
Abstract
Background:
Current guidelines suggest high-dose steroids as first-line treatment for dysthyroid optic neuropathy (DON). When steroids fail, decompressive surgery is mandatory.
Methods:
We conducted a single-center, retrospective cohort study in a tertiary care combined Thyroid-Eye clinic in Milan, Italy. We studied 88 orbits of 56 patients that were submitted to surgical orbital decompression to treat DON from 2005 to 2020. Of these, 33 orbits (37.5%) underwent surgery as first-line treatment for DON whereas the other 55 (62.5%) were decompressed after being unresponsive to very high-dose steroids. Previous orbital surgery, concurrent neurological or ophthalmologic diseases, or incomplete follow-up were considered as exclusion criteria from this study. Surgery was considered successful if no further decompression was needed to preserve vision. Pinhole best corrected visual acuity (p-BCVA), color sensitivity, automated visual field, pupil reflexes, optic disk and fundus appearance, exophtalmometry, and ocular motility were studied before and after surgery (1 week, 1, 3, 6, and 12 months). Activity of Graves' Orbitopathy (GO) was graded using a clinical activity score (CAS).
Results:
Surgery was successful in 77 orbits (87.5%). The remaining 11 orbits (12.5%) needed further surgery to treat DON definitively. All parameters of visual function improved significantly at follow-up and GO inactivated (CAS <3) within 1 month. At 3 months, all 77 responding orbits had p-BCVA >0.63 whereas all of the 11 non-responding orbits had p-BCVA ≤0.63. Visual field parameters and color sensitivity were not associated with response to surgery. High-dose steroid treatment before surgery was associated with a better response rate (96% vs. 73%; p = 0.004). Balanced decompression was associated with a higher response rate compared with medial wall decompression (96% vs. 80%; p = 0.04). A significant inverse correlation was observed between final p-BCVA and the patient's age (r = −0.42; p = 0.0003).
Conclusions:
Surgical decompression was found to be a very effective treatment for DON. In this study, all clinical parameters improved after surgery and further intervention was rarely needed.
Introduction
Dysthyroid optic neuropathy (DON) is a potentially sight-threatening complication of Graves' Orbitopathy (GO). It affects up to 3–5% of GO patients, 1 and its prevalence is calculated as 0.18 per 10,000 population. 2 It is principally caused by the compression of the optic nerve at the orbital apex due to increased orbital content, primarily inflamed and enlarged extraocular muscles. 3
Once DON is diagnosed, urgent treatment is required to prevent potential blindness. 4 The usual dosages of steroids used to treat moderate active GO are not expected to prevent DON, 5,6 except if associated with orbital radiotherapy. 7 The 2021 European Group on Graves' Orbitopathy (EUGOGO) guidelines and the 2022 Consensus Statement by the American Thyroid Association and the European Thyroid Association recommend to treat immediately DON with very high-dose steroids (500–1000 mg of methylprednisolone for 3 consecutive or alternate days, for 2 consecutive weeks, also called “medical decompression” regimen): if response to treatment is absent or poor, surgical orbital decompression is considered mandatory. 6,8
A wide range of surgical approaches have been proposed to treat DON. The transnasal-endoscopic surgery allows excellent access to the posterior and inferior medial wall of the orbit, without facial incisions. 9 The so called “balanced” decompression (medial wall, endoscopic or external, combined with external lateral wall) seems to reduce more proptosis and result in a lower risk of post-surgical diplopia. 10,11
To date, there is no consensus on the best surgical approach to treat DON or guidelines that define the outcomes of surgery. The aim of the present study was to assess the clinical and visual recovery after surgical orbital decompression to treat DON. We also planned to define the outcomes of surgery and identify the parameters associated with successful surgical intervention (at baseline or during follow-up).
Materials and Methods
We conducted a single-center retrospective cohort study in a tertiary care combined Thyroid-Eye clinic in Milan, Italy. The research complied with the Declaration of Helsinki (as revised in 2013). Approval was obtained from our Institutional Review Board (Milano 2), and the need for informed patient consent was waived (approval No. 605; July 27, 2020).
Patient inclusion and exclusion criteria
We included in this study patients submitted to orbital surgery to treat DON, only if they had both pre- and post-surgical ophthalmological examination (at least 6 months of follow-up). The exclusion criteria were previous orbital surgery for any reason or other ocular or neurological concurrent diseases with documented damage to the visual function. We also excluded patients presenting with moderate or severe keratopathy (punctate keratopathy, ulcers, abscesses, or leukomas).
The diagnosis of DON was based on the presence of one or more clinical signs, such as reduction of pinhole best corrected visual acuity (p-BCVA), loss of color vision, altered visual field, relative afferent pupillary defect (RAPD), or evidence of optic disc swelling, in the absence of other clinical explanation and associated with radiological evidence of GO. The diagnosis was always made at our combined Thyroid-Eye clinic, by the Ophthalmologist in agreement with the Endocrinology staff. This team also decided on the most suitable treatment for patients who were referred to the surgeon.
Ophthalmologic examination
Patients underwent complete ophthalmologic and orthoptic examination at each visit, according to the EUGOGO criteria. 12 The follow-up consisted of assessment at 1 week and at 1, 3, 6, and 12 months after surgery, as previously reported. 13 p-BCVA was noted as decimal at the time of the assessment and converted to logmar at the time of the analysis according to the formula: logmar = −log (decimal acuity). Despite both decimal and logmar values being analyzed in this study, p-BCVA is expressed in the paper as decimal notation, unless otherwise specified.
We used the Hardy-Rand-Rittler (HRR) pseudoisochromatic tables for acquired dyschromatopsia (HRR second edition; Richmond Products, Albuquerque, NM) for the evaluation of color perception. We recorded the number of errors in the six screening tables (5–10) for each eye. We performed automated perimetry with the Humphrey field analyzer (HFA; Humphrey Instruments, Inc., San Leandro, CA). We used the Swedish Interactive Threshold Algorithm Fast Test (30-2 SITA Fast) with a Goldmann size III stimulus on a dim background (31.5 apostilb, foveal threshold set on).
Patients were provided near correction and rest breaks, if needed during visual field testing. Unreliable visual fields examinations (fixation losses more than 20%, false positive and false negative more than 33%) were repeated twice, and the test with the best reliability was included in the study. The visual field indices mean deviation (MD), Pattern Standard Deviation (PSD), and Fovea Threshold were evaluated. The severity of abnormal visual field was classified as follows: severe (MD < −16 dB), moderate (−16 dB ≤ MD ≤ −6 dB), and mild (MD > −6 dB).
We assessed orbital inflammation for each orbit with the clinical activity score (CAS). 14 For the purpose of this study the CAS was calculated on 7 points. The disease was considered active if CAS ≥3/7.
Orbital surgery
All interventions were performed by the same experienced orbital surgeon (C.G., 20 years of experience in orbital surgery). Until the end of 2017, due to the surgeon's preference, DON patients were generally treated with the balanced two-wall decompression. Since 2018, due to time optimization of the operating rooms in our Institution, most DON patients have been treated with urgent medial wall decompression, followed by lateral wall decompression only at a later stage if deemed necessary for unsatisfactory visual recovery.
Medial orbital wall decompression was performed by transnasal endoscopic surgery, consisting of antero-posterior ethmoidectomy, medial antrotomy, and sphenoidectomy. The medial portion of the optic canal (about 2–3 mm) was removed and the periorbit incised, allowing orbital content prolapse. Lateral orbital wall was approached through an upper eyelid crease incision (lateral third). The periosteum of the frontal, zygomatic, and sphenoid was isolated. The bones were drilled until the temporal muscle and the dura mater of the medial and anterior cranial fossa were exposed.
After surgery, all patients were administered intravenous dexamethazone (0.07 mg/kg twice a day for 2 days), together with antibiotics and ocular lubricants.
Study outcomes
We defined orbital surgical decompression as being successful when no further surgery was needed to treat residual or relapsing visual impairment due to DON and this was the primary study outcome. Secondary outcomes included: p-BCVA, visual field indices (MD, PSD, Fovea Threshold) and color sensitivity, optic disk appearance, RAPD, CAS, exophthalmos, ocular pressure, and extraocular motility.
Statistical analysis
All data were reported as mean ± standard deviation or with confidence interval (CI) for the mean or as median with range or CI for the median, as appropriate. The D'Agostino Pearson test was used to verify the normal distribution of all continuous variables. To test for differences in parametric or nonparametric variables, we used one way analysis of variance (ANOVA) or Kruskal-Wallis test, respectively. Variables with a non-normal distribution were analyzed with the Mann-Whitney test. Differences in categorical data were tested using the χ 2 -test.
Repeated-measures ANOVA for parametric variables or Friedman test for nonparametric variables with Bonferroni correction were used for repeated multiple comparisons. Correlations of nonparametric and parametric variables were evaluated by conducting Spearman's or Pearson's analyses, respectively. Receiver Operating Characteristic (ROC) curve analyses were applied to all visual and clinical parameters. The minimum alpha criterion for tests of statistical significance was p < 0.05. The statistical analyses were performed using MedCalc statistical software for Windows (version 9.5.0.0; MedCalc Software, Mariakerke, Belgium).
Results
Study population
We examined the records of 67 consecutive eligible patients, for a total of 102 orbits, all submitted to surgical orbital decompression to treat DON at our Institution from 2005 to 2020. Out of the 102 eligible orbits, 10 were excluded because of incomplete follow-up (<6 months) and 4 for the presence of other pathologies affecting the visual capacity (1 for a corneal abscess, 2 for macular degeneration, and 1 for a dense cataract). Eighty-eight orbits of 56 patients were eventually included in the study and analyzed (Fig. 1).
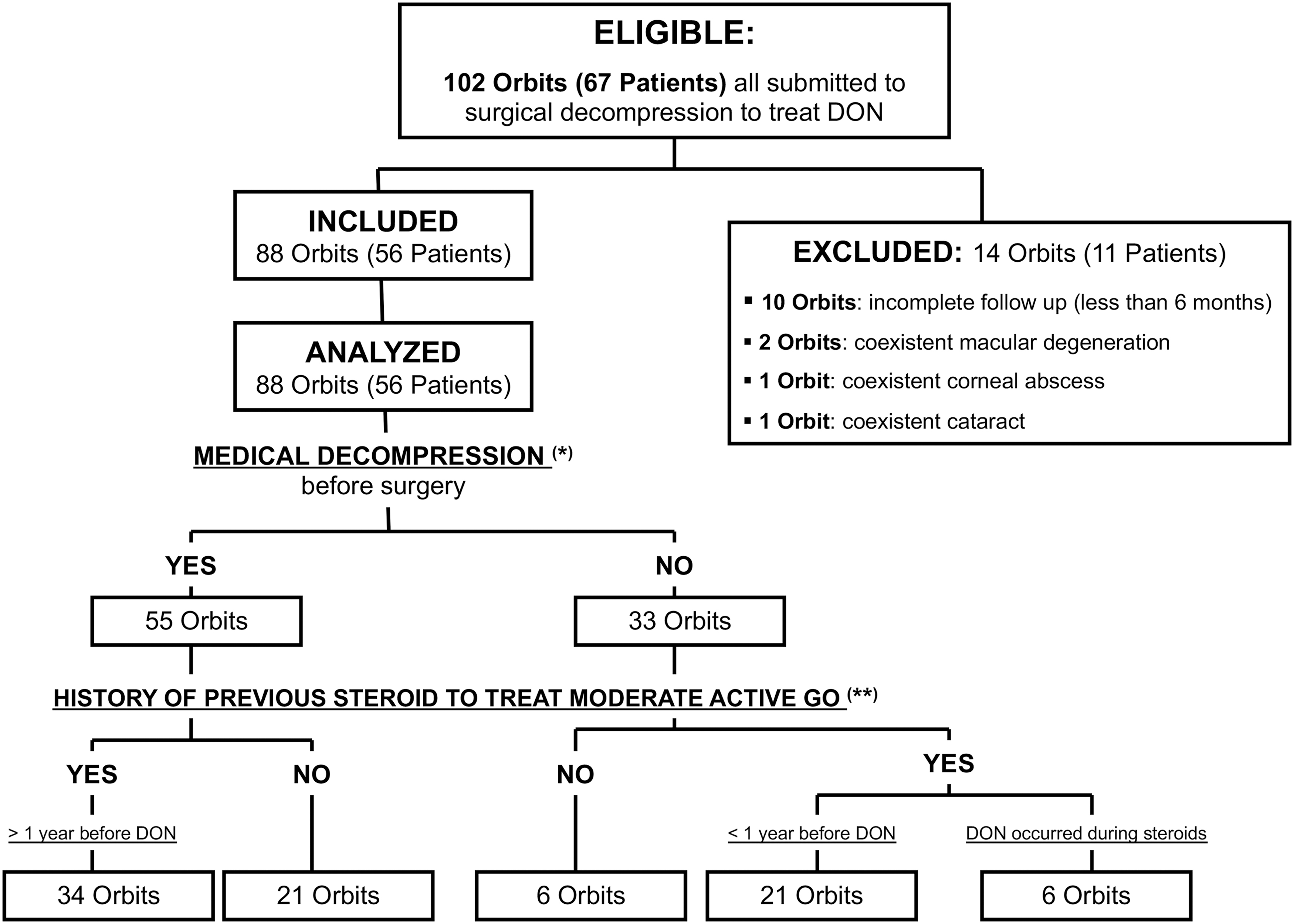
Participant flow diagram. (*)500–1000 mg of methylprednisolone for 3 consecutive days, for 2 consecutive weeks (cumulative dose: 3–6 g). (**)4.5–7.5 g of methylprednisolone divided into 12 weekly infusions.
Patients were 38–83 years of age (mean 60 ± 11 years). Twenty of them (36%) were male, and 36 (64%) were female; 27 (48%) were smokers (12 ± 7 cigarettes a day, range 2–25), 11 (20%) were ex-smokers (mean time since stopped: 9 years, range 1 month to 25 years), and 18 (32%) never smoked. Twenty-four patients had unilateral DON, 28 had bilateral DON, and 4 had bilateral asynchronous DON (3 years, 2 years, 6 months, and 4 months, respectively between onset in the two fellow eyes).
Fifty-two patients had Graves' disease, two Hashimoto's thyroiditis, one primary idiopathic myxedema, and one euthyroid GO. At the time of decompression, 22 patients were hyperthyroid on thionamides, 6 hypothyroid, and 28 were euthyroid (5 without treatment, 10 on methimazole, and 13 on levothyroxine [LT4]). In their past history, 11 patients were treated with radioiodine, 9 with total thyroidectomy, and 2 were submitted to both treatments, all before the onset of the active phase of GO, many even before the onset of GO.
The mean thyroid and orbital disease duration (determined as the time elapsed from the initial diagnosis of thyroid and orbital disease to the date of surgical decompression) was 40 ± 75 months (CI for the mean: 24–56 months, range 2–360 months) and 16 ± 39 months (CI: 7–24 months; range 1–348 months), respectively.
Seven patients had type 2 diabetes, well controlled with insulin (five patients) or oral therapy (two patients). Eleven patients had systemic hypertension, one had hypertensive cardiopathy, one atrial fibrillation, one ischemic cardiomyopathy, and one systemic lupus erythematosus.
DON characteristics at baseline
All the 88 orbits included in the study were assessed before surgery. After surgery, 86 orbits (98%) were assessed at 1 week, 85 (97%) at 1 month, 84 (95%) at 3 months, 81 (92%) at 6 months, and 79 (90%) at 1 year.
At baseline, the great majority of patients had concurrently abnormal p-BCVA, visual field, and color perception. Computed tomography (CT) imaging showed enlarged extraocular muscles with signs of apical crowding in all 88 orbits and also optic nerve stretching in 8 orbits (9%).
Pinhole BCVA was decreased in 83 eyes (94%). The mean pre-operative p-BCVA was 0.55 ± 0.27 (ranging from counting fingers to 1.0; CI: 0.49–0.60). The baseline p-BCVA of orbits unresponsive to surgery was significantly worse compared with that of responsive orbits (Table 1).
Baseline Clinical Parameters of the Orbits Affected with Dysthyroid Optic Neuropathy Submitted to Surgical Decompression
Surgery was considered successful when no further intervention was needed to treat DON definitively.
MD, PSD and Fovea Threshold are parameters measured by the automated visual field. Color sensitivity was measured by the HRR test for acquired color vision defects: this table shows the number of errors registered in the six screening tables of the test. Variables with significant differences are shown in bold.
p-Values: one-way ANOVA.
p-Values: Chi-square test.
500 or 1000 mg of intravenous methylprednisolone for 3 consecutive days for 2 consecutive weeks to treat DON before surgery.
Values are expressed as mean ± standard deviation or confidence interval for the meand or as median with confidence interval for the mediane or as number of events observed.
p-Values: Mann-Whitney test.
p-Values: Kruskal-Wallis test.
ANOVA, analysis of variance; CAS, clinical activity score; DON, dysthyroid optic neuropathy; GD, Graves' disease; GO, Graves' orbitopathy; HRR, Hardy-Rand-Rittler; MD, mean deviation; p-BCVA, pinhole best corrected visual acuity; PSD, pattern standard deviation; RAPD, relative afferent pupillary defect; TRAb, thyrotropin receptor antibodies.
The visual field was abnormal in 86 eyes (98%), ranging from normal (2 eyes, 2%) to severe depression (9 eyes, 10%). Thirty-seven eyes (42%) had moderate depression, 35 eyes (40%) showed mild defects, whereas in 5 eyes (6%) visual field testing was not feasible because of the severely impaired visual acuity. Mean values of MD, PSD, and Fovea Threshold at baseline are shown in Table 1. Dyschromatopsia was detected in 82 (93%) eyes. The median number of errors at the screening tables of the HRR was 3 (range 0–6, CI: 3–4) (Table 1).
RAPD was found at baseline in 28 (32%) eyes (Table 1), optic disk swelling in 24 (27%), and choroidal folds in 18 (20%) with no significant differences between responsive and not responsive orbits.
Therapeutic intervention
Of the 88 orbits studied, 33 (38%) underwent surgery as first-line treatment for DON whereas the other 55 orbits (62%) after unsuccessful “medical decompression.” In both groups, a non-negligible number of patients had been exposed to steroids to treat moderate active GO in their past history. When this treatment occurred more than 1 year before the diagnosis of DON, patients underwent “medical decompression” before surgery. Otherwise, they were referred directly to the surgeon (Fig. 1).
Table 2 shows differences between orbits submitted or not to “medical decompression” before surgery. Forty-three orbits (49%) underwent medial wall decompression, whereas 45 orbits (51%) underwent balanced two-wall decompression. Balanced decompression resulted in a better outcome (no need for further surgery) when compared with medial wall decompression (response rate: 96% vs. 80%, p = 0.04, Table 1).
Baseline Clinical Parameters of the Orbits Affected with Dysthyroid Optic Neuropathy Submitted to Surgical Decompression as First-Line Treatment or After Unsuccessful “Medical Decompression” (500 or 1000 mg of Intravenous Methylprednisolone for 3 Consecutive Days for 2 Consecutive Weeks)
MD (Mean Deviation), PSD (Pattern Standard Deviation) and Fovea Threshold are parameters measured by the automated visual field. Color sensitivity was measured by the HRR test for acquired color vision defects: this table shows the number of errors registered in the six screening tables of the test. Variables with significant differences are shown in bold.
p-Values: one-way ANOVA.
p-Values: Chi-square test.
Values are expressed mean ± standard deviation or confidence interval for the meanc or as median with confidence interval for the median dor as number of events observed.
p-Values: Mann-Whitney test.
p-Values: Kruskal-Wallis test.
When analyzing in detail p-BCVA, visual field indices, or color sensitivity, no significant differences were found during the entire follow-up between orbits subjected to balanced or medial wall decompression (not shown). At 1 year, p-BCVA was 0.86 ± 0.14 in patients who underwent medial wall decompression and 0.85 ± 0.19 in patients who underwent balanced decompression (p = 0.79).
Surgical complications were rarely observed and were mostly mild (five patients with limited mild nosebleed and six patients with mild periocular or maxillary paresthesia). Only in one case a rhinoliquorrhea was observed, which was successfully treated intraoperatively with a multilayer fistula plasty.
Study outcomes
Seventy-seven orbits (87.5%) responded to surgical decompression and did not need further surgery. Eleven orbits (12.5%) did not respond to surgery, as functional parameters transiently improved at 1 week but deteriorated afterward (Fig. 2). The diagnosis of persistent DON after surgery was made generally at 3 months, and additional surgery was performed within 3 months thereafter (mean time: 1 month; CI 0–2 months).

Changes of p-BCVA after surgical orbital decompression (up to 1 year of follow-up). The visual outcome (±SE) of orbits responding to surgery (pinhole BCVA >0.63 at 3 months) is shown with empty circles and a continuous line, whereas that of unresponsive orbits is shown with solid triangles and a dashed line. *p < 0.05 vs. not responding eyes. p-BCVA, Pinhole best corrected visual acuity; SE, standard error.
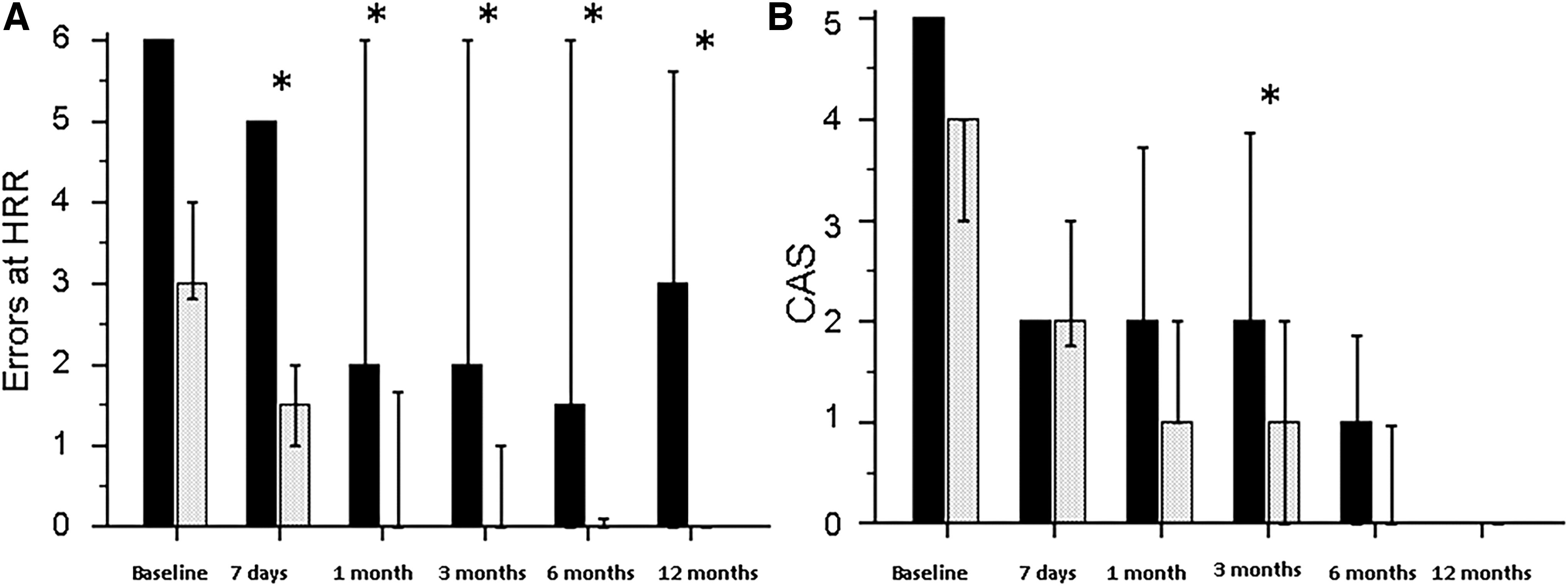
Based on these findings, the visual outcome at 3 months was designated as the primary end point of this study. At that time, three parameters were statistically different between responding and not responding orbits: p-BCVA (mean: 0.87 ± 0.13 vs. 0.44 ± 0.19, p < 0.001, Fig. 2), MD of the visual field (mean: −2.93 ± 3.74 vs. −5.95 ± 3.58, p = 0.007, not shown), and number of errors at HRR (median: 0 [CI: 0–1] vs. 2 [CI: 1–6], p = 0.01, Fig. 3A).
(
At 3 months, all 77 responding orbits had p-BCVA >0.63 whereas all the 11 not responding orbits had p-BCVA ≤0.63. In contrast, MD and HRR values were more dispersed and were not significantly associated with response to surgery. The ROC curve analysis applied to p-BCVA at 3 months resulted in an area under the curve (AUC) of 0.993 (CI: 0.978–1.000; p < 0.0001), with the highest Youden index at a cutoff of >0.63 (100% sensitivity and 88.9% specificity).
This result was also confirmed by converting p-BCVA values from decimal to logmar notation (AUC: 1.00; p < 0.0001; cut off: <0.20 logmar [ = 0.63 decimal]; 100% sensitivity and 100% specificity). Therefore, p-BCVA >0.63 (or <0.20 logmar) at 3 months was considered the primary visual outcome of this study.
Changes of visual function parameters after surgery
Overall improvement of visual parameters was significant compared with baseline (Table 3). After surgery, the group of responding orbits achieved normal or near normal p-BCVA that was significantly higher than that of unresponsive orbits during the entire follow-up (Fig. 2). At 12 months, p-BCVA was higher in patients who were treated with “medical decompression” before surgery (0.89 ± 0.11 vs. 0.82 ± 0.20; p = 0.04; not shown) whereas no difference was observed whether orbits were submitted to one or two wall decompression (0.86 ± 0.14 vs 0.85 ± 0.19; p = 0.79; not shown).
Overall Changes of Clinical Parameters After Orbital Decompression
Color sensitivity was measured by the HRR test for acquired color vision defects: this table shows the number of errors registered in the six screening tables of the test. MD (Mean Deviation), PSD (Pattern Standard Deviation) and Fovea Threshold are parameters measured by the automated visual field.
p-Values: repeated-measures ANOVA.
Values are expressed mean ± standard deviation or as median with confidence interval for the median or as number of events observed, as appropriate.
p-Values: Friedman test.
p-Values: Chi-square test.
The number of errors at HRR significantly decreased after surgery (Table 3: p < 0.001), being significantly higher in non-responders during the entire follow-up (Fig. 3A). MD, PSD, and fovea threshold significantly improved after surgery (Table 3: p = 0.04, p = 0.02 and p = 0.002, respectively). The MD was significantly worse in unresponsive orbits at one (−6.09 ± vs. −2.10 ± dB; p = 0.04, not shown) and 3 months (−4.55 ± vs. −1.90 ± dB; p = 0.007, not shown) after surgery.
Optic disk swelling, RAPD, and choroidal folds
Optic disk swelling completely resolved in 23 out of 24 eyes affected within 1 month and in 1 eye within 3 months. RAPD completely resolved within 1 year in all but 4 of the 28 eyes affected. At 12 months, 7 of the 18 orbits had persistent choroidal folds.
Orbital inflammation
The median CAS at baseline was 4/7 (CI: 3–4; range 0–7), not different whether patients were treated or not with “medical decompression” (Table 2). Most of the orbits (68 orbits, 77.3%) had CAS >3/7 at baseline.
The CAS score was rapidly reduced after surgery in responsive and not responsive orbits. The median CAS decreased from 4/7 to 2/7 within 1 week. At 1 month, only 7 orbits (8%) had a CAS still >3/7 and thus were treated with weekly infusions of intravenous steroids, until inactivation. Of these, four were from the group of orbits submitted primarily to surgery, and the other three from the group pre-treated with “medical decompression” (p = 0.53). At 3 months, all orbits had inactive GO (CAS <3/7) but unresponsive orbits had significantly higher CAS scores (Fig. 3B).
Proptosis and intraocular pressure
Proptosis and intraocular pressure significantly decreased after orbital decompression (Table 3: p < 0.001), with no significant differences in responsive or unresponsive orbits or in patients treated or not with steroids before surgery. Exophthalmometry readings were significantly higher in unresponsive orbits at baseline (Table 1) and thereafter (Fig. 4).
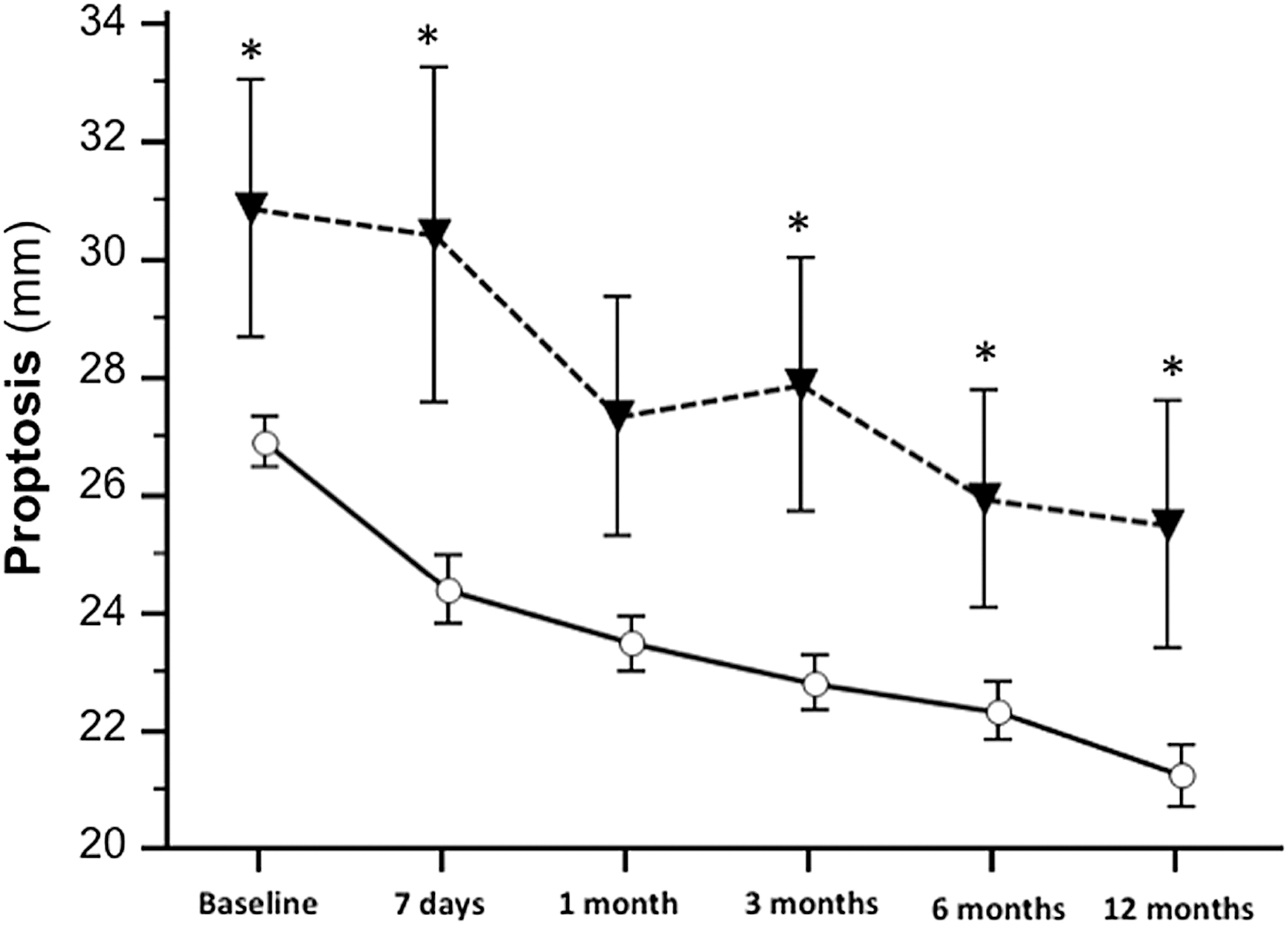
Changes of proptosis (as measured by Hertel's exophthalmometer in millimeters) after surgical orbital decompression (up to 1 year of follow-up). The outcomes of orbits responding to surgery (pinhole BCVA >0.63 at 3 months) are shown with empty circles and a continuous line, whereas the outcomes of not responding orbits are shown with solid triangles and a dashed line. Error bars: SE. *p < 0.05 vs. not responding eyes.
Parameters that could be associated to the study outcome
In this study, administration of “medical decompression” was associated with a significantly higher response rate to subsequent surgery (96% vs. 73%, p = 0.004; Table 1).
Patients' sex and smoking habits did not influence the study outcome. A significant inverse correlation was observed between patients' age and final p-BCVA (r = −0.42; p = 0.0003) but not with the primary outcome. Patients with diabetes appeared to be less likely to be responsive to surgery than non-diabetics, although the difference was not significant (30% vs. 10% needed further surgery, p = 0.20; Table 1). Thyrotropin receptor antibodies (TRAb) at baseline were not significantly associated with the primary outcome (p = 0.62; Table 1).
Orbits submitted to medial wall decompression were significantly more likely to require further surgery (21%) when compared with orbits submitted to “balanced” decompression (21% vs. 4%, p = 0.04; Table 1).
Discussion
To date, surgical orbital decompression is established as the mainstay of DON treatment in patients unresponsive to steroids or other immunosuppressants. 15 Current guidelines suggest “medical decompression” as first-line treatment for DON, as this therapy is effective in about 40% of cases without the need of orbital surgery. 6,8,13,16 In a recent systematic review on surgical and medical treatment of DON, Xu et al. concluded that surgical decompression appears to be better than intravenous steroids in improving visual acuity, relieving proptosis, and reducing DON recurrence. 17
In the present study, visual acuity at 3 months was most strongly associated with successful surgery for DON, resulting in a cutoff >0.63 with good sensitivity and specificity. This is consistent with the reference value proposed by Wakelkamp et al. 18 and by van Geest et al. 19 in their randomized prospective trials. Unlike Wakelkamp et al., we have determined an earlier primary end point (3 vs. 26 months) based on the trend of visual deterioration observed in the orbits unresponsive to surgery.
Our data confirm the high efficacy of orbital surgery in the treatment of DON: most of the orbits studied (87.5%) resulted in definitive treatment after surgery, with good long-term visual acuity (0.85 at 1 year) and no need for further intervention to spare visual function.
The observation that “medical decompression” administered before surgery appears to be associated with a better response rate to surgical decompression (96% vs. 73%) and a better final visual acuity (0.89 vs. 0.80) is an intriguing post hoc analysis result in this study, but it certainly requires confirmation in future prospective research.
Only a small percentage of our orbits (9%) showed persistent inflammation after surgery, which required treatment with steroids in the following weeks. This finding contrasts with that of Wakelkamp et al., 18 who reported that 83% of their patients submitted primarily to surgery required steroids afterward. In orbits affected with DON, it is likely that initial inflammation, especially in patients with predisposing anatomy, triggers soft tissue and muscle congestion. The rapid increase of intra-orbital pressure may cause impairment of orbital venous and lymphatic outflow, self-feeding tissue congestion, optic nerve compression, and consequent visual loss. 20
We believe that our DON patients may have had a baseline CAS more indicative of congestion rather than inflammation and this would explain why the CAS rapidly decreased after surgery, without the need for further steroid treatment.
In this study, balanced decompression was generally associated with a better outcome than medial decompression. Nevertheless, the final p-BCVA achieved with the two procedures was similar (0.86 vs. 0.85). This suggests that unsuccessful medial wall decompression may not preclude achievement of good visual results, as long as patients requiring further treatment are promptly identified.
The major limitation of the present study is its retrospective nature. We were not able to identify strong predictors of response to surgery at baseline due to the small number of unsuccessful events for a multivariate analysis (and limited statistical power). Moreover, we did not collect TRAb data routinely after surgery, and we could not confirm the findings of Eckstein et al. suggesting that higher TRAb levels may be associated with a severe course of GO. 21
One strength of this study is the standardized clinical practice of our combined thyroid-eye clinic. Follow-ups were scheduled at very precise time intervals (1 week, 1, 3, 6, and 12 months after surgery) to which patients adhered very strictly. Similarly, at each follow-up, patients underwent the same standardized set of ophthalmological examinations by the same ophthalmologist (N.C.) and by the same team of orthoptists. Moreover, surgeries were all performed by the same experienced orbital surgeon (C.G.). Another strength of the study is also the size of the study population, with 88 orbits affected with DON, studied before and after surgery.
In conclusion, surgical decompression of the orbit was found to be a very effective treatment for DON. In this study, all clinical parameters significantly improved after surgery and further intervention was rarely needed. These findings certainly require confirmation in future prospective randomized research.
Footnotes
Authors' Contributions
N.C.: clinical management of patients (lead), data collection (lead), statistical analysis (lead), methodology (lead), conceptualization (lead), writing (lead), review, and editing (lead). C.G.: clinical management of patients, conceptualization, review, and editing. G.P.: clinical management of patients, conceptualization, methodology, and review. B.C.: clinical management of patients. A.B.C.: clinical management of patients. M.C.F.: clinical management of patients. S.B.: clinical management of patients. V.M.: clinical management of patients. M.D.: clinical management of patients, data collection (supporting). A.C.: clinical management of patients (supporting), data collection (supporting). I.M.: clinical management of patients, review (supporting). M.A.: clinical management of patients (supporting). F.V.: clinical management of patients (supporting). L.P.: clinical management of patients (supporting). M.S.: clinical management of patients, conceptualization, methodology, review (lead), and editing.
Author Disclosure Statement
All the authors have nothing to disclose. No conflicting relationship exists for any author.
Funding Information
No funding was received for this article.