
Abstract
Background:
Molecular testing (MT) is emerging as a potential prognostic factor that can be available before treatment of differentiated thyroid carcinoma begins. Among patients eligible for either lobectomy or total thyroidectomy as their initial therapy, our study aims were to assess (1) if conventionally available preoperative factors are associated with incomplete response to initial therapy, and (2) if MT results can be a surrogate for the ATA Risk Stratification System (RSS) to estimate risk of recurrence.
Methods:
The data of consecutive thyroid cancer patients without preoperative lateral neck disease or distant metastasis who underwent index thyroidectomy between November 1, 2017 and October 31, 2021 were reviewed. Logistic regression models including preoperative variables such as MT and/or the postoperatively available RSS were constructed to predict disease recurrence, either structural or biochemical. Model discrimination using the c-statistic and goodness-of-fit test were compared.
Results:
Among 945 patients studied, 50 (5.2%) recurred with 18-month median follow-up. Recurrences were detected in 17 (2.9%), 20 (6.7%), and 13 (22.8%) patients with RSS-low, -intermediate, and -high cancers, respectively (p < 0.001). In multivariable analysis, only tumor size was associated with recurrence (odds ratio [OR] 1.3, 95% confidence interval [CI] 1.1–1.5). In a different model analyzing 440 (46.6%) patients with available MT results, recurrence was associated with both larger tumor size (OR 1.4 [95% CI 1.1–1.8]) and MT results (p < 0.001). Including MT improved the c-statistic by 27%, which was statistically no different than the model incorporating only the RSS (p = 0.15).
Conclusions:
Disease recurrence was observed across all ATA RSS categories in short-term follow-up, and tumor size was the only conventional preoperative factor associated with recurrence. When MT results were incorporated, they not only improved predictive ability beyond tumor size alone, but also yielded similar ability as the gold standard ATA RSS. Thus, MT results might aid the development of novel preoperative risk stratification algorithms.
Introduction
For patients with differentiated thyroid carcinoma (DTC) who present with lateral neck disease or distant metastasis, total thyroidectomy (with or without therapeutic neck dissection or adjuvant radioactive iodine [RAI]) is uniformly recommended because of the intrinsically high risk for recurrence. Fortunately, most patients present with less extensive disease and can thus be considered for less extensive treatment, including thyroid lobectomy alone. 1,2
In cases that do not clearly fall within the bookends of the recurrence risk continuum, treatment decisions are more nuanced and use risk stratification schemas, such as the 2015 ATA Risk Stratification System (RSS), to predict recurrence and inform management. While surgical pathology results represent a key snapshot of cancer biology and thus should factor heavily into risk prediction schemas, such reliance on surgical pathology can theoretically subject nearly half of patients to two operations based on newly identified pathological information not known preoperatively. 3 –5
For example, a patient with a 2-cm indeterminate nodule on cytology found after diagnostic lobectomy to be a follicular thyroid carcinoma with microscopic extrathyroidal extension and extensive angioinvasion after diagnostic lobectomy would likely require completion thyroidectomy to facilitate adjuvant RAI and/or surveillance—compared with if the nodule were a 2 cm completely encapsulated follicular variant papillary thyroid carcinoma. Understanding which patients are more likely to recur before any treatment begins may help to expedite care, ensure that the first surgery is the last one, and minimize the risk for recurrence.
Molecular testing (MT) of fine needle aspirates (FNA) improves the diagnostic yield of detecting cancer in indeterminate thyroid nodules. 6 –8 Recent studies have also demonstrated links between MT results and surgical pathology, 9,10 and early recurrence. 11 –16 Among patients eligible for either lobectomy or total thyroidectomy as their initial therapy, our study aims were to assess (1) if conventionally available preoperative factors are associated with incomplete response to initial therapy, and (2) if MT results can be a surrogate for the RSS to estimate risk of recurrence. In this way, we eventually anticipate being able to move the ability to risk stratify to a timepoint before any treatment begins.
Materials and Methods
Consecutive patients who underwent index thyroidectomy (lobectomy or total) for any clinical indication and had pathologically identified primary DTC (papillary, follicular, oncocytic/Hürthle cell) between November 1, 2017 and October 31, 2021 were abstracted from the electronic health record to conduct this retrospective cohort study. Patients with medullary thyroid cancer or noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) were not abstracted. Patients who had initial thyroid surgery earlier or elsewhere for benign disease and then completion thyroidectomy for thyroid carcinoma during the study period were not abstracted. Patients who had previous thyroid surgery earlier or elsewhere for DTC and then required reoperation during the study period were also not abstracted. In cases of multifocal cancer, the thyroid cancer type with the most aggressive histology was recorded, as this dictated clinical care. The University of Pittsburgh Institutional Review Board approved this study (QIIRB No. 1055).
Patients who had lateral neck nodal disease or distant metastasis at presentation were excluded as they represented the highest risk patients (i.e., total thyroidectomy necessary). Patients who had carcinomas smaller than 1.0 cm and low risk according to the RSS were also excluded as they represented the lowest risk patients (i.e., lobectomy alone appropriate; Fig. 1).
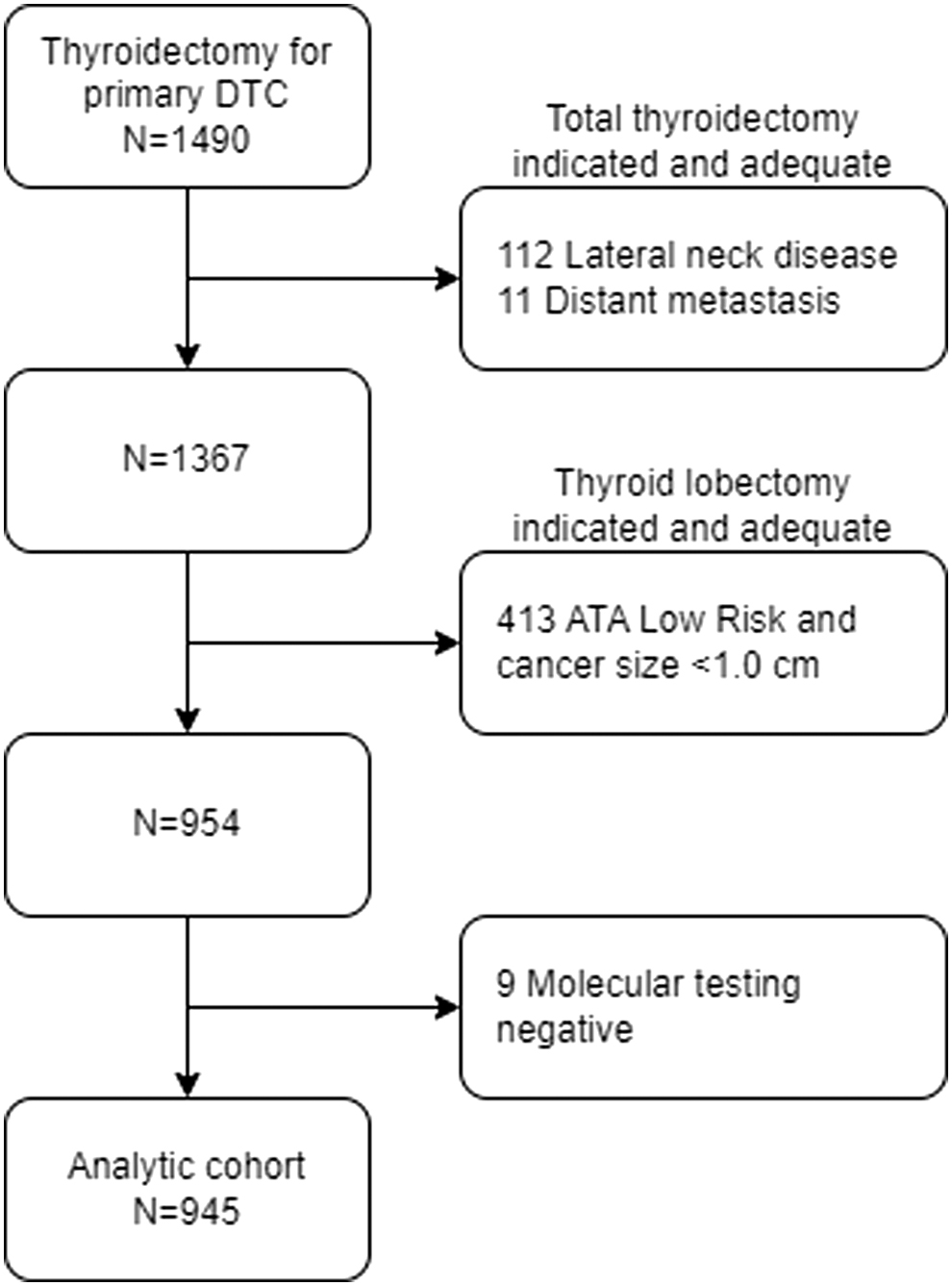
Participant flow diagram to create the study cohort. ATA, American Thyroid Association; DTC, differentiated thyroid carcinoma.
Indications, preoperative evaluation, extent of surgery, and postoperative cancer management followed the 2015 ATA and 2020 AAES Thyroidectomy Guidelines. 1,2 The dates of surgery and last clinical encounter were used to calculate follow-up.
Preoperative characteristics
Typical patient and tumor characteristics included age, sex, preoperative levothyroxine use, Bethesda cytology category (I–VI), and tumor size. All cytological categories were included. Ultrasound characteristics for each primary thyroid cancer were not examined because reporting of findings was not standardized during the study period and prior studies observed limited prognostic value. 17 –19
Because the cancer molecular profile is another variable that can be obtained preoperatively, MT results, when available, were examined as a novel predictor of recurrence. For consistency and because the test type provides specific molecular data including TERT promoter mutation status, only cases with ThyroSeq® version 3 (TSv3) targeted next-generation sequencing assay were used for this analysis. 20 MT occurred as part of routine clinical care following guidelines and/or when results would change management. 1,2 MT information obtained on preoperative FNA cytology and final surgical specimens were included in this study; if MT on both were present, preoperative FNA cytology results were preferentially used. As in any retrospective study, physicians involved in patient care were not blinded to MT results.
Because TSv3 analyzes 112 genes for combinations of molecular alterations, including mutations, fusions, gene expression alterations, and copy number alterations, numerous permutations are possible. In this study, 108 unique molecular permutations, or profiles, were categorized into three Molecular Risk Groups (MRGs) of increasing intrinsic risk for recurrence following previously reported methodology (Table 1): MRG-low, MRG-intermediate, and MRG-high. 21 –23
MRG, Molecular Risk Group.
Recurrence
The primary outcome measure was structural or biochemical recurrence, defined in a nested manner. First, patient records were reviewed to identify those who completed their initial course of therapy according to the 2015 ATA Guidelines and multidisciplinary tumor board review, when needed. 1 Next, we identified structural or functional evidence of disease with any thyroglobulin (Tg) level with or without anti-Tg antibiotics (i.e., structural incomplete response) including biopsy-confirmed recurrence and/or characteristic locoregional (i.e., central and lateral neck) or distant metastasis (lung, bone, etc.) on imaging (ultrasound, RAI avidity, 18 FDG avidity, etc.) following initial negative postoperative studies.
Then, those without evidence of structural recurrence were evaluated for potential biochemical recurrence, defined as suppressed Tg ≥1.0 ng/mL, stimulated Tg ≥10 ng/mL, or rising anti-Tg antibody levels using three timepoints (i.e., biochemical incomplete response). Biochemical recurrence after lobectomy alone was defined as a Tg ≥30.0 ng/mL. Patients who did not fit this nested definition of recurrence (i.e., excellent or indeterminate responses) did not recur.
Additional clinicopathological characteristics
Perioperative details included surgeon specialty (endocrine surgery, otorhinolaryngology, and general surgery), extent of thyroidectomy (total thyroidectomy, completion thyroidectomy, and lobectomy), central neck dissection (prophylactic and therapeutic), and receipt of postoperative RAI. Patients underwent intentional central neck dissections at the discretion of the treating surgeon, as determined from operative report review, and per guideline recommendations. 2 Identification of central neck lymph nodes on final pathology without an explicit purpose documented in the operative report was not recorded as a central neck dissection (i.e., incidental). Cancer size, histological type, bilaterality, multifocality, extrathyroidal extension (none, microscopic, and gross), margin status, vascular invasion, lymphatic invasion, and central neck nodal disease were studied.
Gross extrathyroidal extension was coded using the operative reports. Staging followed the AJCC 8th edition for DTC; cases previously staged according to the 7th edition were restaged based on review of the pathological findings. Surgical pathology was reported according to the accreditation standards outlined in the College of American Pathologists (CAP) Cancer Protocols. 24 Pathologists examining surgical specimens were not blinded to preoperative MT results because this was a retrospective study. The ATA RSS was used to retrospectively assign patients to RSS-low, RSS-intermediate-, and RSS-high risk categories for recurrence. 1
Statistical analyses
Characteristics of patients with and without recurrence were compared using Student's t-test for continuous variables and the χ 2 -test for association or Fisher's exact test, where appropriate, for proportions. The Kaplan–Meier method and log-rank test were also used to describe recurrence-free survival (RFS).
A multivariable logistic regression model using Firth's bias correction was constructed to determine the association of conventionally available preoperative factors (i.e., age, sex, preoperative levothyroxine use, Bethesda cytology category, and tumor size) with incomplete response to initial intended oncological therapy (Model 1). Additional separate models were constructed to assess the contribution of the RSS categories (Model 2 = Model 1+RSS categories) and the MRGs (Model 3 = Model 1+MRGs) in predicting recurrence.
The predictive ability of the risk models was evaluated with the c-statistic, a measure of discrimination. Model calibration was assessed with the Hosmer–Lemeshow goodness-of-fit test. As another approach to compare the RSS categories with the MRGs, we constructed a fourth model incorporating both RSS categories and MRGs (Model 4 = Model 1+RSS categories+MRGs). SAS OnDemand for Academics: Studio (SAS Institute, Cary, NC) was used. Tests were two-sided and statistical significance was set at the 0.05 level.
Results
Baseline patient characteristics
Among 945 patients who underwent thyroidectomy for cancer with mean age 50.6 years (standard deviation [SD] 16.4), 695 (73.5%) were women and 123 (13.0%) took chronic levothyroxine preoperatively (Table 2). The mean tumor size was 2.5 cm (SD 1.4) and 455 (48.1%) patients had cancers with Bethesda cytology categories V/VI. There were 132 (14.0%) patients who underwent lobectomy followed by completion thyroidectomy (Table 3). There were 195 (20.7%) patients who had central neck dissections and 371 (39.3%) received postoperative RAI as part of their initial oncological therapy.
Preoperative Clinical Characteristics and Their Univariable Associations with Recurrence
SD, standard deviation.
Perioperative and Histopathological Characteristics and Their Univariable Associations with Recurrence
Aggressive histologies include tall cell, insular, columnar cell carcinoma, and hobnail variants.
AJCC, American Joint Committee on Cancer (8th edition); ATA RSS, American Thyroid Association Risk Stratification System; PTC, papillary thyroid carcinoma.
As expected, conventional papillary thyroid cancer (PTC) was the most common cancer type (43.0%) followed by follicular variant of PTC (34.4%). Gross extrathyroidal extension was identified in 44 (4.7%) patients and angioinvasion in 98 (10.4%). There were 840 (88.9%), 100 (10.6%), and 5 (0.5%) patients who had AJCC stage I, II, and III disease, respectively. There were 589 (62.4%), 299 (31.6%), and 57 (6.0%) patients who had RSS-low, -intermediate, and -high cancers, respectively (Table 3).
In the subset of 440 (46.6%) patients who received MT, 381 (86.6%) had MT information available preoperatively. There were 221 (50.2%), 172 (39.1%), and 47 (10.7%) who had MRG-low, -intermediate, and -high cancers, respectively (Table 2). Of those with MRG-high cancers, 9 (19.2%) patients had initial lobectomy followed by completion thyroidectomy.
Recurrence
Over median follow-up of 18 months (IQR 9–30), 50 (5.3%) patients developed a biochemical (n = 18) or structural (n = 32) recurrence. Patients with recurrences had longer median follow-up (22.5 vs. 17 months, p = 0.006). Patients who recurred were more likely to be men (p = 0.02) with larger tumors (p = 0.03). Age (p = 0.89), preoperative levothyroxine use (p = 0.19), and Bethesda cytology category (p = 0.57) were not associated with recurrence (Table 2). As expected, patients who had more extensive operations were more likely to recur, as were those who received RAI (72.0% vs. 37.4%, p < 0.001). Aggressive histological features, such as extrathyroidal extension (p < 0.001) and angioinvasion (p < 0.001), were more often found in cancers that recurred (Table 3). Structural recurrences were identified in the central compartment (n = 13), lateral compartment (n = 12), and distant sites (n = 7).
There were 36 (72.0%) patients who recurred after total thyroidectomy, of which 21 (58.3%) were structural and 15 (41.7%) biochemical. There were 12 (24.0%) patients who recurred after completion thyroidectomy, of which 9 (75.0%) were structural and 3 (25.0%) biochemical. There were two patients who developed structural recurrences after lobectomy. No patients were identified to have a biochemical recurrence after lobectomy alone.
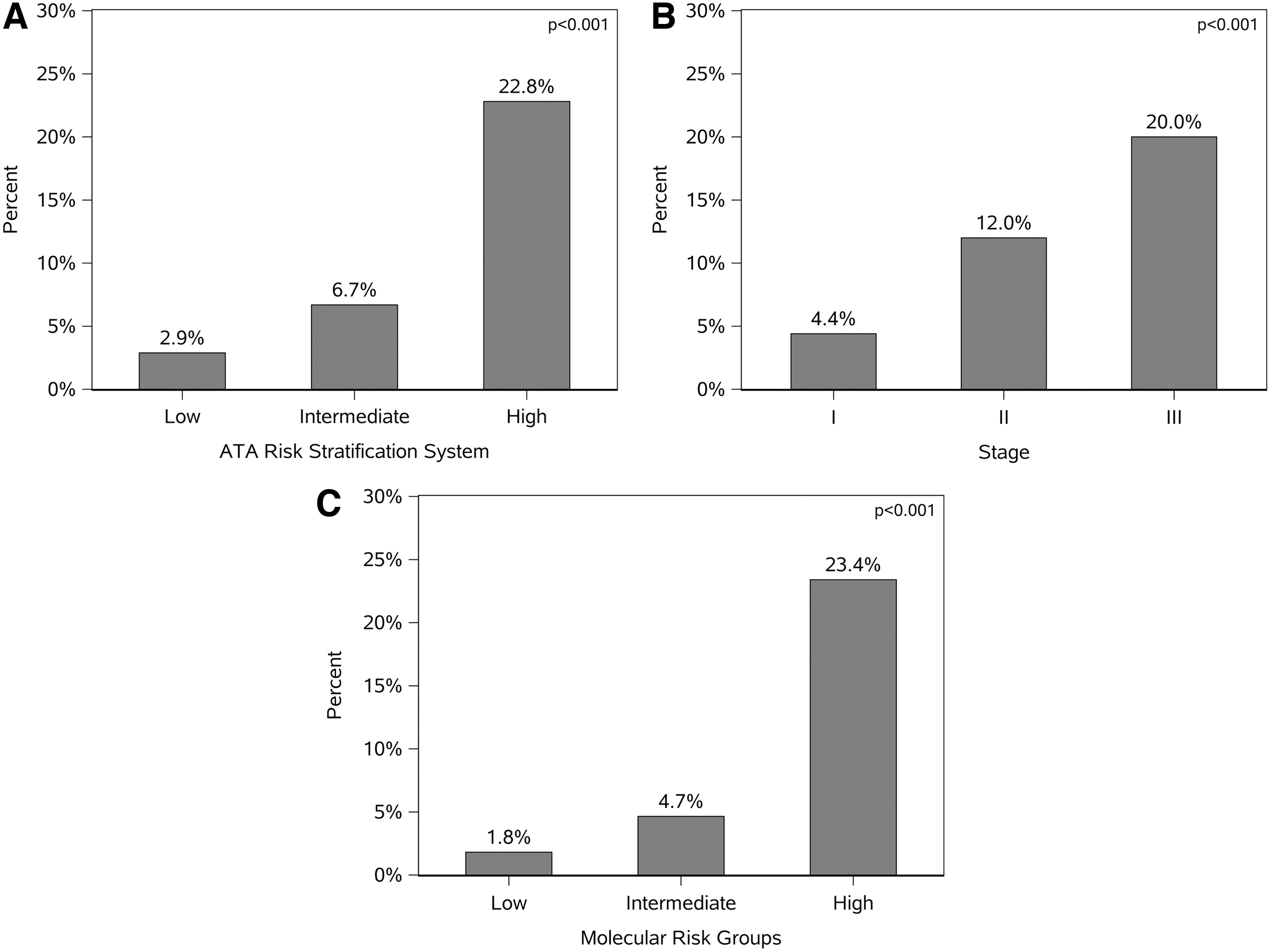
Recurrences were detected in 37 (4.4%), 12 (12.0%), and 1 (20.0%) patient(s) with AJCC stage I, II, and III disease, respectively (Fig. 2A). In the patient with stage III disease, recurrence was structural. Recurrences were detected in 17 (2.9%), 20 (6.7%), and 13 (22.8%) patients with RSS-low, -intermediate, and -high cancers, respectively (Fig. 2B). RSS-high patients recurred as structural in 10 (76.9%) and biochemical in 3 (23.1%). Both AJCC staging and RSS categories were significantly correlated with recurrence in an incremental stepwise manner (p < 0.001 for both).
(
Among patients who had MT (n = 440), recurrences were detected in 4 (1.8%), 8 (4.7%), and 11 (23.4%) patients with MRG-low, -intermediate, and -high cancers, respectively. MRG categories significantly correlated with recurrence in an incremental stepwise manner (p < 0.001; Fig. 2C). All MRG-high cancers had structural recurrence, whereas recurrences within the MRG-low category were predominantly biochemical (Supplementary Fig. S1).
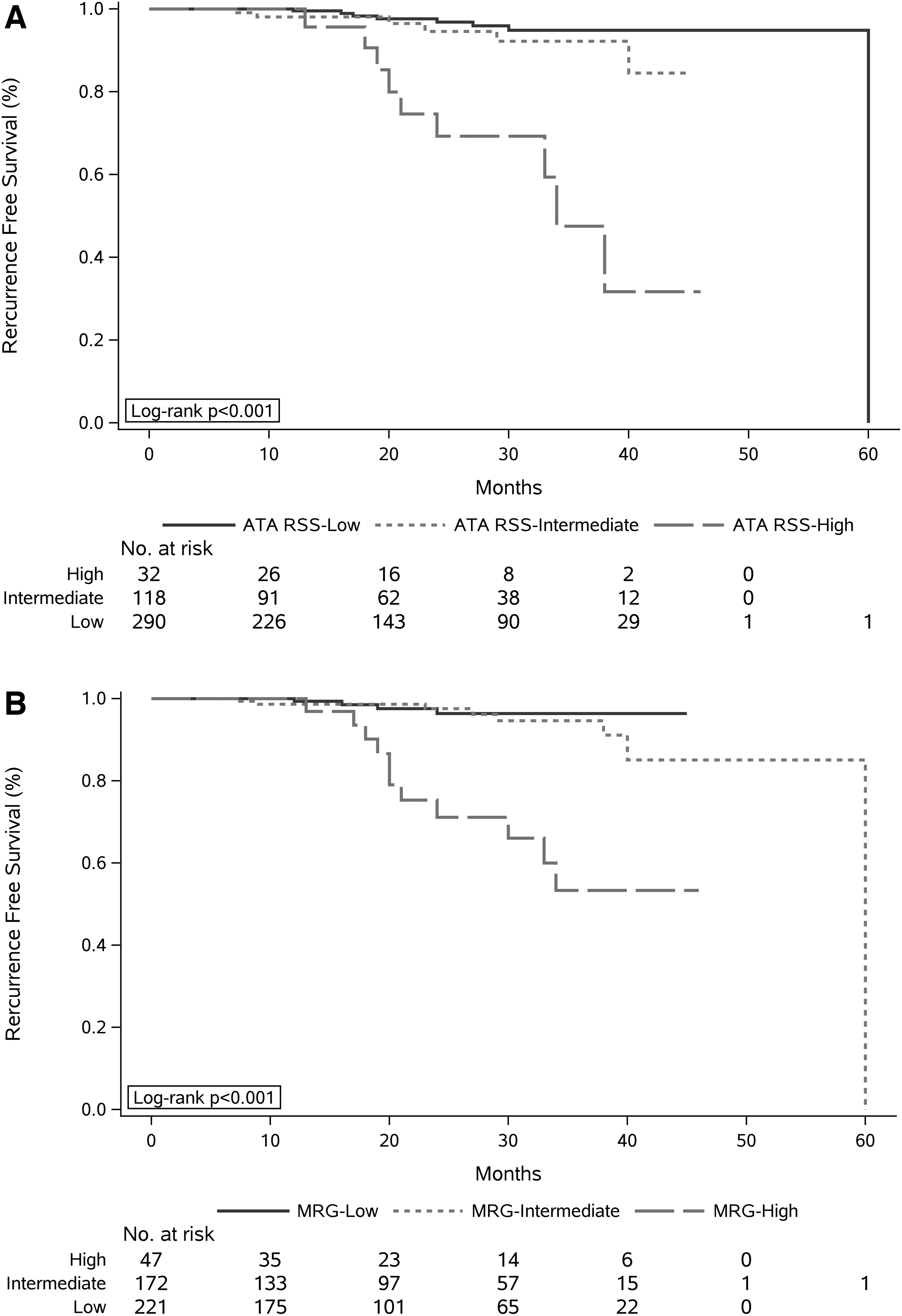
RFS was similar between RSS (Fig. 3A) and MRG (Fig. 3B) categories, suggesting both have similar ability to risk stratify. The 36-month RFS for RSS-high patients was lower than RSS-intermediate patients (47.5% vs. 92.2%, p = 0.004), while the 36-month RFS for RSS-intermediate patients was no different than RSS-low patients (92.2% vs. 94.9%, p = 0.07). The 36-month RFS for MRG-high patients was lower than MRG-intermediate patients (53.4% vs. 91.1%, p < 0.001), while the 36-month RFS for MRG-intermediate patients was no different than MRG-low patients (91.1% vs. 96.4%, p = 0.37).
(
Preoperative prediction modeling
On multivariable analysis incorporating age, sex, preoperative levothyroxine use, Bethesda cytology category, and tumor size (Model 1), only tumor size was significantly associated with incomplete response to initial oncological therapy (odds ratio [OR] 1.3, confidence interval [CI 1.1–1.5], p = 0.003). The c-statistic was 0.64 [CI 0.55–0.72] and calibration was adequate (p = 0.41; Table 4).
Multivariable Modeling Results
Model 1 represents the “base” model of conventionally known preoperative data, including age, sex, preoperative levothyroxine use, Bethesda cytology category, and tumor size in centimeters.
ATA RSS, 2015 ATA Risk Stratification System.
However, when the RSS categories were included with conventional preoperative variables (Model 2), tumor size was no longer associated with recurrence (OR 1.2, [CI 1.0–1.4], p = 0.11) while male sex was (OR 1.9, [CI 1.1–3.4], p = 0.04). RSS-high cancers were associated with four-times the odds of recurrence versus RSS-intermediate cancers (OR 4.1, [CI 1.8–9.2], p < 0.001); and RSS-intermediate cancers were associated with twice the odds of recurrence versus RSS-low cancers (OR 2.2, [CI 1.1–4.4], p < 0.001). The c-statistic was 0.72 [CI 0.65–0.80] and calibration was adequate (p = 0.58; Table 4).
Among the subgroup of 440 patents with MT (Model 3), tumor size was associated with recurrence (OR 1.4 [CI 1.1–1.8], p = 0.005). MRG-high cancers were associated with seven-times the odds of recurrence versus MRG-intermediate cancers (OR 7.2 [CI 2.8–19.5], p < 0.001); and MRG-intermediate cancers were associated with four-times the odds of recurrence versus MRG-low cancers (OR 3.8, [CI 1.3–11.4], p < 0.001). The c-statistic was 0.81 [CI 0.71–0.92] and calibration was adequate (p = 0.52; Table 4). There was no detectable difference in predictive ability between the model incorporating the RSS categories and the model incorporating the MRGs (Model 2 c-statistic 0.72 vs. Model 3 c-statistic 0.81, p = 0.15).
Using another approach to compare the RSS categories with the MRGs, Model 4 was constructed to include both the RSS categories and the MRGs rather than separately (Table 4). Model 4 revealed that older age (OR 0.97 [CI 0.94–0.99], p = 0.02), larger tumor size (OR 1.3 [CI 1.0–1.7], p = 0.03), and MRG category (p = 0.003) were significantly associated with recurrence, while the RSS categories (p = 0.08) were no longer associated with recurrence. The c-statistic was 0.82 [CI 0.72–0.93] and calibration was adequate (p = 0.71).
Discussion
Given that ∼20–30% of thyroid nodules are indeterminate on cytology and that it is currently considered appropriate to perform either a lobectomy or total thyroidectomy for DTCs between 1 and 4 cm, completion thyroidectomy may be necessary based on pathological information. 1,3 –5 With >100,000 thyroidectomies performed annually in the United States, 25 this problem is significant. Knowing which patients in the preoperative setting can be safely triaged to less extensive treatment commensurate with the intrinsic risk for disease recurrence would greatly facilitate high-quality personalized patient-centered care. 26
In this study of 945 patients with histological DTC where we focused on those without lateral neck or distant metastasis based on routine preoperative staging imaging who could be managed with either lobectomy or total thyroidectomy, two-thirds were classified by the existing ATA system as RSS-low risk for recurrence. Even still, incomplete responses were observed across all RSS categories in short-term follow-up. Tumor size was the only conventional preoperative factor associated with recurrence and was associated with a 30% increased risk per centimeter increase in tumor size. After MT results were incorporated in the form of MRGs, model discrimination improved by 27%. This improvement in estimating recurrence risk was not significantly different than when the RSS categories were incorporated, suggesting that the MRGs, which can be known preoperatively, carry predictive capability similar to disease-specific staging characteristics that are typically obtainable only after initial operation.
Numerous prior studies have attempted to identify factors predictive of thyroid cancer recurrence. 27,28 But they all rely on histopathological factors to achieve enough predictive power to be clinically applicable since conventional preoperative factors are limited. We studied only five factors in the preoperative setting as other factors, such as race/ethnicity, body mass index, smoking status, Hashimoto's thyroiditis, personal history of radiation therapy in childhood, or family history of thyroid cancer, have been studied in detail and have not been associated with thyroid cancer recurrence, statistically or conceptually. 29,30 We found that although male sex and tumor size were significantly associated with recurrence only tumor size remained significant in multivariable analyses.
MT results were then examined because it is another preoperative variable that is emerging as a useful prognosticator. Previous studies have reported that specific molecular profiles are associated with key histopathological features linked to disease aggressiveness and recurrence, and, separately, independently with recurrence and distant metastasis. 10,14 –16,22,31 In our prior study examining a cohort inclusive of all DTC with MT information available, we detected an incremental increase in recurrence risk with each MRG category. 22 To expand on this study, we sought to directly compare the ability of the MRGs with the ATA RSS in predicting recurrence among patients eligible for either lobectomy or total thyroidectomy. If the MRGs could be a surrogate for pathological information, knowing the thyroid cancer molecular profile before initiating treatment may help to guide the extent of surgery in particular, among other benefits of this added information.
We observed that the MRGs remained a significant and independent risk factor for recurrence on multivariable analysis even in this more limited patient sample and improved predictive ability beyond tumor size alone. Because the MRGs can be readily known preoperatively, this finding suggests that tumor size and MRGs are two factors that could clarify recurrence risk before any treatment begins, including potentially the extent of surgery. MT thus offers an avenue to inform shared decision-making without relying solely on postoperative data. Similar to earlier studies, 32,33 we confirmed the ability of the RSS categories to predict recurrence, which is the current gold standard method by which thyroid cancer care is delivered.
Moreover, our findings demonstrate that the MRGs are statistically equivalent to the RSS categories in their ability to predict recurrence risk. When we tested this finding by taking another approach to examine the interplay between RSS categories and MRGs by constructing a model that included both RSS categories and MRGs simultaneously (i.e., Model 4), only the MRGs remained significantly associated with recurrence. Taking the findings of Models 2, 3, and 4 together, the MRGs are equally accurate as the RSS categories at predicting recurrence, if not better, within these data. The statistical findings underscore clinical observations that interaction between the MRGs and RSS categories likely exists.
However, until additional validation data are available, the MRGs should not completely replace the gold standard method in routine thyroid cancer care. It is important to stress that testing for a limited number of molecular markers (e.g., BRAFV600E or RAS mutations only) is insufficient for cancer prognostication as it requires knowing the mutational status of multiple genes, including TERT and TP53. However, even when large genetic panels are used, a combination of MT and clinical findings using the armamentarium of available tools (e.g., preoperative imaging and pathological findings) may provide the most comprehensive prediction of recurrence to improve care. As another tool, comprehensive MT results may potentially move the ability to risk stratify to a timepoint before any treatment begins.
We observed a 13–14% rate of requiring completion thyroidectomy in this cohort. While this is lower than the theoretical rate of 40–50% assessed in retrospective studies, this rate is consistent with the reported completion thyroidectomy rate of 12–25% after publication of the 2015 ATA Guidelines. 3 –5,34,35 Reasons to proceed with a completion thyroidectomy are not always apparent in review of medical records, which can include patient preference, clinician preference, or oncological considerations. Further prospective studies are needed to better understand the molecular, patient-specific, and cancer-related variables that would possibly allow further reduction in the need for completion thyroidectomy.
This investigation has several additional limitations. First, as a retrospective study, selection bias is probable and additional unknown preoperative factors predictive of recurrence may exist. For example, ultrasound characteristics were excluded because results were not uniformly reported during the study period and the ability of ultrasonography to provide reliable prognosticative discrimination between low- and intermediate-risk disease is variable. 17 –19 In addition, we did not include socioeconomic variables in the assessment although this would be important to consider for future analyses.
Second, this study was conducted at a single high-volume institution in the United States thus possibly limiting generalizability. A split-sample internal validation approach was not taken due to the small sample size of our study and would not have improved our ability to answer the study question. Indeed, it is important to recognize that the statistical ability of the RSS categories and MRGs to correctly categorize patients with and without recurrence is limited to this patient cohort. Larger sample sizes, other settings, or longer follow-up may alter these findings and explain why there is not a greater separation in RFS between the intermediate- and low-risk groups within both the RSS categories and MRGs. Future multi-institutional studies are certainly needed to externally validate findings.
Third, pathologists were not blinded to MT results, when present. Nevertheless, pathologists followed CAP standards when evaluating surgical specimens. 24 Fourth, we could not ascertain whether MT results factored into the decision-making for completion thyroidectomy in these patients or how MT informed the initial extent of surgery. Fifth, patients who recurred were followed for longer and thus the true recurrence rate may be underestimated. Patients with low-risk tumor features were possibly monitored less intensely resulting in incomplete capture of follow-up.
Last, overall follow-up was short and thus biochemical recurrences were included, which accounted for a significant proportion (36%) of the overall recurrences in this study. Biochemical recurrences may never result in actionable recurrences and thus recurrence may be overestimated. Longer follow-up of this cohort is needed.
Conclusions
In this retrospective cohort study, MT results improved preoperative risk prediction beyond the single conventional preoperative factor of tumor size. Furthermore, the predictive ability of the MRGs was similar to the RSS categories, suggesting that the MRGs could be a valuable surrogate for histology to accurately inform prognosis.
Footnotes
Authors' Contributions
Conceptualization (equal), methodology (lead), software (lead), validation (equal), formal analysis (lead), investigation (lead), data curation (lead), writing—original draft (lead), and visualization (lead) by J.B.L. Validation (equal) and writing—review and editing (equal) by K.A.B. Conceptualization (equal), validation (equal), resources (equal), and writing—review and editing (equal) by K.R. and K.L.M. Resources (equal) and writing—review and editing (equal) by E.K.-F., E.M.M., and N.P.O. Conceptualization (equal), methodology (equal), validation (equal), resources (equal), writing—review and editing (equal), and supervision (equal) by M.N.N., Y.E.N., and S.E.C. Conceptualization (lead), methodology (equal), validation (equal), resources (lead), writing—review and editing (lead), and supervision (lead) by L.Y.
Author Disclosure Statement
M.N.N. and Y.E.N. own intellectual property related to ThyroSeq® and receive royalties through the University of Pittsburgh; they also serve as consultants for Sonic Healthcare USA. All other authors have no conflicts of interest to report.
Funding Information
There was no specific funding for this study. S.E.C. was supported by a generous gift from the William and Susan Johnson Fund for Endocrine Surgery Research for work unrelated to this.
Supplementary Material
Supplementary Figure S1