
Abstract

N
The proband was a term female infant, small-for-gestational age, with hyperthyroidism diagnosed at 5 months of age due to poor weight progression, persistent tachycardia, advanced bone age, and premature fontanelle closure. The family history was negative for thyroid disease. Antithyroid drug (ATD) therapy was initiated for presumptive treatment of Graves' disease. Uncontrolled hyperthyroidism and goiter were treated with a subtotal thyroidectomy at the age of 6 years. She remained hyperthyroid despite under ATD (propylthiouracil [PTU]) and two courses of ablative radioactive iodine therapy during adulthood. A computed tomography scan revealed the presence of a large mediastinal thyroid mass. Surgical removal of the mass led to clinical remission.
At the age of 33 years, she had a first spontaneous pregnancy, complicated by moderate fetal cerebral ventriculomegaly at 24 weeks of gestation. The pregnant woman was referred to medical genetics since amniocentesis for prenatal diagnosis revealed no karyotype [46,XX] nor microarray abnormalities. Sanger sequencing of TSHR from a blood sample from the pregnant patient disclosed a heterozygous gain-of-function pathogenic variant in exon 10—NM_000369.2:c.1358T>Cp.Met453Thr—confirming the diagnosis of NAH. Genetic testing of her asymptomatic parents established de novo occurrence. During the pregnancy, the fetal phenotype progressed to severe ventriculomegaly, hepatosplenomegaly, atrophic kidneys, oligoamnios, and tachycardia (200 beats per minute [bpm]), and ultimately delivery of a stillbirth. Heterozygosity for the maternal TSHR pathogenic variant was then disclosed.
The proband had a second planned pregnancy at the age of 34 years, while taking adequate thyroid replacement therapy. At 14 weeks of gestation, fetal tachycardia was observed (180 bpm—fetal heart rate [FHR] above 95th percentile). Amniocentesis was performed at 18 weeks and Sanger sequencing of fetal DNA confirmed the diagnosis of NAH. Fetal tachycardia and genetic testing were suggestive of fetal hyperthyroidism with presumptive poor prognosis inferred by the previous unsuccessful pregnancy. At 22 weeks of gestation, maternal treatment with MMI was initiated (10 mg daily) with the intention of transplacental fetal treatment. Ultrasound surveillance and weekly FHR monitoring was performed to inform MMI dose titration (Fig. 1). At 24 weeks, the echocardiogram showed no signs of heart failure, and the ultrasound scan showed a fetus with good vitality, normal morphology without goiter, and normal amniotic fluid volume.
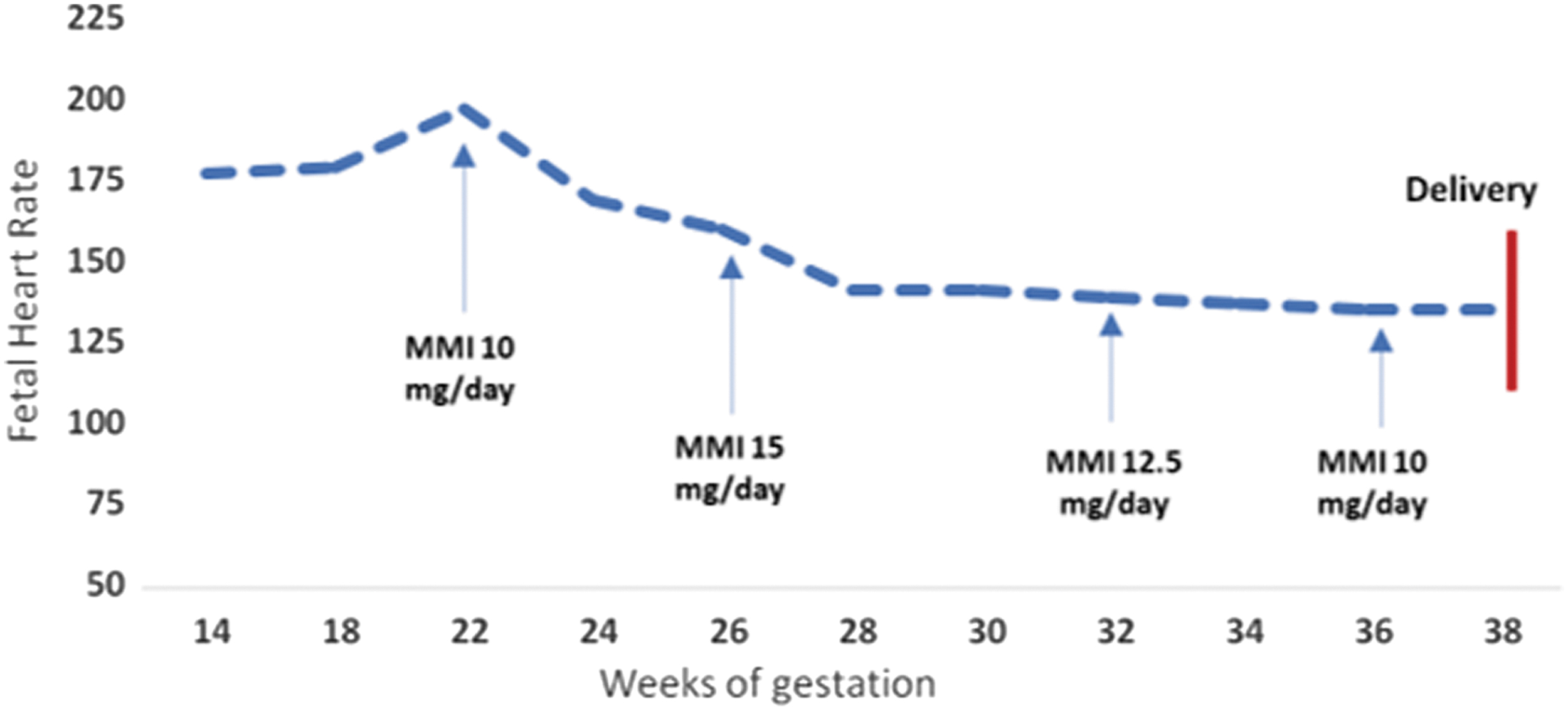
Fetal heart rate during pregnancy. MMI, methimazole.
At 38 gestational weeks, a female appropriate-for-gestational-age baby was successfully delivered by urgent caesarean section due to preeclampsia. MMI was discontinued upon delivery and the mother maintained normal TSH levels (2.47 μUI/mL) on levothyroxine replacement therapy (88 μg daily). The neonate had no goiter. Thyroid function was assessed within the first 24 hours (TSH <0.005 μUI/mL [0.72–11.0], free thyroxine [fT4] 5.46 ng/dL [0.89–2.20], and free triiodothyronine 13 pg/mL [1.73–6.30]), which led to the prompt initiation of MMI therapy (1.5 mg daily, 0.5 mg/[kg·day]), with a favorable clinical response. At 5 months of age, the child remained clinically euthyroid (TSH <0.005 μUI/mL, fT4 1.83 ng/dL, and total triiodothyronine 2.70 ng/mL), with a heart rate of 138 bpm and adequate physical and psychomotor development, while taking MMI 0.6 mg daily.
Prenatal management of fetal hyperthyroidism was particularly challenging in the described case, given the early presentation, poor outcome of the first gestation, and the rarity of the prenatal onset of this condition. 4 The multidisciplinary team chose to initiate MMI, known to have a higher transplacental passage than PTU and lower risk of maternal liver toxicity. 5 This report highlights the importance of multidisciplinary care for accurate diagnosis of NAH and its treatment.
Footnotes
Acknowledgments
The authors wish to thank the proband and her family for permission to report the cases.
Authors' Contributions
S.S.M. reviewed literature, was involved in the multidisciplinary care team that managed the second pregnancy, and drafted the article. M.P.M. was involved in diagnosis, managed the patient since early adulthood, and substantially contributed to article revision. G.I. was the attending obstetrician during the first and second pregnancy and monitored treatment by ultrasound. T.B. was involved in the multidisciplinary care and subsequent follow-up of the newborn. S.G., M.T.P., and J.V. were attending endocrinologist during the second pregnancy. M.S. was attending obstetrician during the second pregnancy. C.P. was attending obstetrician during the first and second pregnancy. M.d.C.R. was attending obstetrician during the first pregnancy. L.G.-M. performed fetal heart evaluation during the second pregnancy and was involved in the multidisciplinary care team. J.D. was involved in the multidisciplinary care team leading the endocrinology team, and critically reviewed the article. C.F.R. was involved in the diagnosis and in the coordination of the multidisciplinary care team, and drafted and critically reviewed the article.
All authors read and approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.