
Abstract
Background:
The 2015 American Thyroid Association (ATA) guidelines shifted recommendations toward less aggressive management of papillary thyroid cancer (PTC). Subsequently, several studies demonstrated a trend in performing thyroid lobectomy (TL) over total thyroidectomy (TT). However, regional variation has persisted without a clear indication of what factors may be influencing practice variation. We aimed to evaluate the surgical management of PTC in patients in rural and urban settings to assess trends of TL compared with TT following the implementation of the 2015 ATA guidelines.
Methods:
A retrospective cohort analysis was performed using the Surveillance, Epidemiology, and End Results (SEER) database from 2004 to 2019 of patients with localized PTC <4 cm who underwent TT or TL. Patients were classified as living in urban or rural counties based on the 2013 Rural-Urban Continuum Codes. Procedures performed from 2004 to 2015 were categorized as preguidelines, while those performed from 2016 to 2019 were categorized as postguidelines. Chi-square, Student's t-test, logistic regression, and Cochran–Mantel–Haenszel test were used.
Results:
A total of 89,294 cases were included in the study. Eighty thousand one hundred and fifty (89.8%) were from urban settings and 9144 (9.2%) were from rural settings. Patients from rural settings were older (52 vs. 50 years, p < 0.001) and had smaller nodules (p < 0.001). On adjusted analysis, patients in rural areas were less likely to undergo TT (adjusted odds ratio 0.81, confidence interval [CI] 0.76–0.87). Before the 2015 guidelines, patients in urban settings had a 24% higher odds of undergoing TT compared with those in rural settings (odds ratio 1.24, CI 1.16–1.32, p < 0.001). There was no difference in the proportions of TT and TL based on setting following guideline implementation (p = 0.185).
Conclusions:
The 2015 ATA guidelines led to a change in overall practice in surgical management of PTC toward increasing TL. While urban and rural practice variation existed before 2015, both settings had an increase in TL following the guideline change, emphasizing the importance of clinical practice guidelines to ensure best practice in both rural and urban settings.
Introduction
The incidence of thyroid cancer has increased drastically over the last several decades, driven by the use of high-resolution thyroid ultrasounds and incidental detection of papillary microcarcinoma (<1 cm) on imaging studies. 1 –3 Relatively stable mortality rates over the same period have led to concerns of overdiagnosis and overtreatment of thyroid cancer. 4,5 In response to several studies suggesting similar outcomes following thyroid lobectomy (TL) or total thyroidectomy (TT), the 2015 American Thyroid Association (ATA) guidelines shifted recommendations toward less aggressive surgical management of low- to intermediate-risk differentiated thyroid cancer (DTC). 6,7 The guidelines recommended that in most cases, patients with tumors <1 cm may undergo TL and patients with tumors 1–4 cm may undergo either TL or TT. 8 Before 2015, there were high rates of TT, and notably, a 6.2-fold variation in thyroidectomy rates regionally across the United States indicating large variation in practice patterns. 9 –12
Following release of the guidelines, several studies have showed an increasing trend in performing TL. 4,13 However, regional variation has persisted without clear indication of what demographic, spatial, or socioeconomic characteristics may be influencing the practice variation, including the potential impact of treatment in the rural versus urban setting. 4
Rural populations make up ∼19% of the United States and face unique barriers to health care. 14 These barriers contribute to the lower health care utilization of rural patients for both primary care and specialty care visits, despite having an overall worse health status than their urban counterparts. 14 Rural disparities are also evident in the cancer population with reported shorter survival for patients in rural areas for several of the most common cancers, including thyroid cancer. 15,16 Furthermore, patients undergoing thyroid surgery in a rural setting incur higher costs, higher complication rates, and are more likely to be managed by low-volume surgeons. 12,16 –19 It is unclear if these differences are due to limited access to care, location, surgical approach, or lack of guideline-concordant care.
The factors that may influence variation in surgical practice patterns (TT vs. TL) for thyroid cancer, including the impact of the rural versus urban setting, are unknown. Understanding the origin of this variation and the impact of the 2015 ATA guidelines is necessary to providing optimal care to all patients with thyroid cancer. We aimed to evaluate the surgical management of papillary thyroid cancer (PTC) in patients in rural and urban settings to assess trends of TL compared with TT following the implementation of the 2015 ATA guidelines.
Materials and Methods
Data source
A retrospective cohort analysis was performed using the Surveillance, Epidemiology, and End Results (SEER)*Stat database from 2004 to 2019. 20,21 SEER 17 was used to collect data from 17 SEER registries (San Francisco-Oakland SMSA, Connecticut, Hawaii, Iowa, New Mexico, Seattle [Puget Sound], Utah, Atlanta [Metropolitan], San Jose-Monterey, Los Angeles, Alaska Natives, Rural Georgia, California excluding SF/SJM/LA, Kentucky, Louisiana, New Jersey, Greater Georgia) that cover ∼26.5% of the US population. This study was determined to not constitute human subjects research on review by the Committee on Clinical Investigations at our institution, and thus, Institutional Review Board approval was not required.
Study population
The database was first queried for all cases with a primary site of the thyroid gland using the International Classification of Diseases (ICD) code C73.9. All PTC cases were included based on ICD-0-3 Site/Histology code: 8050/3, 8052/3, 8130/3, 8260/3, 8340/3, 8341/3, 8342/3, 8343/2, 8344/3, 8450/3, 8452/3. Cases were further stratified by size as <1, 1–2, 2–4, and >4 cm. Cases >4 cm and patients with regional, distant, or in situ stage of disease were excluded from the analysis as the 2015 ATA guidelines recommend TT for these cases. Patients with unknown or missing data for race/ethnicity, stage of disease, or Rural-Urban Continuum Code (RUCC) were excluded. Patients 18 years and older who underwent TT or TL were included in the final analysis (Fig. 1).
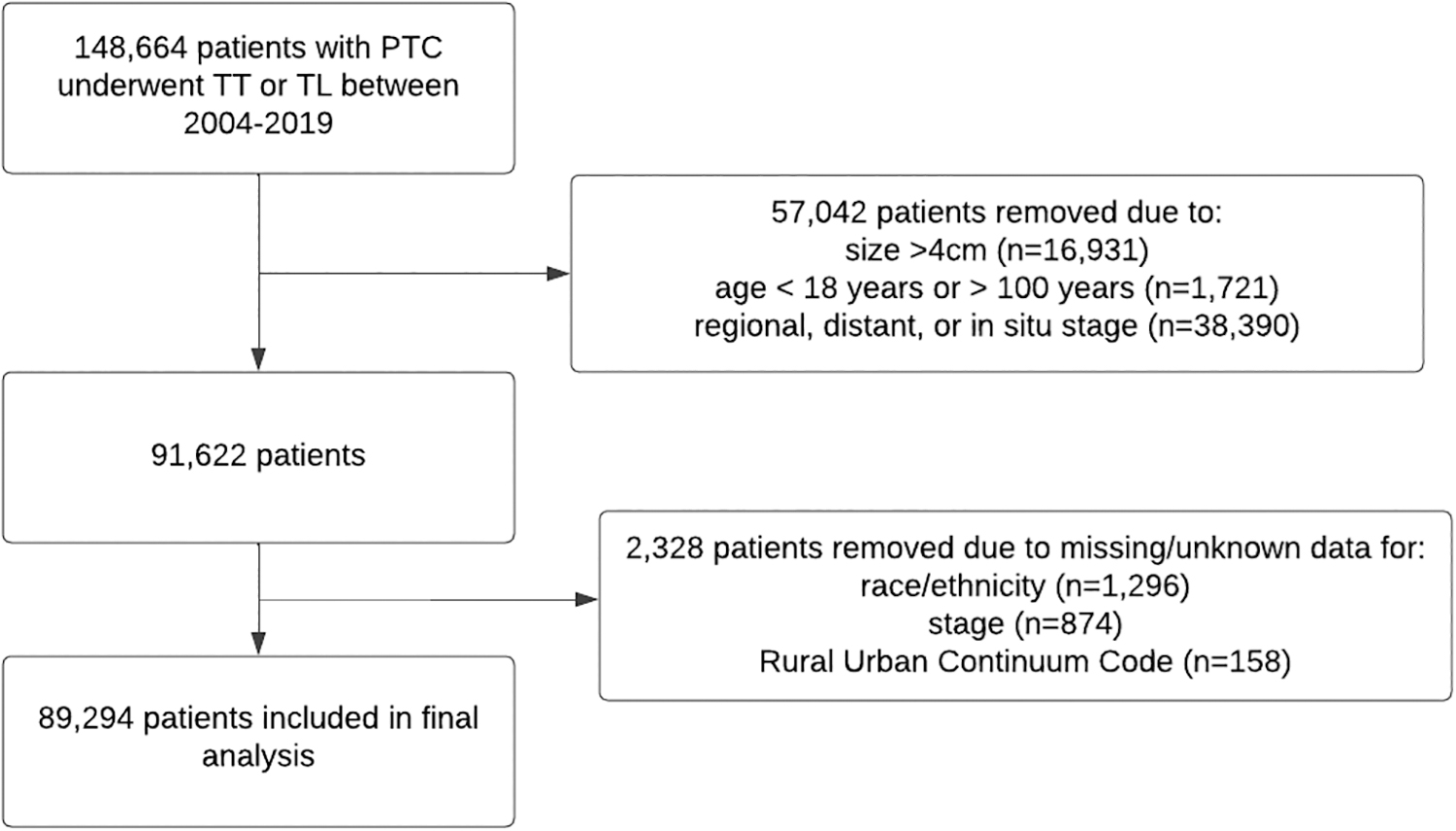
Consort diagram of screening methods for patients identified in the SEER database included in the final analysis. SEER, Surveillance, Epidemiology, and End Results.
TT was defined as subtotal or near total thyroidectomy, total thyroidectomy, or thyroidectomy, not otherwise specified. TL was defined as lobectomy and/or isthmectomy, lobectomy only, or lobectomy with isthmus. Only the first matching case for each person was included.
Covariables
Data collected included patient demographics, procedure type, year of diagnosis, overall survival, postoperative use of radioactive iodine, tumor size, and stage. The origin code was used to categorize patients as Spanish/Hispanic/Latino or non-Spanish/Hispanic/Latino. The race and origin recode was used to categorize patients as non-Hispanic white, non-Hispanic black, non-Hispanic Asian or Pacific Islander, non-Hispanic American Indian and Alaska Native, or Hispanic. Patients diagnosed from 2004 to 2015 were categorized as preguidelines, while those diagnosed from 2016 to 2019 were categorized as postguidelines.
Patients were classified as living in urban or rural counties based on the 2013 RUCC, as used in previous studies. 15,16,22,23 These codes classify metropolitan counties by population size and nonmetropolitan counties by the degree of urbanization and proximity to a metropolitan area. Codes 1–3 were classified as urban, while codes 4–9 were classified as rural using similar methodology to previous studies. 15,24,25 Overall survival was defined as the number of months from diagnosis to death.
Data analysis
Data analysis was conducted using R version 4.2.2 with a p-value <0.05 denoting statistical significance. Continuous variables were summarized as mean (standard deviation [SD]) and categorical variables were summarized as frequencies (percentage). Chi-square and Student's t-test were used to evaluate differences in demographics, procedure type, tumor size, tumor stage, and survival in the rural versus urban setting. Univariable and multivariable logistic regressions were used to estimate the odds of having a TT in rural and urban settings; an interaction term for setting × year of diagnosis was included in the multivariable regression analysis to account for the time-varying effect of setting across the study period.
The Cochran–Mantel–Haenszel method was used to estimate weighted odds ratios (ORs) across the years of the pre- and postguideline periods by setting (rural vs. urban) to assess variability in the proportion of TT and TL pre- and postguidelines for the overall study population and for each size subgroup (<1, 1–2, 2–4 cm).
Results
A total of 148,664 patients with PTC who underwent TT or TL over the study period were identified, of which 89,294 met the final inclusion criteria and were included in the study. The overall population was predominantly female (81%), non-Hispanic (85%), and white (68%), with an average age of 51 years (SD = 14) (Table 1). Most patients underwent a TT (80%). A total of 80,150 (89.8%) patients were from urban settings and 9144 (9.2%) were from rural settings. The population was mostly female with no difference in sex distribution in rural compared with urban settings (81% vs. 81% female, p = 0.739). There was a higher percentage of non-Hispanic/Latino (95% vs. 84%, p < 0.001) and white patients (87% vs. 66%, p < 0.001) in rural areas.
Baseline Characteristics of Patients Undergoing Thyroidectomy or Thyroid Lobectomy from 2004 to 2019
Bold p-values denote statistical significance.
AIAN, API, black, and white race include patients identifying as “non-Hispanic.”
AIAN, American Indian and Alaska Native; API, Asian and Pacific Islander; SD, standard deviation.
Patients from rural settings were older (52 vs. 50 years, p < 0.001) and had a smaller tumor size (p < 0.001), with no difference in radioactive iodine use in rural compared with urban settings (29% vs. 30%, p = 0.342). There was a higher proportion of patients with a tumor size of <1 cm (51% vs. 48%, p < 0.001) in rural compared with urban areas. While there was no difference in the proportion of patients in rural versus urban settings pre- and postguidelines (p = 0.714), there was a higher percentage of TL performed in rural settings (21% vs. 19%, p < 0.001), with no difference in overall survival (p = 0.781).
On adjusted analysis, males (adjusted odds ratio [aOR] 0.77, confidence interval [CI] 0.73–0.80, p < 0.001) and those of black (aOR 1.10, CI 1.02–1.18, p = 0.008) or Hispanic race (aOR 1.08, CI 1.03–1.13, p = 0.009) were more likely to undergo a TT (Table 2). Compared with patients with PTC <1 cm in size, patients with a tumor size of 1–2 cm (aOR 2.06, CI 1.98–2.16, p < 0.001) and 2–4 cm (aOR 1.70, CI 1.62–1.79, p < 0.001) were more likely to undergo a TT. Receipt of postoperative radioactive iodine therapy was also associated with undergoing a TT (aOR 5.19, CI 4.89–5.52, p < 0.001).
Univariable and Multivariable Logistic Regression of Undergoing Total Thyroidectomy Versus Thyroid Lobectomy
Bold p-values denote statistical significance.
Adjusted for setting, year of diagnosis, setting × year of diagnosis, sex, age, race, size, and radioactive iodine.
OR is conditional on the year of diagnosis being zero.
AIAN, API, black, and white race include patients identifying as “non-Hispanic.”
aOR, adjusted odds ratio; CI, confidence interval; OR, odds ratio; Ref., reference.
Compared with patients diagnosed before the 2015 ATA guidelines, patients diagnosed postguidelines were 32% less likely to undergo a TT (aOR 0.68, CI 0.65–0.71, p < 0.001). Patients in rural areas were 19% less likely to undergo TT (OR 0.81, CI 0.76–0.87, p < 0.001) compared with their urban counterparts.
Evaluation of the proportions of TT revealed that while TT was slightly more common in urban settings before the guidelines, both urban and rural settings had decreasing and similar proportions of TT following the guideline change (Fig. 2). The mean proportions of TT (vs. TL) preguidelines were 79.9% and 83.1% for rural and urban settings, respectively. Following the guidelines, proportions of TT in rural and urban settings were 75.5% and 74.3%, respectively. Before the 2015 guidelines, patients in urban settings had a 24% higher odds of undergoing TT compared with those in rural settings (Cochran–Mantel–Haenszel weighted OR 1.24, CI 1.16–1.32, p < 0.001) (Table 3). Following guideline implementation, there was no difference in the proportions of TT and TL based on setting (OR 0.94, CI 0.85–1.03, p = 0.185).
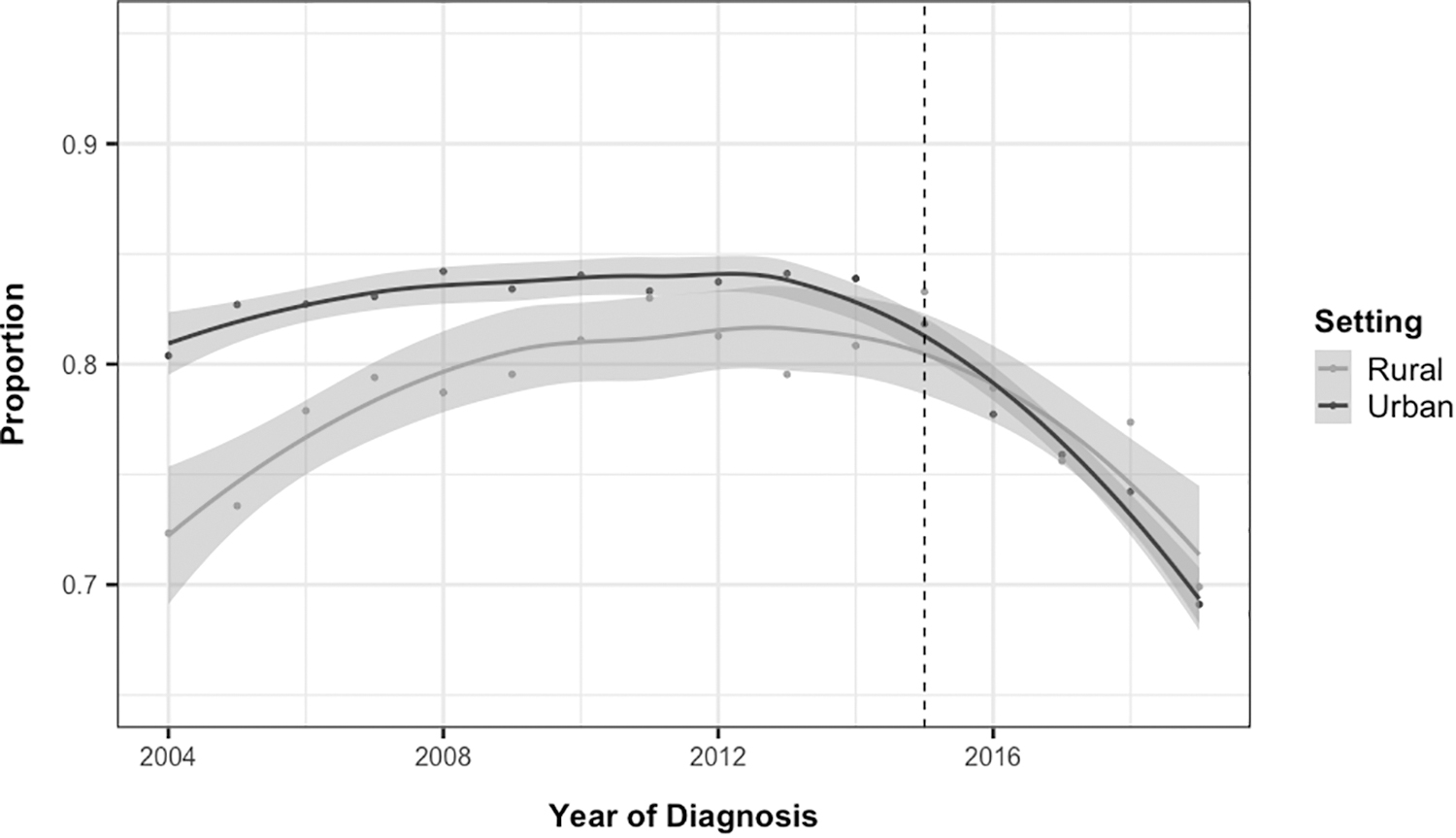
Total thyroidectomy proportion trend for papillary thyroid cancer in rural and urban settings. Dotted line indicates the time point of 2015 ATA guidelines. Shaded gray areas indicate the confidence interval. ATA, American Thyroid Association.
Proportions of Total Thyroidectomy for Papillary Thyroid Cancer in Rural and Urban Settings Pre- and Post-2015 American Thyroid Association Guidelines
Bold p-values denote statistical significance.
Reference group = rural.
Unadjusted.
Similar findings were observed on subgroup analysis based on tumor size (Table 3 and Fig. 3). For tumors <1 cm, proportions of TT (vs. TL) in urban settings were significantly higher at 75.0% compared with 71.6% in rural settings (OR 1.19, CI 1.10–1.29, p < 0.001), while there was no difference in proportions postguidelines (p = 0.250). When evaluating tumors from 1 to 2 cm in size, higher proportions of TT were found in urban versus rural settings preguidelines (88.6% vs. 91.2%; OR 1.33, CI 1.15–1.55, p < 0.001), with no differences postguidelines (0.177). Finally, on analysis of tumors 2–4 cm in size, there was no difference in proportions of TT pre- or postguidelines.
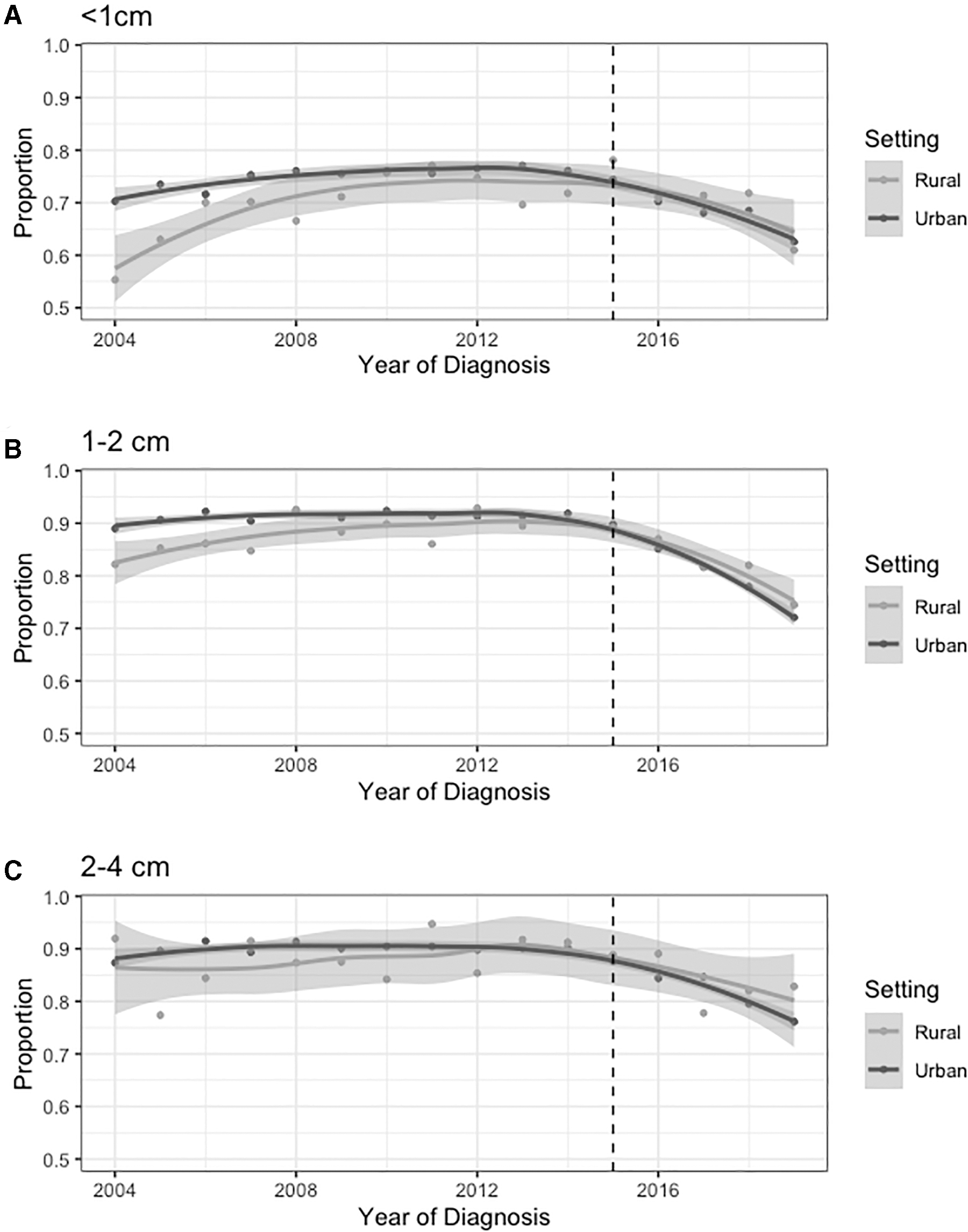
Proportion of total thyroidectomies in rural and urban settings by size; <1 cm (
Discussion
The release of the 2015 ATA guidelines marked a shift toward less aggressive surgical management of DTC. Assessing the impact of guideline dissemination and implementation is necessary to identify any disparities in patients receiving guideline-concordant care, including the differences between rural and urban settings. In this study, we queried SEER for patients with PTC <4 cm undergoing TT or TL from 2004 to 2009. We found that before the 2015 ATA guidelines, there was significant variation in the proportion of TT and TL in rural and urban settings, with patients from urban areas more likely to receive a TT. Following the release of the 2015 guidelines, proportions in both settings were similar with a trend toward increasing TL, demonstrating guideline-concordant care. Thus, surgical management guidelines are essential to promoting standardized care for patients across the rural and urban geographic settings.
Disparities in care for rural versus urban patients are well-established in the literature. Many of these disparities may be driven by factors associated with patients living in rural areas including lower income, lower education, lack of health insurance, and higher unemployment rates. 26 Patients with cancer living in rural areas often present with later stage of disease and are less likely to receive guideline-concordant care, likely, in part, due to the lack of local specialist providers requiring patients to travel for their care. 27,28 Few studies report on rural disparities among the thyroid cancer population, often with conflicting results and low-quality evidence. 17
In contrast to our findings, a single-institution study from Almubarak et al. found that thyroid cancer patients from rural settings are more likely to have advanced stage of disease at diagnosis compared with their urban counterparts, although this association was no longer significant when adjusting for other demographic factors. 29 Some suggest that the incidence of thyroid cancer is higher in urban populations, 16,30 while others report higher rates in rural settings. 18 Conflicting results are also reported regarding survival. Two US studies reported decreased survival for thyroid cancer patients in rural settings, 16,22 while a study out of China found no difference in overall survival, similar to the findings presented in this study. 19 Surgical practice variation across rural and urban areas is well documented for the management of other types of cancer. 31 –33 Importantly, none of the prior studies addresses the surgical management of thyroid cancer patients in rural versus urban settings.
While this is the first report of rural and urban surgical practice differences for thyroid cancer, several prior studies have reported regional and institutional differences in the extent of operation of TT or TL. In a cross-sectional analysis of Medicare data from 2014, Francis et al. report significant regional variation in rates of partial or TT, suggesting variation in practice before the 2015 guidelines. 9 We observed similar variation in proportions of TT and TL based on setting (rural vs. urban) preguidelines. Following release of the 2015 ATA guidelines, there was a trend toward increasing TL, similar to the findings reported in previous studies. 4,13,34 While overall trends suggest a shift toward more TL, regional and institutional variation still exists.
Toumi et al. found that patients in the South region were more likely to have a TT (vs. TL), while those in the North Central region were less likely to have a TT. 4 Wide variations in surgical practice also exist at the institutional level, with higher volume centers trending toward higher TL utilization. 13 Comparatively, although this study found significant procedure variation by setting (rural vs. urban) before the guidelines, after the release of the guidelines, this variation was no longer significant and there were decreasing proportions of TT in lieu of TL in both rural and urban settings. This finding was also evident following analysis based on tumor size with proportions of TL approaching 29%, 15%, and 12% regardless of setting (rural vs. urban) for tumors <1, 1–2, and 2–4 cm, respectively.
Although there was overall unification in procedural trends postguidelines, the relatively high proportions of TT still observed postguidelines raise concerns for overtreatment, suggesting that other factors may contribute to the regional variation observed in other studies. Future studies may assess factors involved in the decision-making process to provide context for the overall slow adoption in a change in practice patterns toward guideline-concordant care.
Despite the overall slow change in surgical trends toward TL, the findings of this study suggest that the guidelines played an integral role in unifying practice patterns across the rural and urban setting. Before the 2015 guidelines, there was significant variation in proportions of TT (vs. TL) and trends in TT were increasing in both settings. Following the guideline changes, there was no longer significant variation by setting and both rural and urban settings observed increasing proportions of TL. The accessibility and integration of the guidelines into practice across rural and urban areas were likely multifactorial. In a survey of ATA members, 92.9% of the respondents agreed with the content of the guidelines and 83% found the recommendations easy to incorporate in their practice, providing context for a similar uptake in guidelines across rural and urban settings. 35
Appropriate dissemination of the findings in up-to-date clinical guidelines will continue to be important to providing standard of care to all thyroid cancer patients, regardless of setting or other social determinants of health factors that may impact availability of resources and care.
This study has several limitations that should be acknowledged. Due to the lack of availability of certain procedural data in the SEER database, consideration was not given to patients who underwent a TL and subsequent completion thyroidectomy, and thus, outcomes should be understood in this context. While the SEER database used for the study includes data from 17 geographical areas and represents 26.5% of the US population, prior work suggests that it underrepresents rural populations, and so, it may not accurately reflect the trend across the country. 36 Indications for surgery as well as patient preferences play an important role in the decision-making process for TT versus TL, but were not available for inclusion in the analysis. Clinical factors including radiation history, family history, and ultrasound findings also play a role in the decision for TL versus TT, however, they are not captured in the SEER database.
Furthermore, the study does not account for any socioeconomic, insurance, or other social determinants of health-related factors that could contribute to upstream differences in access to care. The RUCC is based on the residence of the patient, and thus, an assumption made in the study is that rural patients receive their treatment in rural settings. Thus, we do not account for patients who may travel to seek care outside of their RUCC. Finally, although this is a large cohort of patients, there is a substantial difference in the number of rural versus urban patients, which may limit the comparability.
Conclusion
Following the 2015 ATA guidelines, there was an overall shift in the surgical management of PTC toward increasing TL. While urban and rural surgical practice patterns varied before 2015, both settings had an increase in TL following the guideline change for every size subgroup (<1, 1–2, 2–4 cm). The results of this study underscore the importance of guidelines in unifying care, regardless of treatment setting. Clinical practice guidelines are essential to ensuring best practice in both rural and urban settings.
Footnotes
Authors' Contributions
R.A.C.: conceptualization, data acquisition, formal analysis, visualization, and writing—original draft; N.C.: formal analysis and writing—review and editing; G.L.: data acquisition and writing—review and editing; J.M.B.: conceptualization and writing—review and editing; B.C.J.: conceptualization, supervision, and writing—review and editing.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of Harvard Catalyst, Harvard University, and its affiliated academic health care centers, or the National Institutes of Health.
Author Disclosure Statement
The authors have nothing to disclose.
Funding Information
This work was conducted with biostatistical consultation support from Harvard Catalyst | The Harvard Clinical and Translational Science Center (National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health Award UL1 TR002541) and financial contributions from Harvard University and its affiliated academic health care centers.