
Abstract
Background:
Delays in treatment for thyroid cancer (TC) have been associated with higher overall mortality rates. However, few studies have explored the impact of health disparities on delayed presentation and treatment for TC. This study aims to investigate what patient sociodemographic factors contribute to delays in presentation and treatment of TC.
Methods:
Using the National Cancer Database, we identified patients diagnosed with well-differentiated TC between 2004 and 2016 who underwent thyroidectomy. Multivariable regression analyses were conducted to examine the impact of race, insurance status, income, and distance from treatment facility on time to surgical treatment, stage, the presence of distant metastases, and tumor size.
Results:
We identified 89,105 patients diagnosed with well-differentiated TC who underwent thyroidectomy. Nonwhite patients who were uninsured or had Medicare or Medicaid insurance were more likely to experience delays in care, present with higher stages at diagnosis, and have distant metastases and larger tumors at presentation. Distance from treatment facility was associated with delays in surgical treatment and higher stage at presentation.
Conclusion:
Delays in TC presentation and surgical treatment vary by race, insurance status, and patient location. Health care policies should focus on targeting at-risk individuals to reduce health care disparities in this disease.
Introduction
Delays in diagnosis and treatment have been associated with worse outcomes in multiple diseases, especially in cancer wherein delays in treatment are directly correlated with increased risk of death. 1 Well-differentiated thyroid cancer (TC) has an overall good prognosis and typically progresses slowly. However, recent data demonstrate that even a 90-day delay in surgical treatment for TC is associated with higher all-cause mortality, although its association with disease-specific survival remains unclear. 2
Given that well-differentiated TC is an indolent slow-growing disease process, it is highly likely that the etiology of this outcome may have more to do with the specific patient population most at risk for delaying surgical care than with the surgical delay itself. This study aims to investigate which patient populations are most at risk for experiencing delay in diagnosis and treatment of well-differentiated TC.
Lead-time bias is of particular interest in slow growing, often indolent neoplasms such as TC or prostate cancer. Decreased access to care may lead to delayed diagnosis or difficulties in accessing timely surgical care once diagnosed. More regular health care visits may lead to detection of early stage disease that may have never progressed or has a less aggressive phenotype. This may result in patient populations with better access to care having lower apparent mortality due to increased detection of these tumors. 3 In TC, black patients have 23% higher risk of mortality than white patients. 2 Some authors attribute the disparity in TC survival between black and white patients primarily to lead-time bias. 3
A recent analysis challenged this through an analysis of the SEER database adjusted for socioeconomic status (SES) and screening habits, as well as tumor characteristics, finding that black patients had persistently decreased overall survival (OS) compared with white patients. 4 Unfortunately, this analysis did not evaluate the impact of these factors on surgical delay, nor adjust for surgical delay in the assessment of OS. The factors leading to surgical delay in TC have not been studied.
Given recent data demonstrating that surgical delay is a significant prognostic factor for worse OS, 2 it is important to understand which patient factors contribute to delays in initial presentation and treatment to identify high-risk populations that may benefit from targeted intervention. A study using the California Cancer Registry found that among patients with well-differentiated TC, higher odds of metastatic disease were found for minority patients, patients with low SES per the Yost's index of SES, and patients with Medicaid insurance; in addition, black patients were found to have higher overall mortality than other racial groups. 5
Another study investigated the disease stage on initial presentation in patients with differentiated TC in a public versus a university hospital in New York and found that patients at the public hospital were more likely to present with higher staged cancers. 6 This study aims to build upon previous research using a nation-wide comprehensive cancer database to investigate whether patient race/ethnicity, insurance status, median zip code income, and distance from treatment facility are associated not only with advanced disease at presentation but also with delayed treatment initiation once the diagnosis is made.
Methods
Data were extracted from the National Cancer Database (NCDB), a deidentified cancer registry that encompasses >1500 hospitals in the United States that are accredited by the Commission on Cancer. The NCDB is a joint endeavor of the Commission on Cancer of the American College of Surgeons and the American Cancer Society. The NCDB captures ∼70% of new cancer diagnoses as well as long-term patient outcomes. 7 This study was granted an exempt waiver by the institutional review board at Beth Israel Deaconess Medical Center.
Patient sample and variable selection
Patients ≥18 years old with papillary or follicular TC diagnosed between 2004 and 2016 were included. Papillary or follicular TC was identified using the International Classification of Diseases for Oncology, Third Edition (ICD-O-3) codes. Patients were excluded who received a primary treatment other than surgery, were diagnosed at the time of surgery, or had incomplete data.
Statistical analysis
Separate multivariable regression models were used to study four main outcome variables of interest: (1) delay from diagnosis to surgery (binary outcome: ≤90 days vs. >90 days), (2) advanced American Joint Committee on Cancer clinical stage at diagnosis (binary outcome: stage I vs. stages II, III, or IV), (3) metastasis at diagnosis (binary outcome: presence vs. absence of distant metastases), and (4) tumor size at diagnosis (binary outcome: tumors ≤1.5 or >1.5 cm based on various guidelines suggesting 1.5 cm as a cutoff value). 8 Multivariable logistic regression models were performed, and the results are reported as adjusted odds ratios (AORs).
Five main independent variables were examined: patient (1) sex, (2) race/ethnicity, (3) insurance status, (4) estimated household income based on zip code, and (5) distance from treatment facility.
Race/ethnicity was coded as the following: white, black, Hispanic (regardless of race), Asian, Pacific Islander, and Native American. Income was also a categorical variable based on the patient's zip code. The NCBD divides income into equally proportioned quartiles across all zip codes in the United States; these quartiles for the years included in this study are <$38,000, $38,000–$48,000, $48,000–63,000, and >$63,000. Distance from treatment facility, measured in miles, was divided into quartiles based on the final sample. Patient sex was included as listed on the database. Lastly, the type of TC (papillary and follicular) was included as a covariable to eliminate any confounding effect the specific diagnosis might have.
A separate one-way analysis of variance (ANOVA) with Bonferroni correction was performed to evaluate whether there is an association between type of surgery (binary variable: total thyroidectomy vs. all other thyroid surgery types removing less than the total thyroid) and patient race/ethnicity.
A chi-squared or R-squared statistic of <0.05 was used as an indication of appropriate model fit, and a p-value of <0.05 was considered statistically significant. All statistical analyses were conducted using Stata version 14.2 (Stata Corporation Ltd., College Station, TX).
Results
The database search returned 412,747 patients diagnosed with TC between 2004 and 2016. Of these, 89,105 patients fulfilled the study inclusion criteria and were included for analysis (Fig. 1). The characteristics of the original cohort of patients received from the NCDB query are described in Supplementary Table S1.
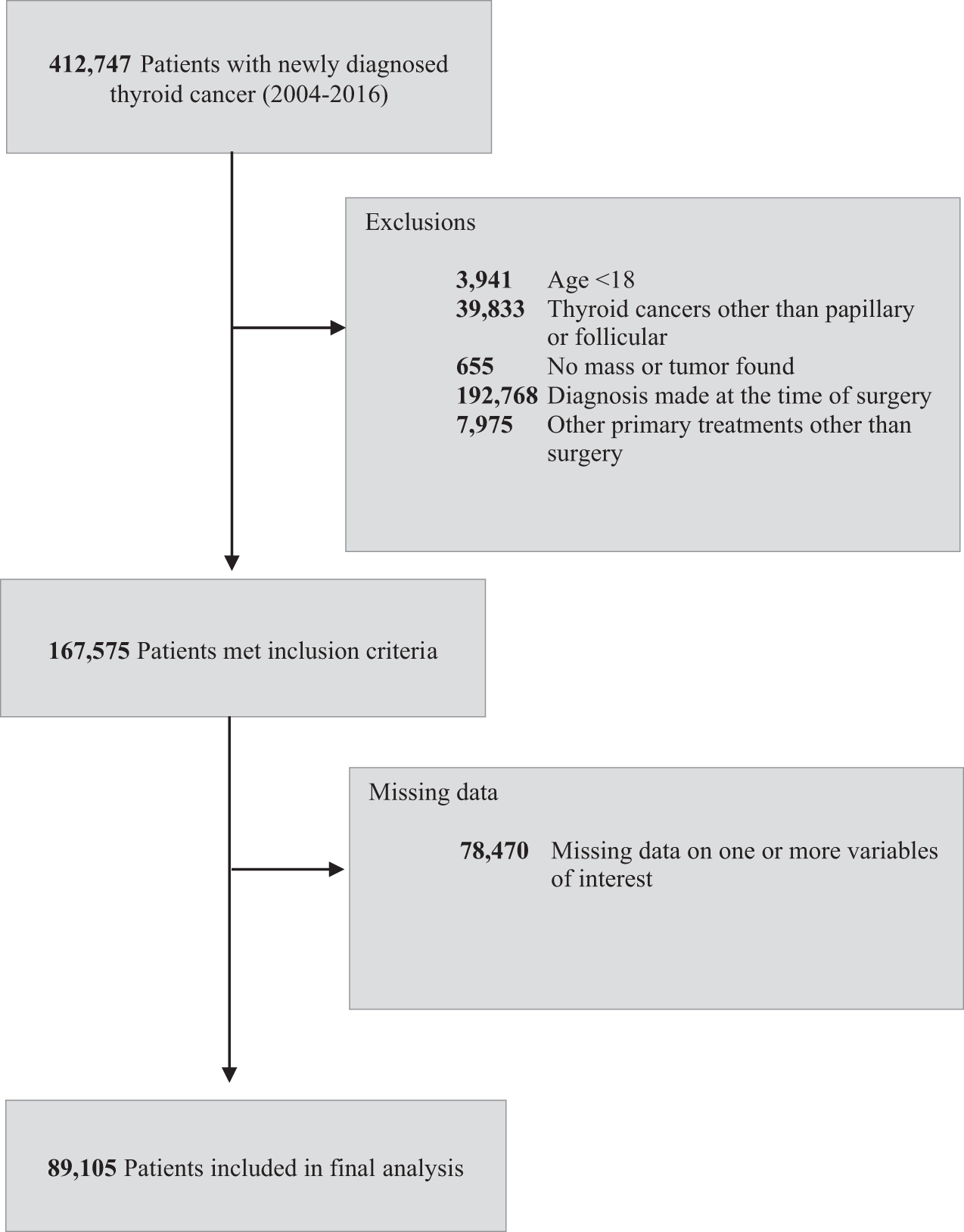
Inclusion and exclusion criteria.
Descriptive statistics
Baseline subject characteristics are noted in Table 1. Mean age was 48.8 years (SD = 15.4). The majority of patients were white (76.9%), female (74.0%), and had private insurance (70.1%). The median distance from the treatment facility was 17.9 km, the 25th percentile was 8.2 km, and the 75th percentile was 39.7 km. For statistical purposes, this variable was divided into four categories by quartiles: 0–25th percentile, 25th–50th percentile, 50–75th percentile, and >75th percentile. By cancer type, 85,525 had papillary TC (96.0%) and 3580 had follicular TC (4.0%).
Patient Characteristics
Median time from diagnosis to surgery was 37 days (IQR: 23–57) and median tumor size at presentation was 16 mm (IQR = 10–25). Patients who presented at stage I of disease comprised 70.9% (n = 63,174), while 12.8% presented at stage II (n = 11,404), 10.0% at stage III (n = 8872), and 6.3% at stage IV (n = 5655). Metastasis at diagnosis was found in 1616 patients, accounting for 1.8% of subjects.
Multivariable regression results
Table 2 lists the AORs when analyzing the impact of the five main independent variables of interest: (1) sex, (2) race/ethnicity, (3) insurance, (4) zip code income level, and (5) distance from the treatment facility, on the four main outcome variables of interest: (1) delays of >90 days elapsed between diagnosis and surgery (Fig. 2), (2) clinical stage at diagnosis (Fig. 3), (3) the presence of distant metastases at diagnosis (Fig. 4), and (4) tumor size at diagnosis (Fig. 5).
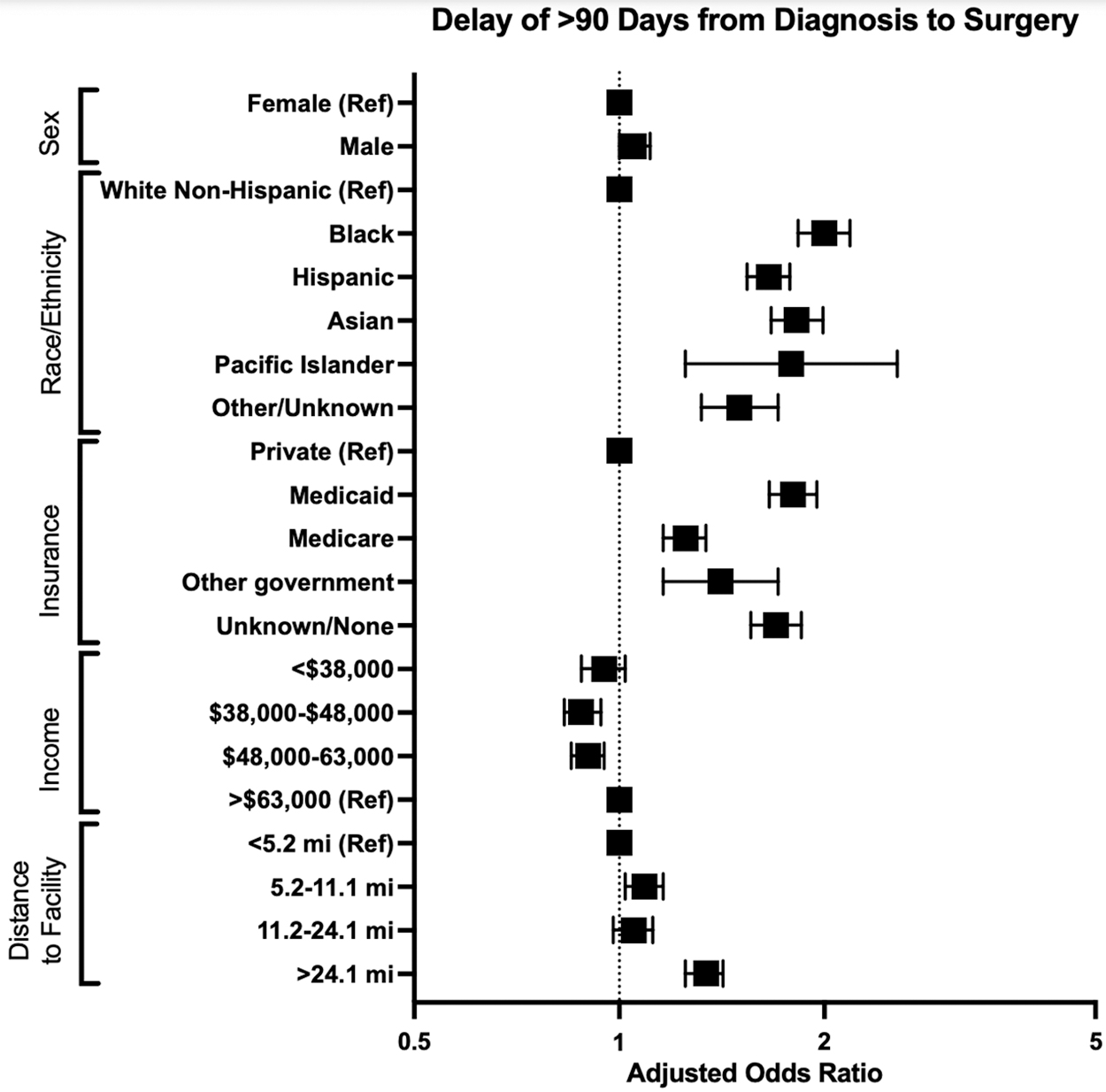
AOR, by sociodemographic factor, of undergoing surgical treatment >90 days after the diagnosis of thyroid cancer, as compared with undergoing surgical treatment ≤90 days after the diagnosis. Reference categories are labeled as “ref.” AOR, adjusted odds ratio.
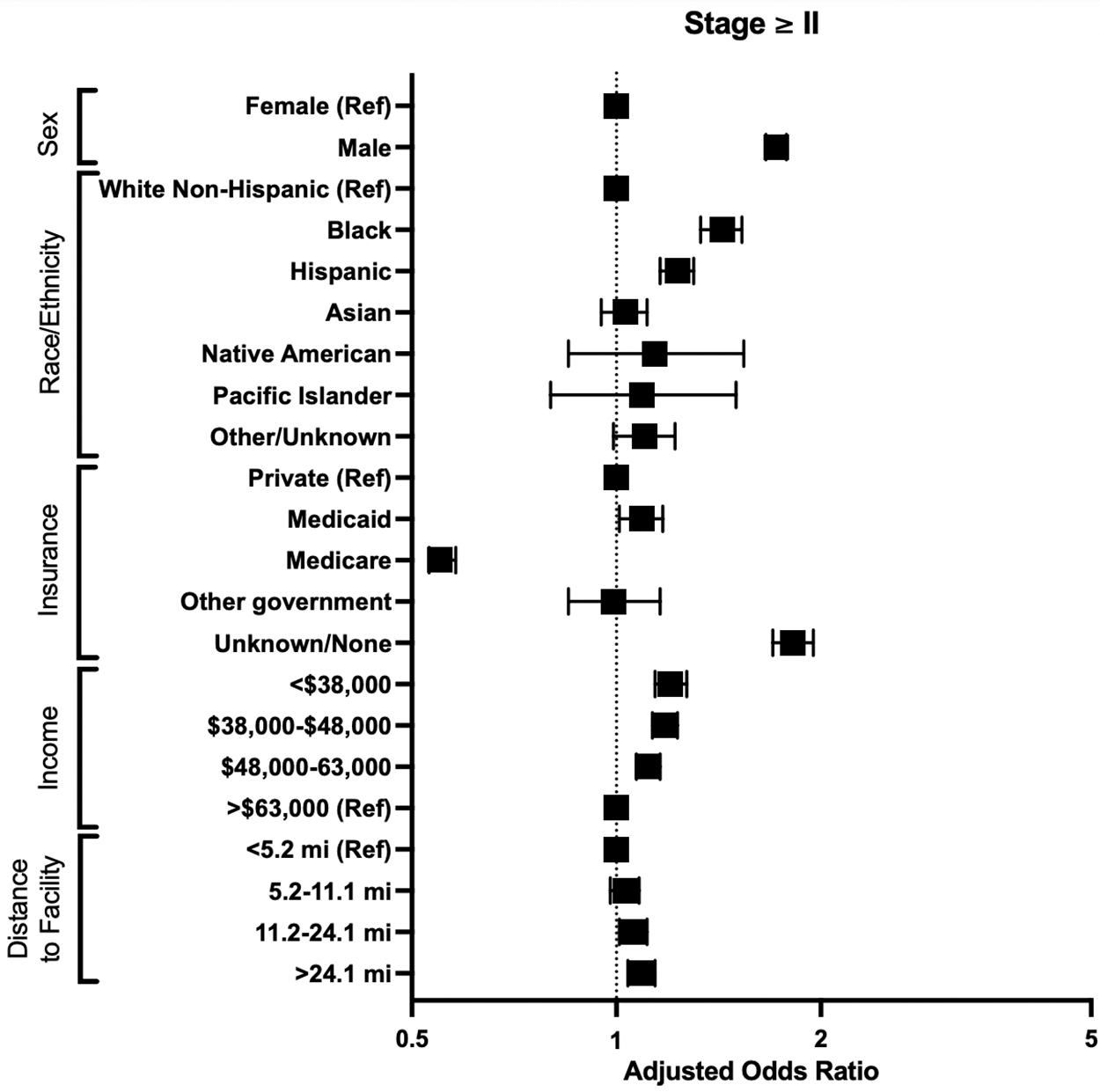
AOR, by sociodemographic factor, of presenting with a clinical stage of ≥II, as compared with presenting with a clinical stage of I. Reference categories are labeled as “ref.”
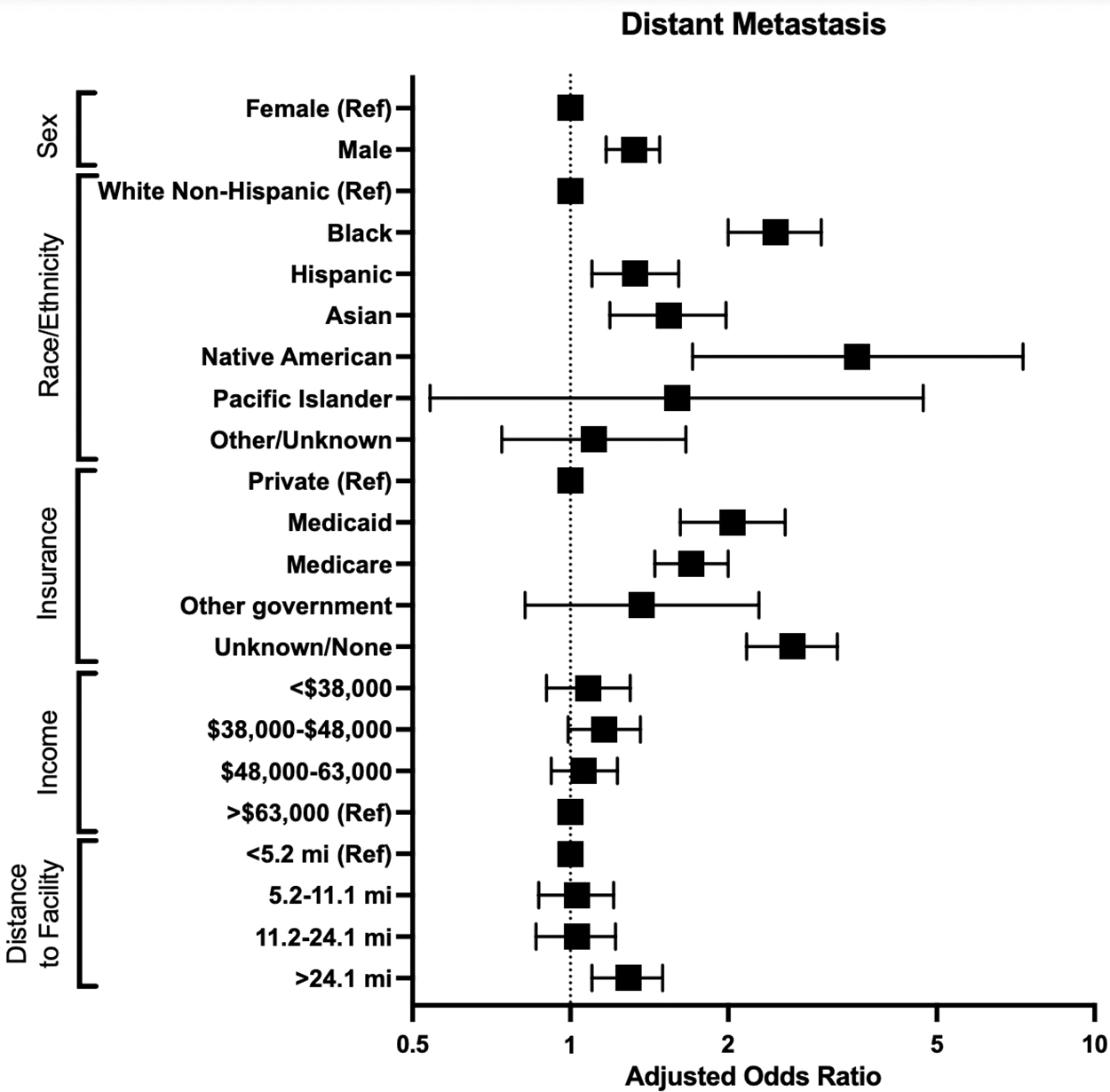
AOR, by sociodemographic factor, of presenting with positive lymph nodes, as compared with presenting with no evidence of metastasis. Reference categories are labeled as “ref.”
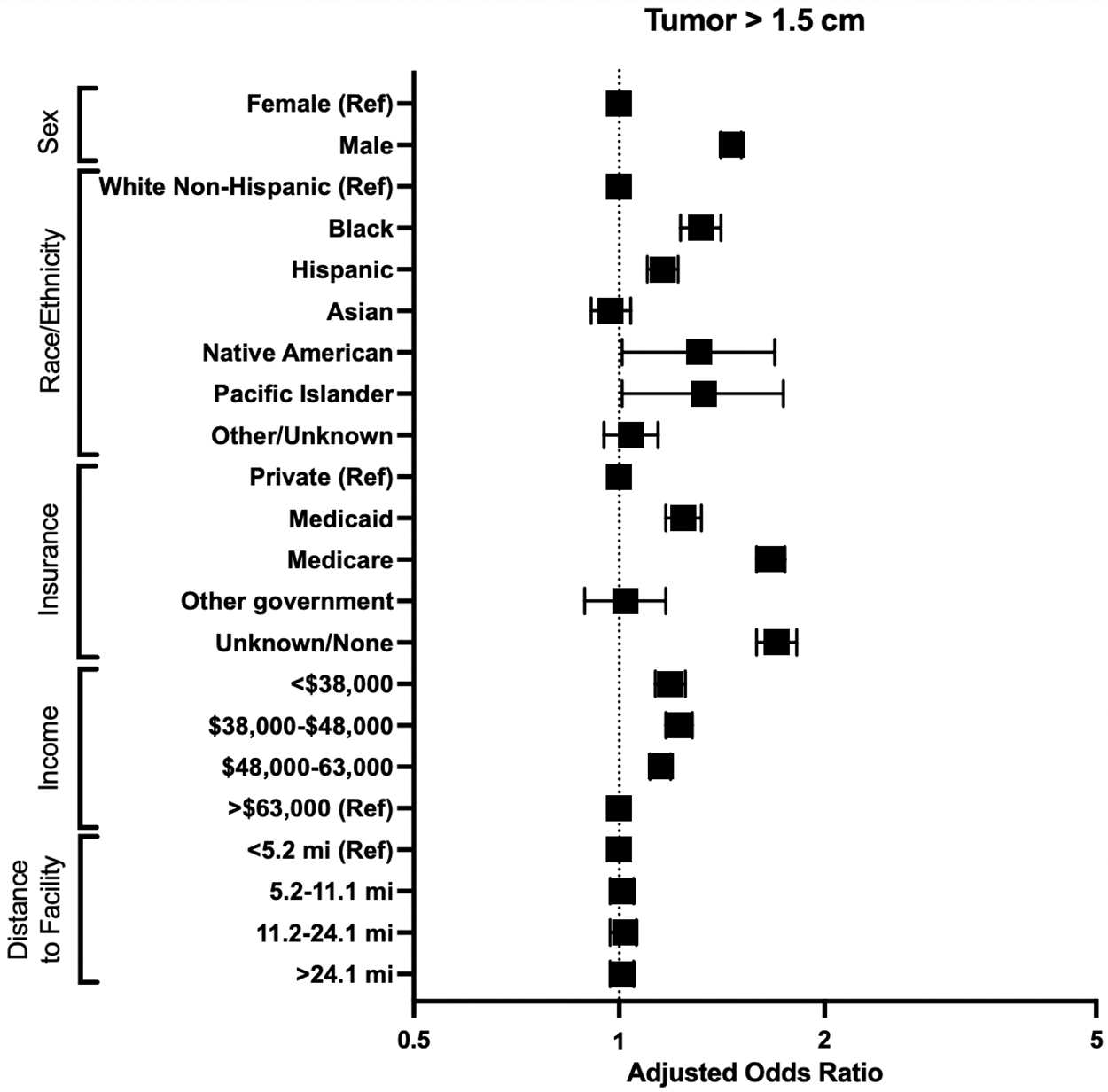
AOR, by sociodemographic factor, of presenting with tumors >1.5 cm, as compared with presenting with tumors <1.5 cm. Reference categories are labeled as “ref.”
Likelihood of Longer Time to Surgery, Higher Stage, Distant Metastases, and Larger Tumor Size by Patient Characteristic
Values listed as AOR (CI).
p ≤ 0.05.
p ≤ 0.01.
p ≤ 0.001.
AOR, adjusted odds ratio; CI, 95% confidence interval; Ref, used as reference value in regression analyses.
Males were more likely than females to present with higher stage disease, distant metastases, and tumors >1.5 cm. As compared with white patients, all nonwhite patients had higher likelihood of having surgery >90 days after their diagnosis, with blacks and Hispanics also having higher likelihoods of presenting at a higher stage and with tumors >1.5 cm. Blacks were 2.46 more likely than whites to present with distant metastases; similarly, Hispanics were 1.33 times more likely, Asians were 1.54 times more likely, and Native Americans were more than 3 times more likely than whites to present with distant metastases.
Moreover, when compared with privately insured patients, patients with Medicaid, Medicare, or no insurance had higher likelihood of having a delay in surgery of >90 days or presenting with a higher stage disease, with metastases, and with tumors >1.5 cm. Patients with Medicaid or with no insurance were more than twice as likely to have distant metastases as compared with privately insured patients. Furthermore, when compared with the highest income quartile, patients pertaining to lower income quartiles were more likely to present with higher stage of disease and with tumors >1.5 cm.
Patients in lower income quartiles were less likely to experience a delay in surgery of >90 days. Lastly, patients living >24.1 miles from the treatment facility were more likely to undergo surgery >90 days after diagnosis and were more likely to present with higher stage disease and with distant metastases, compared with patients living <5.1 miles from the treatment facility.
On a separate ANOVA, a difference was found between surgery type (total thyroidectomy vs. all other thyroid surgery types) (p < 0.001). On analysis per race/ethnicity, white patients were more likely to get a total thyroidectomy as compared with black patients (p = 0.040) and other/unknown race (p < 0.001), and white patients were less likely to get a total thyroidectomy compared with Asian patients (p < 0.001). There was no difference between white patients and Hispanics (p = 0.14), Native Americans (p = 1.00), or Pacific Islanders (p = 1.00).
Discussion
In this study, we assessed the patient factors associated with more advanced TC presentation and treatment in patients with well-differentiated TC. We found that nonwhite patients, nonprivately insured patients, and patients who live farther from the treating facility are generally more likely to present with more advanced disease (i.e., larger tumor size, presence of metastases, and/or higher stage) and less likely to begin prompt surgical treatment once the diagnosis is made. Those in zip codes with lower median incomes are likewise more likely to present with more advanced disease, but less likely to present with a delay to surgery. Furthermore, male sex was also a risk factor consistently associated with more advanced cancers but not with delay in surgical treatment.
Longer delays in surgical treatment are associated with increased risk of overall mortality in TC. We previously demonstrated in a study of the NCDB that time to surgery of 91–180 days, versus 0–90 days, increased the hazard ratio for overall mortality rate by 30%. 2 However, this analysis may have been limited by residual confounding and the inability to assess disease-specific survival. In this study, our findings reveal that race/ethnicity, income, insurance, and distance from treatment facility are associated with delays in TC care, and, therefore, may be associated with increased overall mortality in these patients.
Our findings are consistent with investigations of factors affecting surgical delay for other malignancies. A recent systematic review found that non-Caucasian race, academic setting, and Medicaid/no insurance all led to increased delay in treatment initiation for squamous cell head and neck cancers. 9 Black women, compared with white women, are 73% more likely to have a treatment delay >60 days for breast cancer. 10 In lung cancer, black patients are 66% less likely to receive timely and appropriate therapy. 11 Across several invasive cancers, black patients and Medicaid patients were less likely to receive guideline-concordant care, which was associated with increased mortality. 12
In this study, male patients presented with more advanced disease. This is consistent with literature finding that men are less engaged with their health and are less likely to make health care visits. 13 In addition, racial and ethnic minority groups, independent of other socioeconomic factors, were more likely to experience delays in care—some groups more than twice as likely—when compared with white patients. Health care disparities based on race and ethnicity are common—TC is no exception.
Patients without private insurance also fared worse compared with their privately insured counterparts. Access to health care is dictated by insurance status. Uninsured individuals are less likely to have a usual source of health care and thus are more likely to have unmet medical needs. 14 After universal insurance expansion in Massachusetts, patients with TC were 26% more likely to undergo thyroidectomy. 15 For cancers that are routinely screened for, uninsured patients are more likely to present with advanced disease. 16
In addition, our results also demonstrate higher likelihood of delays and more advanced disease in patients with Medicare and Medicare insurance. This is also consistent with prior studies that have reported that cancer patients with Medicare and/or Medicaid insurance are less likely to receive the recommended radiation and/or chemotherapy and to have the necessary lymph nodes removed. 17
Individuals living in lower income zip codes more often had surgery within 90 days than their higher income zip code counterparts. This result is unexpected, as lower incomes have been associated with poorer access to health care. 18 This may be due to more advanced disease at presentation (known or suspected) resulting in more expeditious time to surgery, as patients with lower incomes were found to have higher likelihood of metastasis at presentation, larger tumors at presentation, and higher staged cancers.
This could be partly due to limitations in the NCDB database, which does not provide individual-level income data, but instead provides the median income of the zip code where the patient resides as a proxy. Lastly, further distance from treatment facility was associated with delays in surgery and presentation with more advanced disease. This is consistent with breast cancer studies that have found that patients with less geographic proximity to radiation therapy facilities are less likely to receive radiation treatment. 19
However, recent findings in differentiated TC have found that further distance to treatment facility could paradoxically lead to improved outcomes given that individuals residing in high-income areas were more likely to travel to a centralized cancer surgery center, leading to higher OS. 20 Therefore, the effect of distance from treatment facility, as well as the other variables investigated in this study, affects delays in surgery for TC in ways that are extremely complex and incompletely understood with the limited data the NCDB provides. These variables were separately studied to minimize confounding bias; however, in real-world applications, they are undeniably working interconnectedly and not as easily separable from one another.
Key strengths of utilizing the NCDB for this study include detailed staging and treatment data, in addition to a large patient population capturing most new cancer diagnoses in the United States. However, there are several inherent limitations of utilizing a large clinical database and some specific to the NCDB. While the NCDB captures ∼70% of new cancer diagnoses in the United States, there is selection bias for patients treated at primarily large academic medical centers. The health disparities found in this study could be even more extreme in nonacademic clinical settings for which the NCDB does not have information.
Moreover, income data are imputed based upon the average in a patient's zip code of residence and not the individual patients' income. Variations in diagnosis and treatment coding may exist both temporally and geographically. Finally, the NCDB does not capture reasons for delayed initiation of treatment or the prediagnostic work-up. Mixed-method studies may be ideal to determine the underlying barriers to timely diagnosis and treatment in these populations at high risk for delay.
Overall, more work needs to be done to combat disparities in diagnosis and treatment of TC. Federal and state health programs must aim to provide better access to care for disadvantaged individuals, which will contribute to the timely diagnosis of their existing medical conditions. Once the diagnosis is made, clinicians and other health care workers must be particularly attentive of these vulnerable patient populations to avoid losing them to follow up and ensure proper adherence to the recommended treatments. Regardless of the methods of the programs implemented, initiatives need to be thoughtful, meticulous, and intentional at reducing health care disparities.
Footnotes
Acknowledgments
G.W.R. acknowledges the ongoing philanthropic support of Mike & Eliz Ruane, John & Claire Bertucci, Ben & Ellen Harvey, and Diana Ryan for his research efforts.
Authors' Contributions
B.L. contributed to conceptualization (lead), formal analysis (lead), methodology (lead), visualization (equal), writing original draft (equal), reviewing, and editing (equal). S.C.F. was involved in formal analysis (supporting), methodology (supporting), visualization (equal), writing original draft (equal), reviewing, and editing (equal). G.W.R. was in charge of methodology (supporting), supervision (equal), reviewing, and editing (equal). B.C.J. took charge of methodology (equal), supervision (equal), reviewing, and editing (equal).
Author Disclosure Statement
B.L., S.C.F., and B.C.J. have no conflicts of interest. G.W.R. is the president of the International Thyroid Oncology Group (ITOG) and the World Congress on Thyroid Cancer (WCTC), is chair of the Administrative Division of the American Head and Neck Society (AHNS), and is the American College of Surgeons (ACS) Otolaryngology Governor.
Funding Information
B.L. and B.C.J. have no funding information to declare. S.C.F. was supported in part by NIH T32 grant 5T32HL007734. G.W.R. has received research grants (no personal fees) from Eisai, Medtronic, and Fluoptics, and is the program director of the Massachusetts Eye & Ear Infirmary Endocrine Surgery Clinical Fellowship, which receives partial funding from Medtronic.
Supplementary Material
Supplementary Table S1