
Abstract
Background:
The frequency and factors associated with thyroid hormone replacement therapy among patients with subclinical hypothyroidism (SCH) remain uncertain.
Methods:
In this electronic health records-based observational cohort study, we included adults diagnosed with SCH from four academic centers (the United States and Mexico) from January 1, 2016, to December 31, 2018. We aimed to identify the determinants of thyroid hormone replacement therapy for SCH and the frequency of treated SCH.
Results:
A total of 796 patients (65.2% women) had SCH, and 165 (20.7%) were treated with thyroid hormone replacement therapy. The treated group was younger [51.0 (standard deviation {SD} 18.3) vs. 55.3 (SD 18.2) years, p = 0.008] and had a higher proportion of women (72.7% vs. 63.2%, p = 0.03) compared with the untreated group. Only 46.7% of patients in the treated group and 65.6% in the untreated group had confirmatory thyroid function tests (TFTs) before the decision to start thyroid hormone replacement therapy was made. There was no difference in the frequency of thyroid autoimmunity evaluation, but a positive thyroid autoimmunity test was more frequent in the treated group compared with the untreated group (48.2% vs. 20.3%, p < 0.001). In a multivariable logistic regression model, female sex (odds ratio [OR] = 1.71 [CI 1.13–2.59], p = 0.01) and index thyrotropin (TSH) level (OR = 1.97 [CI 1.56–2.49], p < 0.001 for every SD [2.75 mIU/L] change) were associated with higher odds of treatment.
Conclusions:
Among patients with SCH, female sex and index TSH level were associated with higher odds of treatment. Moreover, in our population, the decision to treat or not to treat SCH was often based on only one set of abnormal TFTs, and thyroid autoimmunity assessment was underused.
Introduction
Subclinical hypothyroidism (SCH) is a common diagnosis based on biochemical data: an elevated serum thyrotropin (TSH) level in combination with a free thyroxine (fT4) level within the normal reference range. 1,2 SCH affects up to 15% of the adult population and roughly more than one billion adults worldwide. 3 –5 Many symptoms have been linked to SCH; however, most are not specific (e.g., fatigue), and around 30% of patients with SCH have no symptoms. 4,6 –8
Levothyroxine (LT4) is the mainstay of treatment for hypothyroidism. 1,9,10 LT4 use has significantly increased over the last few decades, 11 and it has become one of the most prescribed drugs for adults in the United States, 12,13 despite the relatively low prevalence and stable incidence of overt hypothyroidism in the general population. 3,14 –16 Although it is unclear what is driving the surge in LT4 prescriptions in the United States, it has been described that one of the main factors could be an increase in the diagnosis and treatment of SCH. 17 –19 There is evidence for potential overtreatment of patients with SCH causing a substantial and unnecessary economic and treatment burden 17,20,21 despite inconsistent benefits. 22 –32 Indeed, in a recent clinical guideline, 33 the panel concluded that almost all adults with SCH would not benefit from thyroid hormone treatment based on randomized clinical trials that showed a lack of benefit in patient-important outcomes. Instead, it was recommended that clinicians should monitor the progression or resolution of the thyroid dysfunction in these adults. 33
On the contrary, most of the previous guidelines recommend treatment with LT4 for patients with SCH based on specific criteria, such as TSH level, patient's age, the presence of hypothyroidism-related symptoms, positive thyroid autoantibodies, or evidence of cardiovascular disease. 1,9
To better understand the appropriateness of LT4 use among patients with SCH and to propose strategies to attenuate overdiagnosis and overtreatment of SCH, it is necessary to examine the frequency of and factors associated with LT4 use in patients with SCH. We performed a multicenter electronic health records-based observational cohort study to identify patients' and clinicians' determinants of thyroid hormone replacement therapy for SCH and the proportion of SCH patients treated with thyroid hormone replacement therapy.
Methods
Study design, setting, and patient population
In this electronic health records-based observational cohort study, we included eligible patients from four academic centers: University of Arkansas for Medical Sciences (UAMS) (Little Rock, AR, USA), Mayo Clinic (Rochester, MN, USA), University of Florida (UF) (Gainesville, FL, USA), and Universidad Autonoma de Nuevo Leon (UANL) (Monterrey, Mexico). The study was approved by each academic center's Institutional Review Board (IRB) (Mayo Clinic IRB, study ID no. 19-007744; UAMS IRB, study ID no. 249970; UF IRB, study ID no. 201902544; UANL IRB, study ID not applicable, approval date: February 20, 2020). Each IRB waived the need for informed patient consent, and individual data transfer/use agreements were obtained.
We included adults ≥18 years old, diagnosed with SCH (at least one set of elevated TSH and normal fT4 or total thyroxine (TT4) during the study period; the first instance of high TSH was considered “index TSH” and used for evaluation) from January 1, 2016, to December 31, 2018. The diagnosis of SCH was based on each institution's reference range for TSH and fT4/TT4. Patients who were pregnant, postpartum, severely ill, had a recent hospitalization (within 4 weeks before index TSH), using thyroid-affecting medications (amiodarone, lithium, and tyrosine kinase inhibitors) or using medications for weight loss, with transient hypothyroidism (e.g., acute or subacute thyroiditis), and a history of thyroidectomy, radioactive iodine therapy, or neck radiation were excluded from this study. Severe illness was defined as any acute illness that required hospital admission to the medical ward/intensive care unit.
Data collection
Electronic medical records from the included participants were reviewed, and sociodemographic data, thyroid function tests (TFTs) with dates and values, thyroid peroxidase antibody (TPOAb) status, thyroid ultrasound findings, and factors documented in the clinicians' notes that could influence their decision to treat SCH such as symptoms, comorbidities, family history of thyroid disorders, physical examination findings, and patients' preference/desire for treatment were extracted. We defined thyroid autoimmunity as the presence of positive TPOAbs according to each institution's assay-specific cutoff values. The presence/absence of symptoms was manually extracted from the information documented in each individual patient's medical records, especially from the data reported in the chief complaint, history of present illness, and review of system sections of their charts. Relevant comorbidities were extracted directly from the medical history data included in the chart at the time when the treatment decision was made.
Data related to thyroid hormone replacement therapy, such as confirmation of SCH with a second set of TFTs before thyroid hormone replacement therapy prescription, the timing of therapy in relation to index abnormal TFTs, type and initial dose of thyroid hormone replacement therapy, justification for prescription (documented in patient's chart assessment/plan section), and clinicians' characteristics (specialty, type of clinician) were also retrieved. All the data were extracted using a standardized data extraction sheet in a secure, Health Insurance Portability and Accountability Act-compliant web-based application designed for data collection for research studies (Research Electronic Data Capture). We had multiple meetings to ensure standardization of the data-gathering process. Quality checks were performed to ensure data accuracy and plausibility.
Statistical analyses
Our primary outcome was to identify the determinants of thyroid hormone replacement prescription for SCH. Secondary outcomes were to estimate the frequency of SCH treated with thyroid hormone replacement and factors associated with thyroid function confirmatory testing.
A descriptive summary analysis of patients' baseline characteristics was performed stratified by treatment status. Data are presented as frequencies (percentages) for the categorical variables and means (standard deviation [SD]) for the continuous variables. Differences between categorical variables were assessed using the Fisher's exact test and between continuous variables using the Welch's two-sample t-test.
For our primary outcome, an initial multivariable logistic regression analysis with the most clinically relevant variables and those that were significantly different among the treatment groups (age, sex, presence of any thyroid symptoms, history of arrhythmias, history of osteoporosis, history of cardiovascular disease, index TSH level, and fT4 level) was developed (model 1). Then, we added two additional clinically relevant variables, which had a significant percentage of missing data (thyroid autoimmunity and abnormal thyroid examination) to the model with multilevel multiple imputations for missing data 34 (model 2). Five imputed data sets were created and pooled for analyses using Rubin's rules. 35 Finally, a multivariable logistic regression model including thyroid-related symptoms as the only predictors (only symptoms reported by ≥30 patients were included) was performed to assess for individual symptoms as potential drivers of thyroid hormone replacement therapy (model 3).
For our secondary outcomes, we calculated the proportion of patients who received thyroid hormone replacement therapy. Univariable logistic regressions were performed to examine the factors associated with confirmatory TFTs within 90 days of the index TSH and to examine the factors associated with thyroid hormone replacement therapy in the entire population. A sensitivity analysis for the assessment of factors associated with confirmatory TFTs was performed after excluding patients with SCH diagnosis in 2016 (to exclude patients who might have had previous, not captured by our study design, abnormal TFT laboratory data before January 2016).
We completed a subgroup analysis including only the subset of patients who received confirmatory testing within 90 days after the index TSH. In this subgroup, we performed a univariable logistic regression to examine the factors associated with thyroid hormone replacement therapy and a multivariable logistic regression model to examine the factors associated with thyroid hormone replacement therapy, which was simultaneously adjusted for age, sex, any thyroid-related symptoms, index TSH level, and confirmatory TSH level.
For those univariable analyses with multiple comparisons, we applied Bonferroni corrections. For the multivariable models, we assessed collinearity on the fit of the model using variance inflation factors with a threshold of 4.0 to indicate that collinearity may be negatively affecting model estimates. Results of the univariable and multivariable logistic regressions are reported as odds ratios (ORs) and 95% confidence interval (CI). A p of <0.05 was considered statistically significant and all testing was 2-sided. All statistical analyses were performed using R 4.1, 36 and multiple imputation was performed using the R package mice. 37
Results
Sociodemographic, clinical, and treatment characteristics
A total of 796 patients with SCH were included from the four participating institutions (Mayo Clinic, n = 273; UAMS, n = 194; UANL, n = 63; UF, n = 266). Of those, 65.2% were women, 75.9% were white, 87.3% non-Hispanic, and the population mean age (SD) was 54.4 (18.3) years. Overall, 165 patients diagnosed with SCH (20.7%) were treated with thyroid hormone replacement therapy. LT4 was prescribed in all but one of the cases (99.4%), in which desiccated thyroid extract was prescribed. Initial LT4 dose ranged from 12.5 to 137 μg/day (interquartile range = 25–50 μg/day). The treated group was younger (mean age [SD]; 51.0 [18.3] vs. 55.3 [18.2] years, p = 0.008) and had a higher proportion of women (72.7% vs. 63.2%, p = 0.03) compared with the untreated group.
The treated group had a different composition in terms of employment status when compared with the untreated group (p = 0.01), with a higher number of employed patients (54.7% vs. 39.9%) and a lower number of retired patients (21.1% vs. 34.2%). A family history of thyroid disorders was more frequently found in the treated group compared with the untreated group (29.8% vs. 14.7%, p = 0.0008). The treated group had more patients with weight gain (20.6% vs. 11.3%, p = 0.047) and fatigue (40.6% vs. 25.7%, p = 0.002) compared with the untreated group. No differences were found in other hypothyroidism-related symptoms among treated and untreated patients, such as cold intolerance, depression, constipation, dry skin, hair loss, menstrual abnormalities, and musculoskeletal or cognitive issues (Supplementary Table S1). Additional sociodemographic characteristics, physical examination findings, and comorbidities by treatment groups are displayed in Tables 1 and 2, and Supplementary Table S2, respectively. A summary flowchart including treatment status and confirmatory testing is presented in Figure 1.
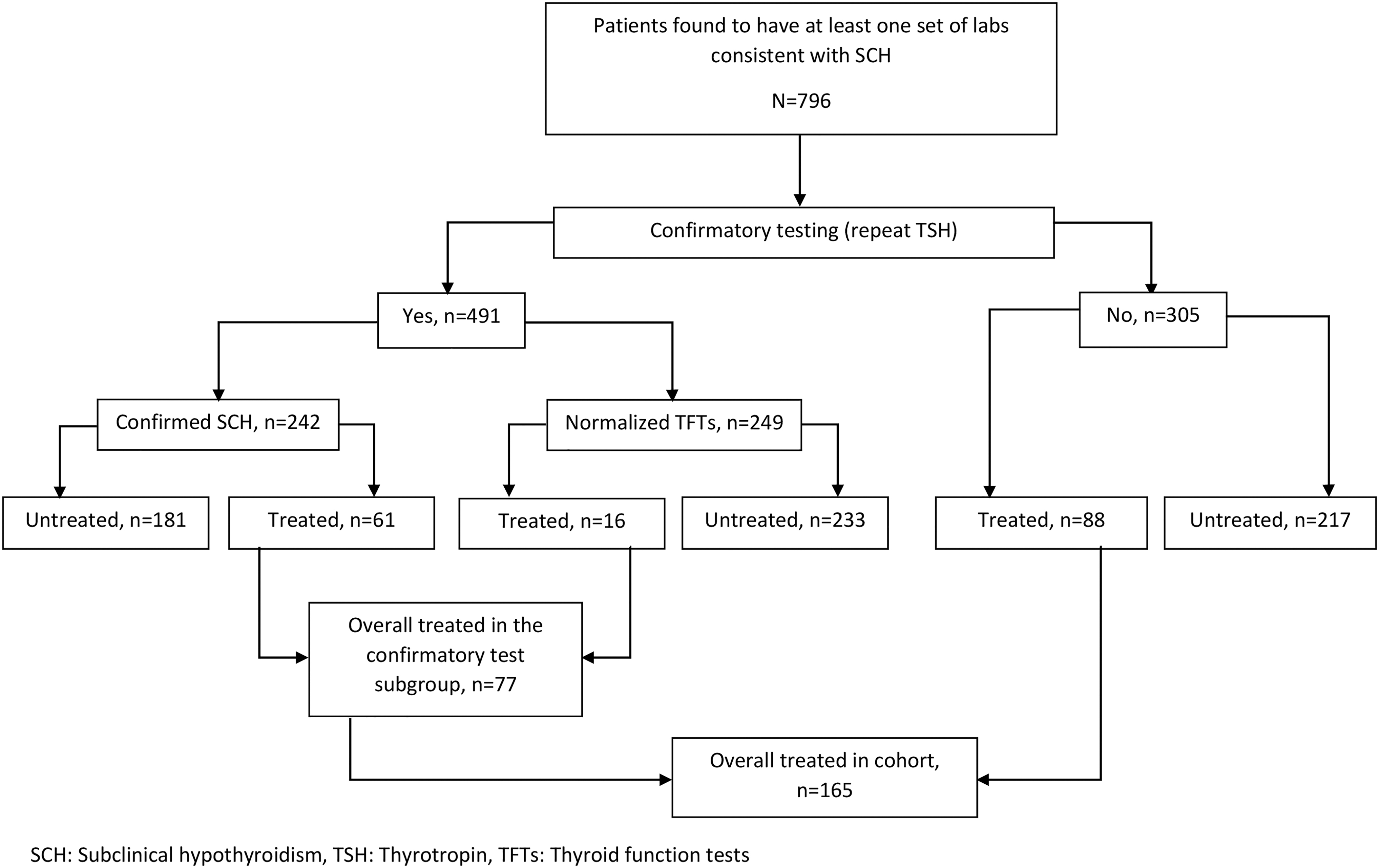
Flowchart summarizing treatment status and confirmatory testing in patients with SCH. SCH, subclinical hypothyroidism; TFTs, thyroid function tests; TSH, thyrotropin.
Demographic and Social Characteristics per Treatment Group
Two-sample t-test p-value.
White versus other races.
FET, Fisher's exact test; GED, graduate equivalency degree; SD, standard deviation.
Clinical and Biochemical Characteristics per Treatment Group
Welch's two-sample t-test.
Fisher's exact test.
BMI, body mass index; fT4, free thyroxine; TSH, thyrotropin.
Biochemical data
The treated group had a higher index TSH level (mean [SD], 7.6 [5.0] mIU/L vs. 6.0 [1.6] mIU/L, p < 0.001) and a higher proportion of TSH level ≥10 mIU/L (11.5% vs. 3.2%, p < 0.001) compared with the untreated group. There was a linear relationship between index TSH and the proportion of patients prescribed LT4 (Supplementary Fig. S1). The treated group had a slightly lower fT4 level (mean [SD], 1.0 [0.2] vs. 1.1 [0.2], p = 0.03) compared with the untreated group. There was no difference in the frequency that thyroid autoimmunity was assessed (33.9% vs. 32.8%, p = 0.78); however, a positive thyroid autoimmunity test was more frequent in the treated group compared with the untreated group (48.2% vs. 20.3%, p < 0.001). A summary of the biochemical data per treatment group is presented in Table 2.
Confirmatory thyroid evaluation
Only 46.7% (77/165) of the patients in the treated group and 65.6% (414/631) of the patients in the untreated group had confirmatory TFTs before the decision to start thyroid hormone replacement therapy was made (Fig. 1). When repeat TFTs were obtained, TSH levels normalized in 50.7% (249/491) patients, and of those, 6.4% (16/249) were treated, and 93.6% (233/249) remained untreated (Fig. 1). Of those patients with repeat TFTs, SCH was confirmed in 79.2% (61/77) of treated patients and 43.7% (181/414) of the untreated patients (Fig. 1). A sensitivity analysis excluding the patients with SCH diagnosis in 2016 (since previous thyroid laboratories were not captured) showed similar results regarding confirmatory thyroid evaluation. A total of 250 patients had confirmatory TFTs done within the first 90 days after index TSH. Characteristics associated with confirmatory testing done within the first 90 days after index TSH are presented in Supplementary Table S3.
Clinician characteristics
More patients whose index TSH testing was ordered by a physician's assistant/nurse practitioner were subsequently treated compared with physicians (28.6% vs. 19.2%, p = 0.02). The main justification for prescribing thyroid hormone replacement therapy was abnormal TFTs (69.1%), followed by presenting symptoms at diagnosis (44.8%), unknown (11.5%), increased cardiovascular risk (4.2%), patient choice (4.2%), pregnancy desire (3.6%), and other (3.6%). On the contrary, the main justification for not prescribing thyroid hormone replacement therapy included normalization of TFTs (35.8%), asymptomatic presentation (27.6%), other reason (25.8%), unknown (19.5%), elderly age (4.3%), and patient preference (2.2%).
Determinants of thyroid hormone replacement therapy
In the model 1, which examined factors associated with the prescription of thyroid hormone replacement therapy, female sex (OR = 1.71 [CI 1.13–2.59], p = 0.01) and index TSH level as a continuous variable (OR = 1.97 [CI 1.56–2.49], p < 0.001; for every SD [2.75 mIU/L] change) were associated with higher odds of treatment (Table 3). Similar results were seen with the model 2 after including thyroid autoimmunity positivity and abnormal thyroid examination (Supplementary Table S4). In addition, in the model 3, which included individual thyroid-related symptoms as the only predictors, fatigue (OR = 1.84 [CI 1.24–2.73], p = 0.002) and weight gain (OR = 1.70 [CI 1.06–2.74], p = 0.03) were associated with higher odds of thyroid hormone replacement therapy prescription (Supplementary Table S5).
Multivariable Logistic Regression Model Examining Factors and Covariates Associated with Thyroid Hormone Replacement Therapy (Model 1)
CI, confidence interval; OR, odds ratio.
Subgroup analysis: determinants of thyroid hormone replacement in patients with confirmatory testing
When only the subset of patients who received confirmatory TFTs within 90 days after the index TSH was analyzed, univariable logistic regression analyses showed that age >65 years was associated with lower odds of treatment (OR = 0.49 [CI 0.24–0.98], p = 0.05), while family history of thyroid disease (OR = 2.60 [CI 1.16–5.85], p = 0.02), positive thyroid autoimmunity (OR = 3.75 [CI 1.39–10.09], p = 0.009), index TSH level (OR = 1.77 [CI 1.19–2.62], p = 0.005), and confirmatory TSH level (OR = 2.42 [CI 1.69–3.48], p < 0.001) were associated with higher odds of treatment (Table 4).
Factors Associated with Thyroid Hormone Replacement Therapy in the Subset of Patients Having a Confirmation Thyrotropin Performed Within 90 Days of Their Index Thyrotropin
The n/N column is presented to gauge how missing data may affect the analysis. For this analysis, subjects with a confirmation TSH occurring more than 90 days from their index TSH were excluded. ORs and corresponding CI were extracted from univariable logistic regression analyses.
Moreover, in a multivariable logistic regression model simultaneously adjusting for age, sex, any thyroid-related symptoms, index TSH level, and confirmatory TSH level, the only factor associated with the prescription of thyroid hormone replacement therapy was the confirmatory TSH level (OR = 2.46 [CI 1.64–3.68], p < 0.001) (Supplementary Table S6) in the subset of patients who received a confirmatory TSH test within 90 days after the index TSH was analyzed. Sex-specific data (demographics and social characteristics, reported SCH symptoms, comorbidities, and other medical- and treatment-related characteristics of the studied population) are presented in the Supplementary Tables S7 to S10. The definitions used for the comorbidities of interest are presented in Supplementary Table S11.
Discussion
In this multicenter cohort study, approximately one of every five patients with SCH was treated with thyroid hormone replacement therapy. Interestingly, only 46.7% of the patients in the treated group and 65.6% of the patients in the untreated group had confirmatory TFTs before the decision to start thyroid hormone replacement therapy was made. Thyroid autoimmunity was checked in about one of every three patients in both groups; however, a positive thyroid autoimmunity test was more frequent in the treated group compared with the untreated group. In the multivariable analysis, female sex and index TSH level were associated with higher odds of treatment.
We described a lower prevalence of treated SCH (20.7%) compared with the only study, 38 to the best of our knowledge, describing the prevalence of treated SCH from an unselected adult population in the United States. In 2003, Fatourechi et al. 38 retrieved data from medical records of patients with TSH levels between 5.1 and 10.0 mIU/L and reported that LT4 therapy was prescribed for 39% of these patients. However, this study analyzed a subsample (n = 450) of the entire initial population (n = 2655) after computer-based random selection according to their thyroid antibody status with ratios of ∼2:2:1 (positive = 43.8%, negative = 40.7%, and not checked = 15.5%), which differs from our study population (positive = 8.7%, negative = 24.4% and not checked = 66.9%).
Fatourechi et al. 38 also explored factors that influence clinicians' decisions to treat SCH, and similarly to our findings, they described that treated individuals were younger, had a higher proportion of women, higher TSH levels, and a higher proportion of positive thyroid microsomal antibodies compared with the untreated group. Women are more frequently diagnosed with and treated for thyroid disorders than men. 3,5,39 This finding could be explained by a perceived increased risk of progression to overt hypothyroidism 15,40 or due to the potential treatment benefit on reproductive outcomes. 41
In our population, the treated group showed significantly higher TSH levels when compared with the untreated group (mean [SD], 7.6 [5.0] mIU/L vs. 6.0 [1.6] mIU/L, p < 0.001). This finding is probably explained by a higher probability of treating patients with higher TSH levels, as we have described, especially if TSH levels are above 7–10 mIU/L as recommended by current guidelines. The European Thyroid Association (ETA) guidelines and the American Association of Clinical Endocrinologists/the American Thyroid Association cosponsored guidelines recommend thyroid hormone replacement therapy for patients with serum TSH >10 mIU/L. 1,9 In addition, the proposed treatment approach in UpToDate recommends that most patients younger than 65–70 years with TSH 7.0 mIU/L or higher should be treated, given the report of increased cardiovascular mortality in this population. 42 However, it is important to consider that although we found a significant difference in the TSH level by treatment groups, this difference might be too small to be clinically significant.
Most patients with SCH are asymptomatic, and when symptoms are present, they tend to be nonspecific, such as weight gain, fatigue, dry skin, and constipation. 6,43 –46 Indeed, patients with SCH did not report a higher hypothyroidism symptom score compared with euthyroid controls in a Danish population-based study. 47 We described that weight gain and fatigue were more frequent in SCH patients who received thyroid hormone replacement compared with untreated individuals. As these symptoms are common and bothersome complaints of adults in the outpatient setting, we suspect that when they are present in conjunction with SCH and in the absence of other possible explanatory etiologies, thyroid hormone replacement is likely prescribed as a therapeutic trial to obtain any potential benefit and with follow up to assess its response.
On the contrary, individuals with SCH and a known family history of thyroid disorders or the presence of goiter on physical examination are frequently treated in clinical practice given their association of these factors with the development of thyroid disorders, 48,49 and the evidence of thyroid volume reduction when treated with LT4. 50
Interestingly, contrary to what is recommended by some guidelines, less than half of the treated individuals had confirmatory TFTs before the decision to start thyroid hormone replacement therapy. The ETA guidelines recommend that an initially raised serum TSH with fT4 within the reference range should be investigated with a repeat measurement of both serum TSH and fT4, along with TPOAbs, preferably after a 2- to 3-month interval. 1 Similarly, the proposed diagnostic approach in UpToDate recommends that if the serum TSH level is elevated, the TSH measurement should be repeated along with a serum fT4 after 1–3 months before diagnosing SCH. 42 The low frequency of confirmatory TFTs occurred despite the strong evidence showing that TSH values normalize without intervention for most adults 39,51 –54 and recent data suggesting that even when LT4 is initiated, up to a third of patients remained euthyroid after LT4 discontinuation, especially those with SCH. 55
When repeat TFTs were obtained, around 50% normalized, likely impacting the decision to start thyroid hormone replacement therapy and avoiding unnecessary treatment. However, we also found that of the 77 treated patients who had confirmatory testing done, around 20% were treated despite the normalization of their TFTs.
Thyroid autoimmunity is another factor frequently assessed when thyroid hormone replacement therapy is considered in the setting of SCH, as the risk of progression from SCH to overt hypothyroidism is related to the presence of TPOAb. 40,56 –59 In this study, thyroid autoimmunity was checked only in one-third of the individuals in both the treated and untreated groups, suggesting that there is potential underuse of this diagnostic aid in the decision-making process in some instances. Most of the guidelines recommend that TPOAb measurements should be considered when evaluating patients with SCH 1,9 ; however, the proposed diagnostic approach in UpToDate does not recommend routine measurement of thyroid antibodies in patients with SCH; instead, they recommended checking when the decision to treat or to monitor is not obvious. 42
Importantly, there is overuse of LT4 as evidenced by frequent initiation of LT4 for patients with SCH in a study analyzing the use of LT4 in the United States for commercially insured and Medicare Advantage enrollees from 2008 to 2018. 19 In addition, Taylor et al. found that the median TSH level at initiating LT4 therapy fell from 8.7 to 7.9 mIU/L from 2001 to 2009 in the United Kingdom, suggesting a more frequent use of LT4 for marginal/mild degrees of hypothyroidism, such as SCH. 60 Our findings have implications for clinicians managing thyroid hormone replacement therapy and their patients with SCH. It is necessary to highlight the importance of a repeat set of TFTs, usually after 1–3 months, to confirm the SCH diagnosis, as we identified that clinicians often decide whether to treat or not to treat SCH based on only one set of abnormal TFTs. In addition, there is an opportunity to increase thyroid autoimmunity assessment as a diagnostic aid in decision-making in some instances. Therefore, adopting those two strategies can potentially reduce the overdiagnosis and overtreatment of patients with SCH and ameliorate the impact and harm of exposing some patients with SCH to long-term thyroid hormone replacement therapy.
Our study has several limitations, including the inability to explore if those patients who entered the cohort at the beginning of the study period had their TFTs checked previously, the potential of selection bias (all four institutions were academic centers), by which the study population may not be truly representative of the general population, and the inability to control for other potential confounder factors. There are also inherent limitations due to the nature of our study; for example, the use of data from electronic health records may have lower accuracy than data collected from prospective cohorts, especially for the data that rely entirely on the effort/time of the clinician's documentation in the chart (e.g., symptoms, patient preferences), as well as the missing or unclear data in the electronic health records needing clarification that we were unable to include in the analyses.
On the contrary, our study has several strengths, including a diverse group of participants from four different populations, a relatively large sample size, which enabled us to assess for multiple covariables, the description of the prevalence of treated SCH, and the inclusion of clinicians' characteristics and justifications for treatment with thyroid hormone replacement in the setting of SCH.
This study described a comprehensive assessment of frequency and determinants for thyroid hormone replacement therapy in adults with SCH. Among patients with SCH, female sex and index TSH level were associated with higher odds of treatment. Moreover, in our population, the decision to treat or not to treat SCH was often based on only one set of abnormal TFTs, and thyroid autoimmunity assessment was underused. Further studies are needed to evaluate the appropriateness of thyroid hormone replacement therapy and whether those factors are associated with SCH overtreatment or can identify patients who might benefit from treatment.
Footnotes
Acknowledgments
Data necessary for the conception of this study were provided by the Arkansas Clinical Data Repository and maintained by the Department of Biomedical Informatics in the College of Medicine at the UAMS. We also acknowledge the UF Integrated Data Repository and the UF Health Office of the Chief Data Officer for providing the analytic data set for this project. This material is the result of work supported with resources and the use of facilities at the Central Arkansas Veterans Healthcare System, Little Rock, AR. Three abstracts containing data from this study were presented at the 90th Annual Meeting of the American Thyroid Association.
Authors' Contributions
S.M., J.P.B., N.M.S.O., and R.R.G. conceived and designed the study with input from all the coauthors. H.J.S. performed the statistical analyses with input from S.M., J.P.B., N.M.S.O., R.R.G., and F.J.K.T. F.J.K.T., O.M.E.K., S.E.M., A.G., A.G., N.M., S.M., S.V., and M.B. carried out the data collection with input from S.M., J.P.B., N.M.S.O., and R.R.G. All the coauthors contributed to critically appraising and reviewing the results and the article. All the authors reviewed and agreed on the final version of the article.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, Department of Veterans Affairs, or the U.S. Government.
Data Availability
The data sets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
No competing financial interests exist. The authors had financial support for the submitted work as specified in the funding section, but the funding institutions did not have any role in the writing of the article or the decision to submit it for publication; no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work.
Funding Information
N.M.S.O. was supported by the National Cancer Institute of the National Institutes of Health under Award Number K08CA248972. S.M. was supported by the Arkansas Biosciences Institute, the major research component of the Arkansas Tobacco Settlement Proceeds Act of 2000, and by the U.S. Department of Veterans Affairs Health Services Research and Development Service of the VA Office of Research and Development, under Merit review award number 1I21HX003268-01A1. Research reported in this publication was supported, in part, by the National Center for Advancing Translational Sciences of the National Institutes of Health under awards UL1 TR003107, UL1 TR000064, and UL1 TR001427.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Table S9
Supplementary Table S10
Supplementary Table S11