
Abstract
Background:
A theranostic probe for accurate staging and treatment is crucial for the management of medullary thyroid cancers (MTCs). The abundance of stroma in most of thyroid cancers, including MTC, opens new avenues for selecting cancer-associated fibroblasts (CAFs) as new molecular imaging and therapeutic targets. [68Ga]Ga-labeled fibroblast activation protein inhibitor (FAPi) molecules have gained importance as alternative molecular imaging agents in the imaging of thyroid cancers. The purpose of this study was to compare the detection efficiency of primary and metastatic lesions of MTCs between [68Ga]Ga-DOTA.SA.FAPi and [68Ga]Ga-DOTANOC positron emission tomography (PET) radiotracers.
Materials and Methods:
In this retrospective study, [68Ga]Ga-DOTANOC and [68Ga]Ga-DOTA.SA.FAPi PET/CT (computed tomography) images were compared using patient-based and lesion-based analysis in patients with MTC for follow-up assessment. The quantitative assessment included comparing standardized uptake values corrected for lean body mass (SULpeak) and tumor-to-background ratios (TBR). The findings on both scans were validated with the morphological findings of the diagnostic CT.
Results:
Twenty-seven patients (21 males and 6 females) with a mean age of 42.4 ± 13.2 years (range 14–66 years) were included in the study. [68Ga]Ga-DOTA.SA.FAPi had similar sensitivities as that of [68Ga]Ga-DOTANOC PET/CT for detecting primary tumors (100% [18 of 18] vs. 94.4% [17 of 18], p = 0.979) involved lymph nodes (98.3% [118 of 120] vs. 95% [114 of 120], p = 0.288), and brain metastases (100%). [68Ga]Ga-DOTA.SA.FAPi demonstrated significantly higher sensitivities than [68Ga]Ga-DOTANOC PET/CT for detecting lung nodules (93.5% [87 of 93] vs. 68.9% [64 of 93], p < 0.0001), liver (100% [105 of 105] vs. 46.4% [49 of 105], p < 0.0001), bone (92.4% [110 of 119] vs. 76.5% [91 of 119], p = 0.001), and pleural metastases 98.2% versus 0%. Higher uptake values and TBR values were reported with [68Ga]Ga-DOTA.SA.FAPi compared with that of [68Ga]Ga-DOTANOC.
Conclusion:
[68Ga]Ga-DOTA.SA.FAPi outperformed [68Ga]Ga-DOTANOC PET/CT in the detection of distant metastases with both patient-based and lesion-based analysis in MTCs.
Introduction
Medullary thyroid cancer (MTC) is a type of neuroendocrine tumor (NET) derived from the thyroid C cells and accounts for <5% of thyroid cancers. 1,2 MTCs do not often accumulate radioiodine and hence not responsive to radioiodine treatment. In this subtype of thyroid cancer, positron emission tomography (PET) imaging modalities, including [ 18 F]F-FDG, [ 18 F]F-Fluorodopa (FDOPA), and [68Ga]Ga-DOTA-labeled somatostatin analogs (SSAs), are used in the initial diagnosis, restaging, treatment assessment, and follow-up surveillance. 3,4
As compared with the other NETs, the tumor detection rate on somatostatin receptor (SSTR)-based PET or PET/CT (computed tomography) in recurrent MTC is only 63.5%, as depicted in a meta-analysis by Treglia et al. And as per the European Association of Nuclear Medicine (EANM) practice guideline for PET/CT imaging in medullary carcinoma thyroid, SSTR PET/CT needs to be considered only in cases with inconclusive imaging results with [ 18 F]F-FDOPA, and [ 18 F]F-FDG PET/CT results and to assess the feasibility of peptide receptor radionuclide therapy (PRRT). 3
Currently, there is no ideal PET tracer with an optimal detection rate for MTC. Hence, developing theranostic probes with promising detection rates and with a possible therapeutic dimension is crucial and could be a potential added value for the substantial improvement of the management of MTCs.
Activated fibroblasts, that is, cancer-associated fibroblasts (CAFs) comprise the crucial components of the tumor microenvironment (TME) and are abundantly expressed in various subtypes of thyroid cancers, including MTC. 5 –7 The bidirectional interaction of the CAFs with the tumor cells facilitates new imaging and therapeutic targets. 5,7 Recent investigations with gallium-68 labeled fibroblast activation protein (FAP) inhibitors have demonstrated a significant theranostic role of fibroblast activation protein inhibitor (FAPi) in various cancers, including thyroid cancer, 8 but not much has been explored on its role in MTC. In this retrospective study, we aimed to conduct a head-to-head comparison of [68Ga]Ga-DOTA.SA.FAPi with [68Ga]Ga-DOTANOC PET/CT imaging for the follow-up surveillance of patients with MTC.
Materials and Methods
This retrospective study was approved by the “All India Institute of Medical Sciences institute ethics committee,” New Delhi, India, and was completed in accordance with the Helsinki Declaration (Ref. No. IECPG: 22/27). Written informed consent was obtained from all patients who participated in the study, for the imaging, use of clinical information to analyze data, and use of images for publication purposes. This study is a collaboration between the Department of Nuclear Medicine, Medical Oncology at All India Institute of Medical Sciences, and the Department of Chemistry, Johannes Gutenberg University, Mainz, Germany, which provided the labeling precursor as depicted in Figure 1.

Chemical structure of the labeling precursor
Patients fulfilling the following eligibility criteria were enrolled in the study: patients with histologically proven MTC, and patients who underwent both [68Ga]Ga-DOTANOC and [68Ga]Ga-DOTA.SA.FAPi PET/CT within a time interval of 1 month, and patients who did not receive any anticancer treatment within 4 weeks. Patients with a known inflammatory condition, dual malignancies, pregnant patients, and those unwilling to undergo two PET/CT scans were excluded from the study. According to the eligibility criteria, 27 patients were included in the study (Fig. 2).

Patient flow diagram.
Synthesis of [68Ga]Ga-DOTA.SA.FAPi and quality control
Radiolabeling of [68Ga]Ga-DOTA.SA.FAPi was conducted as detailed in our previous publications. 8
PET/CT acquisition
The mean injection doses of [68Ga]Ga-DOTA.SA.FAPi and [68Ga]Ga-DOTANOC were 185 MBq. After 60 minutes of intravenous administration of both radiotracers, scans were obtained on a 128-slice GE Discovery 710* 128 Slice PET/CT Scanner with a 40 mm detector at a 0.35-second rotation speed. The patient was in the supine position for all acquisitions. The scans included a CT and a PET scan after a preliminary scout image, to establish the field of view. A diagnostic dosage CT with parameters of 300–380 mAs, 120 kVp, slice thickness 3.75 mm, and pitch 0.6 was used for the CT scan. In patients with brain metastases, spot images were obtained with a slice thickness of 1.25 mm on CT at 120 kVp, 300–380 mAs, and a pitch of 0.6, as needed. A GE Xeleris workstation was used for image processing and analysis. For [68Ga]Ga-DOTANOC and [68Ga]Ga-DOTA.SA.FAPi PET/CT, image capture, and analysis entailed a qualitative and quantitative comparison of the tracers.
Data interpretation
To assess the diagnostic ability of both the radiotracers, patient-based and lesion-based analyses were conducted in both primary and metastatic lesions. Two nuclear medicine physicians with more than 15 years of expertise in interpreting PET/CT scan results independently evaluated and processed both [68Ga]Ga-DOTA.SA.FAPi and [68Ga]Ga-DOTANOC PET/CT scans. They were unaware of the patients' clinical history and histopathological examinations (HPE) status. Any discrepancies in the interpretation were discussed and resolved by consensus.
Data analysis and processing
The qualitative analysis included a visual judgment of radiotracer uptake, which was validated by morphological findings on CT, the reference standard. When radiopharmaceutical uptake was greater than the background, a lesion was considered positive on PET. The uptake in the lesions on both scans were compared with the CT counterpart's morphological features/characteristics. A three-dimensional auto-contour region of interest (ROI) at a 40% SULpeak threshold was carefully drawn around the site of [68Ga]Ga-DOTANOC and [68Ga]Ga-DOTA.SA.FAPi expressing lesions on transaxial images for quantitative comparisons.
To quantitatively compare the uptake in the lesions between the radiotracers, the ROIs were presented as standardized uptake value (SUV) corrected for lean body mass: SULpeak. The SUV values (peak, average, median, and range) for both [68Ga]Ga-DOTANOC and [68Ga]Ga-DOTA.SA.FAPi were recorded for each site. The tumor-to-background ratio (TBR) was calculated by dividing the SULpeak of the primary tumor/metastases by the corresponding background SULpeak values.
Definitions
True-positive lesion
Uptake in the lesion seen on [68Ga]Ga-DOTANOC/[68Ga]Ga-DOTA.SA.FAPi PET/CT images were higher than the background and were found to be positive on diagnostic CT/histological examination.
False-positive lesion
Uptake in the lesion seen on [68Ga]Ga-DOTANOC/[68Ga]Ga-DOTA.SA.FAPi PET/CT images were higher than the background and were found to be negative on diagnostic CT/histological examination.
True-negative lesion
No uptake seen on [68Ga]Ga-DOTANOC/[68Ga]Ga-DOTA.SA.FAPi PET/CT images were higher than the background and the results on diagnostic CT/histological examination.
False-negative lesion
Lesions that were missed in [68Ga]Ga-DOTANOC/[68Ga]Ga-DOTA.SA.FAPi PET/CT images higher than the background were found to be positive for malignancy at diagnostic CT/histological examination.
Statistical analysis
Statistical analysis was performed using MedCalc statistical software (v15.0). Continuous variables were presented in terms of mean, median, standard deviation, range, and interquartile range (IQR). [68Ga]Ga-DOTANOC and [68Ga]Ga-DOTA.SA.FAPi uptakes were compared using Wilcoxon signed-rank test. The sensitivities of [68Ga]Ga-DOTANOC and [68Ga]Ga-DOTA.SA.FAPi PET/CT examinations were calculated and compared. p-Values ≤0.05 were considered significant. Indeterminate results from the [68Ga]Ga-DOTA.SA.FAPi and [ 18 F]F-FDG PET/CT tests were approached as false-negative (FN) or false-positive using a diagnostic quality CT scan as the reference standard. Participants with missing data, including histopathology, tests, or reference standard imaging, were excluded from the analysis (Fig. 2).
Results
Twenty-seven patients with MCT (21 males and 6 females) with a mean age of 42.4 ± 13.2 years (range 14–66 years) were found eligible and were included in the study analysis. Post-intravenous injection of [68Ga]Ga-DOTA.SA.FAPi, all vital parameters remained normal and no adverse events were noted. All the patients underwent a minimum of two lines of prior treatments. The median serum calcitonin levels at the time of imaging were 666.5 pg/mL (25–75% IQR: 389–1145 pg/mL). Twenty-four patients underwent total thyroidectomy and nodal dissection. Fourteen patients (52%) previously received kinase inhibitors, four took mammalian target of rapamycin (mTOR) inhibitors, six patients received local radiotherapy to the neck, seven received palliative radiotherapy to the distant metastatic sites, and four patients received [177Lu]Lu-DOTATATE therapy (Table 1).
Demographics and Clinical Characteristics of Patients
IQR, interquartile range; MTC, medullary thyroid cancer; mTOR, mammalian target of rapamycin; SD, standard deviation; TKI, tyrosine kinase inhibitor.
Comparison of lesion detection and uptake between [68Ga]Ga-DOTANOC and [68Ga]Ga-DOTA.SA.FAPi PET/CT scans
Primary tumor
Among the 27 patients, 18 remnants were identified on diagnostic CT. Intense uptake of [68Ga]Ga-DOTA.SA.FAPi was noted in all the 18 lesions (100%). However, [68Ga]Ga-DOTANOC identified/showed expression in 17 lesions (94.4%, confidence interval [CI]: 78.2–99.5%; p = 0.979). The median SULpeak values were comparable between the tracers (SULpeak [68Ga]Ga-DOTA.SA.FAPi: 6.5; [IQR: 5–8.5], vs. [68Ga]Ga-DOTANOC: 5.3; [IQR: 5.1–7.5, p = 0.206]) (Table 2). The TBR was significantly higher in [68Ga]Ga-DOTA.SA.FAPi than in [68Ga]Ga-DOTANOC (SULpeak; [68Ga]Ga-DOTA.SA.FAPi: 5.5 [IQR: 4.7–7.7] vs. [68Ga]Ga-DOTANOC: 1.3 [IQR: 0.1–1.5]; p < 0.0001).
Comparison of Various Parameters Between [68Ga]Ga-DOTA.SA.FAPi and [68Ga]Ga-DOTANOC Positron Emission Tomography/Computed Tomography Imaging
Not done.
CT, computed tomography; FAPi, fibroblast activation protein inhibitor; SULpeak, peak SUL (standardized uptake value corrected for lean body mass) in a spherical 1-cc Volume of Interest; SUV, standardized uptake value; TBR, tumor-to-background ratio.
Lymph node metastases
Twenty-two (81.5%) out of 27 patients had a total of 120 lymph node (LN) metastasis on CT. While [68Ga]Ga-DOTA.SA.FAPi correctly diagnosed 98.3% (118/120; CI: 94–99.7%) of LN metastases (true-positive [TP]: 118, FN: 2), [68Ga]Ga-DOTANOC diagnosed 95% (114/120; CI: 89.4–98%; TP: 114, FN: 6); p = 0.288. However, The SULpeak and TBR values of the LNs were significantly higher for [68Ga]Ga-DOTA.SA.FAPi (SULpeak; [68Ga]Ga-DOTA.SA.FAPi: 6.9 [IQR: 5.9–9] vs. [68Ga]Ga-DOTANOC: 6 [IQR: 5.4–8.1]; p = 0.031; TBR SULpeak; 5.8 [IQR: 0–8.1] vs. 4.1 [IQR: 0–5.2]; p = 0.003) (Table 2).
Lung metastases
Lung metastases were detected on CT in 16 patients (59.3%). Both [68Ga]Ga-DOTA.SA.FAPi and [68Ga]Ga-DOTANOC showed concordant findings in 13 (81.3%) patients. On detailed lesion-based analysis, out of 93 lung nodules identified on CT, [68Ga]Ga-DOTA.SA.FAPi diagnosed 87 (93.5%, CI: 86.4–97.5%) while [68Ga]Ga-DOTANOC diagnosed 64 (68.9%; CI: 58.4–78%) lesions (p < 0.0001). Similarly, SULpeak and TBR uptake parameters were remarkably higher on [68Ga]Ga-DOTA.SA.FAPi PET compared with that of [68Ga]Ga-DOTANOC (Table 2).
Liver metastases
Thirteen (48.2%) patients out of 27 patients had liver metastasis on CT and [68Ga]Ga-DOTA.SA.FAPi has shown completely concordant findings in all 13 (100%) patients. In contrast, [68Ga]Ga-DOTANOC detected liver metastases in 77% (10/13; CI: 67.7–84.6%) patients. [68Ga]Ga-DOTA.SA.FAPi correctly diagnosed all the liver lesions (105/105), but [68Ga]Ga-DOTANOC could detect only 46.6% (49/105; CI: 36.8–56.5%) liver lesions (p < 0.0001) (Figs. 3 and 4), among whom [68Ga]Ga-DOTANOC completely failed to detect any liver metastases in two patients (Fig. 3). The SULpeak of the liver lesions was higher in [68Ga]Ga-DOTA.SA.FAPi than that in [68Ga]Ga-DOTANOC (SULpeak; [68Ga]Ga-DOTA.SA.FAPi: 6 [IQR: 5.4–11.2] vs. [68Ga]Ga-DOTANOC: 2.2 [IQR: 0.4–5.7]; p = 0.041)(Table 2). Similarly, the TBR values were significantly higher (p = 0.031) with [68Ga]Ga-DOTA.SA.FAPi: 4.8 (IQR: 3.1–5.5) compared with that of [68Ga]Ga-DOTANOC: 0.7 (IQR: 0.3–1.4).
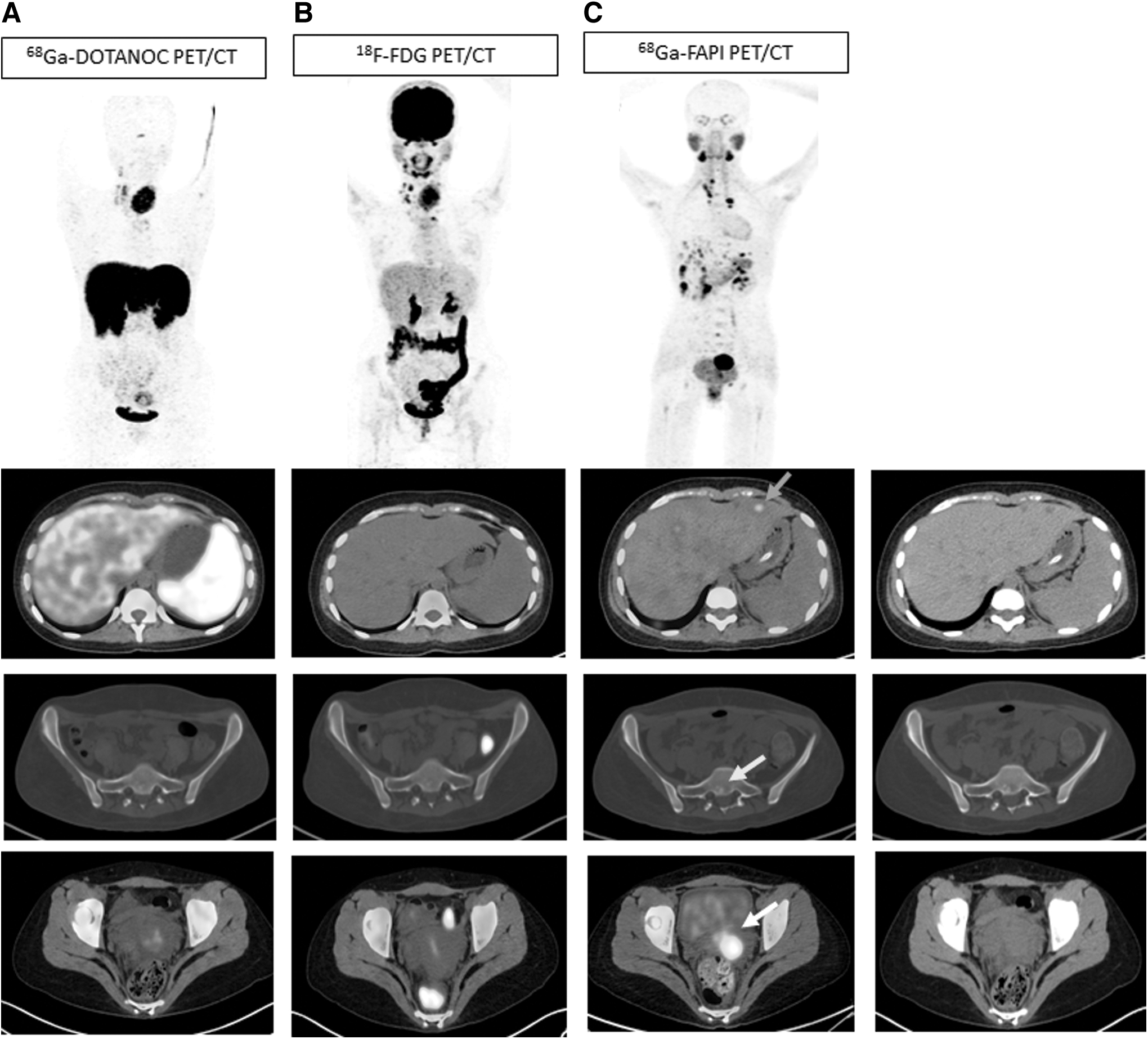
An 18-year-old female patient presented with a painless neck swelling, which on evaluation by fine needle aspiration cytology was suspicious of medullary carcinoma thyroid. Biochemically baseline serum calcitonin level and CEA levels were 54,800 pg/mL and 3909 ng/mL, respectively. The baseline [68Ga]Ga-DOTANOC PET/CT was performed for metastatic workup, which revealed the neck primary with bilateral neck and mediastinal lymph nodes with a few sclerotic skeletal lesions with no SSTR expression (
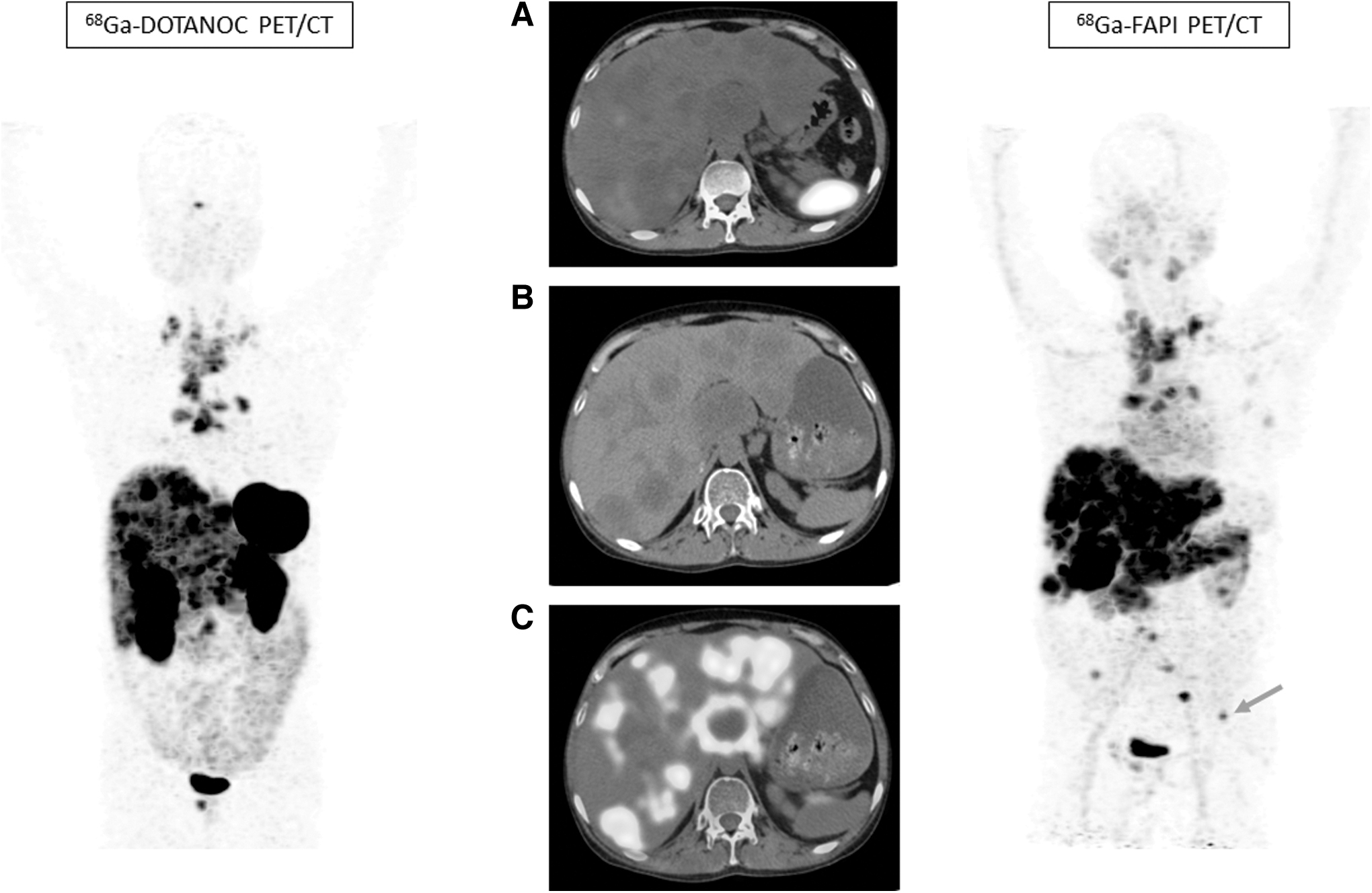
A 25-year-old male with biopsy-proven medullary thyroid carcinoma was referred for baseline staging. [68Ga]Ga-DOTANOC PET/CT (
Bone metastases
Bone lesions were classified according to the number of bone metastasis (Table 2). Among the 12 (44.4%) patients with radiological bone metastases, these were diagnosed in 91.6% (11/12; CI: 61.4–99.7%) of patients with [68Ga]Ga-DOTA.SA.FAPi and 83.3% (10/12; CI: 51.5–97.9%) patients (p = 0.998) with [68Ga]Ga-DOTANOC PET/CT. Out of 119 bone lesions seen in CT, [68Ga]Ga-DOTA.SA.FAPi diagnosed more lesions than [68Ga]Ga-DOTANOC {Number of bone lesions; [68Ga]Ga-DOTA.SA.FAPi: 110 (92.4%, CI: 86.6–96%) vs. [68Ga]Ga-DOTANOC: 91 (76.5%, CI: 67.8–83.7%), p = 0.001} (Figs. 3 and 4). The SULpeak values for bone lesions were 5.8 (IQR: 4.5–11.6) with [68Ga]Ga-DOTA.SA.FAPi and 1.9 (IQR: 1.6–3.9) with [68Ga]Ga-DOTANOC (p = 0.114). However, TBR values were significantly higher in 68Ga]Ga-DOTA.SA.FAPi compared with [68Ga]Ga-DOTANOC {SULpeak; [68Ga]Ga-DOTA.SA.FAPi: 5.8 (IQR: 4.6–9.7) vs. [68Ga]Ga-DOTANOC: 1.5 (IQR: 0.7–2.1); p = 0.0002} (Table 2).
Brain metastases
Both radiotracers had completely concordant findings with the radiological findings in all three patients with brain metastasis (3/3) in all 11 brain lesions. The SULpeak values were not different between the radiotracers (SULpeak; [68Ga]Ga-DOTA.SA.FAPi: 6 [IQR: 3.4–6.9] vs. [68Ga]Ga-DOTANOC: 4.2 [IQR: 2.1–6.2]; p = 0.130). However, The TBR values are 12 (IQR: 1.9–914.2) and 8 (IQR: 5.2–10.9) in the [68Ga]Ga-DOTA.SA.FAPi and [68Ga]Ga-DOTANOC, respectively (p = 0.145).
Other distant metastases
Pleural thickening was detected in three patients with higher detection rates and uptake patterns with [68Ga]Ga-DOTA.SA.FAPi. Both SULpeak and TBR values for the pleural metastases were notably higher with [68Ga]Ga-DOTA.SA.FAPi: 4.3 (IQR: 2–6.6) than that of [68Ga]Ga-DOTANOC: 2.1 (IQR: 1.9–5.1); p = 0.0001 (TBR SULpeak: 3.2 [IQR: 1.1–4.2] vs. 1.6 [0.6–2.3]; p = 0.002) (Table 2).
Effect of prior tyrosine kinase inhibitor/mTOR inhibitor treatment on the uptake values
A subgroup analysis to explore the influence of previous tyrosine kinase inhibitor (TKI)/mTOR inhibitor treatment on the SUL values revealed no difference in the radiotracer uptake on both [68Ga]Ga-DOTA.SA.FAPi and [ 18 F]F-FDG PET scans (Table 3).
Comparison of Uptake Values According to Prior Exposure to Other Anticancer Treatment Options
Discussion
Several PET radiotracers such as [ 18 F][F-FDG, [68Ga]Ga-DOTA-labeled SSTR analogs, and [ 18 F]F-FDOPA have been used for the imaging of MTCs, of which [ 18 F]F-FDOPA shows the best detection efficiency. 3,9 Currently, according to EANM guidelines, FDOPA should be preferred, but Gallium-68 DOTA-labeled SSTR imaging may be useful in cases of inconclusive diagnosis of FDOPA and to assess the feasibility of peptide receptor targeted radionuclide therapy. 3 Despite being a valuable theranostic option, a meta-analysis involving nine studies reported that the tumor detection rate on SSTR-based PET or PET/CT is only 63.5% in recurrent MTC. 5 Hence, there is an imperative need to introduce and evaluate new radiolabeled theranostic molecular imaging probes, which may be used to accurately diagnose, treat, and follow MTC.
In MTCs, RET proto-oncogene mutations are the primary molecular mechanisms underlying tumorigenesis. 2 In addition, it is reported that the interaction between the tumor cell and their TME plays the driving force in tumor progression. 10,11 The activation of the stromal cells in the TME, which is also known as the desmoplastic reaction, is a diagnostic pathological marker for tumor progression. CAFs express α-smooth muscle actin (α-SMA), FAP, and extracellular matrix proteins such as tenascin C (Tn-C).
Koperek et al. found that the three fibroblast activation markers α-SMA, FAP, and Tn-C- are highly expressed in the peritumoral and intratumoral stromal compartments of MTCs, and that the expression of FAP and Tn-C correlates with the level of desmoplasia determined by histological analysis. 12 They also found that the presence of desmoplasia is associated with invasion morphology and a higher incidence of LN metastasis in both papillary thyroid cancers (PTCs) and MTCs. 12 –14 CAFs have been identified as having protumor activity and genetic stability, 14 making this stromal cell type an appealing target for novel therapeutic strategies aimed at inhibiting tumor progression by targeting the TME. This study examined FAPi as a potential theranostic probe in MTC.
In our study, 27 MTC patients were evaluated, and unlike [68Ga]Ga-DOTANOC PET scan (sensitivity: 73.9%), [68Ga]Ga-DOTA.SA.FAPi PET scan detected the majority of the (96%) lesions irrespective of the calcitonin levels. In a study by Ong et al. 15 the results showed better sensitivity of 78% with [ 18 F]F-FDG when calcitonin levels were >1000 pg/mL, but was of limited use if the calcitonin level is <500 pg/mL.
In this study, although the detection rates with [68Ga]Ga-DOTA.SA.FAPi and [68Ga]Ga-DOTANOC PET imaging were comparable, a significantly high uptake, image contrast, and TBR rate were observed with [68Ga]Ga-DOTA.SA.FAPi in the primary and locoregional LN metastases.
Further inspection of 105 liver metastases was detected on CT and [68Ga]Ga-DOTA.SA.FAPi, only 49 (46.4%) were positive on [68Ga]Ga-DOTANOC PET. In an 18-year-old female patient [68Ga]Ga-DOTA.SA.FAPi PET/CT detected multiple liver metastases that were not identified on [68Ga]Ga-DOTANOC PET/CT (Fig. 3). Sahin et al. 16 set diagnostic criteria for identifying 98 liver metastases in 31 patients with gastrointestinal tumors. Among them, 92 lesions were [68Ga]Ga-DOTA-FAPI positive, and on the contrary, only 65 were [ 18 F]F-FDG positive. In agreement with our results, Kuyumcu et al. 17 demonstrated multiple liver metastases on [68Ga]Ga-FAPI-04 PET/CT that were not detected on [68Ga]Ga-DOTATATE PET/CT in a patient with MTC.
Importantly, we observed that [68Ga]Ga-DOTA.SA.FAPi has an exceptionally high detection efficiency and TBR in the liver due to the negligible liver background of SULpeak uptake value as low as 1.3 compared with that of [68 Ga]Ga-DOTANOC (average background SULpeak: 5–6) and [ 18 F]F-FDG (average background SULpeak: 3). This finding reinforces the idea of exploiting [68Ga]Ga-DOTA.SA.FAPi PET/CT for the planning of radiotherapy for liver tumors. Increasing evidence is accumulated on the accuracy of planning radiotherapy with [68Ga]Ga-DOTA.SA.FAPi instead of [ 18 F]F-FDG or [68Ga]Ga-DOTANOC in liver and bone metastases attributing to the increased lesion uptake on FAPI PET/CT with a low background of the liver. 18
[68Ga]Ga-DOTA.SA.FAPi detected more lung and bone metastases and higher activity than [68Ga]Ga-DOTANOC. An 18-year-old female (Fig. 3) showed FAPI uptake in multiple underlying sclerotic bone lesions and liver metastases that were not identified on [68Ga]Ga-DOTANOC PET/CT. The possible reason for such high detection efficiency on [68Ga]Ga-DOTA.SA.FAPi PET/CT may be due to the stromal development and abundant stromal components found even at the early stages of tumorigenesis 19,20 in subcentimetric lesions and suggesting an independent role for FAPI PET/CT in improved lesion detection and aiding accurate staging of MTC.
Our preliminary experience on the theranostic approach of [68Ga]Ga-DOTA.SA.FAPi guided [177Lu]Lu-DOTAGA.(SA.FAPi)2 therapy in a case of aggressive MTC patients highlights a clear survival benefit from FAP inhibitor radionuclide therapy. 21 More recent evidence from our group reveals clinical benefit from [68Ga]Ga/[177Lu]Lu-DOTAGA.(SA.FAPi)2 therapy in patients with radioiodine refractory thyroid cancers. 22 Our data suggest the promising detection efficiency of [68Ga]Ga-DOTA.SA.FAPi is an excellent initial step toward expanding the therapeutic front for MTCs.
Study limitations
Although the present results clearly support imaging with [68Ga]Ga-DOTA.SA.FAPi PET/CT in the restaging of MTC patients, it is appropriate to recognize some potential limitations. The main drawback of diagnostic retrospective studies involves the risk of bias due to deficiencies in the methodology of the study, selection of reference standard or its alternative feasible option, data collection, and execution or interpretation of the test. In this study, the ideal reference standard, histopathology of each lesion was an impractical option, and hence diagnostic quality CT was used as an alternate reference standard. Our study was small and our findings need to be validated in a larger study.
A detailed correlation between the lesion size on CT with the uptake of both radiotracers was not conducted. We did not analyze the association between the molecular signature of the tumor and the tumor uptake of tested radiotracer in this study. Our study results provide a good starting point for discussion and further research. A well-designed prospective diagnostic trial with predefined specific objectives will be quite beneficial in confirming the potential clinical utility of [68Ga]Ga-DOTA.SA.FAPi in the accurate detection of lesions, and contribute to understanding disease mechanisms and the development of novel treatments in patients with MTC.
Conclusion
[68Ga]Ga-DOTA.SA.FAPi and [68Ga]Ga-DOTANOC radiotracers demonstrated similar detection rates in the diagnosis of primary/residual tumors and locoregional LN metastases. [68Ga]Ga-DOTA.SA.FAPi exhibited a superior detection efficiency relative to [68Ga]Ga-DOTANOC PET imaging when used to detect distant metastatic lesions. We firmly believe that the innovation of therapeutic agents should accompany the development of diagnostic agents.
Footnotes
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of All India Institute of Medical Sciences (Ref. No. IECPG: 22/27, April 23, 2020).
Informed Consent
Written informed consent was obtained from all patients to participate in the study.
Authors' Contributions
All authors contributed to the study's conception and design. Material preparation, scan acquisition, data collection, and analysis were performed by S.B., M.P.Y., P.S., S.R., and S.S. The first draft of the article was written by S.B. and M.P.Y. Images were processed and reported by C.B. and M.T. S.A. reviewed the pathology reports. Dr. Ranjit Kumar Sahoo referred patients for scans. F.R., E.S.M., and M.M., our collaborators from the University of Mainz, have synthesized the precursor and finalized the article. All authors commented on previous versions of the article. All authors read and approved the final article.
Disclaimer
This study has not been submitted for review or is not under acceptance for publication in any journal.
Author Disclosure Statement
All the authors included in this article have stated no financial or personal conflict of interest. There is no recent (within the past 5 years), current, or anticipated employment by an organization that may gain or lose financially from the publication of the article.
Funding Information
No funding was received for this article.