
Abstract

A
This 74-year-old woman was initially diagnosed with sMTC at 45 years of age, at which time she underwent total thyroidectomy and neck dissection. RET germline testing revealed no mutations. Her calcitonin became undetectable and carcinoembryonic antigen (CEA) normalized after surgery, from preoperative levels of 1180 pg/mL and 193 ng/mL, respectively. Nineteen years later, she had a biochemical relapse, reflected by a calcitonin measurement of 626 pg/mL and CEA of 10 ng/mL with computed tomography (CT) of neck, chest, and abdomen revealing left cervical neck adenopathy concerning for metastatic disease.
Due to progressive cervical lymphadenopathy on imaging, she underwent repeat neck dissection 21 years after her original surgery, confirming metastatic MTC in lymph nodes. Calcitonin declined to a nadir of 10 pg/mL with CEA of 2.3 ng/mL. She continued to follow annually with calcitonin, CEA, and thyroid ultrasound evaluations. CEA levels remained stable, while calcitonin slowly rose to 37 pg/mL over the next 7 years.
In February 2022, she presented with subacute onset of severe left lower posterior chest pain. Magnetic resonance imaging of the abdomen with and without contrast revealed significant metastatic disease progression: multiple lobulated confluent masses involving the left lung base/pleura (8 × 2 × 8 cm); enhancing masses adjacent to the thoracic aorta (2.1 cm), along the left lateral conal fascia (2.2 × 1.2 cm), left peritoneum; and left abdominal para-aortic enlarged lymph node (Fig. 1). Biopsy of the left pleural-based mass confirmed metastatic MTC (Fig. 2).
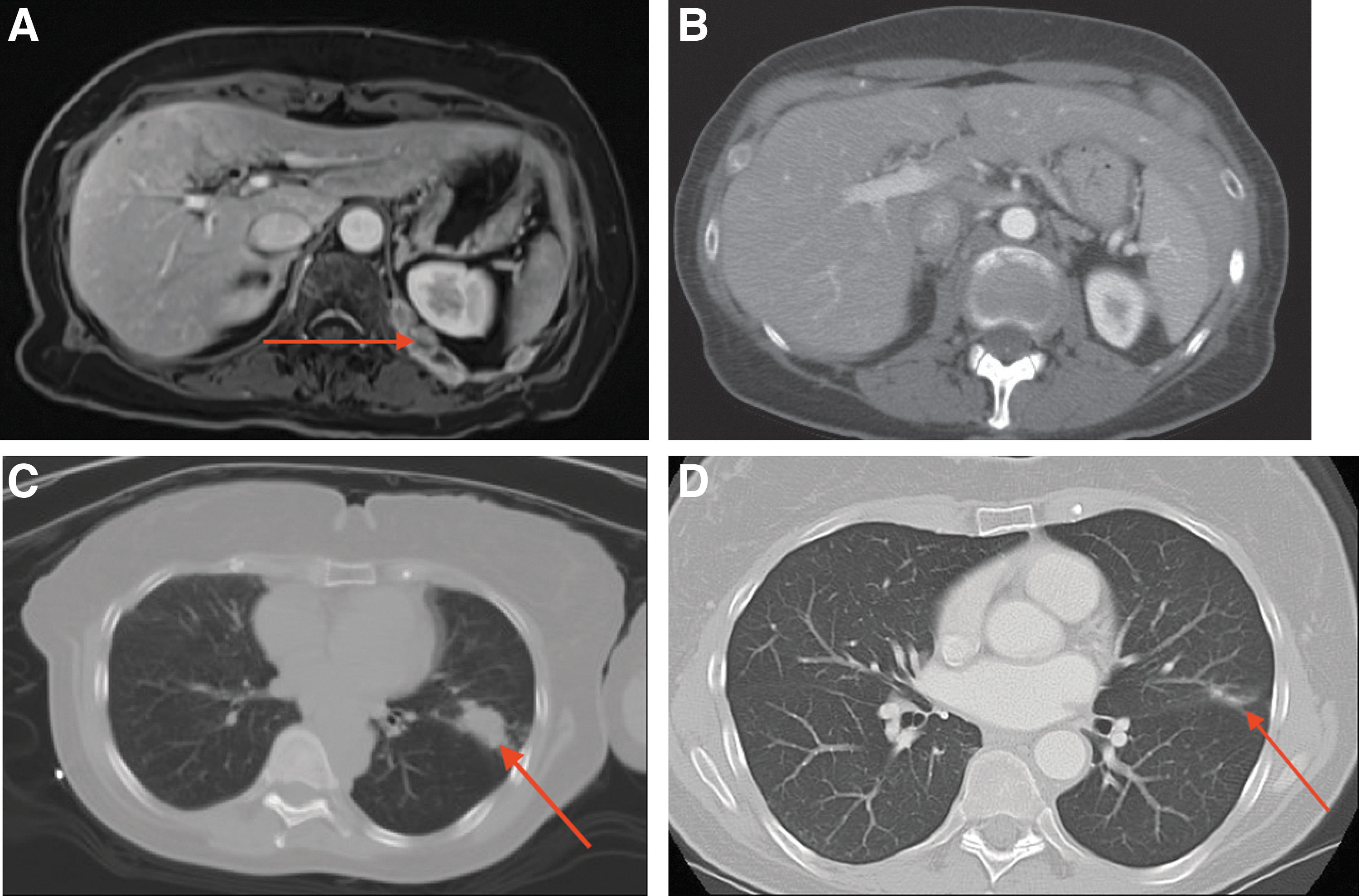
MRI and CT images before and after initiating NTRK-inhibitor treatment. (

Microscopic photographs of metastatic medullary thyroid carcinoma from biopsy of pleural-based mass. (
Calcitonin was 158 pg/mL and CEA was 22 ng/mL, suggesting poor differentiation. She had palliative radiation to the left pleural-based mass (800 CGy over 1 fraction). Molecular testing with next-generation sequencing (NGS) of DNA and RNA of the pleural biopsy specimen identified an ETV6-NTRK2 fusion, microsatellite-stable, tumor mutational burden low (1 mut/Mb), PD-L1 negative with no RET or RAS mutations identified. Exon 4 of ETV6 joined to exon 16 of NTRK2.
She was treated with entrectinib for five days, but was stopped due to constipation, fluid retention, syncope, and brain fog. Repeat scans after 5 days of entrectinib revealed resolution of peritoneal nodules and reduction of the left upper lobe lung mass from 2.7 × 1.5 to 1.9 × 0.8 cm, which was outside of the radiation field. Due to intolerance to entrectinib, larotrectinib was initiated at a low dose of 25 mg once daily, with titration up to 50 mg twice a day over 2 months. The patient declined the approved 100 mg twice daily dosing regimen due to concerns for possible adverse effects.
With larotrectinib 50 mg twice a day, CT scans of the thorax, abdomen, and pelvis 3 months later revealed resolution of the peritoneal nodules, decreased size of the left perifissural opacity from 1.9 × 1.8 to 0.7 × 1.5 cm, and decreased posterior mediastinal soft tissue adjacent to the descending thoracic aorta (Fig. 1). The patient had tolerable grade 1 adverse effect with generalized arthralgias. To the date of the writing of this report, the patient is continuing to take larotrectinib 50 mg twice a day, with a plan for consideration of dose escalation in the event of future disease progression.
RET germline mutation testing is recommended in all patients with MTC. 5 Somatic testing for RET is recommended by the National Comprehensive Cancer Network® Clinical Practice Guidelines in Oncology (NCCN Guidelines®) in MTC patients with germline RET wild-type or unknown status who demonstrate radiological progression for whom systemic therapy may be considered. 5 In addition to multikinase inhibitors approved for metastatic, progressive, or symptomatic MTC (cabozantinib and vandetanib), there are two highly selective RET inhibitors (pralsetinib and selpercatinib) approved by the FDA in 2020 for RET-mutated MTC.
Two NTRK inhibitors are currently FDA approved for any solid tumor with NTRK fusions, specifically entrectinib and larotrectinib. NTRK fusions are identified rarely in PTC, poorly differentiated and anaplastic thyroid carcinoma, but have not been reported until now in sMTC. In the larotrectinib and entrectinib trials, patients with non-MTC were found to have remarkable responses with low adverse event profiles. 6,7 Our patient, with an ETV6-NTRK2 fusion, had a rapid response with near complete resolution of metastatic lesions with larotrectinib at half of the approved treatment dose.
A better understanding of the genetic landscape offers hope for those with progressive MTC to identify potentially targeted therapy. In patients with progressive MTC that is not amenable to surgical or other focal therapies, we recommend that comprehensive NGS testing be performed (with consideration of examination for rare fusions with RNA sequencing), in pursuit of a targetable driver mutation.
Footnotes
Authors' Contributions
O.A. contributed to conceptualization, data collection, investigation, writing—original draft, review, editing, and approval. T.P. was involved in conceptualization, data collection, investigation, writing—original draft, review, editing, and approval. L.N. carried out data collection, writing—review, editing, and approval. M.I.H. was in charge of conceptualization, data collection, investigation, writing—original draft, review, editing, and approval.
Author Disclosure Statement
O.A., T.P., and L.N. have no conflicts to disclose. M.I.H. disclosures are steering committee Eli Lilly & Co (nonfinancial) and research support Eli Lilly & Co (financial support to institution not to author).
Funding Information
O.A., T.P., and L.N.: have no funding information to declare. M.I.H. has financial support to her institution by being part of research support for Eli Lilly & Co.