
Abstract
Background:
Image-guided thermal ablation interventions are novel thermal-based modalities used for the treatment of benign thyroid nodules.
Methods:
We conducted a systematic review and a Bayesian network meta-analysis, examining studies using thermal ablation interventions in the treatment of benign nodular thyroid disease (PROSPERO CRD42022367680). The primary endpoints included volume reduction rate (VRR), and symptomatic score and cosmetic score improvement. Secondary endpoints included vocal disturbances, laryngeal nerve palsy, hypothyroidism, and nodular regrowth (defined by increased nodular volume of >50% for thermal ablation or new nodules arising in remaining thyroid tissue conventional surgery [CS]).
Results:
We included 16 studies (3 randomized controlled trials [RCTs] and 13 comparative case series), describing radiofrequency ablation (RFA), laser ablation (LA), microwave ablation (MWA), high-intensity focus ultrasound (HIFU), and CS, respectively. The review included data from 4112 patients followed for a mean of 11.9 months. Meta-analyses showed no significant differences among RFA, LA, MWA, HIFU, and CS regarding any of the primary endpoints of VRR, symptomatic score, and cosmetic score. In examining the surface under the cumulative ranking area (SUCRA) ranking, CS (SUCRA, 98.49), LA (SUCRA, 51.58), and MWA (SUCRA, 57.0) were identified as the three interventions that were most likely to result in the largest VRR, symptomatic and cosmetic score reduction. RFA, relative risk (RR) 0.19 [95% credibility interval (CI): 0.06 to 0.48], LA RR 0.23 [CI: 0.06 to 0.79], and MWA RR 0.25 [CI: 0.09 to 0.60] were associated with the greatest reduction in risk for postintervention vocal complications compared with CS, with RFA (SUCRA, 61.62) being ranked as the highest in safety. RFA RR 0.05 [CI: 0.00 to 0.40] and MWA RR 0.16 [CI: 0.02 to 0.73] were associated with a reduced risk of transient laryngeal nerve injury compared with CS. RFA RR 0.00 [CI: 0.00 to 0.00] and MWA RR 0.00 [CI: 0.00 to 0.03] were associated with a reduced risk of hypothyroidism occurrence compared with CS, with RFA (SUCRA, 99.86) yielding the highest safety ranking. RFA was associated with a reduced risk for nodular regrowth RR 0.09 [CI: 0.00 to 0.85], compared with CS.
Conclusion:
We have comprehensively reviewed the published literature on the efficacy and safety of thermal ablation modalities for benign thyroid nodules. Important research gaps remain regarding a paucity of both long-term data and high-quality RCTs.
Introduction
Nodular thyroid disease (NTD), which is frequently diagnosed during a routine ultrasound examination, is a common clinical disorder with a prevalence ranging from 20% to about 70%. 1 The majority of thyroid nodules are benign (90%), asymptomatic, and only require annual surveillance. 1 –3 Despite its predominantly benign nature, NTD can result in compressive symptoms, potentially eventually necessitating surgical treatment. While total thyroidectomy is the mainstay treatment in the surgical management of NTD, limitations, including unsatisfactory cosmetic outcomes, vocal disturbances, and postsurgical hypothyroidism, remain areas of concern. 4 In the past, noninvasive treatments such as radioiodine therapy and thyrotropin (TSH) suppression therapy have been used to manage NTD. Even though they are noninvasive, these techniques are not recommended due to their limited efficacy and the occurrence of thyroid dysfunction. 2,5
Image-guided thermal ablation, including radiofrequency ablation (RFA), laser ablation (LA), microwave ablation (MWA), and high-intensity-focus ultrasound (HIFU), is a group of novel thermal ablation modalities intended to provide a safe and efficacious treatment option for NTD, while mitigating the risks associated with thyroid surgery. 6 –9
While the overall principle is similar, the various thermal ablation modalities differ in their technical aspects. RFA operates through a radiofrequency-generated oscillating current that passes through an electrode needle to the targeted tissue, vibrates the polarized molecules and ions, and is finally converted to thermal energy. 10,11 MWA is based on microwave-generated energy delivered to thyroid nodules and the “moving-shot technique” is applied until destruction of tissue is achieved. 10,11 In LA, a beam of light energy is delivered through a needle to the center of the targeted tissue inducing heat-related changes in thyroid nodule. 10,11 Finally, HIFU operates by the conversion of acoustic to thermal energy. 10,11 It induces a focused thermal destruction of tissue with temperatures of up to 85°C without needle insertion. 10
When various therapies for a condition are available, the construction and implementation of multiarm high-quality randomized control trials (RCTs) or comparative studies are a rather challenging task. In addition, conventional meta-analyses, which summarize evidence from published studies, are confined to pairwise, head-to-head comparisons, ultimately failing to incorporate indirect evidence. Network meta-analyses (NMAs), throughout their ability to integrate both direct and indirect evidence (i.e., incorporating data from treatments that may have never been compared), provide global estimates regarding the application of various treatment methods for a given disease.
The aim of the present study is to perform a systematic review and NMA, investigating the efficacy and safety of all the available ultrasound-guided thermal ablation techniques for treatment of benign NTD, in comparison with conventional surgery (CS).
Methods
Eligibility criteria
The systematic review included RCT and comparative cases series that reported on surgical or minimally invasive interventions for the treatment of benign thyroid nodules. Studies were required to include more than 20 patients per treatment arm.
Studies in which the treatment arms failed to form a closed network loop not allowing for the consistency and transitivity assumption to be assessed, as well as studies where one of the two comparative arms referred to a control (nonintervention) group, were excluded.
Information sources and search strategy
A systematic review according to the instructions by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement 2020 and the PRISMA NMA 2015 extension was performed. 12,13 A search of Medline, Scopus, and Google Scholar was conducted by two investigators A.C., and V.B. for articles published from inception through August 2022. Both researchers used identical structured vocabularies complemented with keywords (details of the search are reported in the Supplementary Methods). The systematic review was registered a priori in the Prospective Register of Systematic Reviews (PROSPERO, CRD42022367680). The study was exempt from the need for Institutional Review Board approval as it was a review of published literature.
Selection process and data collection process
Two investigators (A.C. and V.B.) independently assessed the titles and abstracts of the retrieved literature and retrieved relevant full-text publications. Full-text publications were independently evaluated by both researchers for inclusion in the systematic review. When a disagreement arose, a consensus was reached through discussion with a third researcher (G.T.). A table including excluded studies with reasons is provided (Supplementary Table S1).
Data items
The primary endpoints included short-term volume reduction rate (VRR), and symptomatic score and cosmetic score improvement at last follow-up. Secondary endpoints included vocal complications, laryngeal nerve injury, postprocedural hypothyroidism, and nodular recurrence.
Definitions
VRR is formulated as follows: (initial volume – final volume) × 100/initial volume (%). Nodule volume is calculated by the following: volume (mL) = [width (cm) × length (cm) × depth (cm)] × (π/6) where π was 3.1416. 11 Symptomatic scores were self-reported patient measurements on a visual analog scale (scores ranged from 0 least severe to 10 most severe). 11 The cosmetic scores were based on a physician-evaluated scale ranging from 1 to 4 (1—no palpable mass; 2—palpable mass but no cosmetic problems; 3—cosmetic problem on swallowing only or detected by an experienced physician; and 4—a readily detected cosmetic problem). 11 Vocal complications were defined as any newly detected vocal changes including hoarseness of voice or dysphonia following the intervention, while laryngeal nerve injury was defined as any incident of injury to the laryngeal nerve identified through laryngoscopy by an ear, nose, and throat professional. 14
Hypothyroidism was defined as biochemical values of TSH, greater than the upper normal limit set by the given laboratory and free triiodothyronine and free thyroxine values lower than the lower normal values. 15 For comparisons regarding VRR and CS, CS was assigned to a median value of 99% (interquartile range: 98–100) volume reduction by the end of follow-up. We defined recurrence or regrowth as increased nodular volume by >50% compared with the latest ultrasonographic examination for image-guided thermal ablation interventions, the appearance of newly formed nodules in the contralateral lobe for surgical lobectomy, and nodular regrowth arising from the residual tissue in the cases of subtotal and total thyroidectomy. 16 –18
Effect measures and synthesis methods
We performed a Bayesian NMA using both the BUGSnet and GeMTC packages employing the Markov chain Monte Carlo simulation with vague priors for posterior distribution estimation of the incorporated parameters. The generalized linear model with four chains, burnings of 50,000 iterations accompanied by 100,000 iterations with 10,000 adaptations, was applied. The model choice between fixed and random effect model was based on leverage plot examination and appraisal of deviance information criterion values. We weighed model convergence using trace and Gelman–Rubin–Brooks plots. The results of the NMA were expressed and displayed using league matrix tables where mean difference (MD), relative risk (RR), or log RR accompanied by their corresponding 95% credibility intervals (CIs) were demonstrated for all comparisons.
Credibility intervals, which are the Bayesian equivalent of CIs used in frequentist statistics, represent a range of values accounting for a certain percentage of the posterior distribution (in our case 95%). Intervention rankings were processed using the surface under the cumulative ranking area (SUCRA) score and visualized with the use of SUCRA plots. SUCRA provides an arithmetic display of the mean of the posterior distribution, representing the overall ranking of an intervention for a particular outcome, with values ranging from 0% to 100% (details of the search are reported in the Supplementary Methods).
The risk of bias for the included studies was assessed by two independent researchers A.C. and V.B. using the Risk of Bias in Non-Randomized Studies—of Interventions (ROBINS-I) and the revised Cochrane risk-of-bias tool for randomized trials. 19,20 Disagreements between the two investigators were resolved through consultation with a third reviewer (P.T.). Due to the limited number of available RCTs (three studies), we were unable to perform a sensitivity analysis including only RCTs, nonetheless, we proceeded with a sensitivity analysis excluding all studies describing high risk of bias.
Results
Baseline study characteristics
Sixteen studies, 3 RCTs, 2 prospective case series, and 11 retrospective case series comprising 4112 patients and demonstrating 5 interventions were finally included. 11,21 –35 The study flow diagram is summarized in Supplementary Figure S1. The mean follow-up duration was 11.9 months. Between-arm comparisons were conducted, using data from the following numbers and categories of studies: three RFA versus MWA, five RFA versus LA, three CS versus MWA, one MWA versus LA, one CS versus HIFU, one RFA versus CS, and two multiarm comparisons (Table 1).
Baseline Study Characteristics
This means volumes have statistical significant difference between two groups.
CS, conventional surgery; HIFU, high-intensity focus ultrasound; LA, laser ablation; MWA, microwave ablation; N/A, not applicable; PCS, prospective cohort study; RCT, randomized controlled trial; RFA, radiofrequency ablation.
Risk of Bias
The overall risk of bias according to ROBINS-I regarding comparative studies was low to moderate, with 4 out of the 13 included studies describing serious risk of bias. The risk of bias for the three included RCTs according to revised Cochrane risk-of-bias tool 2 was assessed as moderate (Supplementary Figs. S2 and S3).
Network meta-analysis
Volume reduction rate
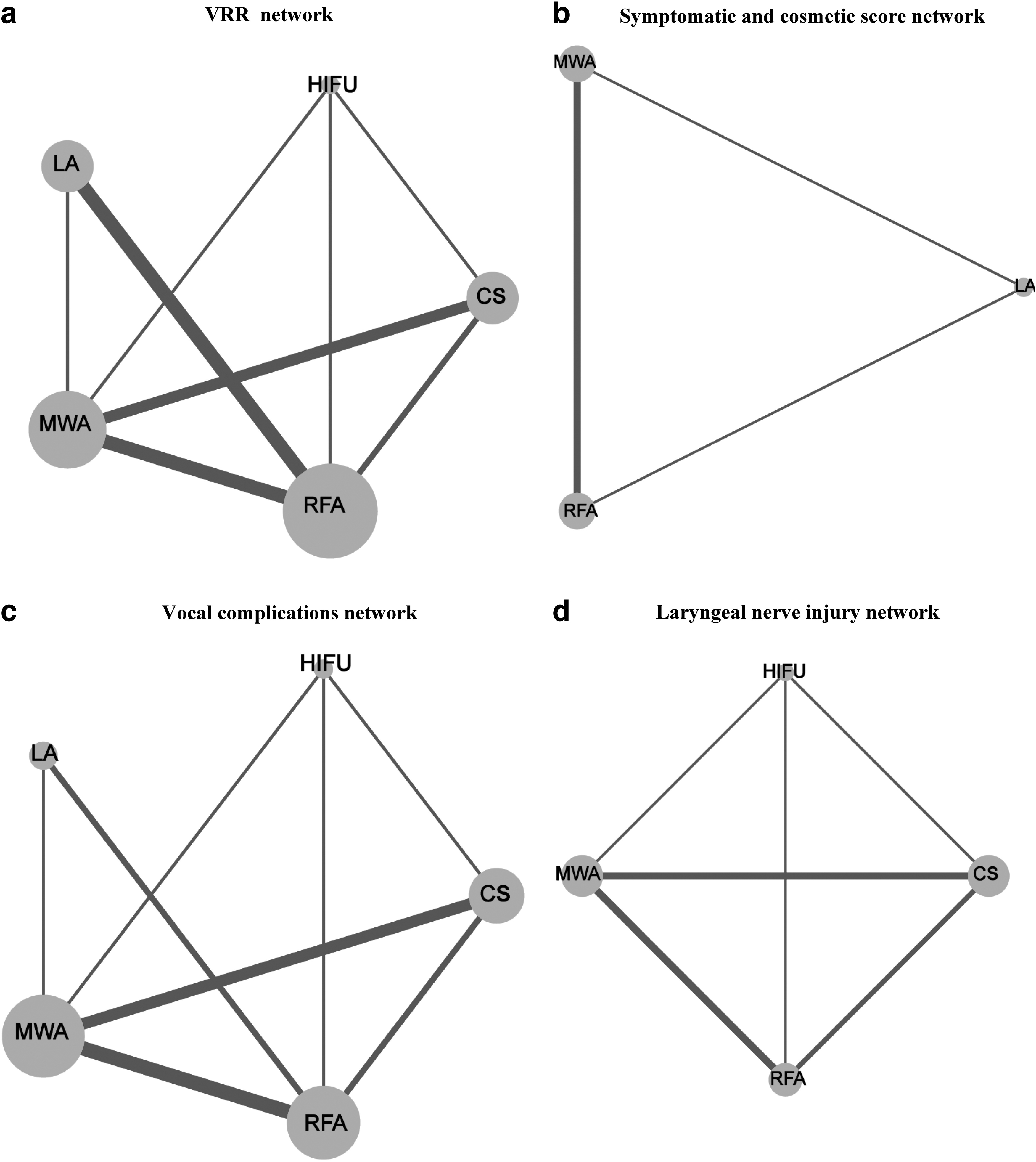
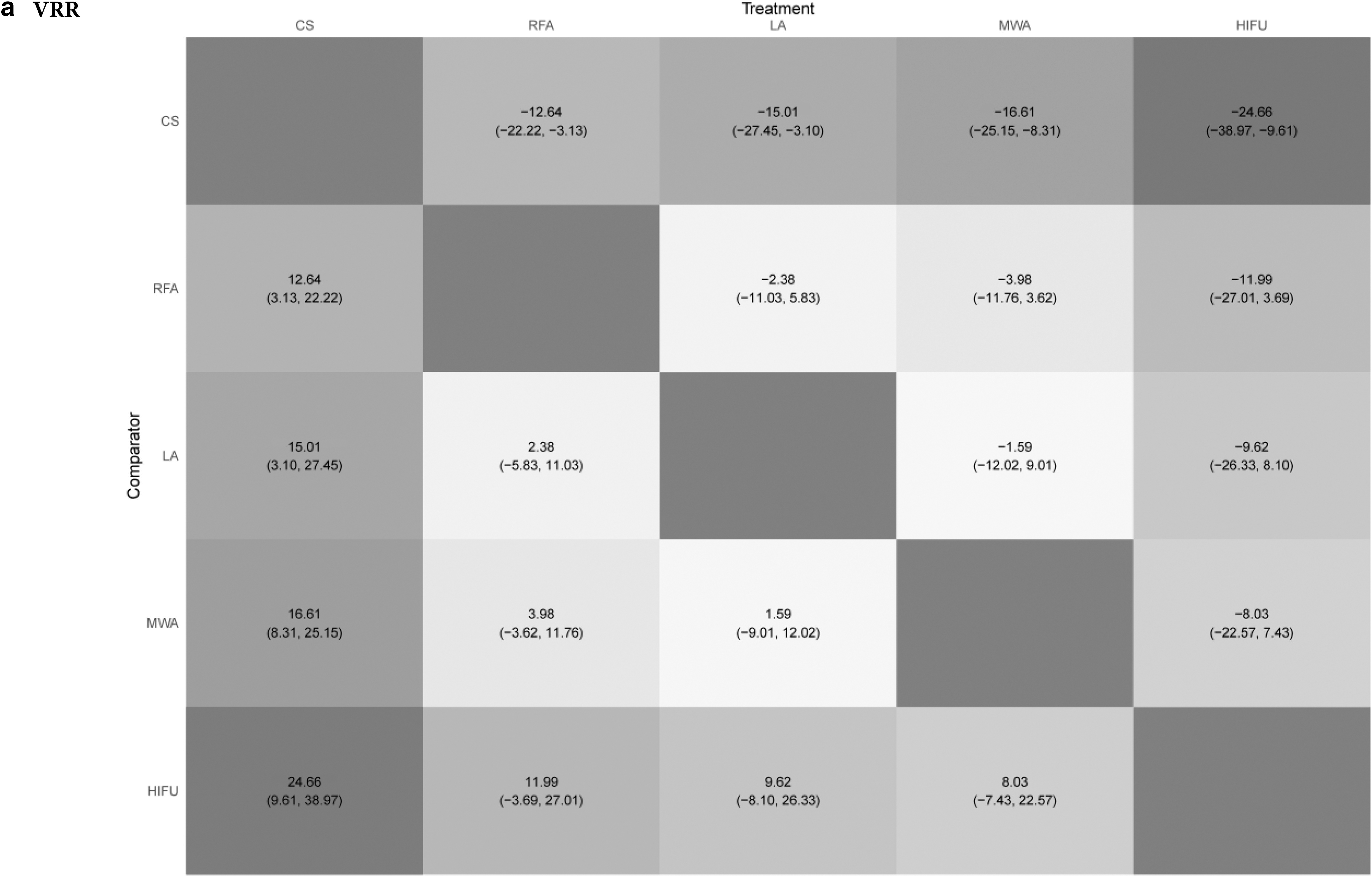
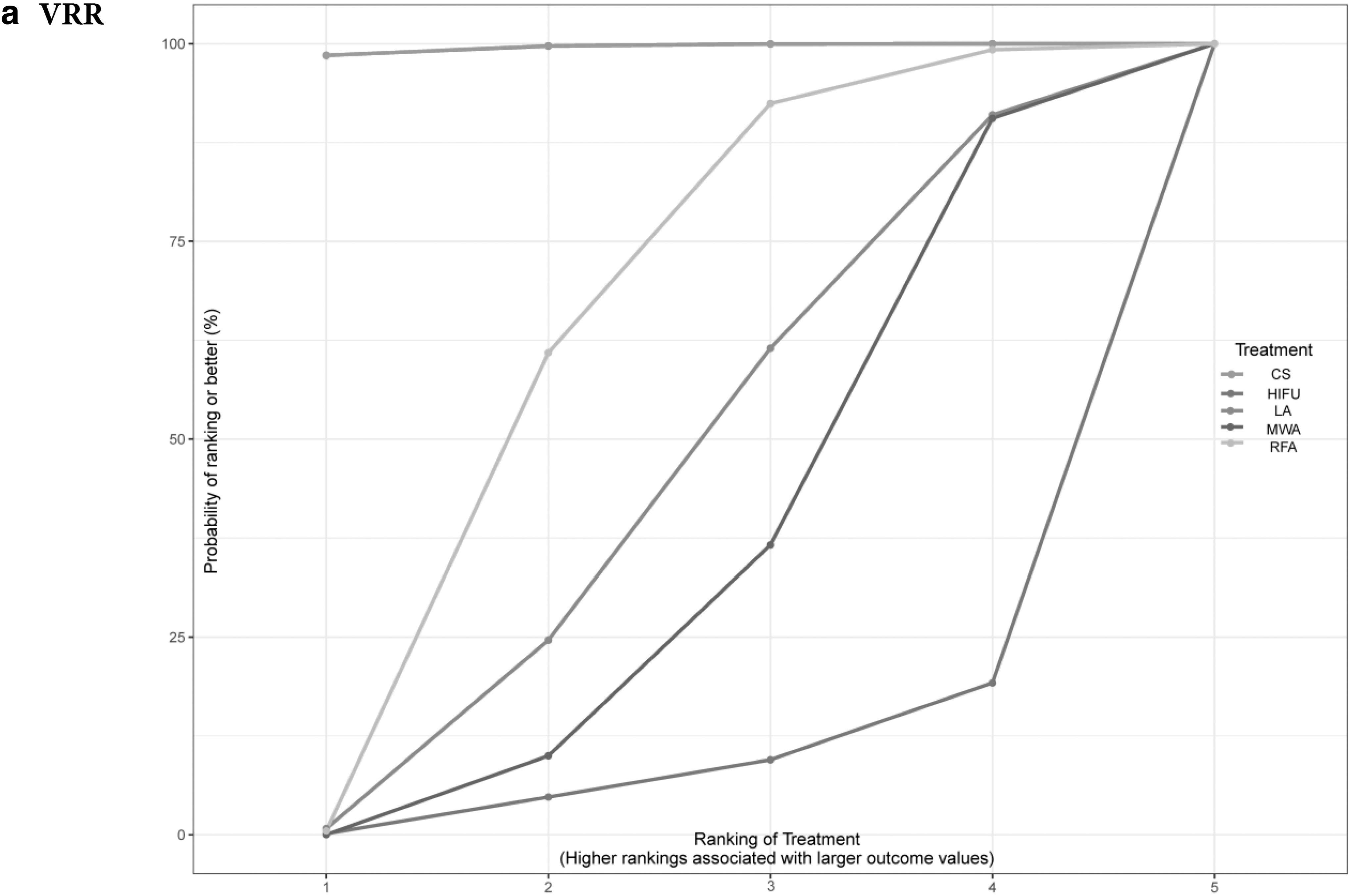
All the 16 eligible studies were included in the VRR network (as none introduced a sever amount of inconsistency). The network included 4112 patients (Fig. 1a). CS demonstrated the highest VRR by the end of follow-up compared with RFA MD 12.64 [CI: 3.13 to 22.22], LA MD 15.01 [CI: 3.10 to 27.45], HIFU MD 24.66 [CI: 9.61 to 38.97], and MWA MD 16.61 [CI: 8.31 to 25.15] without statistically significant differences among the remaining interventions (Fig. 2a). SUCRA probability ranking for interventions most likely to result in the largest volume reduction ranked CS as first (SUCRA, 98.49), followed by RFA (SUCRA, 62.81) and LA (SUCRA, 58.41) (Fig. 3a).
Networks: (
League heat plots: (

Surface under the cumulative ranking: (

The sensitivity analysis network included 11 studies that comprised 3456 patients describing RFA, LA, MWA, and CS interventions. While CS was associated with greater volume reduction compared with RFA MD 11.25 [CI: 2.02 to 20.14] and MWA MD 14.72 [CI: 6.96 to 22.55], the outcomes failed to reach statistical significance for LA MD 11.24 [CI: −1.78 to 24.57]. Statistically nonsignificant differences were identified among MWA and LA MD −3.50 [CI: −15.06 to 8.36], MWA and RFA −3.49 [CI: −11.22 to 3.89], and LA versus RFA 0.01 [CI: −11.23 to 10.64].
Symptomatic and cosmetic scores
All studies providing information regarding symptomatic and cosmetic outcomes were included in the two networks. Symptomatic and cosmetic score networks consisted of the same five studies comprising 2006 patients portraying LA, MA, and RFA comparisons (Fig. 1b). LA was not significantly associated with improvement in symptomatic score, compared with MWA MD 0.03 [CI: −0.51 to 0.56] and RFA MD 0.03 [CI: −0.50 to 0.57]. Regarding cosmetic outcomes, MWA was not significantly different compared with RFA MD 0.01 [CI: −0.09 to 0.12] and LA MD 0.17 [CI: −0.04 to 0.38] (Fig. 2b, c). SUCRA ranking for symptomatic scores ranked LA (SUCRA, 51.58) first and MWA (SUCRA, 51.58) second as the interventions most likely to result in the highest symptomatic score improvement by the end of follow-up. For cosmetic scores, MWA ranked first (SUCRA, 57.0) and RFA second (SUCRA, 54.6) (Fig. 3b, c). The initial symptom score and cosmetic score networks did not include any studies at high risk of bias.
Vocal complications and laryngeal nerve injury
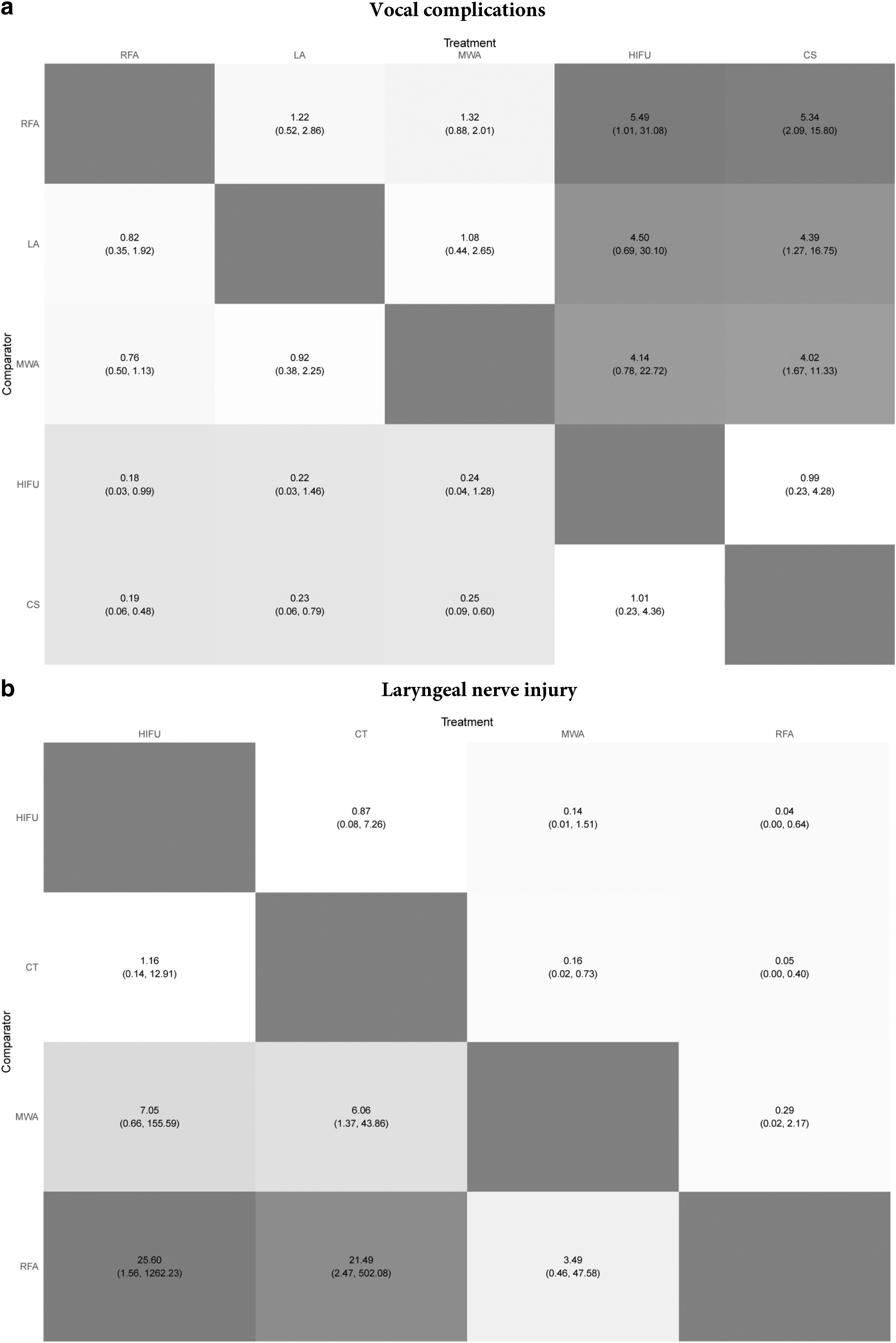
The vocal complications network included 13 studies, incorporating data from 3812 patients (Fig. 1c). RFA, RR 0.19 [CI: 0.06 to 0.48], LA RR 0.23 [CI: 0.06 to 0.79], and MWA RR 0.25 [CI: 0.09 to 0.60] were associated with a decreased risk for postintervention vocal complications compared with CS. We observed statistically nonsignificant differences between minimally invasive modalities apart from the RFA versus HIFU comparison, RR 0.18 [CI: 0.03 to 0.99]. RFA displayed a borderline statistically significant decreased risk for postintervention vocal complications of RR 0.18 [CI: 0.03 to 0.99] compared with HIFU (Fig. 4a). SUCRA ranked RFA as the intervention least likely to result in vocal complications (SUCRA, 61.62) followed by LA (SUCRA, 56.94).
League heat plots: (
The vocal complications sensitivity network included 10 studies of 3398 patients, comparing CS, RFA, MWA, and LA. CS was associated with an increased risk for vocal complications compared with MWA RR 3.68 [CI: 1.38 to 11.89] and RFA RR 5.14 [CI: 1.74 to 19.32], while the results failed to reach statistical significance for LA RR 2.41 [CI: 0.44 to 13.54]. We identified statistically nonsignificant differences among RFA and both MWA RR 0.72 [CI: 0.34 to 1.43] and LA RR 0.47 [CI: 0.11 to 1.68] and MWA versus LA RR 0.65 [CI: 0.15 to 2.43].
The laryngeal nerve injury network included seven studies of 1526 patients (Fig. 1d). Both RFA RR 0.05 [CI: 0.00 to 0.40] and MWA RR 0.16 [CI: 0.02 to 0.73] were associated with a decreased risk of transient laryngeal nerve injury compared with CS. In addition, RFA was associated with a decreased risk for laryngeal nerve injury compared with HIFU RR 0.04 [CI: 0.00 to 0.64] (Fig. 4b). SUCRA score rankings suggested that RFA was the intervention estimated to be least likely to result in vocal complications (SUCRA, 88.30) followed by MWA (SUCRA, 83.70).
The laryngeal nerve injury sensitivity analysis network included 10 studies comparing CS, RFA, and MWA in 1278 patients. CS was associated with an increased risk for laryngeal nerve injury compared with RFA RR 16.05 [CI: 1.84 to 387.95] and MWA RR 4.86 [CI: 1.08 to 34.26], while statistically nonsignificant differences were identified between RFA and MWA RR 3.25 [CI: 0.43 to 47.34].
Thyroidal gland dysfunction
The thyroidal dysfunction network included six studies of 2164 patients (Supplementary Fig. S4a). RFA RR 0.00 [CI: 0.00 to 0.00] and MWA RR 0.00 [CI: 0.00 to 0.03] were associated with a decreased risk of hypothyroidism compared with CS. RFA also was associated with a decreased risk of hypothyroidism compared with MWA RR 0.00 [CI: 0.00 to 0.02] (Supplementary Fig. S4b). SUCRA ranked RFA as the intervention least likely to result in thyroid gland dysfunction (SUCRA, 99.86) (Supplementary Fig. S4c). All the included studies in the thyroidal dysfunction network displayed low to moderate risk of bias.
Nodule recurrence
The recurrence network consisted of 1835 patients and compared CS, MWA, and RFA. 11,24,27 Surgical management included total thyroidectomy, subtotal thyroidectomy, and unilateral lobectomy. The reported recurrence was included in Che et al.'s study, where the surgical management included only total thyroidectomy and lobectomy. 27 CS was associated with a significantly increased risk for nodular regrowth compared with RFA RR 11.72 [CI: 1.17 to 440.36], but not MWA RR 11.58 [CI: 0.93 to 536.73]. SUCRA ranked RFA (SUCRA, 71.0) as the safest intervention regarding nodular regrowth, followed by MWA (SUCRA, 28.9). All included studies in the network displayed moderate to low risk of bias.
Discussion
In this systematic review and NMA, we observed no statistically significant differences in the primary endpoints of VRR, symptomatic score, and cosmetic score, among all the examined thermal ablation techniques compared with CS. CS was associated with an increased risk for voice disturbances and laryngeal nerve injury compared with RFA, LA, MWA and RFA, MWA, respectively. CS was also associated with an increased risk for thyroid hormone disturbances compared with RFA and MWA.
Whereas thermal ablation has been established as a viable alternative to conventional thyroidectomy (either total or lobectomy) in the treatment of benign thyroid nodules, controversy still exists over their place in the therapeutic process. 3,36 The debate around this issue is mirrored by the often-contradicting recommendations issued by different societies. For instance, the American Thyroid Association in their latest guidelines do not refer to the use of thermal ablation in the treatment of thyroid nodules. 37 Conversely, the European Thyroid Association recommended the use of image-guided thermal ablation for patients refusing conventional therapy, 38 while the international RFA Consensus Statement advocated for the use of U.S.-guided ablation procedures alternative to surgery for patients with benign thyroid nodules presenting with compressive and/or cosmetic symptoms. 38 –40 To our knowledge, there are two prior reviews on this topic that used an NMA format. 41,42
Ha et al. conducted the first NMA incorporating 10 studies and 184 patients in 2015. 41 The authors reported an increased VRR for RFA compared with LA, however, their study was limited by a low number of included patients and the analysis of nonclosed loop networks not allowing for the evaluation of the consistency assumption and thus leaving their outcomes vulnerable to imprecision. 41 He et al., in their study of 16 RCTs and 834 patients, published in 2021 reported increased RFA efficacy regarding VRR compared with LA, HIFU, and ethanol ablation at a mean follow-up of 6 months. 42 This analysis also did not form closed-loop networks. Moreover, it is important to note that neither of these studies used the gold standard treatment of conventional thyroidectomy as a comparator (control) in their analysis. 42
This meta-analysis, contrary to the aforementioned studies, showed that the VRR of ablated thyroid nodules did not differ significantly among the multiple thermal techniques. While in our review, Cheng et al. 11 and Cesareo et al. 22 reported superior VRR results for RFA compared with LA and MWA when evaluating these results, it is essential to be aware of the disparities in operational methods observed among the techniques. For instance, during RFA, energy is delivered to the peripheral margins of the nodule, a characteristic that is not ensured with LA. In addition, Cheng et al. in their study, where they reported superior VRR outcomes for MWA compared with RFA, suggested that the source of MWA superiority was its ability to reach higher temperatures during ablation (RFA-induced tissue temperature reaches 110°C, while during MWA the temperature is 150°C). 11
In line with our outcomes, Mauri et al. 32 and Yue et al. 35 displayed nonstatistically significant differences between RFA, LA, and MWA in terms of VRR.
In the present meta-analysis, the differences of cosmetic and symptomatic scores among RFA, LA, MWA were not statistically significant, suggesting equal effectiveness between treatments. While our results are in concordance with the published literature, RFA ranked as the intervention most likely to result in the largest symptomatic score improvement from baseline to the end of follow-up. Similarly, MWA ranked first concerning cosmetic outcomes. Regarding the thermal ablation versus CS comparison, we failed to form a closed-loop network and thus this relationship could not be investigated. Nonetheless, Guan et al. in their systematic review where they compared thermal ablation with conventional thyroidectomy and whereas they displayed improved cosmetic outcomes in favor of thermal ablation, they did not identify statistically significant differences regarding symptomatic score improvement. 5
Recurrent laryngeal nerve palsy and hoarseness are among the most prominent complications following surgical interventions for the treatment of benign thyroid nodular disease. 2,43 In our study, all thermal ablation techniques were associated with a decreased risk for postintervention vocal complications compared with conventional thyroidectomy. In addition, we identified statistically nonsignificant differences among thermal interventions with the exception of HIFU, which was associated with an increased risk for postoperative vocal disturbances compared with RFA.
While such outcomes could have been potentially influenced by factors such as nodular location, size, and the fact that total thyroidectomy was the intervention depicted in the majority of the included studies (total thyroidectomy includes bilateral neck exploration, resulting in higher risk for recurrent laryngeal nerve injury), one cannot overlook the potential protective effect of hydrodissection during thermal ablation. Hydrodissection, a highly recommended practice during thermal ablation, involves the introduction of an anesthetic agent and/or normal saline into the target tissue as a way of preventing vessel and nerve injuries. 2,5
Data regarding the use of HIFU in the treatment of benign thyroid nodules are scarce, and as a result, we could identify only two comparative studies. 30,31 Despite the satisfactory VRR outcomes (similar to that of RFA and MWA), minimal reported postinterventional hypothyroidism and infection rates, longer operative duration, higher pain scores, and the increased cost of the device account for major disadvantages. Moreover and although thermal ablation modalities are considered safe, they come with their own set of potential complications. 30,31 For instance, researchers have previously reported several cases of Horner's syndrome following MWA and HIFU. The phenomenon is attributed to high-energy delivery during ablation and subsequent damage to the sympathetic trunk (especially when ablated nodules are in near proximity to the carotid sheath). 11,31
Thyroid hormonal disturbances following thermal ablation constitute a rare entity. 11,22,24,25,27,28,31,33,35,44 –48 Contrary to thermal ablation, conventional thyroidectomy is consistently linked to postsurgical thyroidal hormone disturbances resulting in lifelong levothyroxine dependency. In our review where six studies reported on postprocedural hyperthyroidism, we have observed that RFA and MWA were associated with a reduced risk of postinterventional hypothyroidism compared with CS. These findings are plausible since minimally invasive techniques target specific nodular structures while aiming to preserve a functioning thyroid gland, while thyroidectomy (often total) grossly removes thyroid tissue, potentially hindering thyroid gland function.
Presently, the two major concerns regarding thermal ablation techniques are their long-term efficacy and the risk of recurrence. The reported regrowth rates in the literature range from 10% to 15%. 49,50 Although we have observed lower nodular regrowth rates for RFA and MWA when compared with CS, our results should be interpreted with caution. First, the inclusion of multiple types of thyroid surgeries, ranging from total thyroidectomy to subtotal thyroidectomy, is a potential source of confounding bias. Furthermore, the limited number of included studies and the brief follow-up do not allow for definite conclusions to be drawn.
Similarly, and although our results favor minimally invasive techniques in terms of safety, one should keep in mind the variety of surgical approaches represented in this review. While the choice of the appropriate resection method is multifactorial and includes parameters such as the number and/or the location of lesions, total thyroidectomy is linked to higher complication rates compared with lobectomy. 51 In our review, the four studies, which undertook hemithyroidectomy or lobectomy, concluded in nonstatistically significant differences between thermal ablation (RFA, MWA, HIFU) and CS. 21,23,24,31
Limitations
The major limitations of our review are the inclusion of retrospective studies, which render our review vulnerable to selection bias and the moderate risk of bias displayed by the limited number of included RCTs. In addition due to the shortage of eligible studies, we did not manage to include thyroid surgery in the cosmetic effects network failing to analyze one of the primary advantages of percutaneous ablation when compared with the surgical approach. The studies included in our meta-analysis defined conventional thyroidectomy by lobectomy, subtotal thyroidectomy, or total thyroidectomy, without reporting on outcomes of respective surgical treatments, potentially introducing confounding bias.
Furthermore, the majority of the studies reported one single ablation session, with the exception of the studies by Ben Hamou et al. 25 and Cheng et al. 11 who reported on single- and two-session ablations, thereby potentially overestimating the efficacy of the ablation methods. 11,22 –26,28 –33,35 Finally, the limited follow-up duration in the included studies did not allow for the evaluation of long-term nodular regrowth rate and the duration of therapeutic success.
Conclusions
Although we have comprehensively reviewed the published literature on the efficacy and safety of thermal ablation modalities in the treatment of benign thyroid lesions, limitations such as the inclusion of variable surgical techniques and the paucity of long-term high-quality data limit our ability to make definitive conclusions. RCTs of thermal ablative therapies for benign thyroid nodular disease with long-term follow-up are needed.
Footnotes
Authors' Contributions
Study conception and design: A.C. and V.B. Data collection: A.C., V.B., and A.B. Analysis and interpretation of results: A.C., V.B., and G.T. Draft article preparation: A.C., V.B., A.I., and T.P. Revision of the article: T.P. and A.M. All authors reviewed the results and approved the final version of the article.
Author Disclosure Statement
All authors declare no conflict of interest.
Funding Information
There is no funding for this study.
Supplementary Material
Supplementary Methods
Supplementary Table S1
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4