
Abstract
Before the 20th century, thyroid surgery was regarded as “horrid butchery” such that no honest and sensible surgeon would ever engage in it. Yet, by the mid-20th century, thyroidectomy had become a respected, life-saving, safe, and increasingly practiced operation. From Kocher to Wells and onward into the 21st century, the evolution of thyroid surgery has continued, enhanced by the integration of endocrinology, genetics, immunology, physiology, technology, training, and multidisciplinary care. The ability to personalize and optimize the care of thyroid disorders has been progressively achieved through shared insights and discoveries, highlights of which are described herein.
The extirpation of the thyroid gland for goiter typifies perhaps better than any other operation the supreme triumph of the surgeon's art.—William Halsted (1852–1922). 1
T
A discussion of the highlights of the last century would be incomplete without briefly acknowledging key advances before the 20th century that enabled safe thyroid surgery to be performed in the first place. Although space limitations preclude a more detailed review of every important advance with an impact on thyroid surgery, many of these topics are addressed in other invited articles in this American Thyroid Association (ATA) Centennial series.
Before the revolutionary developments in anesthesia, antisepsis, and hemostatic instruments in the mid-19th century, thyroid surgery was vehemently condemned due to its high mortality rate. When the brilliant Swiss surgeon–scientist, Dr. Theodor Kocher (1841–1917) (Fig. 1), performed his first thyroid surgery in 1872, the mortality rate from thyroidectomy was as high as 70%. In place of the pain, suffocation, sanguination, and sepsis associated with thyroid surgery, 2 Kocher's utter lack of fuss and confusion characteristic of so many other clinics of that time 3 established meticulous, calm, and logical stepwise care of patients.
Emil Theodor Kocher (1841–1917) whose work revolutionized thyroid surgery and physiology and who was the first surgeon to be awarded the Nobel Prize in 1909 (image from
The discovery of human parathyroid glands by Ivar Sandström (published in 1880) (Fig. 2) and recognition that their preservation prevented tetany (by Gley, 1891 and others) led to further refinements in techniques. The principles of clamp-and-tie blood vessel control, extracapsular dissection, and identification and preservation of the recurrent laryngeal nerves were espoused by Kocher and Mikulicz and further advanced by Halsted, Lahey, and others who followed.
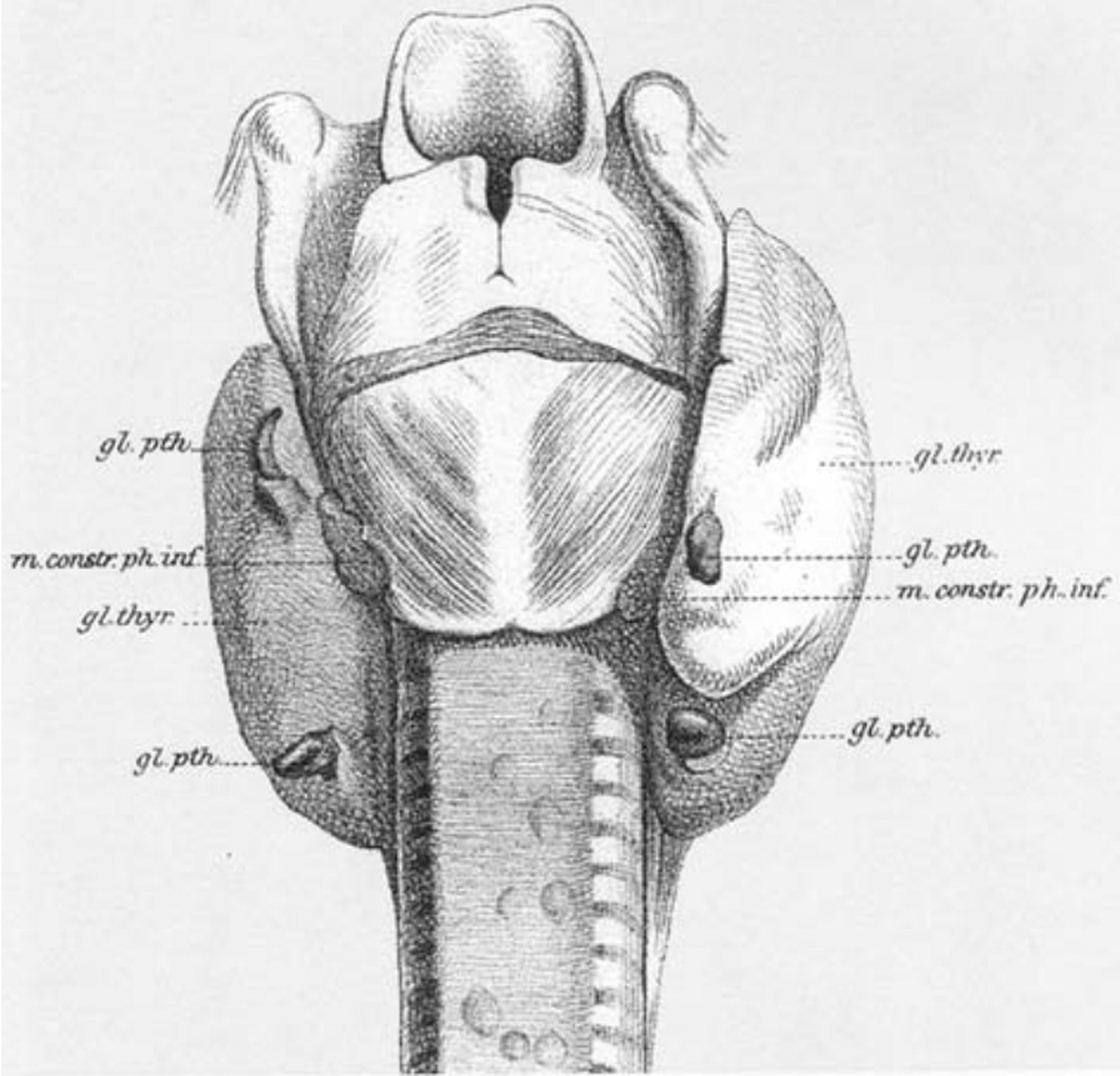
The parathyroid glands, drawn by Ivar Sandström (1852–1889), a Swedish medical student at the University of Uppsala. Owing to his meticulous dissections of animal and human cadavers, he was the first to describe a gland as “hardly as big as a hemp seed, which was enclosed in the same connective tissue as the thyroid, but could be distinguished therefrom by the light colour.” Reprinted from Johansson, 2015, Online Open Access; doi: 10.3109/03009734.2015.1027426.
However, Kocher's disheartened observation that patients who survived total thyroidectomy for goiter, only to be doomed to be cretins, were “saved for a life not worth living” led to his commitment to performing subtotal thyroidectomy or thyroid lobectomy only, while seeking to understand the function, and not just the anatomy, of the thyroid gland. 4 Through his pursuit of a deep understanding of thyroid physiology, combined with his appreciation of regional anatomy, Kocher became the first surgeon to be awarded the Nobel Prize in 1909; by this time, he had transformed thyroidectomy and reduced its mortality risk to <1%. 5,6
A master educator, Kocher laid the foundation for the role of surgeons in advancing the art and science of thyroid surgery and thyroidology for the next century. The contemporary and ensuing generation of thyroid surgeons, including American surgeons, William Halsted (1852–1922), Harvey Cushing (1869–1939), George Crile (1864–1943), Charles Mayo (1865–1939), and Frank Lahey (1880–1953), and the Australian surgeon, Thomas Dunhill (1876–1957), worked collegially to expand and enhance the techniques, sometimes across large geographic barriers and multiple world wars.
For example, Dr. Dunhill visited some of the top thyroid surgery centers in the United States and England, where he shared results of his approach to thyrotoxic goiter, with 230 cases and only 4 deaths in patients treated with unilateral lobectomy and contralateral subtotal thyroidectomy. 7 –9 Dunhill also recognized that earlier intervention rather than last-resort surgery after progressive deterioration from thyrotoxicosis was a key ingredient to minimizing complications.
The American Association for the Study of Goiter, which later became the ATA and whose original members were mostly surgeons, was founded in 1923. In his presidential address to the Association in 1929, the surgeon, Seymour D. Van Meter, stated: “Who thinks a matter out is of no importance whatsoever. The important thing is that the problem should be solved. This was the theory upon which the originators of our Association based their hopes of progress and ultimate success in the solution of the unsolved phases of goiter.” 10
Today's surgical societies have collaborated to ensure that this same determination and meticulous attention to detail are the mainstays of subspecialty training in thyroid surgery. The evolution of a competent thyroid surgeon now includes extensive education in the preoperative, intraoperative, and postoperative care of patients with thyroid diseases, incorporating technical and scientific adjuncts. Given the breadth of new developments in thyroid surgery, it is no surprise that fellowships and additional training have been designed in these areas by our professional societies.
The surgical management of both structural and functional disorders of the thyroid advanced in conjunction with insights in endocrinology. After observed benefits from injection of thyroid extract (1891, by George Murray), consumption of sheep thyroid (1890s), and isolation of thyroxine (T4) (1915, by Kendall), the chemical structure of thyroxine was identified in 1926 (Harington). 11 The first commercial thyroxine was produced in 1949, and triiodothyronine (T3) was isolated soon thereafter in 1952–1953. The availability of both synthetic and desiccated (animal) T4 and T3 resulted in the ability to replace the thyroid hormone and thus avoid hypothyroidism (cretinism), even following total thyroidectomy.
In the 1940s, the antithyroid action of thionamide drugs was recognized, 12 which provided both a new alternative to surgery for thyrotoxicosis and a dramatic decrease in the risk of a postoperative thyroid storm when surgery was undertaken. The additional therapeutic alternative of radioactive iodine (131I) for hyperthyroidism was simultaneously identified, and early success helped spawn the development of theranostics (the combination of drugs or techniques to simultaneously or sequentially diagnose and treat medical conditions).
With thyroidectomy having become a safe, respected, and more widely practiced procedure, the following decades saw developments in preoperative tools that influenced patient selection for surgery. Imaging studies evolved. For a generation in the mid-20th century, the radionuclide 123I thyroid scan provided information about thyroid function (“hot” vs. “cold” nodularity), yet crude anatomic resolution.
Low-resolution ultrasound provided better anatomic detail, but fairly primitive characterization of thyroid nodules beyond size and composition. Expansion in imaging modalities to include cross-sectional scans (CT and MRI), high-resolution B-mode ultrasonography (as well as Doppler sonography, including carotid artery studies), and ultimately [18F]Fluorodeoxyglucose-positron emission tomography/computed tomography scanning led to an increase in detection of thyroid nodularity.
Increased identification of even small nodules through imaging, early (and exaggerated) connotation of malignancy with cold nodules, and availability of the exogenous thyroid hormone led to a steady increase in the practice of thyroid surgery for diagnostic and therapeutic purposes. Total thyroidectomy became commonplace. Fortunately, patient selection and risk stratification were aided by the evolution of expertise in thyroid cytology obtained through fine-needle aspiration (FNA) biopsy.
The widespread adoption of thyroid FNA in the 1980s resulted in a reduction in thyroid surgery for benign disease and an increase in yield of malignancy on surgical pathology of thyroidectomy specimens. 13 The Bethesda System for Reporting Thyroid Cytology (original publication in 2009, updated in 2017, and version 3 expected in 2023) later helped to standardize the reporting of thyroid nodule biopsies 14,15 and to imply cancer risk, according to assignment of samples to one of six categories. A majority of thyroid nodules can be definitively characterized as either benign or malignant by cytology, with high sensitivity (≤3% false-negative rate). Still, 20–30% of FNAs yield indeterminate cytology 16 and until the advent of molecular testing, they would have resulted in a recommendation for diagnostic thyroid lobectomy at a minimum.
The double-edged sword of refinement in ultrasound resolution, combined with a well-intentioned, but oversimplified, belief that early cancer detection is advantageous, contributed to a steady increase in the rate of diagnosis of thyroid cancer, the vast majority of which was well-differentiated and early-stage disease. 17 Throughout the first decade of the 21st century, thyroid cancer was hailed as the fastest growing cancer diagnosis, yet mortality rates from thyroid cancer were noted to be low and essentially stable.
As a result, guidelines for the evaluation and management of thyroid nodules have been, and continue to be, progressively modified in an effort to reduce unnecessary biopsies and overdiagnosis of nonclinically significant cancers. 18 –20 Ultrasound-based risk stratification systems for incidental thyroid nodules have been developed throughout the world to refine criteria for performing FNA or ultrasound surveillance. 19,21 –25 These systems have also standardized the reporting of ultrasound examinations and hence several bear names incorporating the theme of TI-RADS (Thyroid Imaging Reporting and Data System).
In parallel, active surveillance (reserving intervention for evidence of disease progression or patient preference) is a modern approach taken to address small, low-risk thyroid cancers, which relies on serial ultrasonography. Initiated in Kuma, Japan, in 1993, 26 active surveillance has proven to be a safe alternative to immediate surgery in carefully selected healthy patients with papillary thyroid microcarcinoma and is progressively gaining acceptance around the globe. 22,27,28 In addition, in situ ablation of papillary microcarcinomas is now under investigation. 29
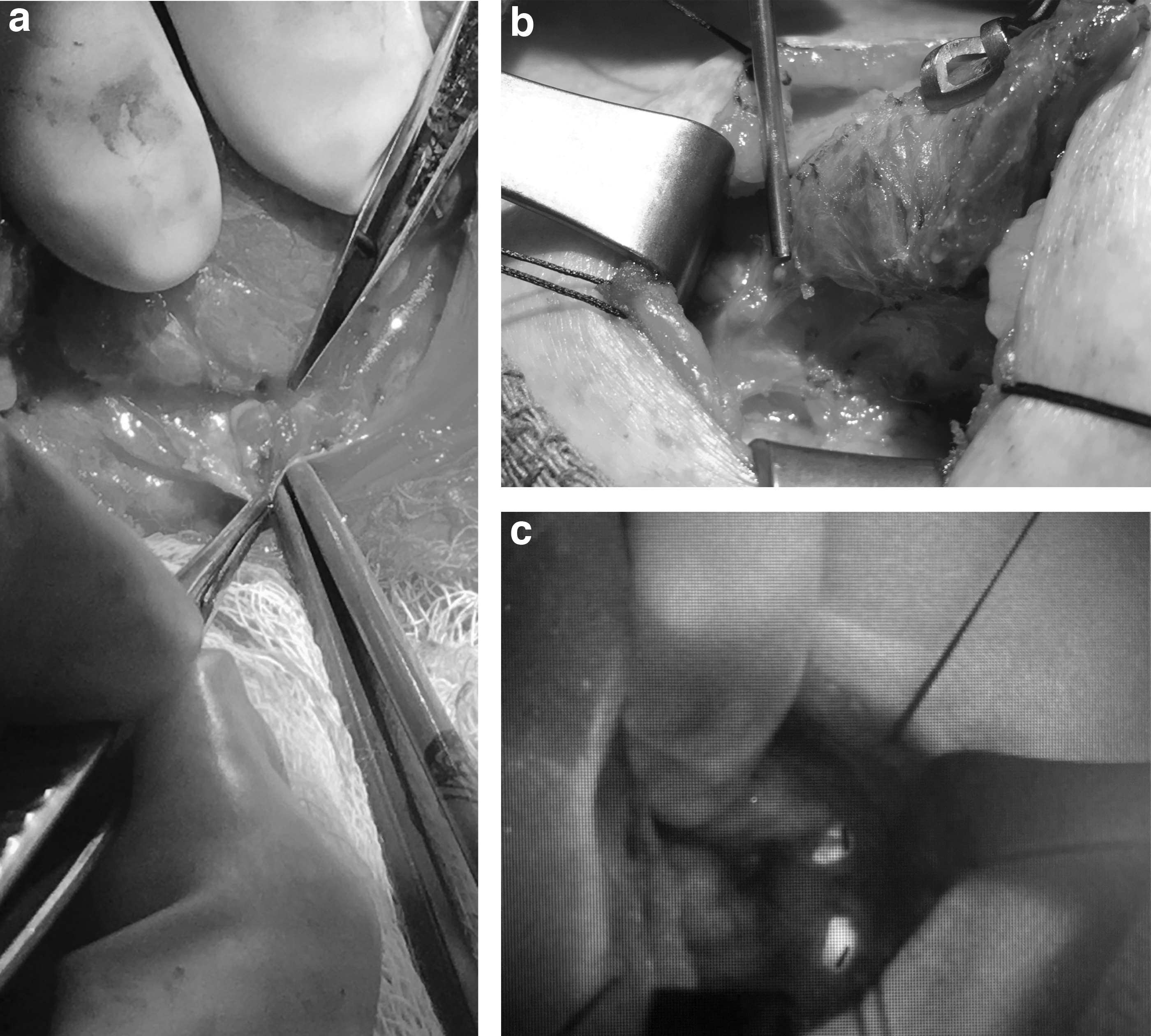
Clinician-performed ultrasonography has enabled interpretation of features in the context of known patient history, symptomatology, and physical findings (Fig. 3a). Ultrasound examination of the neck beyond the thyroid itself has enhanced preoperative planning and postoperative surveillance tailored to the individual patient's condition, and ultrasound-guided FNA may be incorporated as needed.

All of these advancements have resulted in a trend toward de-escalation of treatment for low-risk, differentiated (mainly papillary) thyroid cancer; more selective use of total thyroidectomy plus postoperative 131I ablation; and increasing acceptance of thyroid lobectomy with no 131I ablation for early-stage (low-risk) disease, especially when clinically apparent lymph node metastases are not present.
The application of thermal and chemical ablation techniques to benign thyroid disease as well as for palliation in select cases of metastatic malignancy has grown in popularity and acceptance in the 21st century. Cystic thyroid nodules have been treated with alcohol and other sclerosing agents for decades. 30 Now, volume reduction of large, solid, and mixed benign thyroid nodules by thermal or chemical means has been embraced, pioneered in Asia and Europe and propagated around the globe (Fig. 3b–d). Radiofrequency, laser, microwave, and high-intensity focused ultrasound are all being employed. These techniques will continue to provide alternatives to traditional thyroidectomy and all of them rely on image guidance, predominantly through ultrasound. 29
In spite of these many nonsurgical advances, the global volume of thyroid surgical procedures has continued to grow. From 1996 to 2006, the total number of thyroidectomies performed in the United States increased by 39%, from 66,864 to 92,931 cases per year. Outpatient procedures increased by 61%, while inpatient procedures increased by 30%. 31 By 2016, the number of annual thyroidectomies had increased to 169,000. 32
These figures predate the COVID pandemic that began in 2019, which has further influenced a shift toward ambulatory and outpatient care. In addition to surgical safety, factors such as economics, insurance influences, patient expectations, desire for avoidance of infection, and ability for telehealth and communication have all led to shorter hospital stays and more outpatient procedures. 33 The impact of newer ablative technologies for benign thyroid nodules on surgical statistics has yet to be quantified.
Meanwhile, an array of surgical devices and approaches have been combined to make thyroid surgery safer, faster, less visible, less painful, more precise, and more individualized. Since the origins of thyroid surgery, the vulnerability of the laryngeal nerves has been recognized and regarded with respect. Nerve avoidance, superseded by identification and protection, has been a surgeon's top priority. Progress in hemostasis that prevented exsanguination also enabled identification and dissection of the laryngeal nerves, aided by lighting and magnification. 34
Examination of the larynx, beginning with indirect mirror laryngoscopy, as first described by Manuel Garcia in 1854, 35 evolved to incorporate fiberoptics, stroboscopy, video recording, and even ultrasonography. Most literature citing rates of vocal fold paralysis after thyroidectomy, even into the current century, has been based not on laryngeal examination, but on perceptual voice assessment, which significantly underrecognizes nerve dysfunction.
Nevertheless, in the quest to prevent laryngeal nerve injury in the first place, nerve monitoring technology evolved and has grown in adoption. 36 Endotracheal tube-based surface electrodes and pulsed intermittent or continuous laryngeal nerve stimulation provide objective functional and prognostic information during thyroid surgery, which aids intraoperative decision-making and perioperative management. 37,38
Energy-based devices for hemostasis have been developed and increasingly applied in thyroid surgery. 39 –41 Current vascular sealing tools include ultrasonic, bipolar radiofrequency, and hybrid energy systems. Use of these devices in no way lessens the responsibility for knowledge of regional anatomy and avoidance of thermal injury to delicate structures, especially the laryngeal nerves, parathyroid glands, trachea, esophagus, and the skin. The cost of such devices appears to have been offset by a reduction in operative time, operative blood loss and transfusion need, and hospital length of stay. Furthermore, these devices, along with endoscopic and robotic equipment, have planted the seed that has enabled minimal access thyroid surgery to blossom.
The three broad categories of minimal access thyroid procedures include completely endoscopic procedures (either direct or remote access) with carbon dioxide insufflation; partly endoscopic gasless procedures; and nonendoscopic mini-incision procedures. 39 Remote access to the thyroid has been gained through axillary, breast, facelift, and most recently transoral vestibular approaches. The dominant motivation for such approaches is cosmetic: avoidance of a visible neck scar. However, additional potential advantages include reduced overall trauma, scarring, and postoperative pain in carefully selected candidates with appropriate thyroid and overall anatomy.
Since Kocher's time, the preservation of parathyroid glands and their blood supply has been a paramount goal in thyroid and central neck surgery. The techniques of anticipation, meticulous dissection, and distal vessel ligation beyond the point of parathyroid perfusion remain the gold standard. Parathyroid autotransplantation has been practiced since at least the 1920s. 42 Capitalizing on the biochemistry and ultrashort half-life (3–5 minutes) of the parathyroid hormone (PTH), 43 rapid intraoperative PTH testing was developed initially for parathyroidectomy surgery to treat hyperparathyroidism, but subsequently as a means of assessing normal parathyroid function during and after thyroid surgery.
In 2011, 44 the first reports of near-infrared (NIR) parathyroid autofluorescence were published. Since then, camera-based and probe-based devices have been designed, with FDA approval gained in 2018 in the United States for real-time parathyroid gland identification during surgery (Fig. 4a–c). These devices have been coupled with contrast enhancement (using intravenous indocyanine green) to detect fluorescence not only in the glands themselves but also in their perfusing blood vessels. NIR fluorescence detection has the potential to help identify and preserve parathyroid glands, reduce the operating time, and prevent hypoparathyroidism.
Use of molecular genetics to fine-tune either the need for thyroid surgery or the appropriate extent of thyroid surgery has become an important aspect of the art and science of thyroid surgery in the last 30 years. Medullary thyroid carcinoma (MTC) was the first cancer in which surgeons investigating the role of genetic changes were led to proposing that surgery based on a germline mutation be performed before surgical manifestation of disease. 45 –47 Subsequent knowledge about genetic–phenotypic correlation in patients with mutations of the rearranged during transfection (RET) proto-oncogene led to published guidelines on the surgical management of patients with either sporadic or hereditary MTC. 48,49
Prophylactic thyroidectomy met all the criteria for applying knowledge of hereditary cancer syndromes: the genetic mutation known to cause MTC with complete or near-complete penetrance became testable with high accuracy, the thyroid gland could be removed with minimal morbidity and virtually no mortality, there was a hormone to replace the function of the organ being surgically removed, and there was a reliable marker (calcitonin) to determine if the treatment was curative.
Prophylactic thyroidectomy, defined as removing the thyroid before MTC is clinically apparent, became the standard of care. As genetic–phenotypic heterogeneity has become recognized in families with MTC, the recommended age for prophylactic thyroidectomy in MTC patients has become dependent on the specific knowledge about the mutation and its natural history. 48,50,51
The historical context of the discovery of the RET proto-oncogene and the role of surgeons in the paradigm shift toward suggesting surgery based on germline genetic testing rather than as a treatment of an existing tumor is critical to understand. 9 Multiple endocrine neoplasia type 2 and its subgroupings (MEN2a, MEN2b, and familial MTC) have MTC as a prime feature. In the 1950s, the surgeon, Dr. Samuel Wells, meticulously documented features of various MEN syndromes within multiple kindred as he worked to characterize calcitonin as a marker of MTC and enable early detection.
By using pentagastrin to stimulate calcitonin production from the hyperplastic C cells of the thyroid, he was able to diagnose MTC and treat it surgically before development of lymph node-positive disease. Wells recognized that while some patients were cured by this method, many still died of distant metastatic disease. In 1985, Takahashi, while searching for “transforming” genes by looking at fragments that could result in transformation of normal fibroblasts, identified a gene he named “REarranged during Transfection” or RET. 47
By 1987, the RET proto-oncogene had been mapped to chromosome 10, and genetic linkage analysis had mapped the MEN2a locus to the same chromosome. 52 By 1993, Wells together with Dr. Helen Donis-Keller identified seven RET mutations by screening multiple families with all three MEN2 types. Over the next few years, additional mutations were found by various groups and these mutations were noted to activate the tyrosine kinase.
This eventually led to seminal work by Chi and Wells who proposed the first set of predictive genetic tests for MEN2 based on the identified mutations in the RET proto-oncogene. 45,53 By 1995, Wells showed that prophylactic surgery driven by knowledge of a patient's genetics was the key to long-term survival and opened the door to other future prophylactic surgeries based on genotype. 54 These were the first forays into personalizing thyroid surgery based on germline genetic testing.
Today, the evaluation of thyroid nodules, especially those with indeterminate cytology, has led surgeons to further innovations in the use of nongermline mutational analysis. Before the molecular characterization of thyroid nodule FNA cytology, most patients with indeterminate nodules underwent diagnostic thyroid surgery, usually lobectomy, for what ultimately proved most often to be benign disease. Molecular testing now available to surgeons has allowed for better risk stratification and has dramatically reduced the need for diagnostic surgery.
Unfortunately, due to high costs of these genetic tests, this innovation is not currently accessible worldwide. Surgeons have come to better understand the mutational landscape of thyroid nodules and thyroid cancers. Some mutations such as RAS are known to be “weak drivers” since they are not uniquely found in malignant neoplasms of the thyroid, whereas certain other mutations such as RET, NTRK, ALK, BRAF, TERT, and p53 are now known as “strong drivers” of cancers, with none generally being expressed in normal thyroid epithelial cells. 55
At the other end of the risk spectrum, the use of molecularly driven care has allowed surgeons to comanage patients with anaplastic thyroid carcinoma (ATC) with novel approaches. While most patients with ATC are still presenting with locally unresectable disease and distant spread at time of diagnosis, molecular profiling of suspected ATC is now recommended at diagnosis—including testing for BRAF and NTRK mutations and programmed death-ligand 1 expression by pathologic immunostaining or by molecular testing. 56
Furthermore, the use of blood-based liquid biopsy for circulating (cell-free) tumor DNA shows great promise for even more rapid profiling of aggressive thyroid cancer variants. 57,58 Patients with ATC who have BRAF-mutated tumors may undergo neoadjuvant therapy with BRAF/MEK inhibitors and in some cases with the addition of immune checkpoint inhibitors, leading to potential dramatic tumor responses with enough shrinkage that tumors may become surgically resectable 59 –62 (Fig. 5a–c).
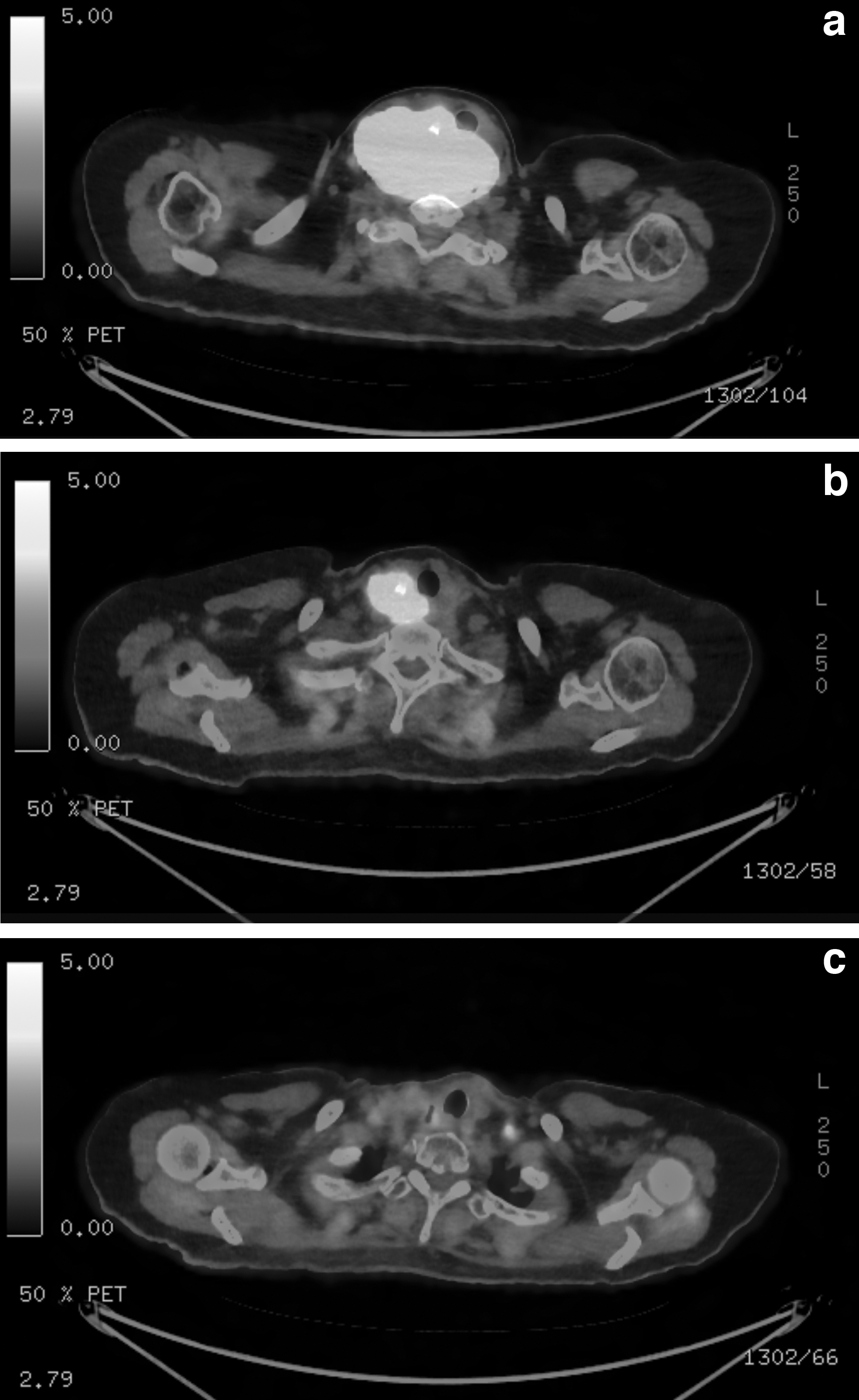
Even nonresectable or disseminated disease may achieve a prolonged palliative response to targeted systemic therapy with or without external beam radiation compared with nontargeted therapy with cytotoxic chemotherapeutic agents. Perhaps these developments in the integration of genetics, immunology, physiology, technology, research, training, and multidisciplinary care epitomize better than any other advances in the last century the ability of risk stratification and personalization of thyroid care (Fig. 6).
Kocher's words remain as true today as they did in his time, yet with contemporary optimism, thanks to ancillary innovations in traditional thyroid surgery in isolation: “A surgeon is a doctor who can operate and who knows when not to.” 4
Footnotes
Acknowledgment
Authors' Contributions
L.A.O. and S.P. were involved in conceptualization, original draft preparation, and writing—reviewing and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.