
Abstract
Background:
An increasing amount of data is being published, which risk-stratify thyroid tumors according to genetic signatures and histological morphology. Typically, follicular patterned lesions have been shown to harbor RAS-like mutations with more indolent behaviors. Our study aims to examine the extent of similarity among three groups of follicular patterned lesions with papillary nuclear features—noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP), encapsulated follicular variant of papillary thyroid carcinoma (EFVPTC) with capsular invasion and/or angioinvasion, and infiltrative follicular variant of papillary thyroid carcinoma (iFVPTC)—to help clarify whether NIFTP and EFVPTC represent a histological continuum and the degree to which the genomic landscape further separates higher risk follicular patterned tumors such as iFVPTC from more indolent ones (EFVPTC and NIFTP).
Methods:
ThyroSeq test results were compared for cases with histological NIFTP, EFVPTC, and iFVPTC in this retrospective study. Genetic drivers were subcategorized by level of aggressiveness. Gene expression alterations (GEAs) and copy number alterations (CNAs) were compared among the three histological groups.
Results:
NIFTP and EFVPTC cases displayed predominantly RAS-like alterations (100% and 75%, respectively) and RAS-like GEAs (55.2% and 47.2%, respectively), and many showed CNAs with 22q-loss. Despite a predominance of RAS-like alterations, EFVPTC cases showed molecular heterogeneity with significantly more intermediate and aggressive drivers (22.3% of cases) than NIFTP (0%) (p = 0.0068). iFVPTC cases displayed molecular profiles in between that of traditional follicular patterned lesions and classical papillary thyroid carcinoma, predominantly displaying intermediate and aggressive drivers (61.6%), which was significantly higher than that of EFVPTC (22.3%, p = 0.0158) and NIFTP (0%, p < 0.0001), illustrating the higher MAP kinase activity of iFVPTC. There was no significant difference, however, in comparing GEAs among the three histological groups.
Conclusions:
While follicular patterned lesions with papillary nuclear features overall tend to display RAS-like alterations, EFVPTC cases, followed by iFVPTC in this series, showed increasing proportions of more aggressive drivers. EFVPTC and NIFTP show much molecular overlap, with predominance of RAS-like alterations, suggesting that these tumors are part of a genetic continuum, while still ranked differentially. Preoperative molecular testing can potentially distinguish EFVPTC and iFVTPC from NIFTP based on a particular molecular signature, optimizing patient management.
Introduction
Molecular mechanisms of thyroid cancer have progressively been uncovered since the early 1990s. 1 An increased incidence of thyroid cancer has also been noted largely due to an increase in follicular variant subtypes of papillary thyroid carcinoma (PTC). Molecular methods have also revealed that the molecular profile of follicular variants of papillary thyroid cancer (FVPTC) displays genetic alterations distinct from classic PTC. 2 The Thyroid Cancer Genome Atlas 3 characterizes gene mutations and fusions into BRAF p.V600E-like and RAS-like groups, which portend differing levels of tumor aggression, and has been shown to be associated with papillary (classic and tall cell) versus follicular patterned tumors, respectively.
FVPTC is currently classified into the encapsulated type with capsular or vascular invasion (encapsulated follicular variant of papillary thyroid carcinoma [EFVPTC]), and the infiltrative or unencapsulated type (infiltrative follicular variant of papillary thyroid carcinoma [iFVPTC]). EFVPTCs have been shown to behave more similarly to follicular adenomas and/or carcinomas, typically harboring RAS mutations and lacking BRAF p.V600E mutations, whereas iFVPTCs typically behave like classic PTCs and display a higher rate of BRAF p.V600E mutations. 4,5 Additionally, noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP), formerly classified as a noninvasive subtype of EFVPTC, have been shown to harbor RAS-like mutations and behave indolently. 6
We therefore chose to examine EFVPTC and iFVPTC in comparison with NIFTP using an extended next-generation sequencing (NGS) panel to determine whether and to what extent molecular overlap exists among these three categories. This analysis would also help clarify whether NIFTP and EFVPTC represent a histological continuum sharing a common tumorigenesis pathway, and the degree to which the genomic landscape further separates higher risk tumors such as iFVPTC from the more clinically indolent NIFTP and EFVPTC. Such an observation could have important implications for the use of molecular diagnostic testing for informing surgical management decisions since none of these tumors can be otherwise distinguished with cytology and imaging preoperatively.
Materials and Methods
The retrospective study protocol was approved by the institutional review board as exempt; waiver of authorization to use identifiable health information for research was approved in accordance with 45 CFR.164.512 (i) (study number i19-00812). NIFTP, EFVPTC, and iFVPTC thyroid resection cases between January 1, 2015, and January 30, 2020, with a preceding ThyroSeq molecular test (performed on fine needle aspiration [FNA] cytology samples) were identified. The slides of all tumors were reviewed to confirm the histological diagnoses. Figures 1 –4 illustrate examples of each entity.
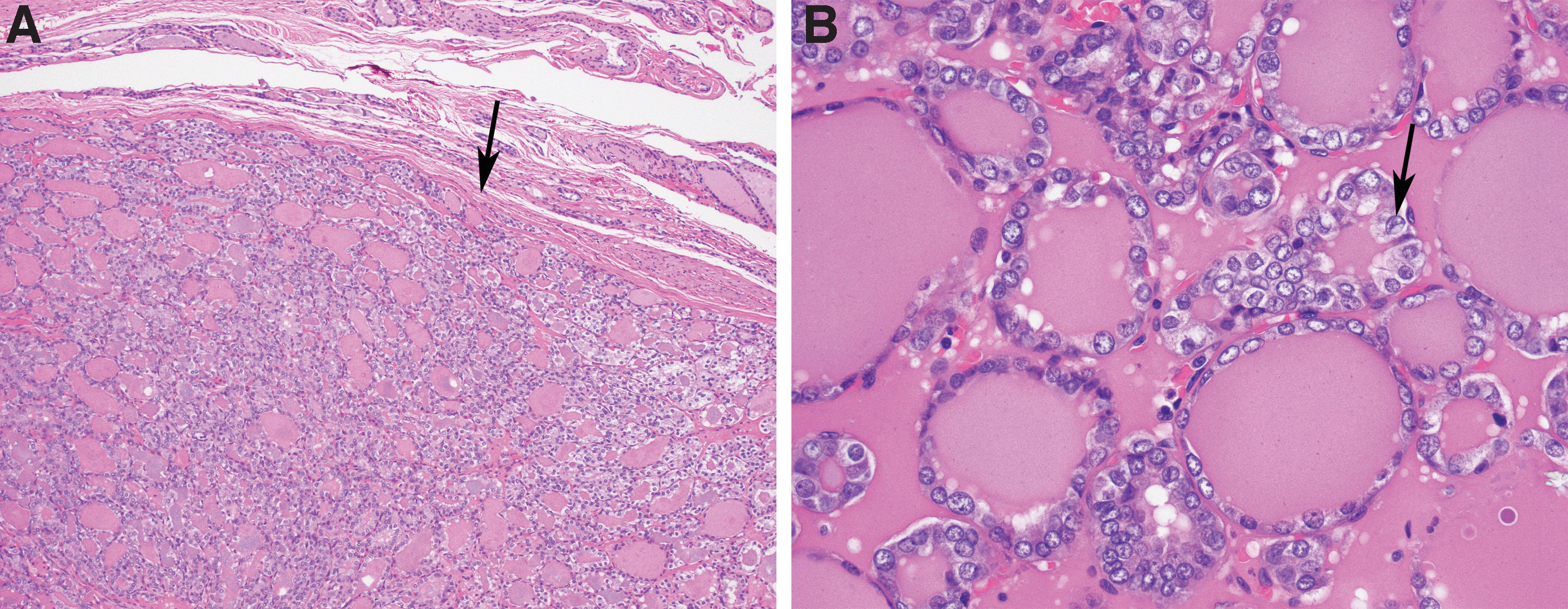
An example of NIFTP at 100 × magnification, which demonstrates a well-circumscribed follicular tumor with thin encapsulation (
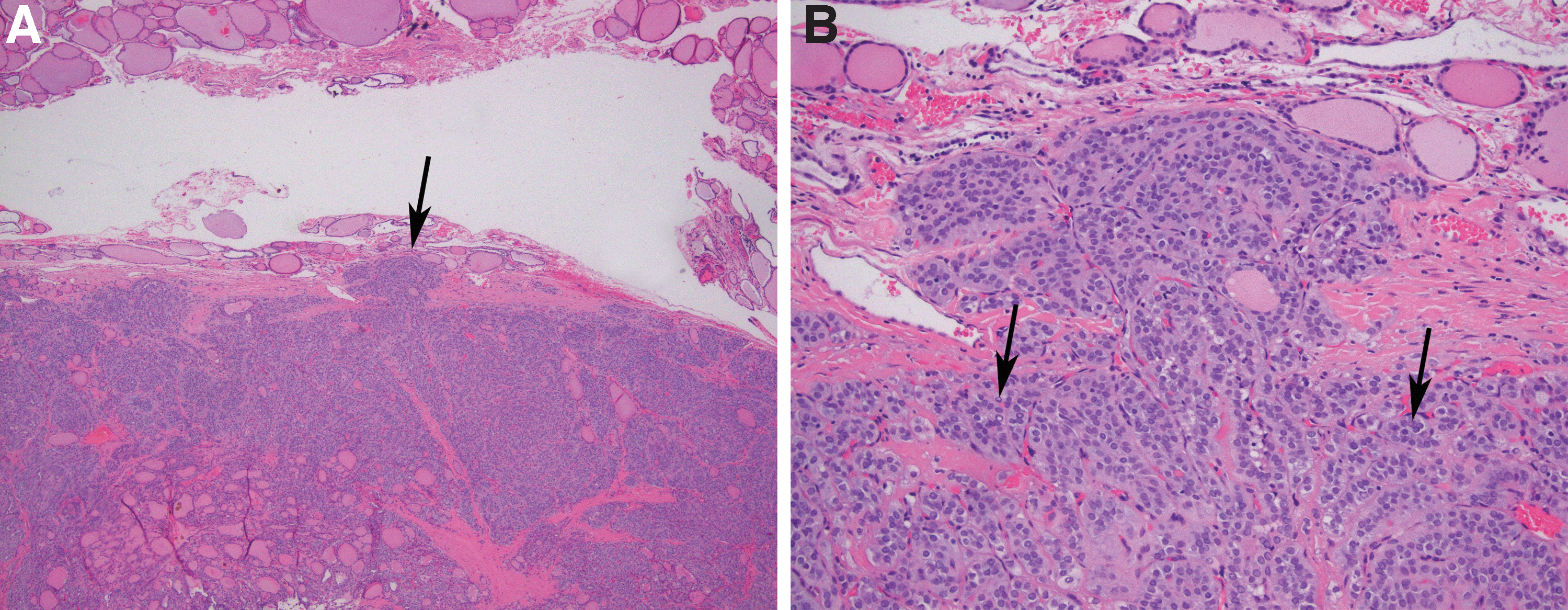
An example of EFVPTC at 40 × magnification, with capsular invasion (
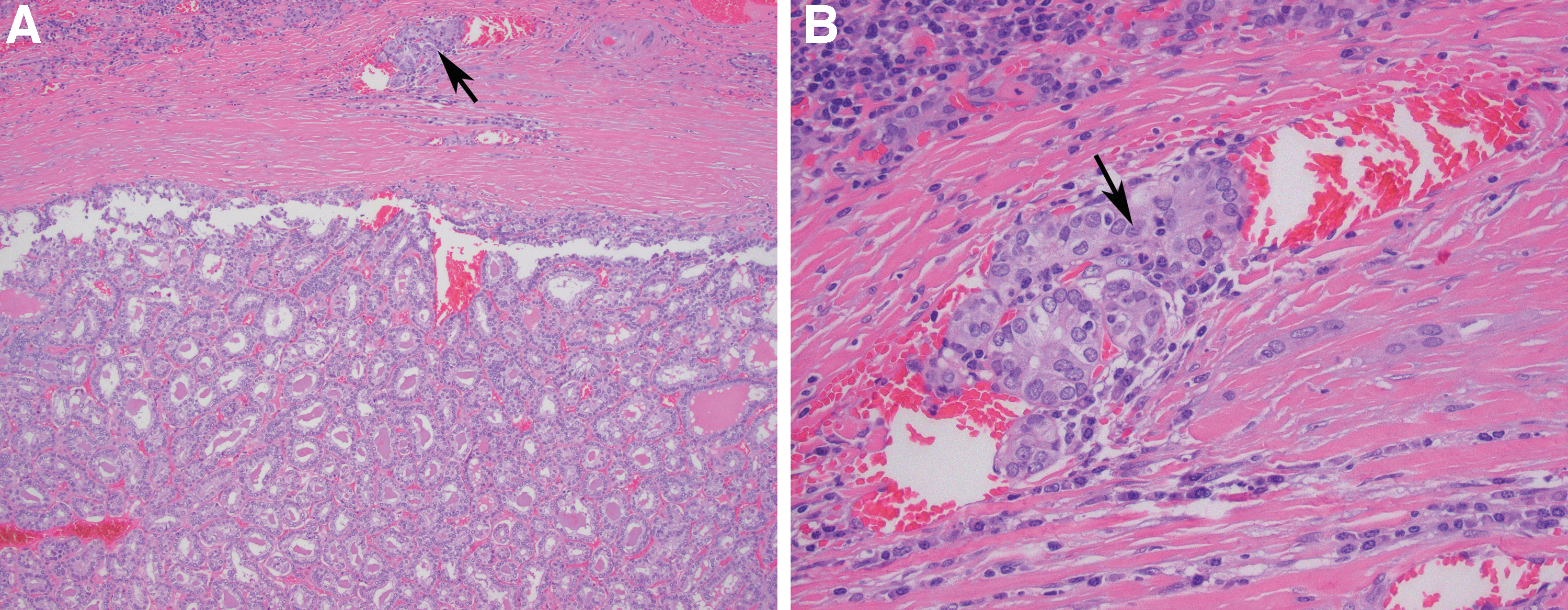
An example of EFVPTC at 100 × magnification, with angioinvasion (
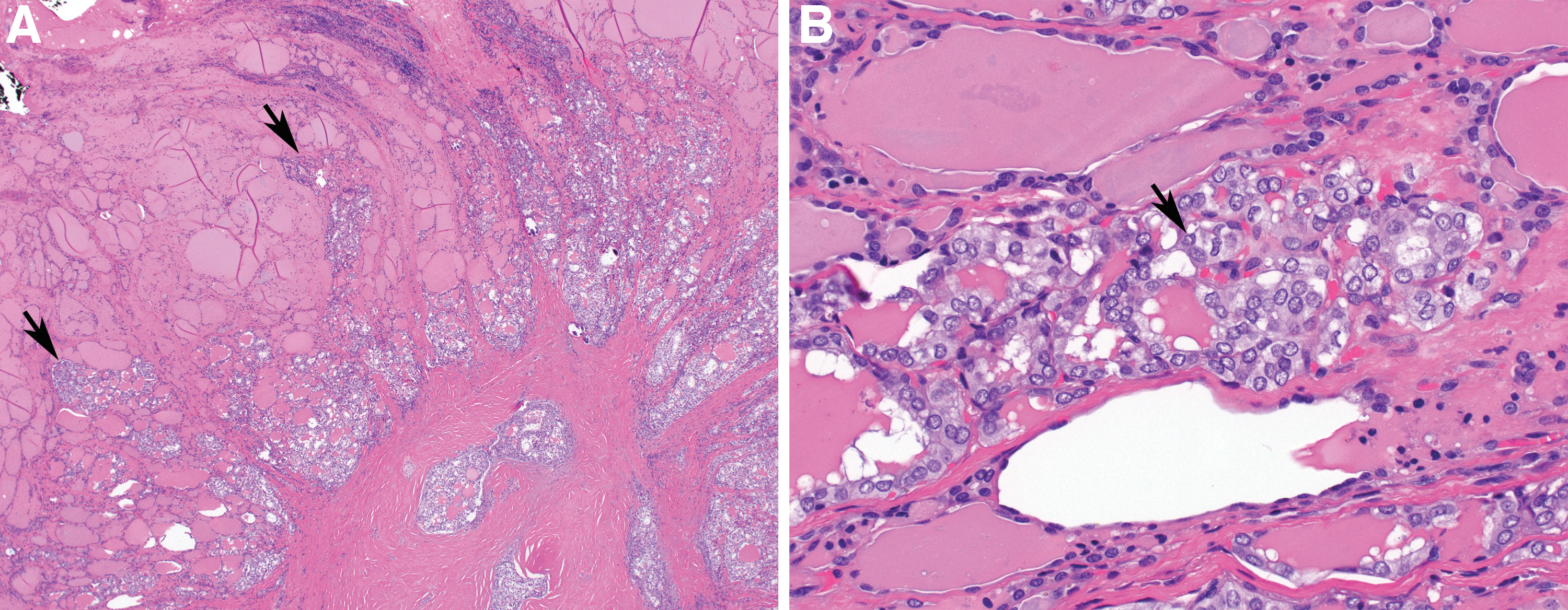
An example of iFVPTC at 40 × magnification, in which an unencapsulated follicular patterned tumor irregularly infiltrates benign thyroid parenchyma (
Five cases initially retrieved were excluded due to the presence of papillae (n = 2), high mitotic rate (n = 1), capsule not fully submitted for evaluation (n = 1), and insufficient for ThyroSeq evaluation (n = 1). Cases were only considered to be NIFTP if they met strict diagnostic criteria. 7 ThyroSeq molecular testing was available on all NIFTP specimens from the preoperative FNA, and all NIFTP specimens in the cohort were BRAF p.V600E negative, consistent with NIFTP diagnostic criteria. Data collected included extent of surgery (lobectomy/hemithyroidectomy vs. total thyroidectomy), patient demographics, FNA cytology results, molecular test results, invasion status (angioinvasion and/or capsular invasion), and presence/absence of lymph node (LN) metastases where applicable. Angioinvasion was considered focal when there were 1–3 foci of invasion and extensive when there were 4 or more foci.
ThyroSeq molecular testing was performed on a total of 70 FNA cytology samples with a needle rinse sample in molecular preservative 8 in cases of indeterminate cytology diagnosis (atypia or follicular lesion of undetermined significance atypia or follicular lesion of undetermined significance [AUS/FLUS], Bethesda III; follicular neoplasm/suspicious for a follicular neoplasm [FN/SFN], Bethesda IV; suspicious for malignancy, Bethesda V). To increase the EFVPTC sample size, eight additional EFVPTC within the study time frame, which lacked FNA cytology ThyroSeq testing and displayed presurgical cytology diagnoses ranging from Bethesda III to VI (positive for malignancy), were retrieved and tested using the formalin-fixed paraffin-embedded tissue blocks to produce a total of 36 EFVPTC cases.
There were 29 NIFTP cases (25 cases were Bethesda III, 4 cases were Bethesda IV), 36 EFVPTC cases (21 cases were Bethesda III, 10 cases were Bethesda IV, 3 were Bethesda V, 2 were Bethesda VI), and 13 iFVPTC cases (11 cases were Bethesda III, 1 case was Bethesda IV, 1 case was Bethesda V). All NIFTP and EFVPTC cytology cases were tested using ThyroSeq v3. iFVPTC cases were tested using ThyroSeq v2 (n = 7) or ThyroSeq v3 (n = 6) depending on which test was in use at the time of FNA sampling.
ThyroSeq v3 is an NGS assay that analyzes 112 genes for a variety of genetic alterations through targeted amplification-based NGS to detect more than 12,000 single nucleotide variations and insertions/deletions, more than 150 gene fusions, abnormal gene expression alteration (GEA), and copy number alterations (CNA) in selected genomic regions. An estimated probability of cancer or NIFTP is calculated and provided in ThyroSeq reports. 8,9
GEAs cover a selected group of genes that are upregulated or downregulated in thyroid cancers and represent a part of the BRAF-RAS score established by TCGA. 3 As such, they can be classified as BRAF p.V600E-like, RAS-like, or non-BRAF p.V600E non-RAS like patterns (the latter will henceforth be referred to as “non-BRAF/non-RAS”). GEA is a reflection, or downstream surrogate marker, of thyroid cancer and not an independent driver event as previously described. 3
Genetic drivers were subcategorized by level of aggressiveness and compared among the three histological groups. TERT promoter mutations followed by BRAF p.V600E-like alterations were designated as the “most aggressive” drivers in this study, with the highest MAP kinase activity, followed by non-BRAF/non-RAS intermediate alterations (i.e., ETV6::NTRK and EML4::ALK fusions) with RAS-like alterations representing the least aggressive drivers with lowest MAP kinase activation potency in this study. TERT promoter mutation, BRAF p.V600E, and non-BRAF/non-RAS alterations are most often associated with more aggressive tumors including classic PTC and iFVPTC, whereas more indolent RAS-like alterations are more often associated with NIFTP and EFVPTC. 3 GEAs were subcategorized as BRAF p.V600E-like, RAS-like, and non-BRAF/non-RAS like and compared among histological groups.
Statistical analyses
The software used for statistical analyses was GraphPad PRISM Version 9.2.0 for Windows 64-bit (GraphPad Software, San Diego, CA). Comparisons were performed using chi-square analyses, and Fisher's exact tests were used when two variables were compared that each had two subgroups. Statistical significance was set as p < 0.05.
Results
Seventy-eight cases received ThyroSeq molecular testing: 29 NIFTP, 36 EFVPTC cases, and 13 iFVPTC cases. All cases in each category displayed a major genomic event (gene mutation, fusion, and/or GEA, and/or CNA), except one case in each category with no alterations found (ThyroSeq negative).
The average ages of patients with NIFTP, EFVPTC, and iFVPTC were 47, 49, and 57 years, respectively. Females outnumbered males in every category. The mean nodule size for all three diagnostic categories ranged from 2.4 to 2.7 cm. The majority of cases in all categories had Bethesda III cytology diagnoses. See Table 1 for tabulation of patient demographics, including age, sex, nodule size, cytology diagnosis, and extent of surgery.
NIFTP, EFVPTC, and iFVTPC Comparison by Age, Sex, Nodule Size, Cytology Diagnosis, and Surgical Procedure
Of the 36 EFVPTC cases, 12 cases displayed angioinvasion (8 focal, 4 extensive), 6 of which also displayed capsular invasion. The remainder displayed capsular invasion only. One EFVPTC had a concurrent classic PTC (microcarcinoma) with LN metastasis.
Of the 13 iFVPTC cases, 4 displayed angioinvasion (3 extensive, 1 focal). LN metastasis and extrathyroidal extension were present in one case that showed an ETV6::NTRK3 fusion.
NIFTP and EFVPTC cases displayed predominantly RAS-like alterations, RAS-like GEAs, and many showed CNAs (22q loss). Unique oncogenic driver alterations for the NIFTP cases included: 14 NRAS, 8 HRAS, 1 KRAS, 3 THADA::IGF2BP3 fusions, 1 BRAF p.K601E, 1 PTEN p.F21Lfs*3, 1 Negative; 20 of which displayed GEAs. The majority of the GEAs were RAS-like (n = 16), two were non-BRAF/non-RAS, and two were BRAF p.V600E-like. Seven cases displayed CNAs, all with 22q loss.
Genomic characterization of the EFVPTC cases included: 10 NRAS, 8 HRAS, 1 KRAS, 2 PAX8::PPARG fusions, 1 EIF1AX splice site mutation, 1 BRAF p.G469A, 1 BRAF p.K601E, 1 BRAF p.N486_P490del, and 1 THADA::IGF2BP3 fusion, which are all considered low-risk oncogenic drivers. Two cases were intermediate risk based on the presence of ETV6::NTRK3 fusion. Cases with an aggressive genomic profile included: 3 BRAF p.V600E and 1 CCDC6::RET fusion. EFVPTC cases with multiple drivers included two more aggressive drivers: 1 with NRAS and TERT promoter mutations (TERT allelic frequency: 32.5%); 1 with HRAS and TERT promoter mutations (TERT allelic frequency: 12%); and 1 case with less aggressive drivers: 1 with HRAS and EIF1AX splice site mutation. Twenty-five cases displayed GEAs. The majority of the GEAs were RAS-like (n = 17), 7 were BRAF p.V600E-like, 1 was non-BRAF/non-RAS. Twelve cases displayed CNAs, all with 22q loss, except for one case which had more widespread chromosomal CNAs (chromosomes 6, 17, 22). A single EFVPTC had no identifiable genomic drivers.
iFVPTC cases showed predominantly BRAF p.V600E-like and non-BRAF/non-RAS-like alterations and lacked CNAs. Tumors with aggressive drivers included: 3 BRAF p.V600E, 1 TERT promoter mutation (allelic frequency unknown), and 1 MET overexpression. Tumors with intermediate drivers included: 2 ETV6::NTRK3 fusions and 1 EML4::ALK fusion. Tumors with low-risk profiles included: 2 NRAS, 1 HRAS, and 1 THADA::IGF2BP3 fusion. Three cases displayed GEAs (1 BRAF-like, 1 RAS-like, 1 non-BRAF/non-RAS). None displayed CNAs. See Figure 5. A single iFVPTC had no identifiable genomic drivers.

Oncoplot displaying demographics and molecular alterations by surgical entity.
In comparing driver mutations among the three histological groups NIFTP, EFVPTC and iFVPTC, we found a statistically significant difference (p < 0.0001) when subcategorizing the drivers by levels of aggressiveness (low-risk/no driver vs. intermediate/high-risk driver) (Table 2 and Figure 6). When comparing only the two more “indolent” groups, NIFTP and EFVPTC, the difference remained significant (p = 0.0068). However, in comparing BRAF-like GEAs versus others (RAS-like, non-BRAF/non-RAS, and none), among the three histological groups, there was no significant difference (Table 3 and Figure 7).
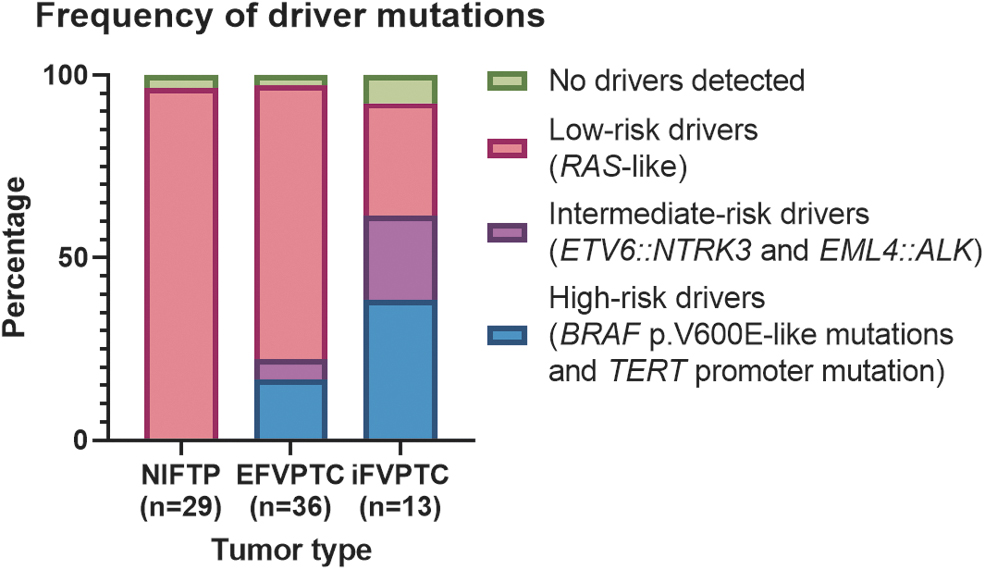
Histological groups and genetic driver risk levels.
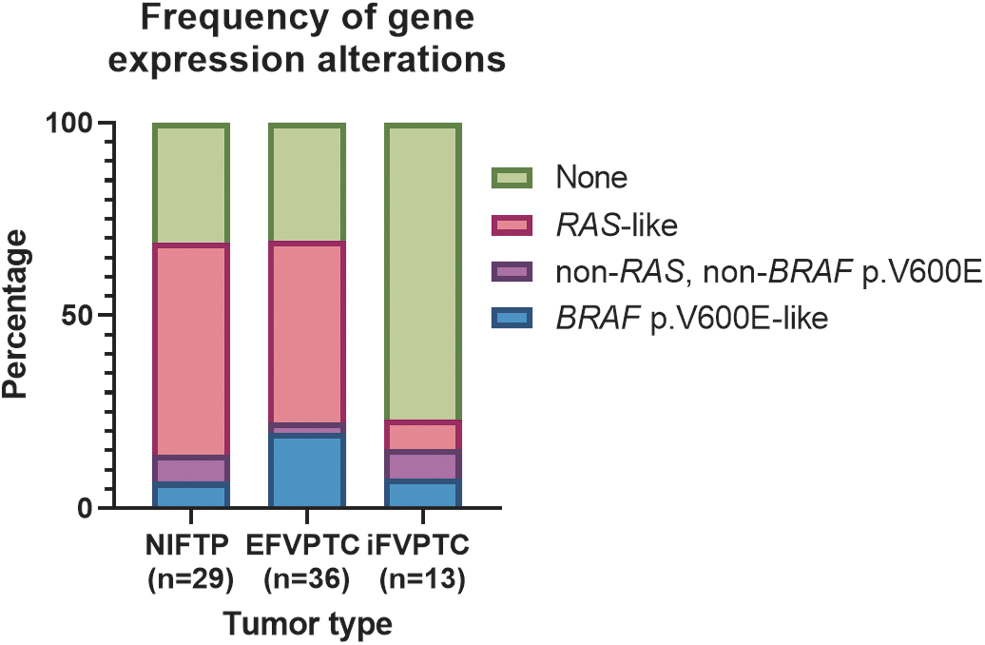
Histological groups and gene expression alteration types.
NIFTP, EFVPTC, and iFVPTC Separated by Low to Higher Risk Genetic Drivers
Two EFVPTC cases multiple driver mutations (RAS-like and TERT promoter mutations). They are classified under high-risk drivers in this table.
Gene Expression Alteration Type by the Histological Group
Discussion
It is clear from previously published foundational studies 3,9 that the genetic landscape of a tumor determines its biological behavior. RAS-like tumors are generally well differentiated with preservation of follicular architecture as well as expression of thyroid-specific genes such as thyroglobulin, thyroid peroxidase, the sodium iodide symporter, among many others. 3 However, BRAF-like tumors display greater activation of MAP kinase signaling resulting in decreased expression of thyroid-specific genes, loss of normal thyroid histological features, and transformation toward papillary architecture. Non-BRAF/non-RAS like tumors driven by fusions such as ETV6::NTRK3 and EML4::ALK fusions fall at an intermediate level of differentiation and MAP Kinase activity.
Our study found that more indolent tumors (NIFTP and EFVPTC) predominantly tended to display RAS-like alterations, although RAS-like mutations were not restricted to these tumors, and were seen in a minority of iFVPTC cases as well. Importantly, while the NIFTP group displayed exclusively low-risk genetic mutation drivers, the EFVPTC group displayed both low-risk mutations (in ∼3/4 of cases) and intermediate to high-risk mutations (in 1/4 of the cases) (Table 2). The more aggressive iFVPTC cases displayed predominantly intermediate-risk and BRAF-like alterations, with a minority of cases displaying less aggressive RAS-like mutations.
EFVPTC and NIFTP are histologically follicular tumors primarily driven by RAS and occasional intermediate-risk drivers. iFVPTC are also histologically follicular but driven by more potent activating mutations that are BRAF-like or occasionally intermediate, leading to the greater occurrence of invasion/infiltration. Although BRAF p.V600E is typically thought of as a marker of classic and other major variants of PTC, iFVPTCs are also associated with this marker and demonstrate more extensive invasion and infiltration compared with histologically follicular RAS-driven tumors such as EFVPTC and NIFTP. 5,10
All NIFTPs in our study were exclusively driven by RAS-like alterations, and although RAS-like alterations were present in 75% of EPVPTC cases, 5.6% and 16.7% of cases demonstrated intermediate-risk and higher-risk drivers, respectively. Furthermore, we found that iFVPTC cases in our study were genomically distinct from NIFTP and EFVPTC with intermediate- and higher risk drivers present in 8/13 (61.6%) cases and lower risk RAS-like mutations in only 4/13 (30.8%) cases. As RAS mutations occurred in all three groups, RAS cannot distinguish between these neoplastic lesions. However, sufficient clonal expression of an RAS mutation distinguishes a neoplasm from a benign hyperplastic nodule. 11
Of note, two EFVPTC cases displayed simultaneous TERT promoter and RAS driver mutations. Typically, TERT promoter mutations are considered high-risk drivers. Although the clinical significance of an isolated TERT promoter mutations is not entirely understood, 12,13 tumors expressing simultaneous TERT promoter and RAS mutations behave more aggressively and have been found in more poorly differentiated thyroid carcinomas. The lack of aggressive features in these two cases despite the expression of both TERT promoter and RAS may suggest that these EFVPTCs were identified at an early stage of tumor evolution before widely infiltrative features were able to develop. These findings indicate that close clinical follow-up is imperative in such cases and additionally highlight the significant value of preoperative molecular testing using FNA samples to assess a tumor's genetic profile in advance of determining the treatment plan.
Since BRAF p.V600E mutations are associated with more frequent extrathyroidal extension and LN metastasis, and RAS mutations with more indolent behavior, 14 understanding the molecular profile could inform the intensity of management. While EFVPTCs and NIFTPs have been shown to display molecular profiles and behaviors similar to histologically follicular tumors, such as follicular adenomas/carcinomas, iFVPTCs have been shown to display features in between those of classical PTC and follicular lesions. 5,10,15 Our study observed that BRAF-like mutations and intermediate driver mutations clustered most with the more aggressive tumors, which would be expected based on TCGA data. 3
As driver potency increased, the likelihood of iFVPTC (vs. NIFTP/EFVPTC) increased. Similarly, RAS mutations clustered with the least aggressive tumor groups. We found BRAF p.V600E mutations in 21% (3/14) of iFVPTC cases, which is higher than the 8.3% (3/36) of EFVPTC cases and 0% of NIFTP cases. Of note, BRAF p.V600E mutations are typically present in more than 50% of classic PTCs 5,16 and, similar to our study's findings, only in 0–26% of FVPTC cases. 5,15 –17 Chandler et al. found that NIFTP cases lacked BRAF p.V600E, EFVPTC cases demonstrated BRAF p.V600E in 12.5% (2/16), and iFVPTC cases displayed the highest number of BRAF p.V600E cases (4/16, 25%). 17 In our study, NIFTP cases lacked BRAF p.V600E mutations. One case displayed the more indolent BRAF p.K601E mutation (1/29), which is typically associated with histologically follicular lower risk tumors in contradistinction to the classic variant PTC and infiltrative FVPTCs associated with BRAF p.V600E and BRAF p.V600E-like drivers. 18 Three EFVPTC cases displayed non-BRAF p.V600E mutations (3/36).
As Rivera et al. have illustrated in their examination into EFVPTC and iFVPTC, the prevalence of extrathyroidal extension and LN metastasis were higher in iFVPTCs and particularly in BRAF p.V600E-mutated tumors. 5 George et al. similarly found that LN metastases were found at a higher rate in iFVPTC cases compared with EFVPTC and NIFTP cases. 10 NIFTP and EFVPTC cases have consistently been shown to have better outcomes than other forms of PTC, with fewer to no recurrences and lack of distant spread. 19 –22 In our study, both NIFTP and EFVPTC cases displayed indolent behavior (no local or distant metastases). However, 16.7% and 5.5% (6/36 and 2/36) of EFVPTC cases harbored BRAF p.V600E like/higher risk alterations and intermediate drivers (respectively), while NIFTP cases lacked BRAF-like/high-risk and intermediate driver alterations. Our results indicate that while the genetic alterations of NIFTP cases overlap considerably with that of EFVPTC, additional more aggressive genetic alterations may be seen once an encapsulated tumor starts to display capsular/vascular invasion.
CNAs in follicular adenomas and follicular carcinomas were compared using comparative genomic hybridization in a study by Hemmer et al. CNA chromosome 22q losses were more common in follicular carcinomas (46%) compared with adenomas (7%). 8,23,24 Our study found 22q loss CNAs in 24.1% of NIFTP cases (7/29) and in 30.6% of EFVPTC cases (11/36); however, our iFVTPC cases lacked CNAs. Taken together, these findings indicate that follicular patterned RAS-like lesions including NIFTP, EFVPTC, and follicular carcinomas harbor CNAs more commonly than follicular adenomas, classic PTCs, and iFVPTCs. 8,24
In addition to a similar prevalence of CNAs in the NIFTP and EFVPTC groups, our study also found that NIFTP and EFVPTC cases showed no significant difference in predominance of RAS-like GEA. The distribution of GEAs in this study, similar to the ThyroSeq v3 validation set, 8 did not distribute in any particular pattern and was present across all three diagnoses. While GEAs were most often RAS-like in our NIFTP and EFVPTC cohorts, 6.9% and 19.4% were BRAF-like GEAs, respectively. While the significance of this finding is not entirely understood, BRAF-like GEAs were more prevalent in EFVPTC compared with NIFTP cases, which correlate with the notion that NIFTP and EFVPTC represent distinct steps on the tumorigenesis continuum, with the two groups showing similar histology and overlapping molecular profiles, with EFVPTC showing minimal invasion, intermediate, and aggressive driver mutations and increased BRAF-like GEAs.
Despite the small sample size, our study adds to the existing literature and makes novel observations when comparing NIFTP, EFVPTC, and iFVPTC. Additional study limitations include the retrospective design, and small group of iFVPTC cases. Secondary to the retrospective nature of our study, this study also had selection bias due to our institution's standard of care, which limited most of our study cases to those with indeterminate cytology diagnoses that had previously received ThyroSeq testing. As our study has shown, NIFTP and EFVPTC cases appear to share similar molecular profiles (RAS-like) with more indolent drivers. However, a subgroup of the EFVPTC cases (∼1/4) displayed an intermediate risk to higher risk mutation profile, similar to iFVPTCs.
While EFVPTC are indistinguishable from NIFTP in presurgical FNA, the different genetic profile that can be identified with genetic testing on FNA samples can be used to a certain degree to guide the surgical decision making. iFVPTC cases, conversely, illustrate molecular profiles in between that of traditional follicular pattered lesions and classical PTC, with higher MAP kinase activity, intermediate and aggressive genetic drivers, and lower differentiation. The identification of more nuances in the molecular profiles of different histological entities can potentially increase the accuracy of preoperative decision-making, patient triaging, and decision-making regarding patient follow-up based on FNA cytology and molecular results.
Footnotes
Authors' Contributions
T.C.B.: Conceptualization, methodology, investigation, data curation, project administration, writing—original draft, writing—review and editing, visualization. F.Z. and C.Z.L.: Methodology, investigation, formal analysis, data curation, writing—review and editing. A.S.: Investigation, data curation, writing—review and editing. W.S. and Y.E.N.: Conceptualization, data curation, methodology, writing—review and editing. S.P.H.: Conceptualization, investigation, methodology, data curation, writing—review and editing, supervision, project administration, visualization.
Author Disclosure Statement
T.C.B., F.Z., C.Z.L., A.S., W.S.: No disclosures. Y.E.N. owns IP and receives royalties related to ThyroSeq from the University of Pittsburgh; he serves as a consultant for Sonic Healthcare USA. S.P.H. received compensation from SonicHealth USA for speaking about ThyroSeq.
Funding Information
This study was funded by the Departmental funds, NYU Langone Health, Department of Pathology.