
Abstract
Background:
Antithyroid drugs (ATDs) are frequently used to achieve euthyroidism in patients with hyperthyroidism. ATDs cause characteristic common and rare adverse events; however, comprehensive comparisons between methimazole (MMI) and propylthiouracil (PTU) in terms of adverse events are limited.
Methods:
In this study, we thoroughly explored adverse events in association with MMI and PTU use with a disproportionality analysis using the Japanese Adverse Drug Event Report (JADER) database and evaluated the prevalence of MMI and PTU prescriptions using the National Database of Health Insurance Claims and Specific Health Checkups (NDB) Open Data Japan. We analyzed 3271 cases of MMI use and 1029 cases of PTU use with respect to 9789 preferred terms (PTs) for adverse events registered in the JADER database by calculating and comparing reporting odds ratios (RORs).
Results:
We found that 8 PTs, including agranulocytosis (p < 0.0001, 4.01-fold), aplasia cutis congenita (p < 0.0001, 123.22-fold), and exomphalos (p = 0.0002, 22.17-fold), demonstrated significantly higher RORs (more than 4-fold) for MMI use than for PTU use. Nineteen PTs, including anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitis (p < 0.0001, 29.84), rapidly progressive glomerulonephritis (p < 0.0001, 6.44), and pulmonary alveolar hemorrhage (p < 0.0001, 7.77), had RORs for PTU use more than four times those for MMI use. NDB Open Data Japan showed more frequent PTU prescriptions than MMI prescriptions for women of reproductive age.
Conclusions:
This large-scale study confirmed that a variety of congenital malformations were identified as having significantly high RORs for MMI use, while diseases related to ANCA-associated vasculitis were specific to PTU.
Introduction
Antithyroid drugs (ATD
Because most ATD-induced agranulocytosis is observed within a few months after the first administration of an ATD, 6 monitoring the neutrophil count once every 2 weeks until 2 months after the first administration is recommended for patients using ATDs in the Japanese guidelines for Graves' disease treatment.
Agranulocytosis is a well-known and severe adverse event caused by ATDs. However, the incidence rates of ATD-induced agranulocytosis vary by study because the occurrence of agranulocytosis is uncommon. The estimated frequencies of ATD-related side effects other than agranulocytosis are 1–5% for arthralgia, 1–5% for gastrointestinal effects, 1–2% for polyarthritis, and 2–6% for fever and skin reactions. 1,7 Less frequent ATD-related side effects include an abnormal sense of taste or smell, ANCA-associated vasculitis, cholestasis, hepatitis, cholestatic jaundice, Stevens–Johnson syndrome, hypoprothrombinemia, insulin-autoimmune syndrome, sialadenitis, thrombocytopenia, aplastic anemia, and pancreatitis. 1,4 These less frequent side effects have been further categorized as “rare side effects” and “very rare side effects” in previous reports; however, the definitions differ by study. 1,4,8,9
The difference in the frequency of side effects between MMI and PTU remains highly controversial. The teratogenic effects of MMI compared with PTU have been widely indicated and the possible involvement of the teratogenicity of PTU in the adverse effects on the head and neck region and urinary tract has been suggested. 10 –21 However, the details of the effects of MMI and PTU on each type of malformation are not yet fully understood. Furthermore, comprehensive analyses and comparative studies of a wide range of adverse events caused by ATDs have been limited.
The Japanese Adverse Drug Event Report (JADER) database contains all pharmacovigilance data that have been spontaneously reported to the Pharmaceuticals and Medical Devices Agency (PMDA) by pharmaceutical industries and medical care providers since April 2004. More than 94% of the reports in the JADER database are from medical professionals, indicating high reliability in pharmacovigilance studies. 22 As of October 2021, the database contained 705,294 case reports of patients with adverse drug reactions. A total of 3271 patients with MMI use and 1029 patients with PTU use were registered, and among them, >100 experienced fetal adverse events. To the best of our knowledge, these data constitute the largest scale database. In this study, we studied the association of MMI or PTU use with every registered adverse event using the JADER database.
Materials and Methods
Study design and participants
This study did not require institutional review board approval because the JADER database is an anonymized database open to the public. This study attempted to examine the correlation between every type of adverse event and the ATDs available in Japan based on information contained in the JADER database. The JADER database contains data on reports in a format based on the E2B (M2) guideline of the International Conference on Harmonization of Technical Requirements for Registration of Pharmaceuticals for Human Use. For this study, data recorded in the JADER database from April 2004 to September 2021 were downloaded from the PMDA website. We extracted data from the following files: patient demographic information (DEMO) files, drug information (DRUG) files, adverse events and patient outcomes (REAC) files, and disorder history (HIST) files. Each file type was linked to a specific identification number.
Statistical analysis
We assessed the association between MMI and PTU use and every type of adverse event reported in the database. In the JADER database, the disease names are listed according to the preferred terms (PTs) provided by the Medical Dictionary for Regulatory Activities/Japanese version (MedDRA/J). We also analyzed the prescription data in the 6th version of the National Database of Health Insurance Claims and Specific Health Checkups (NDB) Open Data Japan. These data contain prescription information from all Japanese medical practitioners' receipts for health insurance claims in fiscal year 2019. Cases that lacked essential data were removed from the analysis. The associations of each drug with every PT contained in the JADER database were assessed by calculating the reporting odds ratio (ROR), which is an established parameter in pharmacovigilance research. RORs were calculated using a two-by-two contingency table.
The RORs are expressed as point estimates with 95% confidence intervals [CIs]. Haldane–Anscombe 1/2 correction was applied to calculate RORs when the ROR could not be obtained because one or more 0s were present in the 2 × 2 contingency table used to calculate RORs. Correlations were considered significant when the lower bound of the two-sided CI of the ROR for the risk of the PT exceeded 1. Next, we compared the RORs between the MMI and PTU groups for the PTs with 3 or more patients in each group and assessed the difference with a z test.
If the z test for the RORs between the MMI and PTU groups showed p < 0.05, statistical significance was considered. We previously reported that deleting cases of concomitant use from the database could lessen the impact of the confounding influences of concomitant drugs; thus, in the secondary analysis, we deleted cases with concomitant MMI and PTU use and repeated the process. 23 The data were analyzed using R software (version 4.1.1; The R Foundation for Statistical Computing, Vienna, Austria).
Results
In the JADER database, 705,294 patients were registered. None of patients lacked identification numbers or generic names of the drugs used; thus, we could analyze all of them to calculate RORs. The participant flow is shown as a diagram (Fig. 1). A total of 3271 patients received MMI therapy, and 1029 patients received PTU therapy. In addition, the demographic characteristics of the whole population and each treatment group are given in Table 1. A total of 9789 PTs for adverse events were registered in the database. MMI had significant RORs for 186 PTs, and PTU had significant RORs for 143 PTs. PTs that demonstrated significant RORs and ROR point estimates higher than 5 for ATDs are given in Tables 2 and 3. Among these PTs, 96 were associated with 3 or more cases of either MMI or PTU use.

Study population flow diagram. ATDs, antithyroid drugs; MMI, methimazole; ROR, reporting odds ratio; PTU, propylthiouracil.
Population Characteristics
Patients without age information were excluded.
MMI, methimazole; PTU, propylthiouracil.
Preferred Terms That Had Point Estimates of Reporting Odds Ratios Higher Than 5 for Methimazole Use
Haldane–Anscombe 1/2 correction applied.
PT, preferred term; ROR, reporting odds ratio.
Preferred Terms That Had Point Estimates of Reporting Odds Ratios Higher Than 5 for Propylthiouracil Use
IgA, immunoglobulin A.
We conducted a z test for the difference between log (ROR) for MMI and PTU use based on the 96 PTs. We found that among the 96 PTs, 8 had significantly high RORs for MMI (fold change >4, p < 0.05). The PT for adverse reactions with significant p-values (fold-change of RORs vs. PTU) was agranulocytosis (p < 0.0001 [4.01]), and the PTs for teratogenic effects with significant p-values were aplasia cutis congenita (p < 0.0001 [123.22]); exomphalos (p = 0.0002 [22.17]); vitello-intestinal duct remnant (p = 0.003 [22.73]); intestinal fistula (p = 0.014 [4.93]); and congenital intestinal malformation (p = 0.014 [54.68]). We also found that 26 PTs associated with PTU use had significantly high RORs (fold change >4, p < 0.05).
The PTs for adverse reactions with significant p-values (fold-change of RORs vs. MMI) were ANCA-positive vasculitis (p < 0.0001 [29.84]); rapidly progressive glomerulonephritis (RPGN) (p < 0.0001 [6.44]); pulmonary alveolar hemorrhage (p < 0.0001 [7.77]); ANCA positive (p < 0.0001 [10.87]); and goiter (p < 0.0001 [5.61]); and the PT for teratogenic effects with a significant p-value was congenital hypothyroidism (p = 0.0004 [6.26]) (Fig. 2). Supplementary Table S1 provides changes in the number of cases for PTs related to congenital malformations or pregnancy every 4 years and cases of congenital malformations in association with MMI use have decreased since 2016. Data on ATD dosage were lacking for 28.5% of the patients with MMI use and 38.6% of the patients with PTU use. Thus, we analyzed the remaining dose-available data and found that the mean doses of MMI and PTU were 13.25 and 142.65 mg/day, respectively, in the JADER database (Supplementary Fig. S1).
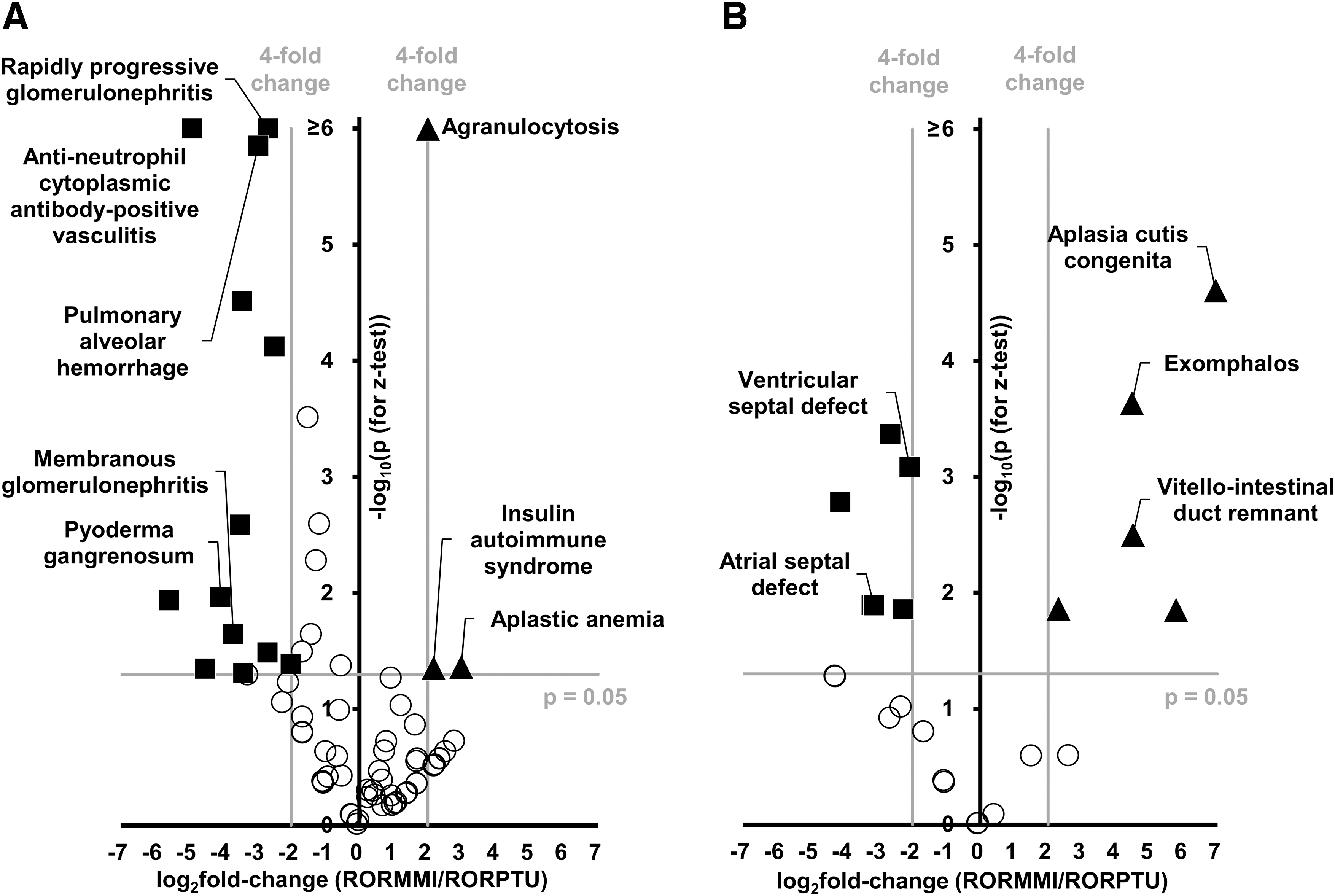
Volcano plot of the z test for reporting odds ratios between the methimazole and propylthiouracil groups in the Japanese Adverse Drug Event Report database. (
Next, we omitted cases of concomitant MMI and PTU use and reanalyzed them to exclude the overlap between the two drugs. MMI had significant RORs for 176 PTs, and PTU had significant RORs for 114 PTs in this analysis. PTs that indicated ROR point estimates higher than 5 for ATDs are given in Tables 4 and 5. Among these PTs, 78 were associated with 3 or more cases of either MMI or PTU use. The z test revealed that among the 78 PTs, 1 had a significantly high ROR for MMI use and had at least a 4-fold change in the ROR for MMI use compared with that for PTU use (rhabdomyolysis, p = 0.017 [fold-change of RORs vs. PTU 5.66]).
Preferred Terms That Had Point Estimates of Reporting Odds Ratios Higher Than 5 for Methimazole Use
Cases of concurrent propylthiouracil use were omitted.
Preferred Terms That Had Point Estimates of Reporting Odds Ratios Higher Than 5 for Propylthiouracil Use
Cases of concurrent methimazole use were omitted.
Furthermore, 12 PTs for adverse reactions and 8 PTs for PTU teratogenic effects had significantly high RORs compared with MMI and had at least a 4-fold change in the ROR (ANCA-positive vasculitis, p < 0.0001 [fold-change of RORs vs. MMI 24.89]; RPGN, p < 0.0001 [9.07]; pulmonary alveolar hemorrhage, p < 0.0001 [9.32]; goiter, p = 0.00017 [7.79]; ANCA positive, p = 0.001 [10.14]; and ventricular septal defect, p = 0.0005 [5.19]) (Fig. 3). The abovementioned results were summarized with PTs categorized into standardized MedDRA queries (Supplementary Table S2). When we analyzed the data separately by sex, there were no overall significant sex differences (Supplementary Tables S3–S6). A recent report suggested an association between MMI use and acute pancreatitis. 24

Volcano plot of the z test for reporting odds ratios between the methimazole and propylthiouracil groups in the Japanese Adverse Drug Event Report database after the exclusion of cases with concurrent use of the other antithyroid drug. (
Analysis of 14 pancreatitis-related PTs in the JADER database revealed that none of the PTs showed significant RORs, but 11 cases of pancreatitis were found only in patients with MMI use and not in those with PTU use. We next compared our results with those of two previous large-scale observational studies in the context of teratogenic effects (Supplementary Table S7). A Scandinavian study reported 16–18 cases of malformations of the digestive system and a Korean study reported 27 cases of MMI embryopathy. 12,14 On the contrary, in this study, 47 and 107 cases were reported, respectively.
An analysis of the 6th version of the NDB Open Data Japan revealed that 20.2% of all ATD tablets prescribed in Japan in 2019 were PTU tablets and 79.8% were MMI tablets, in 2014, 22.2% were PTU tablets and 77.8% were MMI tablets. Because MMI and PTU doses are often 2 to 3 tablets, the number of tablets could be proportional to the number of patients. Moreover, 59.4% of PTU prescriptions and 37.5% of MMI prescriptions were issued to women aged 20–49 years in 2019, and a similar trend was observed in 2014 (Fig. 4A, B). Thus, PTU was used more frequently than MMI in women of reproductive age. This trend in ATD prescription for women of reproductive age may contribute to the observed higher RORs for congenital malformations in association with PTU use compared with MMI use.
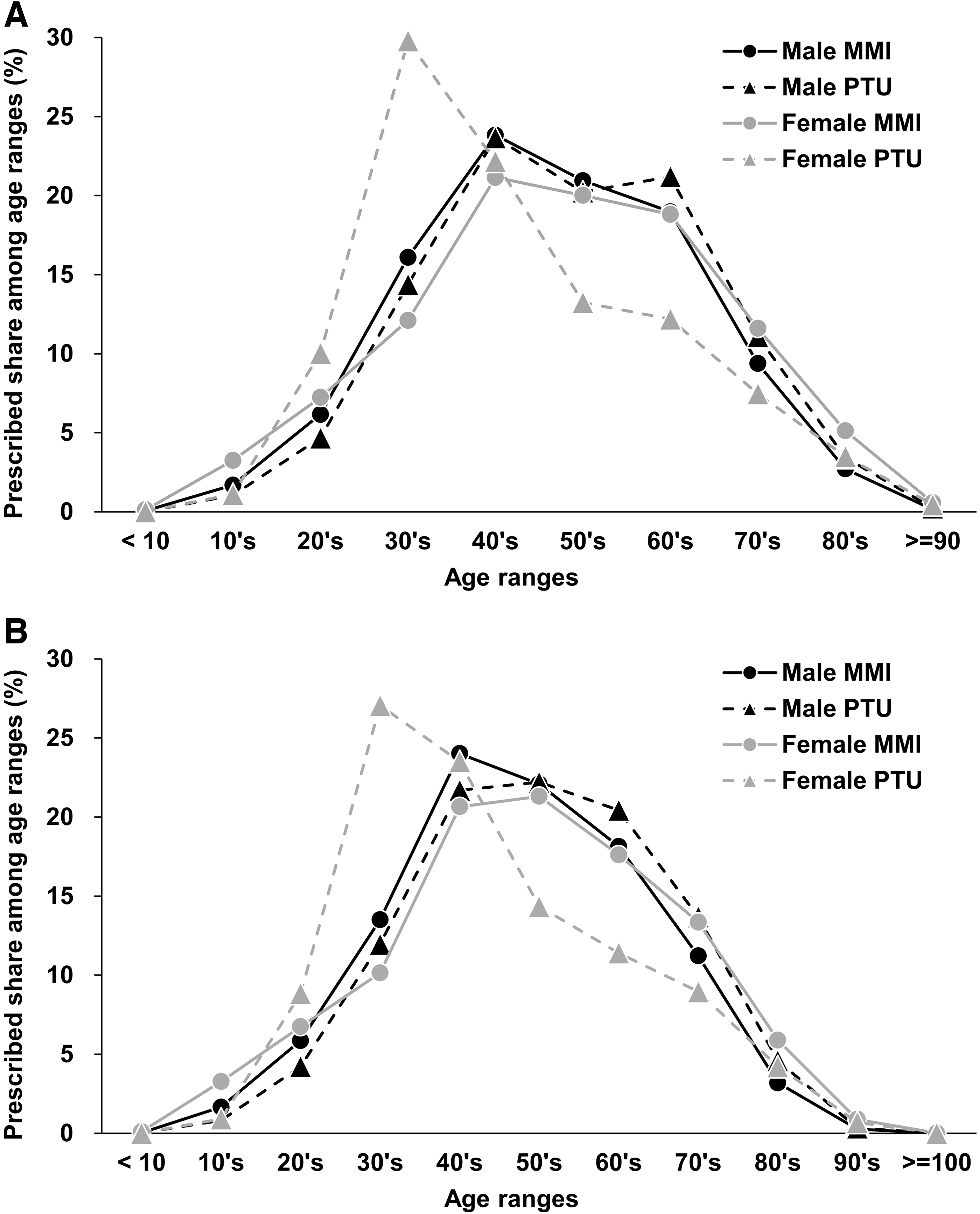
Age-specific ratio of methimazole and propylthiouracil prescriptions in Japan. The data were obtained from the (
Discussion
The JADER database contained a large number of rare adverse events associated with ATDs, including 1078 cases of agranulocytosis, 322 cases of ANCA-associated vasculitis, 58 cases of rhabdomyolysis, and >170 cases of congenital malformations. To the best of our knowledge, this study analyzed adverse events of ATDs by using the highest number of cases thus far. In this study, we explored adverse events associated with MMI and PTU use with a disproportionality analysis using the JADER database. We also compared the differences in RORs between MMI and PTU use.
We also excluded cases of patients using both MMI and PTU because these cases can mitigate biases that often appear in this type of analysis. 23 The higher ROR values for MMI and PTU use were largely unaltered before and after the exclusion. Although the significantly higher RORs for PTU use compared with MMI use identified by the z test were similar even after the exclusion of cases of concurrent PTU and MMI use, the associations with most PTs, which were higher for MMI use and included congenital malformations, became insignificant. Because patients who are pregnant or may become pregnant are often switched from MMI to PTU to avoid gestational side effects, both PTU and MMI could be registered as used drugs. Thus, cases of congenital malformations were greatly affected by this exclusion, probably owing to the switching of ATDs.
A systematic review and large-scale observational studies have consistently shown a significant risk for perinatal side effects in pregnant women with MMI use, whereas mixed findings have been reported for this risk with PTU use. 12,14,25 Another study concluded that situs inversus ± dextrocardia and cardiac outflow tract defects were associated with exposure to PTU, whereas choanal atresia, omphalocele, and total situs inversus were associated with exposure to MMI. 20 In addition to choanal atresia and exomphalos (omphalocele), the use of MMI showed significantly higher RORs for vitello-intestinal duct remnant, intestinal fistula, and esophageal atresia in this study. MMI may affect the development of the gastrointestinal tract, which results in a wide range of malformations. Of note, the RORs for ventricular septal defects and atrial septal defects had significantly higher values for PTU use, consistent with the abovementioned finding. 20
The cardiac outflow tract, ventricular septum, and atrial septum are derived from the endocardial cushion, and PTU might modulate the formation of the endocardial cushion during their developmental periods. The interim report of the Pregnancy Outcomes of Exposure to Methimazole Study (POEM Study) in Japan demonstrated that 5 of 85 neonates in the MMI group had congenital malformations, but none of the 121 neonates in the PTU group had malformations. 26 In the POEM study, “methimazole-related congenital malformations” included choanal atresia, esophageal atresia, aplasia cutis congenita, umbilical duct defects, and exomphalos. In this study, the PTs with significantly higher congenital malformation-related RORs for MMI use included congenital gastrointestinal malformation, choanal atresia, and aplasia cutis congenita. Therefore, this study and POEM study demonstrated common congenital malformations.
The decline in reports of teratogenicity in association with MMI use since 2016 in the JADER database may have been noted by the relevant interim report of the POEM study in 2011. However, as described previously, the ROR for congenital malformations associated with MMI use did not reach statistical significance compared with that for PTU use when patients with concurrent MMI and PTU use were excluded. Further investigations are needed to analyze switching from MMI to PTU during gestational periods to clarify the effects of MMI on congenital malformations in the excluded patients.
Agranulocytosis is a life-threatening complication of ATDs for which the granulocyte count must be assessed routinely. However, whether the risk of agranulocytosis differs between PTU and MMI use remains controversial. The reported incidence of ATD-mediated agranulocytosis is 0.2–0.5%. 27 A Danish study showed a higher incidence of agranulocytosis for patients with PTU use (0.27% for PTU use vs. 0.11% for MMI use; p = 0.02), while Japanese and Korean studies indicated approximately twice as many agranulocytosis cases in patients with MMI use compared with those with PTU use. 5,28 Conversely, a meta-analysis demonstrated that the agranulocytosis incidence did not significantly differ between the MMI and PTU groups. 29
In this study, the ROR of agranulocytosis for MMI use was approximately four times higher than that for PTU use, and this difference remained significant (at 3.69-fold) even after the elimination of patients with concurrent MMI and PTU use. Because MMI-induced agranulocytosis, unlike PTU-induced agranulocytosis, is dose dependent, the relative risk ratio between MMI and PTU use should be interpreted with caution. The risk of agranulocytosis for MMI and PTU use may depend on a patient's ethnic background. Large-scale studies in other regions are warranted to further determine the safety of ATDs in each country.
Insulin autoimmune syndrome (IAS) produces autoantibodies to human insulin, which results in spontaneous hypoglycemia. MMI is thought to be a major cause of IAS, followed by tiopronin and alpha lipoic acid. 30 However, PTU-induced IAS has not yet been reported. In this study, the z test showed a significantly higher ROR for IAS associated with MMI use. Although the difference became insignificant after the exclusion of patients with concurrent PTU and MMI use, 22 cases of IAS were associated with MMI use and no cases were associated with PTU use. This finding supports the idea that IAS is a specific complication of MMI use but not of PTU use. As described in a recent systematic review, 31 IAS is predominantly observed in Asian countries probably owing to specific HLAs (e.g., HLA-DRB1*0406). Comparisons with the incidence of IAS in other countries may also be of interest.
ANCA-associated vasculitis, also known as ANCA-positive vasculitis, is a disorder characterized by severe, systemic, small-vessel vasculitis. Japanese ANCA-associated vasculitis cases are frequently reported, but the racial/ethnic differences in the prevalence of ANCA-associated vasculitis are unclear. 32 The proportion of ANCA-positive cases was estimated at 4–64% in patients with PTU use and 0–16% in patients with MMI use. 33 A postmarketing adverse event report demonstrated that the ratio of the estimated incidence of ANCA-associated vasculitis was 39.2-fold higher for PTU use than for MMI use. 34 We found that the ROR of ANCA-associated vasculitis was 29.84-fold higher for PTU use than for MMI use in this study. ANCA-associated vasculitis is related to clinical manifestations, including alveolar hemorrhage, RPGN, membranous nephritis, and pyoderma gangrenosum. 35 –41
A previous study analyzing 16 patients with PTU-induced ANCA-associated vasculitis indicated that more than half of the patients presented with multiple organ complications, particularly kidney-related symptoms. 42 In this study, we identified 270 cases of ANCA-associated vasculitis with PTU use, and the difference in the RORs between PTU and MMI use for the symptoms related to ANCA-associated vasculitis was less pronounced after the exclusion of patients with concurrent PTU and MMI use, for example, alveolar hemorrhage (ROR: 1.66 for MMI use vs. 15.52 for PTU use; 9.32-fold change; p < 0.0001) and RPGN (ROR: 16.82 for MMI use vs. 152.54 for PTU use; 9.07-fold change; p < 0.0001). Because multiple PTs for one disease could be registered in the JADER database, careful interpretation is required regarding the relevant PT group. ANCA-associated vasculitis without severe symptoms might be predominantly registered as “ANCA-positive vasculitis” in the JADER database.
The incidence of rhabdomyolysis induced by ATDs was reported to be relatively low in previous studies. Four reports demonstrated eight cases of rhabdomyolysis associated with MMI use, but not with PTU use, in patients with Graves' disease. 43 –46 In this study, we identified 43 and 2 cases of rhabdomyolysis in response to MMI and PTU use, respectively, after excluding patient with concurrent MMI and PTU use (ROR: 1.49 for MMI use vs. 0.26 for PTU use; 5.66-fold change; p = 0.016). Periodic confirmation of serum CPK levels may be important for patients using MMI.
An analysis of NDB Open Data Japan, a comprehensive prescription database, showed that prescriptions for 5-mg MMI tablets were 3.86 times more common than prescriptions for 50-mg PTU tablets in terms of the total number of tablets. A Japanese randomized controlled study demonstrated that 30 mg/day MMI, 15 mg/day MMI, and 300 mg/day PTU were equally effective for the initial treatment of mild to moderate hyperthyroidism caused by Graves' disease. 47 The analysis suggested that PTU was more likely to be prescribed to women of reproductive age. This trend in PTU prescription could cause a bias to increase the ROR of PTU use for PTs related to congenital malformations or pregnancy. It is difficult to compare the total number of adverse events between the MMI and PTU groups because >9000 PTs cannot be analyzed separately for teratogenic effects and nonteratogenic effects.
This study is subject to several limitations. The reports in the JADER database often lacked data on preexisting comorbidities and historical dose data. For example, 83.2% of patients with MMI use and 85.8% of patients with PTU use only had data for a single drug. Therefore, we could not estimate the effects on the results. Evaluation of teratogenic effects in pregnant women was difficult because all PTs were reported as fetal rather than maternal in the database. We applied the z test to compare RORs between PTU and MMI use for each PT, but the comparison method between RORs has not been fully established. Although there are some PT drug combinations with possible inverse causality, they should also be analyzed to avoid biases because of arbitrary omission.
Although all cases should be registered in the database to calculate a representative relative risk, RORs cannot be described as a representative normal risk ratio or an odds ratio when a biased population is registered. Because the JADER database is a spontaneous reporting system, several unavoidable limitations are associated with this type of database analysis. These limitations include missing data, underreporting, overreporting, data registry errors, and a lack of control data. In this study, we did not gather data on coexisting illnesses, drug doses, or durations of exposure. Further analytical observational studies and monitoring must be performed.
Conclusion
We comprehensively evaluated and compared the adverse events associated with the use of MMI and PTU using the JADER database. Eight PTs, including agranulocytosis, had significantly higher RORs for MMI use, and 19 PTs, including ANCA-associated vasculitis, had significantly higher RORs for PTU use. Because the JADER database is a spontaneous reporting system, several limitations must be considered.
Footnotes
Acknowledgments
The authors acknowledge all contributors to the JADER database. The authors also thank Misa Katayama (Yokohama City University) for her excellent secretarial assistance.
Authors' Contributions
J.S. conceived the concept of this study. M.A. and J.S. wrote the article. M.A. was responsible for data collection and performed the statistical analysis. H.K., T.T., and Y.T. made substantial contributions to the interpretation of data and revised the article for important intellectual content. All authors approved the submission of the article. J.S. is the guarantor of this work and, as such, has full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Author Disclosure Statement
None of the authors have any conflicts of interest to disclose.
Funding Information
J.S. acknowledges support from a Grant-in-Aid for Scientific Research (C) 20K08866 from MEXT of Japan and the Japan IDDM network, Japan Diabetes Foundation, Uehara Memorial Foundation, Mochida Memorial Foundation for Medical and Pharmaceutical Research, Kamome Memorial Foundation of Yokohama City University, Naito Foundation, Astellas Foundation for Research on Metabolic Disorders, Manpei Suzuki Diabetes Foundation, and A*STAR-AMED JOINT CALL for the Strategic International Collaborative Research Program (SICORP).
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7