
Abstract

C
IGSF1 deficiency is the most common genetic form of central CH, and has become a well-described and characterized condition. 1,6 However, reports of isolated central CH due to variants in TBL1X and IRS4 are scarce (Supplementary File S1). So far, isolated central CH due to a variant in TBL1X has been described in only eight individuals, from six families (four Dutch, one Japanese, and one Spanish), and in the case of IRS4, in only nine individuals, from five families (four Dutch and one Finnish) (Supplementary File S1).
Loss-of-function variants in these genes, encoding TBL1X and IRS4, respectively, cause a phenotype of mild to moderate isolated central CH, which segregates in an X-linked recessive inheritance pattern. Some heterozygous female carriers present with mild isolated CH, while most are euthyroid. 2 In the case of TBL1X loss of function, hearing thresholds lower than age-specific reference intervals (RIs) have also been reported. 4 To expand the knowledge on isolated central CH, we present clinical and genotype data of 16 newly identified individuals with isolated central CH due to TBL1X and IRS4 variants.
Methods
In the Netherlands, DNA analysis for isolated central CH genes is centralized and only performed at the Amsterdam UMC Genome Diagnostics laboratory. All newly identified Dutch individuals with central CH due to variants in TBL1X or IRS4 were asked for permission to include their clinical information in the Biobank of Congenital Abnormalities of the Thyroid Axis, instituted by the Department of Pediatric Endocrinology, Emma Children's Hospital of the Amsterdam University Medical Centers. Use of biobank data for this study was approved by the Biobank Review Committee of the Amsterdam UMC location AMC (2020_200#A2020115). Patients or their legal guardians signed informed consent forms for publication of clinical and genotype data. The research was completed in accordance with the Declaration of Helsinki as revised in 2013.
Patients were diagnosed in the clinical setting—either after detection by neonatal CH screening, segregation analysis or in the work-up of a clinical condition—and identified by NGS of IGSF1, IRS4, TBL1X, TRH, TRHR, and TSHB, or Sanger sequencing of a specific variant. TBL1X and IRS4 primer sequences are available upon request. Methods used to perform in silico analyses and classify variants are given in Supplementary File S2.
Results
Since previous Dutch publications on TBL1X and IRS4 in 2016 and 2018, respectively, 4,5 the Amsterdam UMC Genome Diagnostics laboratory identified 16 new individuals with central CH due to variants in TBL1X or IRS4: 8 with a TBL1X variant (from seven families) and 8 with an IRS4 variant (from five families). Clinical characteristics and variants are summarized in Table 1. Fifteen of 16 individuals were males. All probands in this case series had biochemically confirmed central CH. Additional endocrine screening revealed no other endocrine abnormalities. The female with a heterozygous IRS4 variant had central CH and was being treated with thyroxine (T4). All male hemizygous carriers had central CH. Twelve of 16 individuals were identified through newborn screening (NBS). Supplementary File S3 presents all available NBS results.
Clinical Characteristics of Individuals with Central Congenital Hypothyroidism due to Variants in TBL1X and IRS4
Individuals with isolated central CH from the same family are grouped by number, but have different suffixes.
Variants of these individuals were previously reported by Naafs et al., 1 however, without detailed phenotypic information of the probands.
ADHD, attention-deficit/hyperactivity disorder; ADD, attention-deficit disorder; ASD, autism spectrum disorder; CH, congenital hypothyroidism; F, female; fT4, free thyroxine; IRS4, insulin receptor substrate 4; M, male; NA, not available; NBS, newborn (blood spot) screening; RI, reference interval; TBL1X, transducin beta-like 1; TSH, thyrotropin.
Neonatal health problems leading to hospitalization such as hypothermia and feeding problems were previously reported in a cohort of individuals with isolated central CH. 1 In our current cohort five individuals experienced symptoms in the neonatal period. Four had minor feeding problems and one had hypothermia and mild jaundice.
None of the participants reported hearing difficulties; however, formal audiometric measurements were not performed.
Figure 1 shows schematic representations of the TBL1X and IRS4 genes, including known and novel variants leading to central CH. Supplementary File S2 presents the predicted effects of novel variants. To summarize, TBL1X variants possibly either lead to TBL1X deficiency or severely impair normal folding and functioning of the WD40 domain (the scaffold for nuclear protein–protein interactions), and IRS4 variants are mRNA-truncating nonsense and frameshift variants that possibly result in a truncated protein.
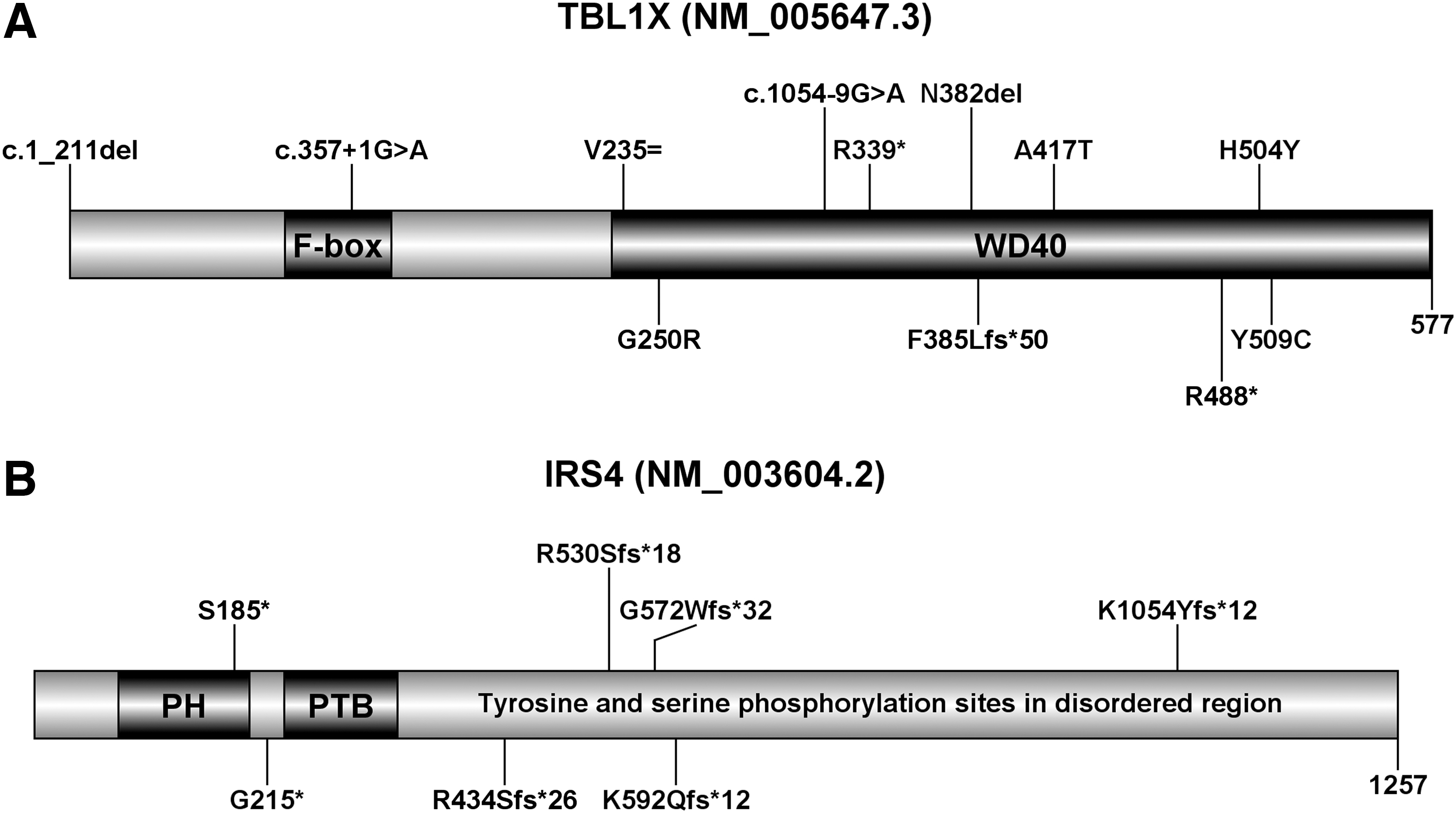
Schematic representations of TBL1X and IRS4 including known and novel variants. (
Discussion
These results imply that the previously reported clinical features of isolated central CH due to pathogenic variants in TBL1X and IRS4 remain the prominent clinical findings.
Eight individuals with mild central CH from seven families with a variant in TBL1X were identified. The TBL1X protein is a subunit of the silencing mediator of retinoid and thyroid hormone receptors and nuclear receptor co-repressor 1 complexes, which associate with the thyroid hormone receptor and repress or promote gene expression in the absence of triiodothyronine. Dysfunction or deficiency of TBL1X leads to a negative shift of the free T4 set-point, due to altered transcription of TSHB and TRH. 7
Previously, one individual with central CH due to a TBL1X (truncating) nonsense variant was found to have additional clinical features, including attention-deficit/hyperactivity disorder (ADHD), gastrointestinal dysmotility and Arnold–Chiari malformation type I. 8 The authors linked the additional clinical features to possible transcriptional implications of TBL1X dysfunction. We report two individuals with a truncating TBL1X variant and ADHD (Table 1). ADHD has now been diagnosed in three patients with a truncating variant, which may indicate a genotype–phenotype correlation requiring further research. 8
Eight individuals with mild central CH from five families were identified with a variant in IRS4. IRS4 is expressed in several tissues, including the hypothalamus and pituitary gland. IRS4 transduces signals from cell membrane receptors with tyrosine or serine/threonine kinase activity to cytoplasmic downstream effectors.
Although the exact pathophysiological mechanism of IRS4-related central CH remains to be elucidated, 2 the known variants present an interesting mechanistic hypothesis. All reported variants are premature termination codon variants. Since IRS4 is a single exon gene, nonsense-mediated mRNA decay escape is feasible for the resulting IRS4 mRNA variants. Possibly, truncated IRS4 proteins are formed, which can localize to the cell membrane and enact a dominant negative effect on TRH production, TSH production, or the TSH bioactivity regulation pathway. This hypothesis suggests functional importance of the IRS4 C-terminus. According to PhosphoSitePlus, the C-terminus of IRS4 holds several serine phosphorylation motifs not previously implicated in known IRS4 functions. Functional studies are needed to explore the function of the IRS4 C-terminus, which could provide further insight to how IRS4 is involved in the TSH production/bioactivity regulation signaling pathway.
We believe that worldwide most individuals with isolated central CH are still undiagnosed, presumably because of mild/hidden clinical features and relative rarity, thwarting clinical detection. 1 The Dutch NBS program enables early detection of both primary CH and central CH through analysis of total T4 and thyroxine-binding globulin, in addition to TSH. The fact that almost all cases of mild isolated central CH due to TBL1X and IRS4 variants are from the Netherlands, probably shows the power of the Dutch NBS method in detecting isolated central CH. In a large retrospective study of 20 years of central CH screening in the Netherlands, 154 individuals with central CH were identified. 1 Thirty-five had isolated central CH, which was explained by variants in IGSF1 in most cases (17 of 35), followed by TBL1X (5 of 35) and IRS4 (5 of 35).
Undeniably, severe CH is detrimental to fetal and infant development. However, the (negative) effects of untreated isolated central CH are unknown. A recent study showed that Dutch children with early treated isolated central CH had similar full-scale intelligence quotient tests scores to their unaffected siblings. 9 Unfortunately, such data on individuals with late detected isolated central CH are lacking. Future study should focus on assessing the effect of early versus late detection and treatment of isolated central CH on health, cognition, and quality of life.
This study presents three major limitations. First, thyroid biochemistry of probands was investigated using different assays, and in different laboratories. Therefore, it was not possible to present a detailed account of thyroid hormone abnormalities at diagnosis, especially since most individuals were identified in the neonatal period, when different RIs apply. 10 Second, due to the retrospective nature of this study, we could not include audiometric measurements and segregation analysis, the latter was not fully performed in all families, hence comprehensive pedigrees are missing. Third, no further functional studies were performed to confirm the predicted effect of splice site variants, hence caution is warranted with the interpretation of these variants.
In summary, we add 16 Dutch cases of isolated central CH due to variants in TBL1X and IRS4 to the 21 previously described cases, including four novel TBL1X variants and one novel IRS4 variant.
Statement of Ethics
The authors have no ethical conflicts to disclose. The patients and/or or their legal guardians agreed to participate and signed informed consent to store medical information for research/publication in the Biobank of Congenital Abnormalities of the Thyroid Axis, instituted by the Department of Pediatric Endocrinology, Emma Children's Hospital of the Amsterdam University Medical Centers. Use of biobank data for this study was approved by the Biobank Review Committee (Biobank Toetsings Commissie) of the Amsterdam UMC location AMC (2020_200#A2020115). The research was completed in accordance with the Declaration of Helsinki as revised in 2013.
Data Availability Statement
Variant data have been submitted to ClinVar. Original data generated and analyzed during this study are included in this published article.
Footnotes
Acknowledgments
The authors are grateful for participation of all patients. The authors furthermore thank the following clinicians for helping with the recruitment of participating patients: Dr. A.E. Brandsma (Department of Pediatrics, Maasstad Ziekenhuis, Rotterdam), Dr. M. Sinnema (Department of Clinical Genetics, MUMC, Maastricht), and Dr. A.A. van Boekholt (Department of Pediatrics, VieCuri, Venlo).
Authors' Contributions
Acquisition of data, interpretation of data, genetic analyses, in silico analyses, and writing of first draft by P.L. Acquisition of data, interpretation of data, and review and editing by J.C.N., M.R.G., and C.F.M. Interpretation of data, genetic analyses, and review and editing by H.B. Interpretation of data, review and editing, and revision of intellectual content by A.B. Acquisition of data, interpretation of data, writing of first draft, review and editing, and project coordination by N.Z.-S. Interpretation of data, writing of first draft, review and editing, and project coordination by A.S.P.T. All authors critically reviewed article drafts and approved the final article as submitted.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary File S1
Supplementary File S2
Supplementary File S3