
Abstract

F
Molecular testing (MT), such as ThyroSeqv3 (TSv3) and Afirma gene sequencing classifier, has become a valuable resource to further assess ITNs. 2 Regarding TSv3, higher-risk thyroid nodules are classified as “positive” due to the detection of specific mutations or molecular alterations. Contrarily, low-risk profiles are reported as either “negative” (ROM ∼3%), “currently negative” (ROM 5–10%) or “negative but limited” (ROM indeterminate).
Identifying those who will benefit most from MT is paramount for optimal patient care. Nonetheless, interpreting and translating MT results into patient management decisions can prove challenging for clinicians. Thus, this study's primary goal is to evaluate the number of patients undergoing surgery despite a benign result on TSv3 and to further assess the ROM of these nodules. A secondary outcome of this study is to assess whether or not the malignant nodules are aggressive by reviewing the postoperative histopathology findings.
The protocol for this retrospective study was reviewed and approved by the West-Central-Montreal and McGill University Health Center (MUHC) Research Ethics Boards (MP-05-2022-3173, MEO-05-2023-9079).
We obtained 837 TSv3 results from 820 consecutive patients aged 18 years old and over who were seen between 2018 and 2021 at the Jewish General Hospital and the MUHC, two tertiary care centers in Montreal, Canada. Nodules were selected for MT as a result of a shared decision made by the clinician and the patient. At these institutions, clinicians are encouraged to use the McGill algorithm 3 to assist with decision-making, but are not limited to it (Supplementary Methods). This algorithm recommends using MT for ITNs that would have otherwise been recommended for diagnostic surgery, namely those classified as Thyroid Imaging Reporting and Data Systems (TI-RADS) 4 and 5. FNA samples were collected by experienced thyroid specialists and were analyzed by board-certified pathologists with experience in cytological diagnostics. Samples were analyzed at the TSv3 commercial laboratory at the University of Pittsburgh Medical Center.
Nodules included in the analysis met the following criteria: TSv3 result being “negative,” “currently negative,” or “negative but limited,” being classified as Bethesda III or IV and measuring 1–4 cm (Fig. 1). All other nodules were excluded. Collected data included patient characteristics (age at time of FNA and sex) and nodule characteristics (size, laterality, and mutations).
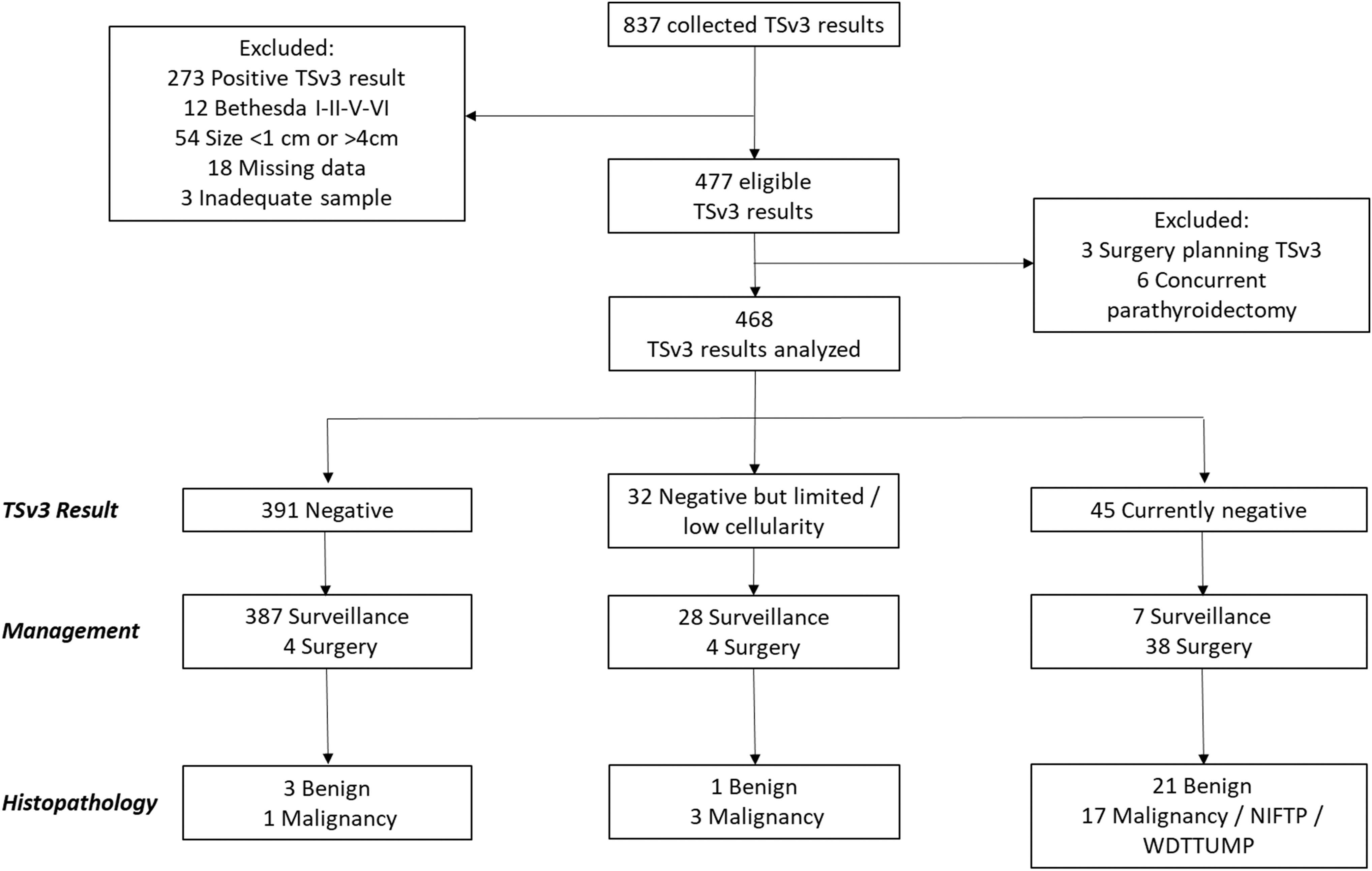
Classification of data. TSv3, ThyroSeq v3; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; WDTTUMP, well differentiated thyroid tumor of uncertain malignant potential.
Patients with thyroid nodules included in the study were then separated into two categories: those who underwent surgery and those who did not. Patients who had surgery near the thyroid bed for another reason (i.e., parathyroidectomy) or those who underwent TSv3 to plan the extent of surgery rather than to determine if surgery was necessary were excluded. Collected data included details of the surgery (date, reason, laterality, and type), postoperative histopathology, lymph node involvement, extrathyroidal extension, aggressive/invasive features, and treatment with radioactive iodine.
Nodules were further classified as benign or malignant according to histopathology results. Patients with incidental malignant findings (i.e., papillary microcarcinoma) in thyroid gland specimens that did not correspond to the tested nodule were not recorded as having malignant disease. For analysis purposes, we considered noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) or well-differentiated thyroid tumor of uncertain malignant potential (WDTTUMP) as malignant. 2
Descriptive statistics, including mean, standard deviation, confidence intervals (continuous variables), and percentages (categorical variables), were performed using nonparametric testing of Mann–Whitney U test. For frequency analysis in contingency tables, statistical analyses of associations between variables were performed using chi-square test or Fisher's exact test (with significance set at p < 0.05). Statistical analyses were performed using STATA® (STATA Corp., College Station, TX).
A total of 468 ITNs were included in the analysis (Supplementary Table S3). The mean age was 56.0 ± 13.7 years, and 386 patients (82.5%) were female (Table 1). Two hundred and fifty-seven nodules (54.9%) were located on the right, 200 nodules (42.7%) on the left and 11 (2.4%) on the isthmus. The mean nodule size was 1.95 ± 0.76 cm. Bethesda III nodules represented the majority of the cases (n = 344; 73.5%). Twenty-one patients had a TI-RADS 3 nodule (4.5%), 76 had a TI-RADS 4 nodule (16.2%), 45 had a TI-RADS 5 nodule (9.6%), and in 326 cases (69.7%), TI-RADS score was not documented. The average follow-up for patients was 23.0 ± 12.6 months.
Distribution of the Patient's Characteristics According to the Demographics, Nodule Characteristics, Clinical Management, and Test Performance
CI, confidence interval; FU, follow-up; min, minimum; max, maximum; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; SD, standard deviation; TI-RADS, Thyroid Imaging Reporting and Data Systems; WDTTUMP, well-differentiated thyroid tumor of uncertain malignant potential.
TSv3 reported 391 nodules as “negative,” of which 387 (99.0%) were managed with surveillance, while the remaining 4 (1.0%) underwent surgery (Table 1). Histopathology revealed that three nodules were benign and 1 (0.3%) had a follicular variant of papillary microcarcinoma (Supplementary Table S1). Of the 32 nodules classified as “negative but limited,” 28 (87.5%) were managed by surveillance while 4 (12.5%) underwent surgery.
Histopathology revealed one benign nodule and three malignant tumors (follicular variant of papillary carcinoma) (Supplementary Table S1). Of the 45 nodules classified as “currently negative,” 7 (15.6%) were managed with surveillance, whereas 38 (84.4%) underwent surgery. Histopathology revealed 21 benign tumors and 17 malignancies/NIFTP/WDTTUMP (Supplementary Table S1). None of the patients with a malignancy had extrathyroidal extension or lymph node metastasis. The most common reason for surgery, especially in the “currently negative” group, was patient concern about long-term surveillance.
In the “negative” group, 15% of nodules had mutations, the most common being TSHR (Supplementary Table S2). In the “currently negative” group, all the nodules presented with at least one mutation or molecular alteration, the most prevalent being EIF1AX of which 44% were malignant.
In this study, 84% of the 468 ITNs were classified as “negative” by TSv3. Of those patients, 99% were managed with surveillance and 0.3% of nodules were malignant. In the “negative but limited” group, 87.5% of patients were managed with surveillance and 9.4% of those nodules were malignant. Finally, in the “currently negative group,” 15.6% were managed by surveillance and 37.8% of nodules were malignant. Overall, one patient had aggressive cancer (poorly differentiated thyroid cancer, pT2N0). Of note, two of the patients managed conservatively presented with ultrasonographic changes during follow-up and underwent a repeat FNA with findings of Bethesda V. Malignancies were confirmed in both on postsurgical histopathology.
We obtained a ROM of 0.3% for nodules with a “negative” result, which is lower than that of 3% previously reported by Steward et al. 4 However, their study included nodules classified as Bethesda V as well as larger-sized nodules (average 2.42 cm) compared with ours (average 1.95 cm). Therefore, it is possible that the prevalence of cancer was lower in our study. Nonetheless, other studies calculated a negative predictive value (NPV) of 100% and 98.3% and the few malignancies reported were low-risk carcinoma. 5,6 These findings are consistent with those obtained in our study. Yet, not all nodules were resected in these two studies mentioned earlier as well as ours, so the true number of false negatives (FN) and NPV remain unknown.
For the “currently negative” group, the majority of patients (84.4%) underwent surgery due to a mutation identified by TSv3, despite the reported ROM of 5–10%. While most had benign nodules, 37.7% had a malignancy/NIFTP/WDTTUMP, which is higher than previously reported. 5,6 Of that number, nearly half were identified as NIFTP/WDTTUMP, hence we cannot exclude that different results may have been obtained by other institutions.
In this study, the mean follow-up is 23 months after TSv3 results, which compares with other studies where ITNs are followed after a benign result on MT. 7 –9 Some prospective studies have reported an FN rate of 1–6% after 12–27 months of follow-up. 8,9 Longer follow-up will be needed to establish an accurate FN rate.
Several limitations can be acknowledged from this study. First, we could not assess if patients underwent surgery at another institution. Also, TSv3 testing was not performed systematically on all ITNs; the decision was made by the clinician based on a comprehensive clinical picture and patient's preference. Thus, a selection bias may have been introduced toward lower-risk nodules since patients with a more worrisome clinical picture would have undergone surgery. Finally, TI-RADS 3-4-5 nodules were sent to MT. Recent data suggest that low-/intermediate-risk ITNs would benefit the most from MT compared with high-risk ITNs. 10 We cannot assess if this is also true in our population as the TI-RADS score is unavailable in numerous patients.
This study shows that the majority of patients with “negative” and “negative but limited” results on TSv3 opted for surveillance, whereas most of those with “currently negative” results underwent surgery. We found the ROM in the “negative” group to be lower than expected, and that of “currently negative” to be higher. Overall, one case of aggressive cancer was identified and belonged to the “currently negative” group. These findings highlight the need for more research, especially regarding nodules classified as “currently negative.” It is important to recognize the possibility of an FN and to follow ITNs with routine ultrasounds. Hence, we recommend that patients with “currently negative” and “negative but limited” results are followed more closely than those with “negative” results.
Footnotes
Authors' Contributions
Investigation (lead), formal analysis (equal), writing original draft (lead), and writing review and editing (lead) by E.C.-P. Formal analysis (equal), writing original draft (supporting), and writing review and editing (equal) by S.T. Writing review and editing (lead) by M.N. Database review and completion (equal), and writing review and editing (equal) by V.-I.F., M.A., M.P., K.R., M.P.H., and N.S. Formal analysis (lead), writing original draft (supporting), and writing review and editing (equal) by S.D.d.S. Conceptualization (lead), database review and completion (lead), writing original draft (equal), and writing review and editing (equal) by R.J.P.
Supplementary Material
Supplementary Methods
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3