth, socioeconomic score (SES) according to the Israeli Bureau of Statistics, body mass index (BMI) at TC diagnosis/referent date, documentation of infertility and pregnancies before and after the time of TC diagnosis/referent date, oral contraceptive use/number of purchases per participant after diagnosis/referent date (served as an indirect indicator of pregnancy intent owing to a lack of information on women's will to conceive).
Determination of infertility
The presence of infertility and the time of its diagnosis were determined based on infertility diagnosis documentation in patient files and documented purchase of medications used solely for infertility treatment. The two events were examined and compared across groups, both individually and as a combined variable (documented diagnosis and/or fertility drugs). Cases with a documented male infertility diagnosis were excluded from the infertility rate analysis.
Determination of pregnancy
Pregnancy was determined based on documentation of obstetric ultrasound, pregnancy 50-g oral glucose tolerance test (OGTT), and delivery at a CHS hospital in one of the two study districts. The three events were analyzed and compared across groups, both individually and as a single combined variable indicating pregnancy (imaging and/or OGTT and/or delivery at CHS hospital). Time to first-ever pregnancy following TC diagnosis was calculated as the time between the date of diagnosis of TC, and the recorded date of the event(s) used to identify pregnancy. The time from TC diagnosis to the first event indicating pregnancy was also calculated.
Statistical analysis
Data were analyzed using IBM SPSS Statistics for Windows v27 (IBM Corp., Armonk, NY). Data are expressed as median (interquartile range [IQR]) for continuous skewed variables, or number (percent) for categorical variables.
For the comparison between TC patients and the age-matched healthy controls, we used the Mann–Whitney test (for skewed variables) or Pearson's χ 2 test (for categorical variables). Comparisons of infertility and pregnancy rates between female TC patients and healthy controls were performed for the entire cohort, as well as stratified to age quartiles.
For the comparisons of infertility and pregnancy rates between TC patients with/without RAI treatment and between patients with repeated RAI versus no RAI treatment, which were not age matched, we used both nonage-adjusted comparisons (Pearson's χ 2 test or Mann–Whitney test) as well as age-adjusted comparisons (logistic regression analysis for infertility and pregnancy rates, or general linear model analysis for time to infertility and pregnancy).
A linear regression analysis (forward) was performed to predict time to first pregnancy (TTP) using the following variables: TC diagnosis and RAI treatment (three categories: control, TC no RAI, TC with RAI), age at diagnosis/referent date, BMI, and TSH level at diagnosis/referent date, and use of levothyroxine.
Results
The study included 1164 patients with TC who met the inclusion criteria and 5030 age-matched controls without thyroid pathology.
Baseline characteristics
Median age was 31.6 years (IQR: 26.7–35.4) at diagnosis and median follow-up time was 10 years (IQR: 5–10) (Table 1). There were no between-group `differences in basal TSH level, rate of prior diagnosis and/or treatment of infertility, and rate of prior pregnancy.
Baseline Characteristics of Thyroid Cancer Patients and Controls at Diagnosis/Referent Date
BMI, body mass index; IQR, interquartile range; SES, socioeconomic score (1—lower class, 2—middle class, 3—upper class); TC, thyroid cancer; TSH, thyrotropin.
SES differences between TC patients and controls were found to be statistically significant. However, most of the women in both groups belonged to the middle class.
TC patients had a higher BMI than the age-matched controls.
Levothyroxine treatment and TSH levels after TC diagnosis/referent date
Following diagnosis, 799 of 1164 (68.6%) of TC patients started levothyroxine treatment (Table 2). Additional 246 purchased levothyroxine before TC diagnosis. The minimal and maximal TSH levels in the TC patients were 0.03 (IQR: 0.01–0.16) and 46.0 mIU/L (IQR: 6.8–114.8), respectively. The minimal TSH level was <0.5 mIU/L in 924 of 1164 (79.4%) patients, indicating a suppressive levothyroxine dose at that time. In the controls, all repeated TSH levels were within the normal range. There was no statistically significant difference in TSH levels at the time of infertility diagnosis/treatment between TC patients and controls; TSH levels in TC patients were significantly lower than in controls before the first post-TC pregnancy.
Clinical and Laboratory Findings Following Thyroid Cancer Diagnosis/Referent Date: a Comparison Between TC Patients and Controls
Documented diagnosis in the patient file and/or use of fertility drugs.
First imaging scan or first pregnancy OGTT or first documented birth.
IF, infertility; OGTT, oral glucose tolerance test; TC, thyroid cancer.
Use of oral contraception
The percentages of women who purchased oral contraception (OCP) and the median number of purchases per participant were comparable in both the TC patients and control groups: 559 of 1164 (48.1%) and 2311 of 5030 (45.9%), respectively, p = 0.24; 13 (IQR: 4–32) and 11 (IQR: 3–31), respectively, p = 0.286.
Infertility rate
The overall infertility rate was significantly higher in the TC cohort compared with controls (p = 0.008) (Table 2). The median age of TC patients and controls at the time of infertility diagnosis/treatment was similar.
The finding of a higher infertility rate in TC patients compared with controls was consistent in subgroup analyses that included only 799 of 1164 (68.6%) of TC survivors who started levothyroxine treatment after diagnosis (198/799, 24.8% of TC patients, vs. 1025/5030, 20.4% of controls, p = 0.005) and when comparing TC patients and controls after excluding women with prior infertility diagnosis or treatment (278/967, 28.7% of TC patients, vs. 1025/4192, 24.5% of controls, p = 0.006).
Pregnancy rate and TTP
The post-TC diagnosis/referent date pregnancy rate in TC patients and controls was 46.9/47.7% (Table 2). There was no significant between-group difference either when each event indicating pregnancy was analyzed separately (imaging scan, OGTT, delivery in a CHS hospital) or when the combined variable (any one of these events criteria) was used (p = 0.625).
The findings of a similar pregnancy rate in TC survivors compared with healthy controls remained consistent when only the 799 of 1164 TC survivors who started treatment with levothyroxine following diagnosis were included (47.5% of TC patients, vs. 48.5% of controls, p = 0.568); after excluding women with prior infertility from both the TC and control groups (47.5% of TC survivors vs. 48.5% of controls, p = 0.568); after excluding women who consumed OCP after the date of TC diagnosis/referent date (34.8% of TC survivors vs. 36.6% of controls, p = 0.402).
At their first pregnancy after diagnosis, TC survivors were older than controls (median 33.3 vs. 32.7 years, p = 0.021).
The TTP after TC diagnosis/referent date was significantly longer in TC patients than in controls (p < 0.001). Regression analysis showed that the only variables associated with a longer TTP were younger age at diagnosis/referent date (B = 3.8, SE = 0.1, p < 0.001) and TC with RAI treatment (B = 8.6, SE = 2.2, p < 0.001).
Nulliparous subgroups
Approximately 60% of participants in both groups had no prior pregnancy documentation at the time of TC diagnosis/referent date (Table 3). Like the findings for the whole cohort, the nulliparous TC patients had a subsequent higher rate of infertility diagnosis and/or treatment than controls, but there was no between-group difference in pregnancy rate.
Infertility and Pregnancy Rates of 3711 Nulliparous Participants Following Thyroid Cancer Diagnosis/Referent Date: a Comparison Between TC Patients and Controls
Documented diagnosis in patient file and/or use of fertility drugs.
First imaging scan or first pregnancy OGTT or first documented birth.
Infertility and pregnancy rates after diagnosis/referent date by age
At the time of diagnosis/referent date, TC patients and controls were divided into age quartiles (Fig. 2). Infertility rate was significantly higher in TC survivors than controls in the second quartile (26.8–31.6 years) and the fourth quartile (>35.7 years), and comparable in both groups in the first and third quartiles. In all age quartiles, no statistically significant difference was found in the pregnancy rate between TC patients and controls.

Rates of infertility and pregnancy after TC diagnosis/referent date in patients and healthy age-matched controls, divided by age quartiles. (
RAI treatment
RAI treatment was administered in a total of 611 of 1164 TC patients (52.5%) (Tables 4 and 5). As given in Table 4, RAI-treated patients were younger when diagnosed with TC than untreated patients. After adjusting for age, statistical analysis revealed no significant difference between the RAI-treated and untreated subgroups in postdiagnosis infertility or pregnancy rates. The median time to first pregnancy in patients treated with RAI was significantly longer than in patients who did not (45 vs. 29 months, p = 0.02).
Infertility and Pregnancy Rates of 1164 Thyroid Cancer Patients: a Comparison Between Repeated Radioactive Iodine–Treated and Non-RAI–Treated Patients
Documented diagnosis in the patient file and/or use of fertility drugs.
First imaging scan or first pregnancy OGTT or first documented birth.
RAI, radioactive iodine.
Infertility and Pregnancy Rates of Thyroid Cancer Patients: a Comparison Between Patients Who Received Repeated Radioactive Iodine Treatments Compared with No RAI Treatment
Documentation in the patient file and/or use of fertility drugs.
First imaging scan or first pregnancy OGTT or first documented birth.
Overall, 292 patients (25.1%) were repeatedly treated with RAI.
Infertility rates did not differ between this subgroup and the 553 patients who were not exposed to RAI (Table 5). Despite this, patients who received multiple treatments had a higher pregnancy rate. Patients who received repeated RAI treatments had a significantly longer time to their first postdiagnosis pregnancy (47 vs. 29 months, p = 0.002).
Discussion
This population-based study of female AYA patients in Israel demonstrated that, although the TC patients were more likely to be diagnosed with infertility and to use infertility therapies than healthy matched controls, the overall pregnancy rate was comparable between the two groups. RAI treatment, whether given once or repeatedly, was not significantly associated with fertility or pregnancy outcomes.
Infertility rate
The effects of TC on infertility have not been thoroughly investigated in population-based studies. Our finding of an increased infertility rate in patients with TC is in accordance with the Ontario Cancer Registry study of Velez et al., 5 including AYA survivors of the most common cancers and healthy controls matched for age and parity. Among the 5144 TC patients (35.9% of the whole cohort), the rate of infertility diagnosis was 12% versus 10.2% in controls (p < 0.001). As in our study, the association remained statistically significant on separate analysis of nulliparous women as well.
The underlying cause of the higher infertility rate among young TC survivors is unknown. The age of TC patients and control women at the time of infertility diagnosis/treatment was comparable. Furthermore, chemotherapy or other systemic treatments that may destroy reproductive cells are rarely administered to TC patients. Possibly, the increased risk of hypo/hyperthyroidism associated with the use of levothyroxine contributed to the higher rate of infertility. 16 Indeed, 70% of our TC patients began treatment with levothyroxine soon after being diagnosed, and their wide range of TSH levels represents periods of hypo/hyperthyroidism during follow-up.
Pregnancy rate
Despite the higher infertility rate and older age at the first pregnancy after the diagnosis in TC survivors, we found no difference in their likelihood of pregnancy compared with healthy controls (46.9% vs. 47.7%, p = 0.625). These results were maintained on separate analyses of TC and controls who were nulliparous at TC diagnosis. Accordingly, Baxter et al. 6 in a study of 890 TC survivors in Canada, found no difference in the cumulative 10-year childbirth rate between patients with TC and healthy age-matched controls (40.8% vs. 41.4%), overall or when stratified by parity. Anderson et al., 8 however, reported a lower overall pregnancy rate in TC survivors in Scotland between 1981 and 2012 than in the general population (SIR 0.79; 95% confidence interval [CI] 0.72–0.86), in addition to a decreased cumulative incidence of first pregnancy in nulliparous women (hazard ratio: 0.69; CI 0.59–0.81). Similarly, in a retrospective cohort study of 18,850 women with well-differentiated TC from California, Wu et al. 7 reported that overall and age-specific birth rates were lower in survivors than the contemporaneous US national birthrates, regardless of receipt of ablative RAI treatment.
It is noteworthy that patient–control comparisons of pregnancy rates in cohort studies can be influenced by cultural and social factors. The fertility rate in Israel exceeds that of other developed countries (2.9 children per woman in 2020), and it is the highest among the member countries of the Organization for Economic Cooperation and Development (OECD). 17
Infertility and pregnancy rates following RAI treatment
Our results demonstrated that treatment with RAI, administered to approximately half the patients with TC, had no effect on infertility and pregnancy rates. These findings are consistent with a recently published meta-analysis 15 and two large population-based studies 7,18 but contrast with another large study from Hong Kong. 19 Of note, the pregnancy rate in all these studies 7,18,19 was considerably lower than in this study. Different follow-up periods and outcome measures (live-birth vs. pregnancy rate) may have contributed to the observed variability, but it may also reflect Israel's exceptionally high pregnancy rate, as discussed previously.
Infertility and pregnancy rates following repeated RAI treatment
This study is, to the best of our knowledge, the largest population-based investigation to date of the effects of repeated RAI on pregnancy rate in female TC survivors. Patients given repeated RAI treatments (25.1% of the TC group) showed no difference in infertility rate and a higher pregnancy rate compared with patients who did not receive RAI (47.5% of the TC group). In the few small studies that looked into this factor, the cumulative RAI dose was also found to have no effect on lowering pregnancy rates or outcomes. 20 –23
Time to pregnancy
Time to first pregnancy after the TC diagnosis/referent date was significantly longer in patients than in healthy controls (37 vs. 31 months, p < 0.001), and consequently, TC patients were older at pregnancy than controls (33.3 vs. 32.7 years, p = 0.021). Contrary to a recent Chinese report we found no association between preconception TSH levels and increased TTP. 24 The difference in TTP appeared to be attributed to RAI. Indeed, the median TTP in patients who were not exposed to RAI was comparable (and even shorter) with that of healthy controls. This finding is consistent with previous reports of RAI-treated patients having longer TTP than untreated patients. 7,19
The difference in TTP in our cohort was greater than the 6–12 months recommended after RAI treatment. 4 It is possible that subjective factors played a role in TTP. In a recent study from The Netherlands on the effect of RAI therapy on ovarian reserve, Van Velsen et al. 14 reported that in 40% of the single-RAI treatment group and 33% of the multiple-RAI treatment group, the desire to have a child was influenced by the diagnosis or treatment.
The longer TTP should be taken into consideration in treatment decisions and fertility counseling, particularly in women with TC who are of advanced reproductive age.
Limitations and strengths
Our study has several limitations. First, some data may have been missed owing to the biases inherent in a retrospective design. Furthermore, data on the type of surgery, pathological features, and RAI doses were missing from the database. Second, there was no way to ascertain the criteria used for infertility diagnosis. Third, data on our patients' marital status was unavailable, therefore, we were unable to examine the relationship between TC diagnosis, marital status, and chances of postdiagnosis pregnancy. We also did not have access to the Israeli live-birth registry, so we analyzed pregnancy rates rather than birth rates. Finally, our findings may not be generalized to medically uninsured TC patients or those from other countries.
The study's strengths include the large number of female AYA patients with TC, the size of the age-adjusted control group, the analysis of infertility rates, and the availability of data on RAI treatment, including repeated administrations.
Conclusions
Our report provides reassuring evidence of a comparable chance to conceive between female AYA patients with TC and healthy age-matched controls. However, the findings of a higher rate of infertility, and a longer TTP in TC survivors highlight the need for tailored management and fertility counseling.
Footnotes
Acknowledgments
The authors thank Dr. Adi Turjeman from the Research Authority of Rabin Medical Center for her valuable help in the planning of the study and data retrieval.
Authors' Contributions
D.H.: conceptualization (lead); methodology (lead); writing—original draft (lead); writing—review, editing, and revising (lead). M.Y.-G.: conceptualization (lead); methodology (lead); formal analysis and interpretation of the data (lead); software (lead); writing—review, editing, and revising (equal). L.L.: conceptualization (lead); writing—original draft (lead); writing—review, editing, and revising (lead). All authors have read and agreed to the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.