
Abstract
Background:
There is some controversy on the potential relationship between autoimmune processes and clinicopathologic features as well as prognosis of differentiated thyroid cancer (DTC), and the evidence is limited by its largely retrospective nature. We examined the relationship between the presence of autoimmune thyroiditis (AT) and 1-year thyroid cancer treatment outcomes in a large multicenter study using prospectively collected data.
Methods:
We included data from consecutive DTC patients enrolled in the Italian Thyroid Cancer Observatory (ITCO) database (NCT04031339). We divided the groups according to the presence (AT) or absence (no autoimmune thyroiditis [noAT]) of associated AT. We used propensity score matching to compare the clinical features and outcomes between the two groups at 1-year follow-up.
Results:
We included data from 4233 DTC patients, including 3172 (75%) females. The American Thyroid Association (ATA) risk levels were as follows: 51% (2160/4233) low risk, 41.3% (1750/4233) intermediate risk, and 7.6% (323/4233) high risk. There were 1552 patients (36.7%) who had AT. Before propensity score matching, AT patients were significantly younger and had a smaller and bilateral tumor (p < 0.0001). Patients with AT more frequently fell into the low- and intermediate-risk categories, while the ATA high risk was more frequent among noAT patients (p = 0.004). After propensity score matching, patients with AT more frequently showed evidence of disease (structural/biochemical incomplete response) versus excellent/indeterminate response, compared with patients without AT (7.3% vs. 4.5%, p = 0.001), with an odds ratio of 1.86 ([confidence interval: 1.3–2.6], p = 0.0001). However, when considering only structural persistence as the outcome, no statistically significant differences were observed between patients with or without AT (3.4% vs. 2.7%, p = 0.35). The elevated risk associated with the ATA intermediate and high risk at diagnosis remained consistently statistically significant.
Conclusions:
In this large prospective series, biochemical persistence was more frequent, at 1-year follow-up, in AT patients. However, there was no significant association between the presence of AT and structural persistence of disease. These findings may be explained by the presence of a residual thyroid tissue.
Introduction
The relationship between differentiated thyroid cancer (DTC) and thyroiditis detected in extratumoral thyroid tissue is well known. 1,2 Despite being two extremely frequent diseases, their association cannot be considered fortuitous, although the underlying pathogenetic mechanisms, possibly common or interacting, are not known. Chronic autoimmune thyroiditis (AT) accompanies frequently papillary thyroid carcinoma (PTC), but it is also often found in patients with follicular thyroid carcinoma (FTC). 3 Abundant but controversial data, almost exclusively based on retrospective series, exist on the possible increased risk of developing thyroid cancer (TC) in patients with AT. 4 –6 Similarly, data are not definitive when considering the possible impact of the autoimmune process on TC, clinicopathologic features, and prognosis. Two large meta-analyses, including data largely from retrospective series, reported that patients with coexistent AT had less aggressive characteristics at presentation and better outcomes of PTC than patients without AT. 2,7
However, some authors insist on a null or negative influence of the autoimmune process on cancer course. 8 –10 A recent study using mouse model showed that AT developing at the same time of DTC influences its course minimally, while a pre-existing thyroiditis markedly decreases both incidence and severity, indicating a critical role of the immune system on TC pathogenesis. 11 Although highly valuable for insights provided to this topic, this model cannot fully recapitulate human disease since both the carcinogenetic process and the murine iodine-induced thyroiditis are different from the corresponding human diseases. The discrepancies observed among different studies, related to the positive or negative impact of AT on DTC outcome, could be due to several factors, including the time relationship between the autoimmune and the neoplastic process, the low sample volumes, the diagnostic biases, the different outcome definitions, the genetic and environmental backgrounds, and the retrospective design of the studies.
To obtain more reliable insights into this controversial topic, we compared the clinical features and outcomes of patients with chronic AT with those without AT in a large prospectively collected Italian database of DTC patients. We aimed to evaluate possible differences between the two groups in terms of response to initial treatment, evaluated at 1-year follow-up visit.
Methods
In 2013, a web-based database was founded and named Italian Thyroid Cancer Observatory (ITCO). Starting from the Thyroid Cancer Center of Sapienza University of Rome (the coordinating center), the network expanded and now includes 51 Italian centers. Data are prospectively collected, and to date, more than 10,000 patients with histologically confirmed diagnoses of differentiated, medullary, poorly differentiated, and anaplastic TC are included [see (a) in the Supplementary Methods] (NCT04031339).
We have already reported the baseline data of the first enrolled patients, 12 a validation of the baseline risk estimates on the first 2000 patients reaching 1-year follow-up evaluation, 13 and an assessment of the role of extrathyroidal extension. 14
All ITCO database records were reviewed, and consecutive cases that satisfied the following criteria were considered for the analysis: (1) histological diagnosis of TC (with exclusion of medullary TC, non-invasive follicular thyroid neoplasm with papillary like nuclear features, well differentiated tumor of uncertain malignant potential); (2) available information on the presence of thyroiditis based on thyroid peroxidase antibody and/or thyroglobulin antibody (TgAb) levels higher than the upper normal limits, and at least one of the following: (a) anamnestic data consistent with AT; (b) characteristic ultrasound features (i.e., nonhomogeneous pattern with diffuse reduction of echogenicity) before surgery; and (c) histological description of a diffuse inflammatory infiltrate; 15 (3) availability of all information on the initial treatment and histological data of the tumor required for the American Thyroid Association (ATA) recurrence risk assessment; 16 (4) availability of the results for the 1-year follow-up visit, including all data needed to classify the estimated treatment response; (5) complete data of the features used to compare the group; (6) clinical centers that are in the top three quartile in terms of case frequency (only high volume was included to guarantee a more precise and reliable information).
According to the above-reported inclusion criteria, 4233 patients were included, out of the 10,078 recorded at data lock (November 2021) (Fig. 1).
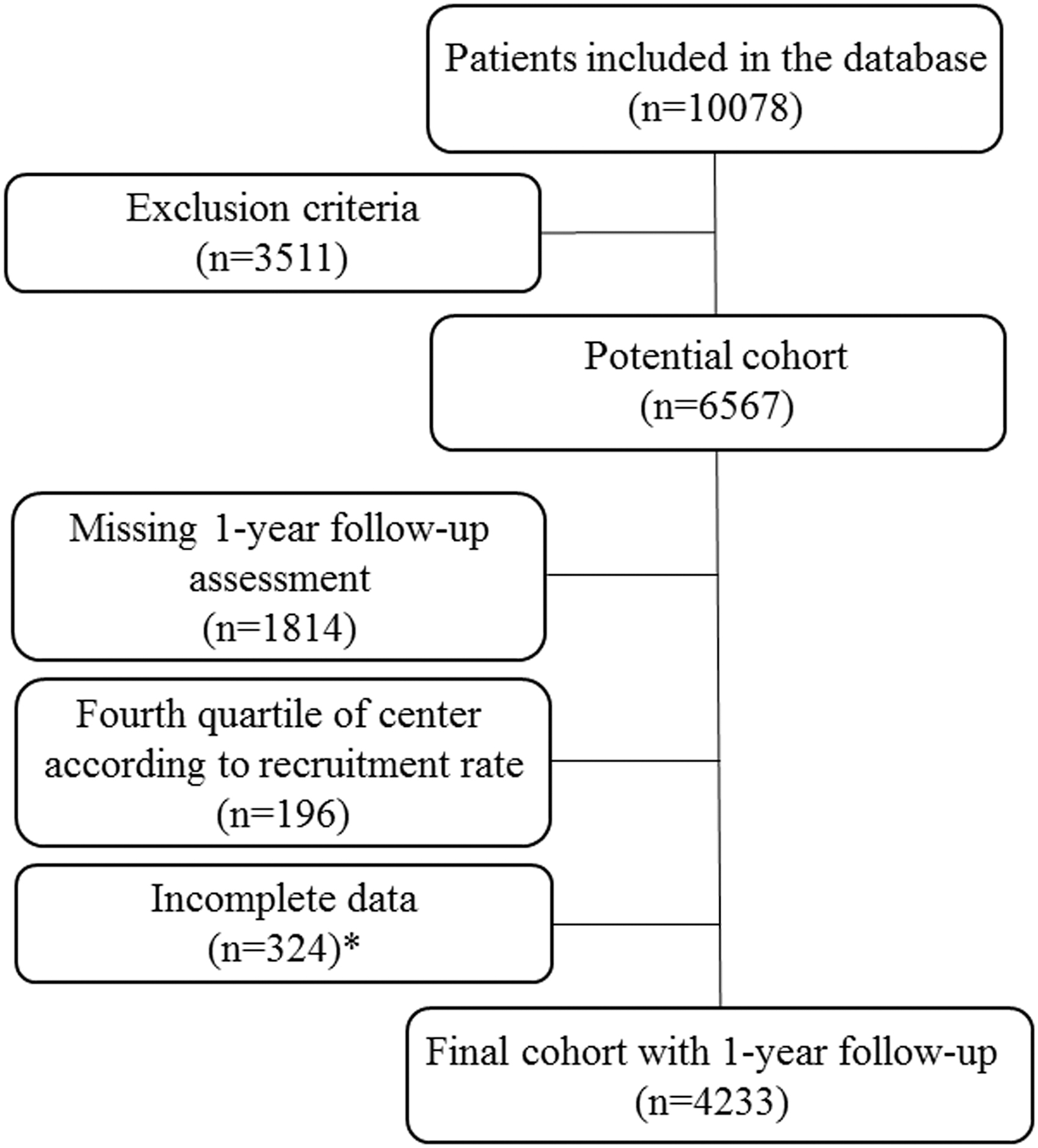
Participants' flowchart. *There were no statistical differences in terms of sex, age, race, or ATA risk (p = 0.6, 0.5, 0.22, 0.14, respectively) between the final cohort, and this group of 324 patients who were excluded due to the lack of specific information that we deemed important for our analysis. ATA, American Thyroid Association.
Data on the initial treatment were recorded for each case. Treatment of the primary tumor was classified as thyroid lobectomy or total thyroidectomy. The latter category also included patients who had a completion thyroidectomy following thyroid lobectomy. For all patients who had a total thyroidectomy, we recorded if they received radioactive iodine treatment (RAI).
The estimated risk of persistent disease was determined by the study team in accordance with the 2009 ATA guidelines 17 and relevant 2015 updates 16 based on the data available immediately after the initial treatment. If the surgical treatment consisted of lobectomy followed by completion thyroidectomy, the histopathology data collected during both surgical procedures were considered. Response to initial therapy was evaluated based on the clinical evaluation carried out at the 1-year follow-up visit (6–18 months after the initial treatment). These data included imaging findings (cervical ultrasound in all patients and 131I whole-body scan in selected individuals) and basal or stimulated serum thyroglobulin (Tg) and anti-TgAb levels.
Additional imaging studies were performed per the clinicians' discretion. According to the 2015 ATA guidelines, an excellent response was defined as no clinical, biochemical, or structural evidence of disease after initial therapy (no evidence of disease); biochemical incomplete response was defined as abnormal Tg, that is, suppressed Tg ≥1 ng/mL or stimulated Tg ≥10 ng/mL, with negative imaging. However, because data from only one time point were evaluated, we were unable to evaluate TgAb levels trend: all cases classified as biochemical incomplete responses had measurable Tg levels.
Structural incomplete response was defined as persistent or newly identified locoregional or distant metastasis; and indeterminate response was defined as nonspecific biochemical/structural findings that could not be confidently classified as either benign or malignant. 16 Indeterminate responses included cases with Tg <1 ng/ml but detectable and/or positive TgAb. Considering that indeterminate responses at 1-year follow-up often represent cases with an indolent tumor behavior that eventually achieve a final excellent response, 18 we grouped patients as follows: (1) those with excellent and indeterminate response versus those with biochemical and structural persistence, and (2) those with excellent, indeterminate, and biochemical response versus those with structural persistence. The results were defined as specified in the ATA guidelines for patients who had undergone thyroidectomy followed by RAI, 16 and as advocated by the European Society for Medical Oncology 19 for those whose initial treatment consisted of surgery alone (thyroidectomy or lobectomy).
The prospective study was approved by the Coordinating Center Ethics Committee (Sapienza University of Rome, Ref. 3366). The study was performed in accordance with the ethical standards of the Institutional Research Committee and with the Declaration of Helsinki as revised in 2013.
Statistical analysis
For exploratory purposes, the distribution of continuous variables was summarized using median with interquartile ranges (IQRs). Nominal variables were described in terms of frequency counts and corresponding percentages. The chi-squared test was used to evaluate significant associations in contingency tables. Welch's t-test was used to assess the association between continuous variables in different groups. The response to treatment, initially, was analyzed as a categorical variable with four levels (structural incomplete, biochemical incomplete, indeterminate, and excellent). We analyzed treatment response as a binary variable as either an excellent/indeterminate or structural/biochemical incomplete response, too. Finally, a binary response variable composed of excellent/indeterminate/biochemical incomplete versus structural incomplete was analyzed [see (b) in the Supplementary Methods].
To analyze the effect of thyroiditis on treatment response, the patients may not be comparable in terms of other features such as sex, age, treatment, tumor size, extrathyroidal extension, lymph node metastasis, histology, tumoral foci, vascular invasion, and administered activity of radioiodine. The propensity score was defined using these characteristics, and the predicted value was used to create propensity score-matched groups [see (c) in the Supplementary Methods]. The p-value was defined as statistically significant when <0.05.
Results
Patients
The clinicopathologic characteristics of the 4233 patients included are reported in Table 1. Female patients were predominant (3172/4233, 75%), and the median age at diagnosis was 49 years (IQR 39–59 years). The majority of patients (4072/4233, 96.2%) underwent total thyroidectomy, associated with central and/or lateral neck dissection in 1582 of the 4233 (37.4%) cases. RAI treatment was performed in 2560 of the 4233 (60.5%) patients. In terms of histology, PTC was most prevalent (3960/4233, 93.5%), and the median tumor size was 12 mm (IQR 7–20 mm). The tumor was unifocal in 2498 of the 4233 (59%) patients and multifocal in 1675 of the 4233 (39.6%) patients; among these, multifocality was bilateral in 1134 of 1629 (69.6%) patients.
Clinical and Pathological Characteristics of the Study Cohort (N = 4233)
The estimated risk of persistent disease followed the 2009 ATA guidelines 17 and relevant 2015 updates 16 according to the available data after the initial treatment.
ATA, American Thyroid Association; CC, central compartment; F, female; FTC, follicular thyroid carcinoma; IQR, interquartile range; LC, laterocervical compartment; LT, lobectomy; PTC, papillary thyroid carcinoma; RAI, radioactive iodine treatment; TT, total thyroidectomy.
Extrathyroidal extension was present in 1298 of the 4233 (30.6%) cases, being microscopic in 1170 of the 1298 (90.1%) cases. Lymph node metastases were documented in 976 of the 4233 (23.1%) patients, whereas distant metastases at diagnosis were present in 109 of the 4233 (2.6%) patients. Vascular invasion was reported in 704 of the 4233 (16.6%) cases. According to the ATA risk stratification system, 2160/4233 (51%), 1750/4233 (41.3%), and 323/4233 (7.6%) patients were classified at a low, intermediate, and high risk of recurrence, respectively. Finally, associated thyroiditis was reported in 1552 of the 4233 (36.7%) patients of the entire cohort.
Association of thyroiditis with clinical and pathological variables
The clinical and pathological characteristics of TC patients divided according to the presence/absence of associated AT (AT/noAT [no autoimmune thyroiditis]) are reported in Table 2. AT patients were significantly younger (p < 0.0001) and were more frequently female (1296/1552 [83.5%] vs. 1876/2681 [70%], p < 0.0001). The use of RAI was more frequent among noAT patients (1651/2681 [61.6%] vs. 909/1552 [58.6%] patients with thyroiditis, p = 0.01), although no differences were noted in the RAI activity administered (p = 0.45). NoAT cases were treated more frequently with lobectomy (112/2681 [4.2%] vs. 49/1552 [3.2%], p = 0.01), while AT cases performed more often a neck dissection (654/1552 [42.1%] vs. 928/2681 [34.6%], p < 0.0001).
Clinical and Pathological Characteristics of Thyroid Cancer Patients According to the Presence/Absence of Associated Chronic Autoimmune Thyroiditis, Before Propensity Score Matching
Please note that when the data were not available in the whole cohort, the number of cases included is reported in parentheses in the first column.
AT, autoimmune thyroiditis; noAT, no autoimmune thyroiditis.
Patients with AT more frequently had a papillary histotype (1479/1552 [95.3%] vs. 2481/2681 [92.5%], p = 0.0005), a smaller tumor (11 mm vs. 12 mm, p < 0.0001), and a bilateral tumor (472/1534 [30.8%] vs. 662/2639 [25.1%], p = 0.0009). No differences were found in the rates of extrathyroidal extension, vascular invasion, lymph node, and distant metastatic dissemination. Finally, according to the ATA risk stratification system, patients with AT had more frequently a low (803/1552 [51.7%] vs. 1357/2681 [50.6%]) and intermediate (658/1552 [42.4%] vs. 1092/2681 [40.7%]) risk of recurrence, while the ATA high risk was more frequent among noAT patients (91/1552 [5.9%] vs. 232/2681 [8.6%], p = 0.004).
The effect of thyroiditis on initial treatment response
At the 1-year follow-up visit, we observed an excellent response in 3368 of the 4233 patients (79.6% of the entire cohort), while 141 of the 4233 (3.3%) patients had a structural incomplete response. Patients with AT had more frequently a biochemical incomplete response (62/1552 [4%] vs. 48/2681 [1.8%]) and an indeterminate response (484/1552 [31.2%] vs. 130/2681 [4.8%]) (Table 3).
Treatment Response at 1-Year Evaluation According to the Presence/Absence of Associated Chronic Autoimmune Thyroiditis (N = 4233)
Among the 141 patients with structural persistence of disease, 117 (82.9%) had a local involvement, 43 (30.5%) had distant metastases, and 19 had local and distant persistent disease (i.e., 98 cases, 69.5%, had only local disease).
After propensity score matching (Table 4), patients with AT more frequently had evidence of disease (structural or biochemical incomplete response) versus excellent and indeterminate response, compared with patients without AT (114/1552 [7.3%] vs. 66/1552 [4.3%], p < 0.0001), with an odds ratio (OR) of 1.97 ([confidence interval, CI: 1.4–2.7], p < 0.0001). This risk was lower than that predicted by the ATA intermediate risk (OR 2.54 [CI: 1.76–3.7]) and the ATA high risk at diagnosis (OR 10.8 [CI: 6.7–17.5], p < 0.0001) (Table 5). However, on considering only structural persistence as the outcome, no statistically significant differences were observed between patients with or without AT (52/1552 [3.4%] vs. 42/1552 [2.7%], p = 0.35), with an OR of 1.3 ([CI: 0.8–1.97], p = 0.26). The risk predicted by the ATA intermediate and high risk at diagnosis remained statistically significant (OR 3 [CI: 1.77–5] and 14.2 [CI: 7.6–26.6], respectively, p < 0.0001) (Table 6). Consistently, biochemical incomplete responses were more frequent in AT cases (62/1490 [4.5%] vs. 24/1528 [1.5%], p < 0.0001), with an OR of 2.64 ([CI: 1.6–4.4], p < 0.0001).
Clinical and Pathological Characteristics of Thyroid Cancer Patients According to the Presence/Absence of Associated Chronic Autoimmune Thyroiditis, After Propensity Score Matching
Please note that when the data were not available in the whole cohort, the number of cases included is reported in parentheses in the first column.
Evidence of Disease (Structural Incomplete Response+Biochemical Incomplete Response) After Having Matched Patients 1:1 (Top), and Odds Ratio for Structural Incomplete Response+Biochemical Incomplete Response Versus Excellent Response+Indeterminate Response at 1-Year Follow-Up (Bottom)
BIR, biochemical incomplete response; CI, confidence interval; IR, indeterminate response; OR, odds ratio; SE, standard error; SIR, structural incomplete response.
Evidence of Structural Disease (Structural Incomplete Response) After Having Matched Patients 1:1 (Top), and Odds Ratio for Structural Incomplete Response Versus Excellent Response+Indeterminate Response+Biochemical Incomplete Response at 1-Year Follow-Up (Bottom)
Discussion
In this study, we presented the clinical features and outcomes of more than 4000 prospectively collected DTC patients, with or without associated chronic AT. AT cases had a significantly lower ATA risk, and no differences were found at presentation in terms of extrathyroidal extension, vascular invasion, and locoregional or distant metastases, compared with noAT patients. In addition, AT cases were diagnosed at a significantly younger age and had smaller tumors, likely due to the early detection of the tumor facilitated by the coexisting thyroid disease. This finding is in line with a case–control study that showed earlier stage diagnosis of PTCs in patients with known thyroid autoimmunity. 20
After thorough matching to minimize selection bias, we observed no significant differences in structural persistence at the 1-year follow-up after initial treatment between DTC patients with and without AT. However, patients with AT more frequently exhibited evidence of disease when considering both structural and biochemical persistence together (7.3% vs. 4.3%, p = 0.001). Consistently, biochemical persistence was more frequent in AT cases than in noAT cases (4% vs. 1.5% after matching) likely due to the persistence of residual thyroid tissue. The higher occurrence of Tg-producing thyroid tissue in AT cases could be due to the greater difficulty in achieving a complete surgical thyroid removal and a complete nodal resection in patients with coexisting AT, as such surgical cases may be subject to less mobility of the gland and a more fibrosis. The presence of thyroid autoimmunity is thus reported as one of the predictors of a challenging thyroidectomy. 21,22
Although discordant data have been always reported on this topic, a recent meta-analysis, including 47,237 patients from 65 articles, including 12,909 AT patients and 34,328 noAT cases, showed that DTC patients with AT may have favorable clinicopathologic characteristics, lower recurrence rate, and better 20-year survival rate. 7 Nevertheless, the authors claimed for more prospective studies to reliably elucidate this relationship. Indeed, although appropriate statistical analyses, residual confounding variables influencing the results could not be ruled out, and most of the included studies were retrospective without available clinical details. In this context, the strengths of the present study need to be mentioned. The present large series is consecutive, longitudinal, and prospective.
Moreover, the present patients' cohort has been collected starting from 2013, whereas the series included in the above-mentioned meta-analysis embrace a very long time span during which different guidelines' suggestions were followed and different outcome classifications were applied. In particular, among the 16 of the 65 articles on this topic, which report data on the outcome, only 6 specify the percentage of patients treated by RAI, corresponding to the majority of patients in most studies. Finally, this is the only study analyzing data after propensity score matching, applied with the aim to minimize the bias due to confounding variables such as treatment, administered activity of radioiodine, follow-up protocols, or other intervention, and to increase the reliability of the results obtained.
This study is subjected to some limitations. First, the definition of AT, based exclusively on biochemical data and/or, ultrasonographic, and/or histological findings, may be considered a drawback of the study. Nevertheless, the histological classification of associated AT is extremely variable among sites and sometimes not even reported by the pathologist. A reliable assessment of the presence of associated AT will definitely need the histological revision of cases by one or two pathologists. This will require the exchange of samples, thus leading to the reduction of the cases included. A future study including a central evaluation of specimens has been already planned. Second, the follow-up period was only 1 year. Nevertheless, it is well accepted that the risk classification performed at 1 year after initial treatment is highly predictive of the final response to treatment. 23 –25 Future analyses on the same series will evaluate the outcome at 5 years after initial treatment.
Furthermore, indeterminate responses were likely overestimated in AT cases, due to the persistence of TgAb. These cases were included among excellent responses, based on data reporting that the vast majority of patients with an initial indeterminate response spontaneously achieve an excellent response, 18 and relying on the “dilution” effect of such a large series. A longer follow-up period will provide valuable information on the percentage of cases initially classified as indeterminate or biochemically incomplete that may be reclassified as excellent responses. Finally, an interinstitutional variability in the accuracy of case descriptions, in the histological classification, and in the clinical/biochemical/ultrasonographic evaluation can be envisaged due to the multicenter nature of this cohort, although we previously demonstrated that these differences did not impair the prediction of the outcomes. 13
In conclusion, our large prospective series of DTC patients demonstrated an excellent response in more than 90% of cases in both groups at the 1-year follow-up after initial treatment. Importantly, the presence of chronic AT did not have a significant impact on structural disease persistence, but it was associated with a higher frequency of biochemical persistence. Future studies will focus on evaluating the same patient cohort with a longer follow-up period to provide a more comprehensive assessment of treatment outcomes and the potential long-term effects of thyroiditis.
Footnotes
Acknowledgments
We thank all the collaborators of the ITCO Network: Matteo Trevisan and Carla Colombo (Endocrine Oncology Unit, IRCCS Istituto Auxologico Italiano, Milan, Italy); Roberta Rossi (Endocrinology, Geriatrics and Internal Medicine, University of Ferrara, Italy); Pietro Locantore, Cesare Morgante, and Annamaria D'Amore (Università Cattolica del Sacro Cuore and Fondazione Policlinico Universitario A. Gemelli IRCCS, Rome, Italy); Nicoletta Rolli and Lisa Caresia (Endocrinology and Diabetology Unit, Azienda Ospedaliera-Universitaria di Verona, Italy); Antonella Carbone (Endocrine Unit, Tinchi Hospital, ASM, Matera, Italy); Maria Giulia Santaguida (UOC Endocrinologia, AUSL Latina, Italy); Monica Cereghino (Unit of Endocrine Organs and Neuromuscolar Pathology, Fondazione Campus Bio-Medico, Rome, Italy); Liliana de Laurentiis, Sara Margarella, and Roberto Parisi (UOC Endocrinologica Diabetologica, AOU San Giovanni di Dio e Ruggi d'Aragona, Salerno, Italy); Francesca Piccinini and Eleonora Zanni (Endocrinology Unit, Azienda Ospedaliero-Universitaria Policlinico di Modena, Italy); Sofia Carducci, Cristina Clausi, and Ilaria Piva (Unit of Endocrinology, University of Padua, Italy).
Authors' Contributions
S.D.L. and L.F.: Conceptualization (equal), formal analysis (equal), writing—original draft (lead). S.D.: Statistical analysis (lead). G.G., S.F., and C.D.: Conceptualization (equal), formal analysis (equal), writing—original draft (supporting). F.D., F.B., E.P., S.M., A.Pi., A.N., M.C.Z., I.G., M.T.S., G.A., U.C., M.M., M.D., F.R.,
Author Disclosure Statement
C.D. is an Associate Editor at Thyroid, but he had no role in the review of this article and was blinded to the peer-review process. All other authors have no conflicts of interests to disclose.
Funding Information
The study was supported by the Sapienza University of Rome Research Grant (RM11916B83A211FC) to C.D. and by the Italian Ministry of Health (THY-CANC ID 2.773.026) to S.D.L. and L.F. All other authors have no funding information to declare.
Supplementary Material
Supplementary Methods