
Abstract
Background:
The relationship between isolated hypothyroxinemia (IH) in pregnancy and adverse pregnancy outcomes is controversial, with no consensus on the need for treatment.
Summary:
We conducted a systematic review and meta-analysis examining adverse pregnancy and neonatal outcomes in women with IH in pregnancy. We searched PubMed, Embase, Web of Science, and the Cochrane Central Register of Controlled Trials for publications from inception to December 2022. Randomized clinical trials and cohort studies were included. Random-effects meta-analyses were used to estimate pooled relative risks (RRs) for each outcome. We included 21 articles, of which 19 investigated the relationship between IH and maternal and neonatal outcomes and 4 investigated the efficacy of levothyroxine (LT4) treatment. Compared with euthyroid pregnancies, IH pregnancies were associated with an increased risk of preterm birth (RR 1.35 [confidence interval, CI, 1.16–1.56]; I 2 = 9%), premature rupture of membranes (RR 1.41 [CI 1.08–1.84]; I 2 = 0%), gestational diabetes (RR 1.34 [CI 1.07–1.67]; I 2 = 76%), macrosomia (RR 1.62 [CI 1.31–2.02]; I 2 = 42%), and fetal distress (RR 1.72 [CI 1.15–2.56]; I 2 = 0%). However, no statistically significant differences were noted in adverse outcomes according to LT4 treatment status.
Conclusions:
There is evidence suggesting that IH in pregnancy may be associated with an increased risk of adverse pregnancy and neonatal outcomes. However, it is unclear whether LT4 may mitigate the risk of these adverse outcomes.
Introduction
Thyroid hormones are essential for maintaining normal pregnancy and fetal development. Isolated hypothyroxinemia (IH) was defined as a normal thyrotropin (TSH) concentration and low free thyroxine (fT4). 1 IH is relatively common in pregnant women, with a prevalence of 1.3% to 4.3%, and up to 23.9% in iodine-deficient areas. 2,3 Differences in prevalence are related to iodine intake, fT4 diagnostic cutoff point, gestational week of diagnosis, and fT4 testing methods. Iodine deficiency is one of the most common causes of IH. 4 Environmental pollution (thiocyanate, polychlorinated biphenyls), obesity, advanced maternal age, iron deficiency, vitamin D deficiency, and insulin resistance are also associated with IH. 5
Numerous studies have reported that hypothyroidism and subclinical hypothyroidism are associated with adverse pregnancy and neonatal outcomes. 6 –8 However, research on IH is more focused on the impact on the cognitive development of offspring, 9 and it is not clear whether it may be associated with adverse pregnancy outcomes. The Generation R study in the Netherlands showed that IH was associated with an increased risk of preterm birth. 10 Su et al. found that women with IH were at increased risk of fetal distress, small-for-gestational-age infants, and skeletal deformities. 11 However, Chen et al. found that there was no significant difference in the incidence of adverse maternal outcomes or perinatal complications between IH patients and pregnant women with normal thyroid function. 12
In addition, there is uncertainty about whether levothyroxine (LT4) mitigates adverse outcomes in pregnant women with IH. In particular, a large randomized clinical trial (RCT) found that LT4 intervention did not improve adverse pregnancy outcomes. 13 However, a recent study by Li et al. found that LT4 treatment could reduce the risk of miscarriage and neonatal intensive care unit (NICU) admission among pregnant women with IH. 14 We thus conducted a systematic review summarizing the evidence on the association between IH and adverse pregnancy outcomes as well as the effect of LT4 therapy.
Methods
We performed a systematic review and meta-analysis to assess (1) the association of IH on maternal and neonatal outcomes, and (2) the efficacy of LT4 treatment of IH in preventing maternal and neonatal adverse outcomes. This report follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standards for reporting of systematic reviews. 15
Study search
We systematically searched the literature published from inception to June 1, 2022, in PubMed, EMBASE, Web of Science, and the Cochrane Central Register of Controlled Trials, with an updated search conducted on December 1, 2022. A librarian with experience in database designed the search strategy used the combination of the following four concept keywords: (1) mothers and pregnancy, (2) hypothyroxinemia, (3) maternal and fetal adverse outcomes, and (4) LT4 therapy. Supplementary Table S1 provides the complete search strategy. In addition, we manually screened the references of related articles and current review articles for potentially relevant articles.
Study selection and data extraction
Studies were independently assessed by two authors (X.G. and X.W.), and any disagreements were resolved by discussion with a third author (Z.S.). This systematic review and meta-analysis included only RCTs and cohort studies comparing IH pregnant women with euthyroid pregnant women or LT4 therapy in IH patients with untreated IH patients. Thyroid function tests were required to be performed in all participants during pregnancy. We included IH patients with normal TSH and decreased fT4.
We examined the following respective adverse pregnancy and neonatal outcomes: preterm birth, placental abruption, premature rupture of membranes (PROM), gestational diabetes, gestational hypertension, preeclampsia, low birth weight (LBW), macrosomia, small for gestational age (SGA), NICU admission, malformation, and fetal distress. Gestational diabetes was defined as fasting plasma glucose ≥5.1 mmol/L or abnormal oral 75 g glucose tolerance test (T1h ≥ 10 mmol/L, T2h ≥ 8.5 mmol/L). 16 Gestational hypertension was defined as blood pressure more than 140/90 mmHg on at least two occasions after 20 weeks of gestation, no history of hypertension before pregnancy. 17 Preeclampsia was diagnosed as gestational hypertension and coexistence of proteinuria. Fetal distress was diagnosed on fetal heart rate variability analysis. Nonhuman studies, reviews, guidelines, meeting abstracts, case reports, populations not meeting inclusion criteria, outcomes that were not predefined in our list, studies lacking necessary information, and non-English studies were excluded.
Two review authors (B.P. and J.L.) extracted data from eligible studies independently. The extracted data included: basic study information (name of first author, year of publication, country, and study design), sample size, gestational age at diagnosis, diagnostic criteria for IH, thyroid function detection assay, study outcomes, gestational age at LT4 initiation and LT4 treatment dose, and prevalence of different types of adverse outcomes in each group.
Study quality assessment
Two authors independently assessed the study quality (C.Z. and B.G.). We used the Newcastle–Ottawa scale 18 for cohort studies (score of 6 or higher considered as high quality) and the Cochrane Collaboration tool 19 for RCTs. The authors' rated the risk of bias of studies as “low risk,” “high risk,” or “unclear risk.”
Statistical analysis
We performed meta-analyses when there were data from two or more studies investigating the same outcomes, with more than 10 patients in the IH group. We performed random-effects meta-analyses using Review Manager (RevMan 5.3; Cochrane Collaboration, Oxford, United Kingdom) to estimate pooled relative risks (RRs) and their associated confidence intervals (CIs) for each outcome. Cochran's Q test (p < 0.05, statistically significant) and I 2 tests were used to assess heterogeneity. The I 2 values of 25%, 50%, and 75% were considered as having low, moderate, and high heterogeneity, respectively. 20 Publication bias was assessed using Egger test plots using Stata 16 (StataCorp, College Station, TX).
To identify major sources of heterogeneity and to assess the robustness of pooled results, prespecified subgroup analyses were performed based on different gestational ages, fT4 cut-point values for diagnosing IH, and the study design.
Results
Study selection
A total of 9582 citations were initially identified. After excluding duplicate entries, 7209 titles and abstracts were screened, of which 58 full-text articles were eligible for evaluation. Twenty-one articles were included in this study. The reasons for exclusion of each study at the full-text review stage are reported in Supplementary Table S2. Among the 21 studies included, 19 studies investigated the effect of IH on maternal and neonatal outcomes 9,11,12,21 –36 and 4 studies investigated the efficacy of LT4 treatment in preventing maternal and neonatal adverse outcomes. 13,14,29,31 The PRISMA flowchart is shown in Figure 1.

PRISMA flow diagram.
Characteristics of the included studies
We included 1 RCT, 16 prospective cohort studies, and 4 retrospective cohort studies, all of which were considered high quality (Supplementary Table S3). The characteristics of the studies are summarized in Table 1 for observational studies and Table 2 for interventional studies. In part I, namely, the analysis of the association of IH on maternal and neonatal outcomes, 19 articles were published from 2007 to 2022 from 10 countries, including a total of 12,129 pregnant women with IH. In part II, namely, the analysis of the impact of LT4 treatment on maternal and neonatal outcomes, 4 articles, 1 from the United States and 3 from China, were published from 2017 to 2022, including a total of 895 pregnant women treated with LT4 and 1247 pregnant women without LT4 treatment.
Study Characteristics of Observational Studies
DPC, Diagnostic Products Corporation; fT4, free thyroxine; IH, isolated hypothyroxinemia; LBW, low birth weight; NICU, neonatal intensive care unit; PROM, premature rupture of membranes; SGA, small for gestational age; T1, first trimester; T2, second trimester; TSH, thyrotropin; TT4, total thyroxine.
Study Characteristics of Interventional Trials
LT4, levothyroxine.
The effect of maternal IH on pregnancy outcomes
Figure 2 and Supplementary Figure S1 show the outcome estimates for associations between IH and pregnancy outcomes. Compared with pregnancies of euthyroid women, pregnancies in women with IH were associated with an increased risk of preterm birth (RR 1.35 [CI 1.16–1.56]; I 2 = 9%), PROM (RR 1.41 [CI 1.08–1.84]; I 2 = 0%), gestational diabetes (RR 1.34 [CI 1.07–1.67]; I 2 = 76%), macrosomia (RR 1.62 [CI 1.31–2.02]; I 2 = 42%), and fetal distress (RR 1.72 [CI 1.15–2.56]; I 2 = 0%). No association was found with placental abruption, gestational hypertension, preeclampsia, LBW, SGA, NICU admission, or malformations.
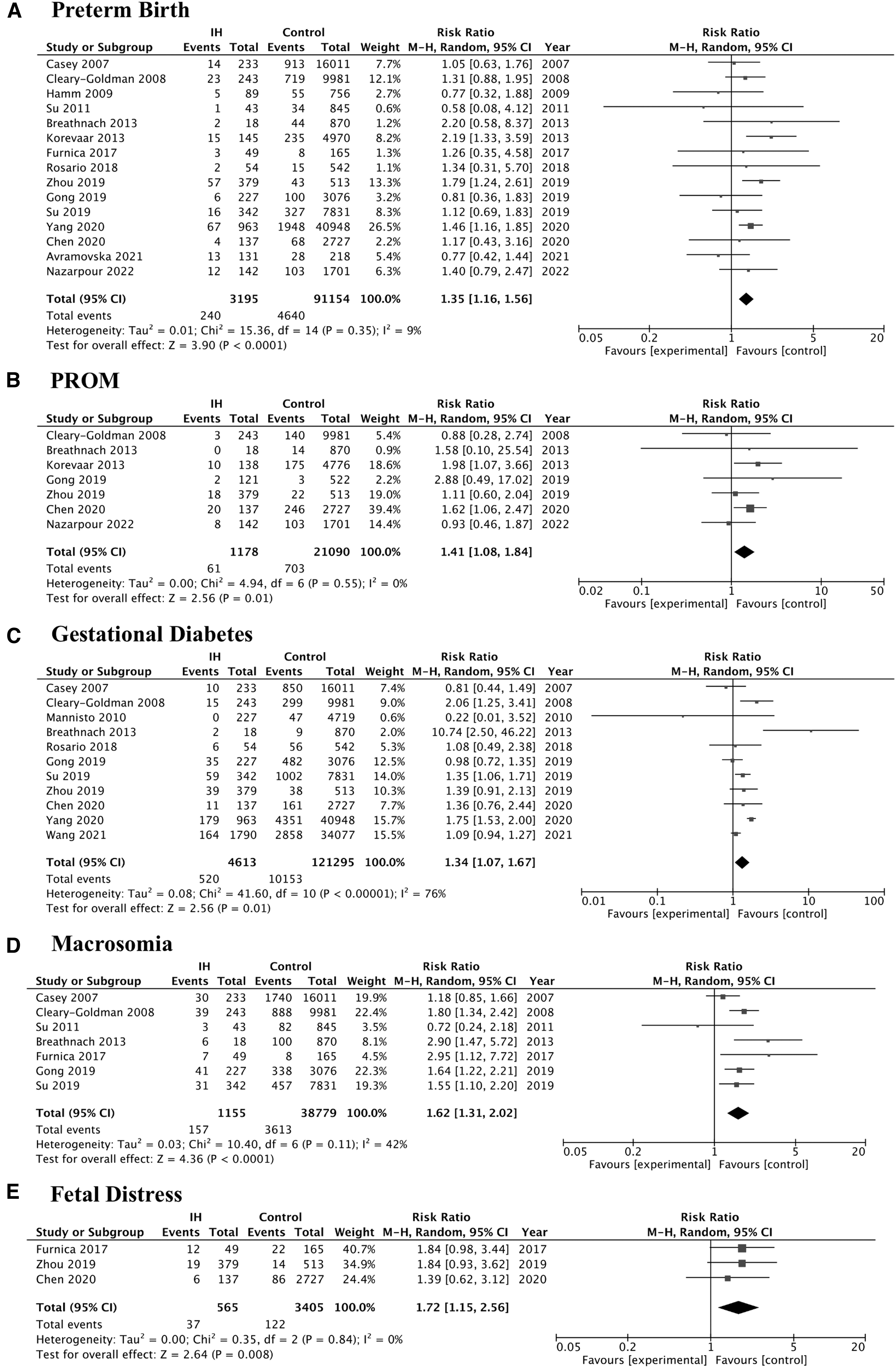
Pooled relative risks of adverse pregnancy outcomes in pregnant women with IH compared with pregnant euthyroid women. CI, confidence interval; IH, isolated hypothyroxinemia; PROM, premature rupture of membranes.
The effect of LT4 intervention on pregnancy outcomes of IH
Table 3 shows the pooled pregnancy and neonatal outcome estimates for women with IH according to LT4 treatment status. There was no significant association with LT4 treatment of IH and the outcomes of preterm birth, placental abruption, PROM, gestational diabetes, gestational hypertension, preeclampsia, LBW, macrosomia, and NICU admission.
Pooled Relative Risk Estimates of Adverse Pregnancy Outcomes in Women with Isolated Hypothyroxinemia According to Levothyroxine Treatment Status
CI, confidence interval; RR, relative risk.
Subgroup and sensitivity analyses
In a prespecified sensitivity analysis, the risk of preterm birth was significantly increased in IH diagnosed in the first trimester (RR 1.30 [CI 1.08–1.58]; I 2 = 0%), but there was no significant association observed for IH diagnosed in the second trimester. In IH diagnosed in the second trimester, the risk of gestational diabetes (RR 1.61 [1.19–2.18]; I 2 = 5%) and macrosomia (RR 1.73 [1.36–2.20]; I 2 = 0%) were significantly increased (Table 4).
Association of Isolated Hypothyroxinemia with Adverse Pregnancy Outcomes According to Gestational Age
According to different fT4 cut-point values used for diagnosing IH, when using the fT4 < 2.5th percentile, gestational IH was associated with preterm birth (RR 1.42 [CI 1.18–1.70]; I 2 = 7%), placental abruption (RR 1.92 [CI 1.05–3.51]; I 2 = 0), PROM (RR 1.75 [CI 1.15–2.67]; I 2 = 0%), gestational diabetes (RR 1.55 [CI 1.16–2.06]; I 2 = 76%), and macrosomia (RR 1.74 [CI 1.46–2.06]; I 2 = 84%). When using the fT4 < 5th percentile, IH was associated with preterm birth (RR 1.69 [CI 1.18–2.40]; I 2 = 0%) and fetal distress (RR 1.84 [CI 1.16–2.91]; I 2 = 0%). When using the fT4 < 10th percentile, we analyzed only preterm birth and gestational hypertension and found no significant association (Table 5).
Association of Isolated Hypothyroxinemia with Adverse Pregnancy Outcomes According to Free Thyroxine Cut-Point Values
In prospective studies, there were significant associations between IH and preterm birth (RR 1.36 [CI 1.14–1.61]; I 2 = 18%), PROM (RR 1.41 [CI 1.08–1.84]; I 2 = 0%), gestational diabetes (RR 1.40 [CI 1.03–1.89]; I 2 = 71%), gestational hypertension (RR 1.25 [CI 0.95–1.66]; I 2 = 41%), and macrosomia (RR 1.66 [CI 1.19–2.31]; I 2 = 52%). In retrospective studies, IH was only associated with macrosomia (RR 1.82 [CI 1.06–3.11]; I 2 = 33%) (Supplementary Table S4).
In considering study country, gestational IH was associated with preterm birth (RR 1.28 [CI 1.01–1.63]; I 2 = 16%), placental abruption (RR 2.03 [CI 1.06–3.88]; I 2 = 0%), and macrosomia (RR 1.82 [CI 1.23–2.70]; I 2 = 63%) in studies from outside of China. Gestational IH was associated with preterm birth (RR 1.41 [CI 1.17–1.56]; I 2 = 4%), PROM (RR 1.47 [CI 1.04–2.06]; I 2 = 0%), gestational diabetes (RR 1.30 [CI 1.04–1.63]; I 2 = 80%), gestational hypertension (RR 1.51 [CI 1.01–2.72]; I 2 = 76%), and macrosomia (RR 1.56 [CI 1.25–1.94]; I 2 = 0%) in studies from China (Supplementary Table S5).
Discussion
In this systematic review and meta-analysis, we observed that maternal IH was significantly associated with an increased risk of premature birth, PROM, gestational diabetes, preeclampsia, macrosomia, and fetal distress. However, LT4 treatment was not associated with a reduction in the risk of preterm birth, placental abruption, PROM, gestational diabetes, gestational hypertension, preeclampsia, LBW, macrosomia, and NICU admission.
Several studies have reported on the relationship between IH and preterm birth, and three existing meta-analyses have had variable findings. A meta-analysis by Korevaar et al. used individual participant data to investigate the relationship between thyroid dysfunction in pregnancy and premature birth. 8 A total of 904 pregnant women with IH were included with fT4 below the 2.5th percentile as the cutoff point. Korevaar et al. showed that pregnancy IH was related to the risk of premature delivery and early premature delivery. 8 Similarly, Parizad Nasirkandy et al. reported that the a RR of 1.31 (95% CI: 1.04–1.66) for preterm birth in IH on (using data from 7 studies, including 1078 women with IH and 44,377 control women). 37
However, the meta-analysis of Sheehan et al. did not show a significant association between IH and preterm birth. 38 Only 5 related studies with a total of 603 pregnant women with IH were included in the meta-analysis by Sheehan et al. 38 Our meta-analysis included 3195 pregnant women with IH from 11 studies, so it is the most comprehensive review to date and the findings are consistent with the results of Korevaar et al. 8 In a subgroup analysis, we observed that IH diagnosed in the first trimester, but not in the second, was associated with an increased risk of preterm birth. Furthermore, IH defined by fT4 levels below the 2.5th–5th percentile was associated with an increased risk of preterm birth. These results suggest that severe IH or IH occurring in the first trimester increases the risk of preterm birth.
In the analysis of IH and gestational diabetes, we included 11 studies and found that the incidence of gestational diabetes mellitus was significantly higher in patients with IH. Luo et al. included nine articles in their meta-analysis examining to analyze the relationship between IH and gestational diabetes mellitus. 39 IH was associated with a 1.45-fold increased risk of gestational diabetes, which was similar to our results. Bassols et al. also reported that fT4 was significantly inversely correlated with maternal HbA1c. 41 Gu et al. observed that low levels of fT4 were associated with hyperglycemia and insulin resistance. 41 In our subgroup analysis, only IH diagnosed in the second trimester was associated with an increased incidence of gestational diabetes. This may be due to the progression of glucose intolerance in pregnant women as pregnancy progresses.
Toloza et al. reported that in an individual participant meta-analysis including 933 pregnant women with fT4 below the 2.5th percentile, no significant association was observed between IH and gestational hypertension or preeclampsia. 42 Similarly, no association between IH and gestational hypertension or preeclampsia was found either in the overall meta-analysis or in a subgroup analysis with fT4 < 2.5th percentile. In our meta-analysis, we included a larger number of patients, but we did not adjust for age, ethnicity, smoking, or other factors, which is a limitation of our analysis.
We observed that pregnant women with IH were at increased risk of macrosomia and fetal distress compared with pregnant women with normal thyroid function. A meta-analysis including data from 929 individuals with IH showed that IH was associated with a lower rate of SGA and higher mean birth weight and that a 1-standard deviation increase in fT4 was associated with a 21-g decrease in birth weight. 43 Gestational diabetes and fluctuations in blood glucose associated with IH may contribute to fetal weight gain. Furthermore, many studies have reported that pregnant women with IH have a higher body mass index, which may also play a mediating role between IH and macrosomia. 13,44 The adverse pregnancy outcomes, such as hypertension, placenta previa, and PROM, may also cause fetal distress.
In this study, IH was defined as a normal TSH concentration and low fT4, but there were variable cutoff point for the lower limit of fT4, including the use of the 2.5th/5th/10th percentiles. 1 In sensitivity analyses, the studies using fT4 < 2.5th percentile as the cutoff point were those where IH was associated with preterm birth, placental abruption, PROM, gestational hypertension, and macrosomia. When fT4 < 10th percentile was used as a cutoff, no significant association was observed. This suggests that the diagnostic definition of IH may influence the relationship between IH and adverse outcomes. The authors of a recent meta-analysis also suggest using the 2.5th percentile cutoff for fT4 levels to define IH, 45 and our findings are confirmatory.
Several studies have shown that iodine status affects pregnancy and neonatal outcomes, 46 but unfortunately, only four of the studies included in this article provided iodine nutrition levels, and we did not have sufficient information for a formal subgroup analysis. Among our included literature, there were nine studies from China, and they were all of high quality. China has successfully corrected iodine intake deficiencies since the salt iodization policies; iodine nutrition levels are currently appropriate nationwide. 47
However, considering the potential population differences, we performed subgroup analyses to analyze the results of the studies, according to whether they were performed in China or not. We observed an increased risk of preterm delivery and macrosomia for IH in pregnancy, regardless of whether the studies were performed in China or outside of China. IH was associated with more adverse pregnancy outcomes such as gestational diabetes and gestational hypertension in the studies from China. This suggests that multiple confounding factors associated with IH, such as population differences, iodine status, and management practices of pregnant women, may influence obstetric outcomes.
There is an increased risk of pregnancy complications associated with IH during pregnancy, but there is no consensus on the need for IH treatment in pregnancy. The American Thyroid Association guidelines do not recommend LT4 therapy for women with IH (weak recommendation, low-quality evidence). 1,48 RCTs have not demonstrated the beneficial effect of LT4 on adverse pregnancy outcomes and child cognition. In the evaluation of the effect of LT4 treatment on pregnancy outcomes, Casey et al. 13 found no improvement in adverse pregnancy outcomes among 263 IH patients who received LT4 and 261 controls without IH who received placebo at a mean gestational age of 17 weeks. However, starting treatment in the second trimester may affect LT4 efficacy on maternal and neonatal outcomes. Li et al. conducted an interventional trial involving 463 IH pregnant women with IH in the first trimester who were treated with LT4 and 501 untreated women and found that LT4 treatment was significantly associated with a reduced the incidence of miscarriage and NICU admission. 14
Zhou et al. initiated isolated IH treatment with LT4 in the second or third trimester and found that treatment was associated with a reduced the risk of preterm birth and LBW infants. 31 In this systematic review, four studies on LT4 treatment were included, and the meta-analysis did not reveal a beneficial effect of LT4 treatment. A large birth cohort study from Spain suggested that LT4 treatment was safe and was associated with improved pregnancy outcomes of women with an unsatisfactory fT4 level (≤7.5 pg/mL) at before the 9th week of gestation; 49 however, we did not include this study in our meta-analysis because the authors only compared fT4 ≤ 7.5 pg/mL with those >7.5, without considering TSH level. Future well-designed RCTs with large sample sizes, enrolling women in early pregnancy, are urgently needed to inform whether thyroid function screening and LT4 treatment improve pregnancy and neonatal outcomes in women with IH. Risk factors and fT4 level thresholds should be explored.
To the best of our knowledge, this is the most comprehensive systematic review and meta-analysis to date that quantifies the risk of adverse maternal and neonatal outcomes in pregnant women with IH. We also examined the impact of LT4 therapy on adverse pregnancy and neonatal outcomes, advancing knowledge from previous systematic reviews. 50 The studies included in this review were considered of high quality. However, we did not have individual participant data, making it impossible to conduct individual participant data meta-analysis. Another limitation is that the definition of IH varied from study to study, thus influencing the heterogeneity of the overall assessment. For this reason, we conducted sensitivity analyses exploring various cutoffs for fT4 values. We were unable to evaluate the influence of other factors, such as differences in baseline indicators, iodine status, and underlying diseases, among the study population in the original literature, which may have explained the heterogeneity. Another limitation is that this systematic review was not registered in advance in the International Prospective Register of Systematic Reviews.
We believe that substantial evidence exists to support an association between IH in pregnancy and a variety of adverse maternal and infant outcomes, but the efficacy of levothyroxine treatment in preventing these adverse outcomes remains uncertain and more research is needed.
Footnotes
Authors' Contributions
Y.H.: Writing—original draft (lead). X.G. and X.W.: Data curation (equal). C.Z. and B.G.: Investigation (equal). B.P. and J.L.: Visualization (equal). A.L.: Conceptualization (lead). Z.S.: Writing—review and editing (lead).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by Chinese National Natural Science Foundation (81700697, 82100831).
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5