
Abstract
Background:
Between 10% and 15% of hypothyroid patients experience persistent symptoms despite achieving biochemical euthyroidism. Unexplained persistent symptoms can be a sign of somatization. This is associated with distress and high health care resource use and can be classified as somatic symptom disorder (SSD). Prevalence rates for SSD differ depending on classification criteria and how they are ascertained, varying between 4% and 25%. As this has not been studied in hypothyroid patients before, the aim of this study was to document somatization in people with hypothyroidism and to explore associations with other patient characteristics and outcomes.
Methods:
Online, multinational cross-sectional survey of individuals with self-reported, treated hypothyroidism, which included the validated Patient Health Questionnaire-15 (PHQ-15) for assessment of somatization. Chi-squared tests with the Bonferroni correction were used to explore outcomes for respondents with a PHQ-15 score ≥10 (probable somatic symptom disorder [pSSD]) versus a PHQ-15 score <10 (absence of SSD).
Results:
A total of 3915 responses were received, 3512 of which contained the valid PHQ-15 data (89.7%). The median score was 11.0 (range 0–30 [confidence interval 10.9–11.3]). The prevalence of pSSD was 58.6%. Associations were found between pSSD and young age (p < 0.001), women (p < 0.001), not working (p < 0.001), having below average household income (p < 0.001), being treated with levothyroxine (LT4) (rather than combination of LT4 and L-triiodothyronine [LT3], LT3 alone, or desiccated thyroid extract) (p < 0.001), expression of the view that the thyroid medication taken did not control the symptoms of hypothyroidism well (p < 0.001), and with number of comorbidities (p < 0.001). pSSD was associated with respondent attribution of most PHQ-15 symptoms to the hypothyroidism or its treatment (p < 0.001), dissatisfaction with care and treatment of hypothyroidism (p < 0.001), a negative impact of hypothyroidism on daily living (p < 0.001), and with anxiety and low mood/depression (p < 0.001).
Conclusions:
This study demonstrates a high prevalence of pSSD among people with hypothyroidism and associations between pSSD and negative patient outcomes, including a tendency to attribute persistent symptoms to hypothyroidism or its treatment. SSD may be an important determinant of dissatisfaction with treatment and care among some hypothyroid patients.
Introduction
Hypothyroidism is common affecting 1–7% of the population. 1 –3 Persistent symptoms occur in 10–15% of hypothyroid patients compared with controls. 4 –6 Hypotheses for the cause of these symptoms include: (a) inability of levothyroxine (LT4) to emulate normal physiology and restore L-triiodothyronine (LT3) at tissue level; (b) confounding effects of comorbidities; (c) autoimmune inflammation; (d) LT4 prescribed or taken by patients suboptimally; (e) people with unexplained symptoms being more likely to be investigated and diagnosed with minor and incidental perturbations of thyroid dysfunction; (f) the impact of the diagnostic label of chronic disease; and (g) somatic symptom disorder (SSD). 7 –9 Direct evidence to support the above propositions is unavailable, although it is likely that all are contributory.
In the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V), SSD refers to persistent bodily symptoms associated with significant functional impairment, psychological distress, and high health care resource use. 10 SSD is thought to result from an exaggerated awareness of bodily sensations, interpreted as being indicative of underlying disease. 11,12 The etiology of SSD is unclear, although associations with past traumatic experiences, personality traits, and psychosocial stresses have been described. 13,14 Genetic factors predisposing to bodily distress and to chronic pain may contribute. 15,16
SSD is a relatively recent classification, introduced in 2013 in the DSM-V. 10 Reviews describing prevalence rates of earlier classifications related to somatization (such as somatization disorder analyzing 32 studies from 24 countries), reported a pooled estimate of the point prevalence of 16.5%. 17 However, somatization disorder is a severe form of SSD and is limited to distress related to medically unexplained symptoms. In contrast, SSD relates to distress associated with physical symptoms in known medical conditions and medically unexplained symptoms and thus prone to have been underestimated.
A systematic review reported prevalence rates for somatoform disorders in the general population to range from 11% to 21% in younger, 10% to 20% in the middle-aged, and 1.5% to 13% in older age groups. 18 A 2022 review of 59 studies found a mean prevalence of SSD of 12.9% based on self-report. 19 A population-based study in more than 3000 people in Taiwan reported a prevalence of SSD of 5%, 20 and a German study of 1780 general practitioners reported a prevalence of SSD of 7.7% among their patients. 21 Based on the above findings, we can surmise that the prevalence of SSD in the general population is between 5% and 25%.
Studying SSD in hypothyroidism may help to understand the nature of persistent symptoms. Furthermore, identifying SSD may avoid unnecessary and expensive investigations, reduce the risk of inappropriate and harmful therapies, 22 –28 and direct patients and physicians to interventions shown to be helpful in SSD. 29
In this study, probable somatic symptom disorder (pSSD, defined as a score ≥10 using the Patient Health Questionnaire-15 [PHQ-15]) in patients with hypothyroidism was explored. The research questions were as follows: what is the prevalence of pSSD among patients with hypothyroidism, and what is the relationship between (a) pSSD and respondent characteristics and (b) pSSD and patient-reported outcomes?
Methods
Study design
Multinational, large-scale, cross-sectional, online questionnaire survey of people with a diagnosis of hypothyroidism. Some of the findings have been published. 30
Patient Health Questionnaire-15
The PHQ-15 is a questionnaire that is self-administered. It has been used in research and clinically as a screening test for somatization. 31 It includes 15 symptoms, which comprise the most frequent somatic complaints encountered in primary care. High scores correlate closely with somatoform disorder, disability, functional impairment, and use of health care resources. 31 This instrument has been validated and used extensively, 32 is equivalent or better in performance to other tools, and is recommended by the American Psychiatric Association. 10 The PHQ-1531 has a sensitivity of 78–83% and a specificity of 42–71% for somatization 33,34 and is well suited for use in large-scale studies internationally. 35 The PHQ-15 lists 15 somatic symptoms, 13 of which are related to physical symptoms, while 2 (feeling tired or having little energy, and trouble sleeping) are associated with depression. 31,32
Each symptom is scored as 0, 1, or 2 (“not bothered at all,” “bothered a little,” “bothered a lot,” respectively). The sum score is used as a measure for symptom load. A score of ≥10 is associated with somatization equivalent to clinical disorder. 31 In this study, values of the PHQ-15 were considered valid when the provided answers were undoubtedly ≥10 or <10. Therefore, respondents with a PHQ-15 score of ≥10 were included even if they did not respond to all questions of the PHQ-15 and categorized as having pSSD. Respondents whose scores could not exceed 9 even if the missing data scored maximally were included and categorized as not having SSD. Respondents who had left out parts of the PHQ-15 and could have attained a score indicating SSD were excluded as we could not undoubtedly attribute their responses. pSSD (score ≥10) was used as a research classification rather than a medical diagnosis of SSD.
Questionnaire
The questionnaire was cognitively tested in 30 English-speaking patients with hypothyroidism across 5 rounds in accordance with published methodology. 36 Minor changes were made to establish consistent comprehension. Translations of the English version of the questionnaire were made into French, German, Italian, and Spanish. Each translation was performed by two certified native translators. Idioms were replaced with appropriate alternatives. A pilot was conducted in English with 387 respondents (344 completed and 43 partially completed) for data validation, which demonstrated good face validity and response. The final version took 30–45 minutes to complete and was hosted online in Qualtrics between April 11, 2020, and January 3, 2021 (Supplementary Data).
Dissemination
Advertisements and information sheets to explain the purpose of the survey were prepared in the aforementioned five languages and promoted through Thyroid Federation International, a global network of patient thyroid disorder organizations, affiliates, and partners via social media and web pages (Supplementary Fig. S1).
Inclusion criteria
Participants had to be ≥18 years and to be using medication for hypothyroidism.
Institutional review board waiver statement
The non-interventional nature of the survey and the fact that data were anonymized rendered the study exempt from institutional board approval. The study was conducted in accordance with Declaration of Helsinki as revised in 2013. All participants gave informed consent.
Statistical analyses
The data set was calculated to detect a delta of 0.1 in proportions for z-tests, using GPower3.1.9 for a power of 95% and alpha set at 0.05, which calculated the number of participants to be around 1000 (1066). Chi-squared tests with the Bonferroni correction were used, via Python 3.10. A binary PHQ-15 score <10 or ≥10 (corresponding to the absence or presence of pSSD) was used as an independent variable and was compared against 10 dependent variables comprising demographic and other baseline characteristics (gender, age, marital status, employment, ethnicity, years in education, household income, comorbidities, cause of hypothyroidism, treatment for hypothyroidism). In addition, the PHQ-15 binary score was compared against five respondent outcomes:
Results
Respondent baseline characteristics
A total of 3912 responses were received, 3512 of which contained the valid PHQ-15 data (89.7%) (Table 1). Women comprised 94.4% (3317/3512) of respondents. Most respondents (87.2%; 3063/3512) were older than 30 years. Responses from the United Kingdom dominated (35.6%; 1249/3512). The majority of respondents were white (86.5%; 3039/3512), employed (71.9%; 2524/3512), had received more than 8 years of education (84.45%; 2966/3512), had comorbidities (72.9%; 2560/3512), and were treated with LT4 (75.8%; 2662/3512).
Baseline Respondent Characteristics
Causes in free text included: “radiation,” “radiotherapy,” “stress,” “viral,” “injury to the thyroid,” “puberty,” “menopause,” “eating disorder,” “none,” “levothyroxine brand switch,” “insulin resistance,” “endocrine disruption,” “fluoridation,” “flu vaccine,” “gallbladder surgery,” “Hereditary,” “genetic,”“hormonal contraceptive,” “allergy,” “aging,” “leaky gut,” ‘hysterectomy,” “mono,” “quitting smoking,” “sluggish thyroid,” “antibiotics,” “Yodo,” “hypothyroidism.”
DTE, desiccated thyroid extract; LT3, L-triiodothyronine; LT4, levothyroxine.
Prevalence of pSSD
The median PHQ-15 score was 11.0 (range 0–30 [confidence interval 10.9–11.3]). Women respondents (n = 3317) had higher PHQ-15 score than men (n = 164) (mean 11.3, standard deviation [SD] 5.7 vs. mean 7.6, SD 5.6, respectively, p < 0.001). Tiredness was the most common symptom experienced by 90.3% (3161/3501) of respondents (Supplementary Table S1).
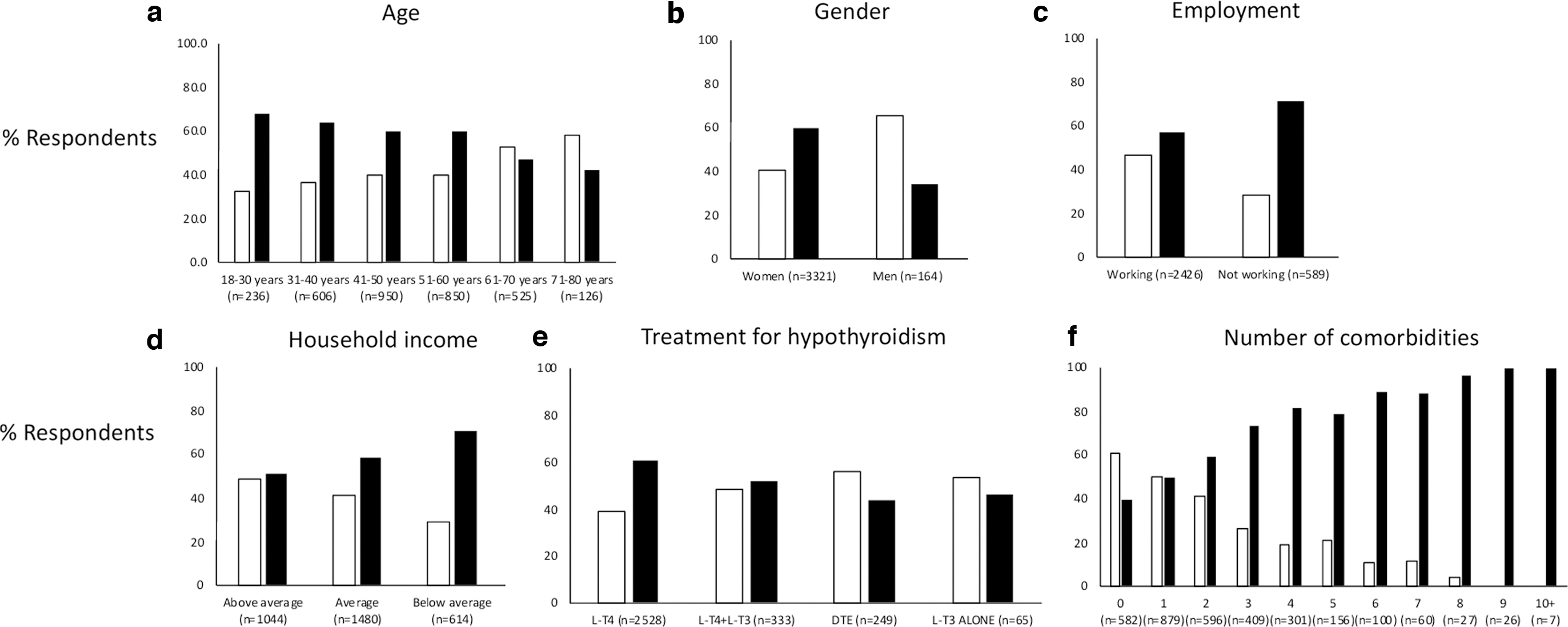
Associations between pSSD and demographic and other baseline characteristics
Significant associations with pSSD were found with age, gender, employment status, household income, treatment for hypothyroidism, and number of comorbidities (Table 2). By binary categorization into PHQ-15 scores <10 and ≥10, the following groups were identified as having higher pSSD prevalence: aged 18–30 years, women, not working, having below average household income, being treated with LT4 (compared with combination of LT4 and LT3, LT3 alone, or desiccated thyroid extract) (Table 2; Supplementary Table S2), and having one or more comorbidities (Fig. 1). No associations were found between pSSD and marital status, years of education, cause of hypothyroidism, and ethnicity.
Association between pSSD (PHQ-15 score ≥10) and respondent characteristics: (
Chi-Squared Analysis for Independent Variables Against Patient Health Questionnaire-15 Scores <10 and ≥10
The adjusted threshold by the Bonferroni method was for the p level of 0.001667.
Associations between pSSD and respondent attributions of causes of symptoms
There was a significant association between pSSD and attribution of symptoms to hypothyroidism or its treatment for 13 of the 15 symptoms, the non-significant symptoms being “fainting spells” and “pain or problems during intercourse” (Fig. 2 and Table 3). Respondents with pSSD were equally likely to blame hypothyroidism or its treatment for typical hypothyroid symptoms (such as constipation, tiredness, or atypical symptoms, such as, stomach pain, backache, or dizziness.) 37,38
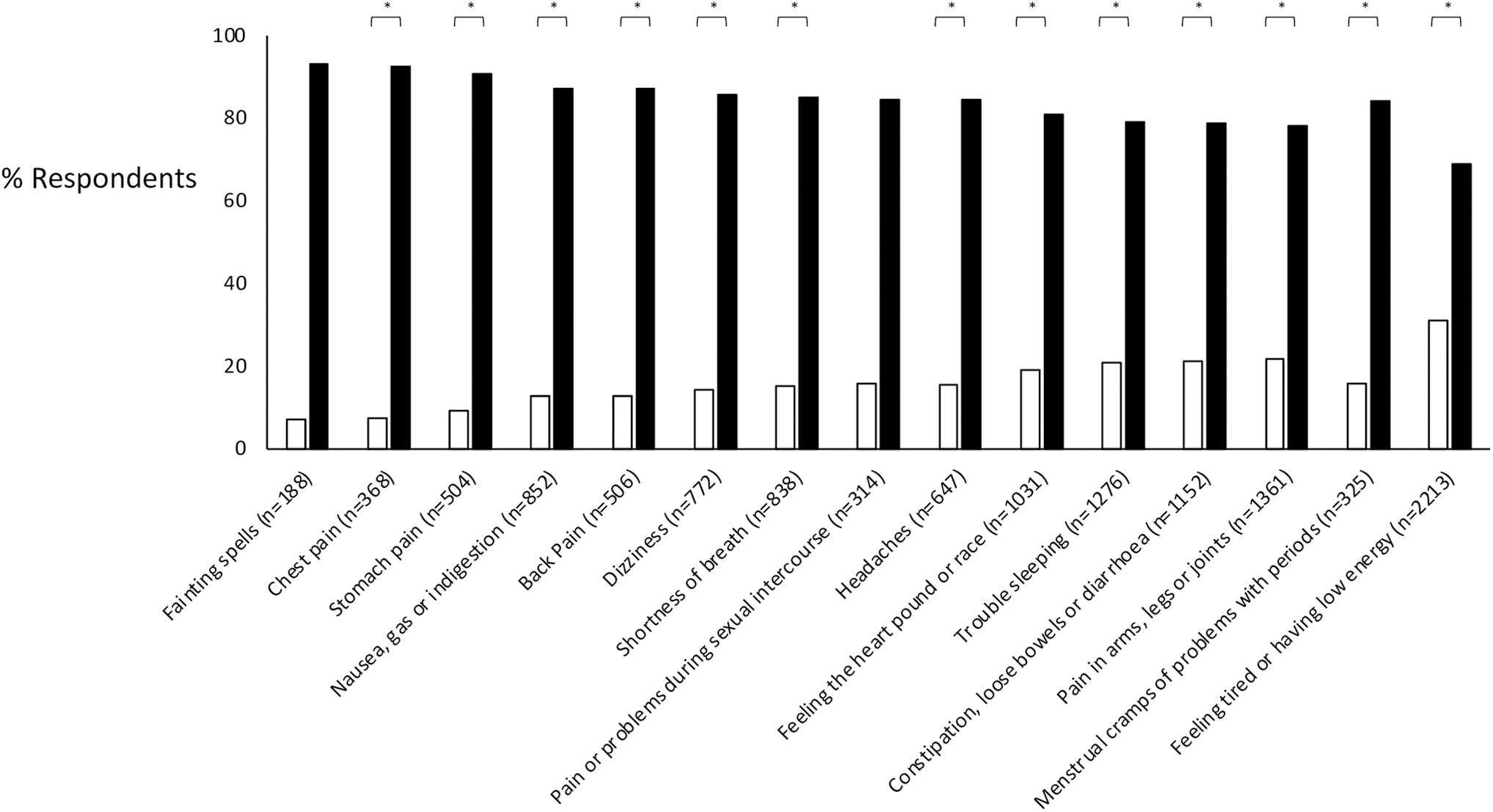
Attribution of the PHQ-15 symptoms by respondents to hypothyroidism or its treatment. Respondents were asked to indicate if they attributed the symptom to the hypothyroidism or its treatment, or to other causes. Data are shown for those respondents who attributed their symptoms to hypothyroidism or its treatment, by severity of somatization as expressed by PHQ-15 score <10 (white bars) and PHQ-15 score ≥10 (black bars). For each pair of bars, the number of observations (n) is also provided. Comparison between white and black bars was statistically significant at p < 0.001 for all symptoms except “fainting spells” and “pain or problems during intercourse.” The figures in brackets shown in the horizontal axis indicate the number of respondents who had each symptom. The number of valid responses (Table 2) for each symptom is shown in Supplementary Figure S1.
Attribution of Respondents' Symptoms to Hypothyroidism or Its Treatment
Respondents who had one or more of the symptoms listed in the PHQ-15 questionnaire (scored as “bothered a little” or “bothered a lot”) were further asked to indicate whether they attributed the symptom to “hypothyroidism or its treatment” or to other causes. Respondents were categorized as not having SSD if their PHQ-15 score was <10 and as having pSSD if their PHQ-15 score was ≥10. Comparisons in attribution of symptoms were made between respondents with pSSD with those without SSD by chi-squared tests with the Bonferroni correction. The chi and p-values for the comparisons are shown below. The adjusted threshold by the Bonferroni method was for the p level of 0.001724.
PHQ-15, Patient Health Questionnaire-15; pSSD, probable somatic symptom disorder; SSD, somatic symptom disorder.
Association between pSSD and control of symptoms of hypothyroidism
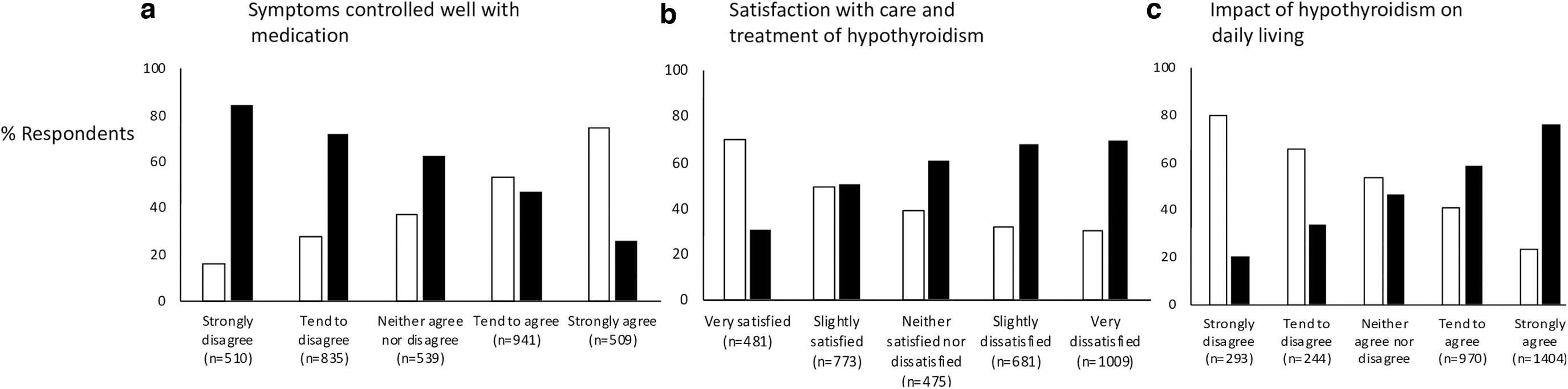
pSSD was associated with the expression of the view by respondents that the thyroid medication taken did not control the symptoms of hypothyroidism well (Fig. 3a and Table 2).
Association between pSSD (PHQ-15 score ≥10) and (
Association between pSSD and satisfaction with care and treatment of hypothyroidism
There was a significant association between pSSD and dissatisfaction with care and treatment of hypothyroidism (Fig. 3b and Table 2).
Association between pSSD and impact of hypothyroidism on daily living
There was an association between a negative impact on daily living and pSSD (Fig. 3c and Table 2).
Anxiety, low mood/depression
Both anxiety and low mood/depression were prevalent in respondents with pSSD (82.6%, 1689/2046, and 84.9%, 1739/2049, respectively), and the association was statistically significant (Table 2).
Discussion
SSD is common, associated with persistent symptoms, individual and societal burden, high levels of health care utilization and economic cost. 39 Yet there is little information in the literature about SSD in hypothyroidism, 40,41 while impaired quality of life and dissatisfaction with care and treatment are well documented. 42 –45 We used the validated PHQ-15 questionnaire 31 to assess somatization and to test the hypothesis that SSD is a contributor to persistent symptoms and dissatisfaction. We have used pSSD as a research classification based on self-reported responses to a questionnaire, to gain insights on the nature of persistent symptoms in hypothyroidism. It should be noted that this is not equivalent to a medical diagnosis of SSD (which requires individual assessment by an expert). Respondents' characteristics were similar to hypothyroid patient populations reported in the literature. 1,2,46 –48 The PHQ-15 has been used previously to screen for SSD, 31,49,50 study associations between somatic symptoms and demographic factors 51 and behaviors 52 and quantify somatic distress associated with specific diseases such as diabetes, 53 thus providing potentially useful insights.
The proportion of respondents with pSSD was higher (58.6%) than normative data (7.2%) (Supplementary Table S3). 54 SSD is common among patients with chronic diseases; 55 –57 thus, it is not surprising that this was also the case in hypothyroidism. The significance of this finding rests with how clinicians approach the common scenario of hypothyroid patients with persistent unexplained symptoms. Research in Europe conducted in 2019–202158–77 shows that thyroid specialists usually offer pharmacological solutions to such patients in the form of combination therapy of LT4 with LT3, despite evidence from randomized controlled studies indicating no benefit from combination treatment compared with LT4 alone. 9,45 In the light of these findings, a pharmacological approach is inappropriate for some of these patients, as their underlying psychosocial needs will not be addressed.
The high prevalence of pSSD among participants demonstrated in this study does not support binary “mind” versus “body” dualism, which sometimes leads to dismissive attitudes by health care professionals toward patients with unexplained symptoms. On the contrary, the findings suggest that a biopsychosocial approach 78 to the conundrum of persistent symptoms despite euthyroid biochemistry may be appropriate. The experience of health care professionals who manage patients with unexplained persistent symptoms suggests that they may respond to empathetic listening, affirmation that their symptoms are real, explanations that physical and psychological symptoms are intimately integrated, avoidance of over-investigation and use of cognitive behavioral and other established psychological therapies, ideally in a multidisciplinary setting. 79,80
In our study, pSSD was associated with young age, women, low household income, employment status, and multiple comorbidities. Some of these variables are likely to be interdependent; however, the above findings are in keeping with other studies of SSD in general populations. 81 –84 The association between pSSD and treatment with LT4 as opposed to LT3-containing treatments may indicate that hypothyroid patients treated with LT3-containing medication become less symptomatic than those treated with LT4, particularly if overtreated (e.g., observations of beneficial effects of high doses of LT3 on mood in patients with resistant depression 22 ). However, the association between pSSD and LT4 treatment cannot be assumed to be causal, nor is it possible to infer from these data that LT3-containing treatments should be used to provide relief from the symptoms of SSD.
pSSD was associated with attribution of persistent symptoms to hypothyroidism or its treatment, including symptoms not recognized to be associated with hypothyroidism or thyroid hormone replacement. Among the symptoms included in the PHQ-15, tiredness and pain were the most frequently reported symptoms. This aligns with findings that somatization symptoms tend to cluster into four groups: fatigue, pain, cardiorespiratory, and bowel symptoms. 85 The high prevalence of pain symptoms, especially back pain and headaches in this sample is consistent with the Global Burden of Disease study. 86 Patients with SSD who experience back pain and headaches that cluster with fatigue may attribute symptoms that occur frequently in the general population to hypothyroidism. The above findings are consistent with insights from other studies relating to the symptomatology of hypothyroidism and how symptoms may be perceived by patients, particularly in view of the fact that most of the symptoms of hypothyroidism are nonspecific and often experienced by the euthyroid population. 37
A study of patients with subclinical hypothyroidism who were not aware of their serum thyrotropin (TSH) levels showed no difference in symptoms compared with euthyroid controls. 87 In another study, patient awareness that they had a thyroid diagnosis was associated with an increased prevalence of symptoms, and conversely, in patients not aware that they had a thyroid diagnosis, a higher serum TSH was associated with fewer symptoms. 6 Self-knowledge of a diagnosis of hypothyroidism therefore seems to be an important factor in how symptoms are perceived and experienced. Another important factor is that recent studies indicate that the majority of patients diagnosed and started on thyroid hormone replacement have mild or subclinical hypothyroidism, 88,89 or even transient elevation in serum TSH. 90 Furthermore, several studies and meta-analyses show similar rates of symptoms in subclinical hypothyroid patients as in euthyroid controls. 45,91
An association was found between pSSD and respondent opinion that the thyroid medication taken did not control their symptoms of hypothyroidism well, which could be indicative of a patient belief that all or most persistent symptoms experienced are due to hypothyroidism. This is likely to be false given that persistent symptoms such as those included in the PHQ-15 questionnaire occur in the background general population and particularly in patients with comorbidities other than hypothyroidism. In this respect, it is of interest that evidence from another survey of hypothyroid women indicates that patient beliefs about the nature of their illness may play a role in the development of symptoms, such as depression, anxiety, and anger. 92
The association between dissatisfaction with care and treatment of hypothyroidism and pSSD parallels those described for medically unexplained symptoms in general 93 and may reflect the frustrating nature of persistent symptoms and inadequacy of available services. Similarly, the association between pSSD and a negative impact of hypothyroidism on daily living was significant and may be subject to patients' attributions of symptoms to hypothyroidism. As SSD is usually established by the age of 30 years, 39 in most cases, it precedes the onset of hypothyroidism by 1–2 decades 1 and therefore may be a causal contributor to the phenomenon of persistent symptoms in some patients who are given the diagnosis of hypothyroidism.
The prevalence of self-reported anxiety and low mood/depression among respondents with pSSD was high (72.3% and 71.8%, respectively). It should be noted that these were not medical diagnoses of anxiety or depression, but a research classification self-report. The fact that the survey was carried out during the COVID pandemic may have increased anxiety and low mood/depression and could explain the above high levels. However, an association between hypothyroidism and psychiatric morbidity (including use of anxiolytic and antidepressant medication) has been noted before and seems to hold true both before and after the diagnosis of hypothyroidism. 28 An association between SSD and anxiety and depression is well established in the general population. 94 Our findings suggest that hypothyroid patients presenting with symptoms of SSD have a high likelihood of an underlying anxiety or mood disorder, which is important for clinicians managing patients with hypothyroidism to be aware of.
The cause of persistent symptoms in patients with hypothyroidism is still unknown, a causal relationship with SSD is not established and underlying biological explanations are also plausible. However, our findings are of importance in the management of patients with hypothyroidism and indicate that somatization plays a significant role in the presentation of some of these patients.
The study has limitations. Some nations were overrepresented, the data were self-reported, respondents were invited via patient organizations and social media, there was some sample heterogeneity, the assessments of quality of life, anxiety, and low mood/depression did not utilize validated instruments, informative data on cause of hypothyroidism were unavailable in 28.5% of responses, directly comparative data on prevalence of pSSD in a control population were unavailable, and we had no access to thyroid biochemistry. The high percentage of pSSD needs to be taken in the context of the fact that only a minority (10–15%) of hypothyroid patients report impaired quality of life, 46 and dissatisfied patients are more likely to respond to surveys. 30,43,44 In mitigation of the above, the large sample size, cognitive testing, piloting, and inclusion of a patient representative in the research team were the strengths.
In conclusion, this study demonstrates a high prevalence of pSSD among people with hypothyroidism who responded to the survey, a tendency to attribute persistent symptoms to hypothyroidism or its treatment and associations between pSSD and negative patient outcomes. SSD may be an important determinant of dissatisfaction with treatment and care among some hypothyroid patients. Our findings require independent confirmation with studies that focus on SSD and address the limitations outlined above. Close collaboration between the disciplines of thyroidology, psychology, and sociology is likely to be key in progressing our understanding in this area.
Footnotes
Acknowledgments
The authors wish to thank the patient organizations and their members for disseminating the survey and for responding to the questionnaire.
Authors' Contributions
P.P.: Conceptualization (lead), methodology (equal), supervision (equal), writing—review and editing (lead). L.H.: Conceptualization (equal), funding acquisition (lead), methodology (equal), review and editing (equal). E.V.N. and E.P.: Conceptualization (equal), methodology (equal), review and editing (equal). C.M.V.D.F.-C.: Methodology (equal), review and editing (equal). A.P.W.: Review and editing (equal). H.A.H.: Data curation (equal), investigation (equal), methodology (equal), project administration (lead), supervision (equal), review and editing (equal). J.A.-M.: Data curation (equal), review and editing (equal), project administration (equal). A.J.T.: Investigation (lead), methodology (lead), project administration (equal), supervision (lead), review and editing (equal). M.B.: Investigation (equal), methodology (equal), project administration (equal), supervision (equal), review and editing (equal). P.L.: Resources (lead), methodology (equal), review and editing (equal), investigation (equal). A.J.P.: Methodology—review and editing (equal), formal analysis (lead), review and editing (equal).
Author Disclosure Statement
P.P., E.V.N., E.P., and A.P.W. report honoraria from IBSA Institut Biochimique SA. L.H. reports honoraria from IBSA Institut Biochimique SA, Lundbeck, Horizon, Merck, and Berlin Chemie. C.M.V.D.F.-C. reports honoraria from Lloyds Register Foundation and Janssen UK. H.A.H., J.A.-M., A.J.T., M.B., P.L., and A.J.P. report no competing financial interests.
Funding Information
This study was funded by IBSA Institut Biochimique SA, (grant no.: 4500131227) who had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Data