
Abstract
Background:
To gain maximum therapeutic effect while minimizing side effects, it is imperative for patients with hypothyroidism to use their levothyroxine (LT4) correctly, such as adhering to the prescribed regimen. Little is currently known about how patients actually use LT4 in real life. We investigated the use of LT4, as well as the thyroid health (thyrotropin [TSH] and health-related quality of life [HR-QoL]), and evaluated if proper LT4 use is associated with better thyroid health.
Methods:
A cross-sectional observational study was conducted in a Belgian community sample of adults using LT4 for hypothyroidism since ≥2 years. Participants completed a self-administered questionnaire on patient characteristics, self-reported adherence to LT4, timing of intake, and co-medication. They also completed the thyroid-specific patient-reported outcome (ThyPRO-39) questionnaire, measuring the HR-QoL. Pharmacy dispensing data were used to calculate the medication possession ratio (MPR).
Results:
We included 856 participants (mean age 61.4 ± 14.3 years, 86% [740/856] females). Approximately one in four participants (138/563) had out-of-range TSH levels. Generally, ThyPRO-39 scores were in the lower part of the range (indicating better HR-QoL), with the scales “emotional susceptibility” and “tiredness” showing the worst scores. Approximately 28% (178/632) of the participants were classified as non-adherent (MPR <80%), corresponding to at least 73 cumulative days per year without LT4 intake. Twenty-five percent (212/854) of participants self-reported non-adherence, with unintentional non-adherence (forgetfulness) most frequently reported (21.9%, 187/854). Only 39% (329/836) of participants complied with the recommendation of ingesting LT4 ≥ 30 minutes before eating. Additionally, 7% (58/856) of participants concurrently used molecules that bind to LT4, without applying the recommended dosing interval. There was no significant correlation between LT4 usage (adherence, timing of intake, and interaction with complex forming drugs) and TSH or HR-QoL.
Conclusions:
We found that many participants with hypothyroidism did not use their LT4 as effectively as possible, particularly with respect to timing of administration. However, the participants' HR-QoL seemed largely satisfactory, and there was no significant correlation between correctly using LT4 and thyroid health.
Introduction
Hypothyroidism is a common endocrine condition characterized by thyroid hormone deficiency. If untreated, it may lead to serious adverse health effects on multiple organ systems and substantially impair well-being. The mainstay of treatment is to restore the euthyroid state by oral administration of levothyroxine (LT4). 1 –4 The persistence of residual symptoms that compromise quality of life (QoL) has been described in up to 15% of treated hypothyroid patients. 5 –9 Several potential explanations have been proposed, but the underlying mechanism is unclear. 10
To gain maximum therapeutic effect while minimizing side effects, it is imperative for patients with hypothyroidism to use their LT4 correctly. Despite the apparent simplicity of a once-daily orally administered hormone replacement therapy, there are some issues that might complicate its use. For almost all patients, LT4 is a lifelong therapy. Non-adherence to medication is a major obstacle to the effective management of many chronic diseases. 11 Although LT4 is one of the most commonly prescribed drugs in Europe and the United States 12 –15 (and its use is still increasing with lower thyrotropin [TSH] thresholds for initiating LT4 and even treating people having normal thyroid function 16,17 ), there is surprisingly little research about LT4 adherence in hypothyroidism. 8,18 –21
The absorption of LT4 is decreased with concurrent food ingestion. Studies have shown a reduction of intestinal absorption from ∼80% (fasted) to 40–64% (with food). 22 –24 It is thus recommended to take LT4 at least 30 minutes before food or 3 hours after the last meal. 4,25 –27 Other medications, such as calcium and iron, may bind to LT4 and decrease its absorption. It is therefore advised to separate administration of these drugs and LT4 by several hours. 28 –30 Distancing the timing of administration of LT4 from ingestion of food or interacting medications may be inconvenient to fit into patients' daily lives. It is currently unknown to what extent patients comply with these intake recommendations.
We aimed to investigate LT4 use (i.e., adherence, timing of intake, and presence of drug interactions) and thyroid health (i.e., TSH levels and health-related quality of life [HR-QoL]) in a Belgian community sample of patients with hypothyroidism. We also explored whether correct LT4 use may be associated with better thyroid health.
Methods
Study design
This cross-sectional observational study was conducted between November 2018 and June 2019 in 183 community pharmacies in Belgium. Community pharmacists consecutively approached patients presenting with a prescription for LT4 (H03AA01, Anatomical Therapeutic Chemical [ATC] Classification) for enrollment. Participants were required to meet the following inclusion criteria: (1) using LT4 for at least 2 years (to ensure that patients are not in the initial dose titration period), (2) being age 18 years or older, and (3) having accessible pharmacy dispensing data (including data from other pharmacies in Belgium). Exclusion criteria were as follows: (1) current or previous thyroid cancer, (2) pregnancy, (3) using a thyreostatic drug (H03B, ATC) in addition to LT4, and (4) inability to complete a Dutch-language questionnaire. We planned to recruit five participants from each of the pharmacies.
Approval for the study was granted by the ethics committee of Ghent University Hospital (B670201837525), and all participants provided written informed consent.
Data collection
Questionnaires
Participants completed two self-administered paper-based questionnaires.
The first questionnaire was developed by the multidisciplinary research team. It collected the following information: sociodemographic characteristics, body weight and length, smoking status, alcohol consumption, frequency of thyroid-related physician consultations, cause of hypothyroidism, level of symptom control (“Over the past 4 weeks, how bothersome were your thyroid symptoms?”; participants were asked to draw a line on a 0–100 Visual Analogue Scale [VAS] ranging from 0 mm [“not at all”] to 100 mm [“more than I can image”] 31 ), dose, duration of use and timing of intake of LT4, whether LT4 dose had been changed in the past 6 months, occurrence of LT4 side effects, use of liothyronine or desiccated thyroid extracts, current co-medication (including timing of intake), and occurrence of major life events (e.g., divorce, decease of a close relative) and being diagnosed with a major illness in the past 6 months (as we hypothesized that this might impact HR-QoL, cfr. infra).
The questionnaire also assessed self-reported adherence using the 5-item version of the Medication Adherence Report Scale (MARS-5) 32 and participants' beliefs about LT4 using the Beliefs about Medicines Questionnaire (BMQ-Specific). 33,34 The MARS-5 and BMQ-Specific are described more in detail in Supplementary Appendix SA1.
The second questionnaire was the short version of the thyroid-specific patient-reported outcome (ThyPRO-39), a comprehensive and well-validated measurement tool for the assessment of HR-QoL in patients with benign thyroid disease. 35,36 It consists of 39 items summarized into 12 scales and 1 single-item measuring overall QoL. The questionnaire encompasses three main areas: physical symptoms (goiter, hyperthyroid, hypothyroid, and eye symptoms), mental health (tiredness, cognition, anxiety, depression, and emotional susceptibility), and impact of the disease (impaired social life, daily life, cosmetic concern, and overall QoL). Each scale's total score ranges from 0 to 100, with higher scores indicating poorer HR-QoL. A composite score was also computed.
Pharmacy refill adherence
Pharmacy refill adherence to LT4 was assessed by the medication possession ratio (MPR), a well-established measure of implementation adherence (i.e., how well the patient's actual intake matches the prescribed dosing regimen) using pharmacy dispensing data. 37,38 For each patient, we collected dispensing data over an observation period of 2 years (i.e., 2 years before inclusion in the study). The MPR was calculated by dividing the total number of days' supply by the number of days in the observation period. Days' supply was calculated based on dispensing data (dispensing date, package size, and number of packages supplied) and dosing regimen (extracted from the patient questionnaire). Of note, LT4 is only available in tablet formulation in Belgium.
If a patient combined two dosage strengths (e.g., 75 and 100 μg), we used the mean MPR of both dosage strengths. An MPR of ≤80% was considered as non-adherence, in line with prior research. 39
Thyroid function
The patient's most recent TSH level, together with the laboratory's reference range, was collected as an objective measure of thyroid health. This information was retrieved from the patient's primary care physician. TSH measurements >6 months before patient inclusion in the study were excluded from analysis.
The patient-reported cause of hypothyroidism was confirmed with the primary care physician.
Data analysis
Drug interactions with complex forming agents
Co-medication was screened for potential drug interactions between LT4 and complex forming agents (e.g., aluminum, calcium, iron, lanthane, magnesium, which were selected because of their impact on LT4 absorption). 28 –30 Timing of intake of LT4 and the complexing agents was extracted from the patient questionnaire. If the patient did not apply the recommended dose separation (i.e., LT4 2 hours before or 4 hours after the complexing agent), we defined this as presence of an interaction.
Statistical analyses
Data are reported as counts with percentages, means with standard deviations, or medians with interquartile ranges (IQRs), as applicable.
Chi-square tests were used to explore relationships between categorical variables. Independent samples t-tests were used to compare normally distributed continuous data between two groups, and the Mann–Whitney U tests for non-normally distributed continuous data. Spearman's rho was used to estimate correlations between two non-normally distributed continuous variables.
Linear regression analysis was used to evaluate the impact of MPR-based adherence to LT4, timing of LT4 administration, and presence of an interaction between LT4 and a complex forming agent on ThyPRO-39 composite scores. Use of psycholeptics or psychoanaleptics (N05 and N06, ATC), occurrence of a major life event in the past 6 months, and being diagnosed with a major illness in the past 6 months were added to the model as covariates.
Statistical analyses were performed with SPSS Statistics V.28 (IBM, Armonk, NY). A p-value below 0.05 was considered statistically significant.
Results
Study population
In the 183 participating pharmacies, 1523 patients presenting with a prescription for LT4 were approached for enrollment, of which 1111 (72.9%) were eligible. Approximately 77% of them (856/1111) agreed to participate (Fig. 1). “No time” and “no interest” were the most common reasons for nonparticipation.
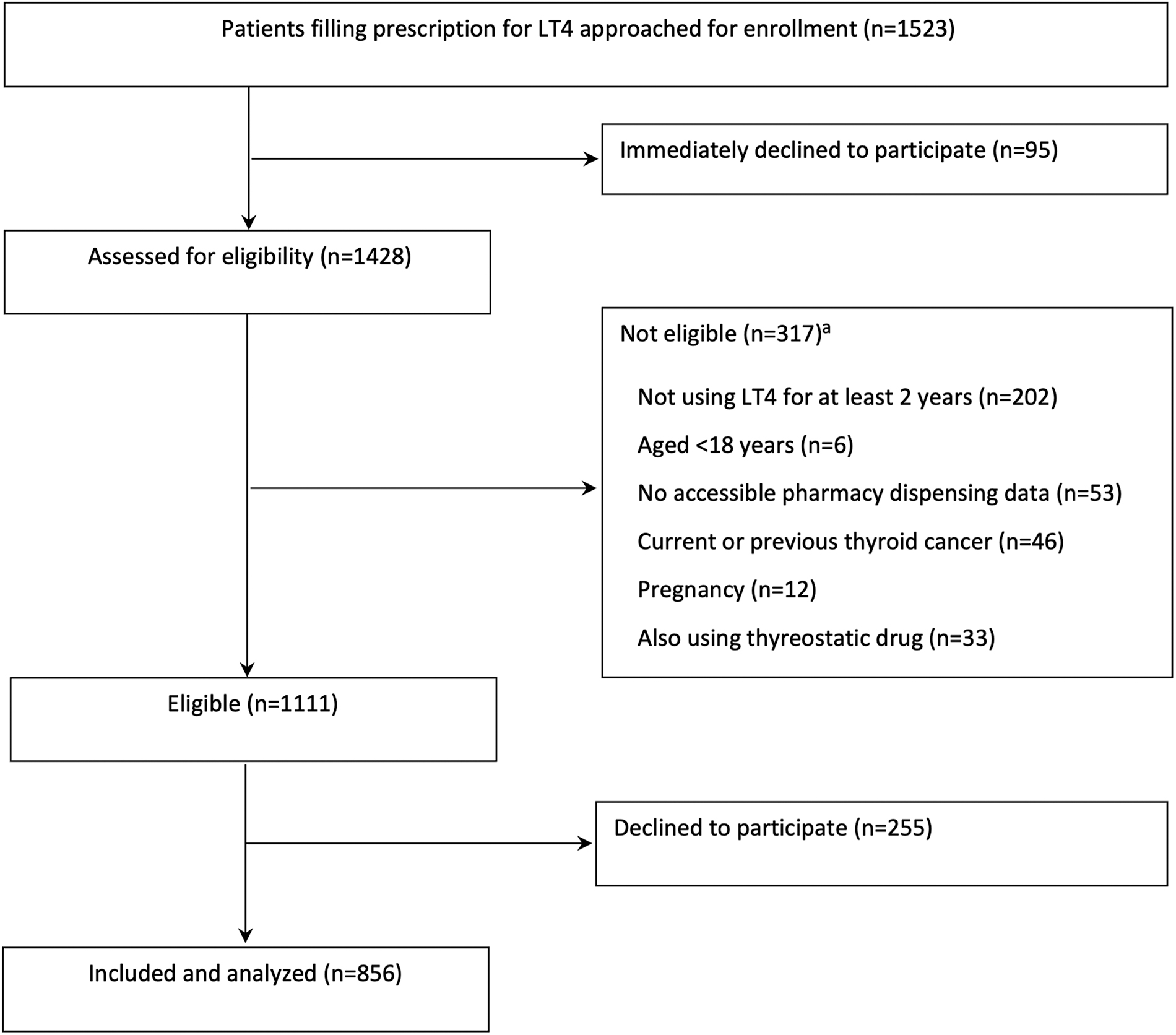
Flow diagram of the patient recruitment process. aMultiple reasons possible.
Approximately 86% of participants (740/856) were women; the mean age was 61.4 ± 14.3 years (Table 1). More than half of participants were either overweight (35.7%, 301/843) or obese (22.3%, 188/843). Participants used a median of 4 (IQR: 2–7) other medications in addition to LT4, with statins (used by 33.1% of participants, 283/856), proton pump inhibitors (27.9%, 239/856), selective beta blockers (20.4%, 175/856), paracetamol (19.6%, 168/856), and nonsteroidal anti-inflammatory drugs (NSAIDs; 17.8%, 152/856) being the most frequently used drugs.
Patient Characteristics
Data are presented as n (%) of patients, unless indicated otherwise.
Subject to missing data.
Including all current medication and supplements (prescription and over-the-counter; acute, chronic, and as needed).
Very diverse, for example, red yeast rice, saffron, curcuma, “sleep herbs.”
BMI, body mass index; IQR, interquartile range; NSAID, nonsteroidal anti-inflammatory drug; SD, standard deviation.
Thyroid health
The most commonly reported causes of hypothyroidism were Hashimoto's disease (43.6%, 373/856) and thyroidectomy (21.8%, 187/856) (Table 2). Only 28.5% (244/856) had consulted an endocrinologist in the past 2 years. The median TSH level of our sample was 1.50 (IQR 0.63–2.84) mU/L; about one quarter of participants (138/563) had out-of-range TSH levels (14.6% [82/563] below and 9.9% [56/563] above reference range). Participants with out-of-range TSH levels were significantly older than participants with within-range TSH (63.9 ± 13.5 vs. 60.8 ± 14.5 years, p = 0.027), but they did not differ with respect to gender (p = 0.457), body mass index (p = 0.729), living situation (p = 0.991), education level (p = 0.091), smoking status (p = 0.483), and cause of hypothyroidism (unknown cause vs. other cause; p = 0.893) (Table 3).
Thyroid Health
Data are presented as n (%) of patients, unless indicated otherwise.
Patient and/or GP did not know cause, did not want to provide cause, or provided unspecified cause (e.g., “slow thyroid”).
N = 563 since TSH values determined >6 months before inclusion date were excluded.
Scores range between 0 and 100, with higher scores indicating worse HR-QoL.
“Over the past 4 weeks, how bothersome were your thyroid symptoms?”; VAS scores range between 0 (“not at all”) and 100 (“more than I can image”).
GP, general practitioner; HR-QoL, health-related quality of life; QoL, quality of life; ThyPRO-39, thyroid-specific patient-reported outcome; TSH, thyrotropin; VAS, Visual Analogue Scale.
Characteristics of Participants with Within-Range Thyrotropin Levels Versus Participants with Out-of-Range Thyrotropin Levels
Regarding HR-QoL, “emotional susceptibility,” “tiredness,” and to a somewhat lesser extent “depressivity” were ThyPRO-39 scales showing the worse scores (Table 2). Self-rated overall symptom control on a 0–100 VAS indicated that our sample perceived their thyroid symptoms as not bothersome at all (median VAS: 1.0 mm, IQR 0.0–5.0). However, a small subgroup of the studied population (4.1%) marked a VAS score >50, which suggests poor symptom control. A statistically significant correlation between ThyPRO-39 composite scores and VAS scores was found (r = 0.277, p < 0.01). ThyPRO-39 composite scores did not significantly correlate with TSH values (r = 0.052, p = 0.222).
LT4 use
Participants were treated with LT4 for a median duration of 10 years (IQR 5–19) (Table 4). The median dose was 1.23 μg/kg body weight (IQR 0.88–1.54). The majority (88.3%, 754/854) had a simple dosing regimen with the same LT4 dose each day, while 11.7% (100/854) was prescribed an alternating days regimen. Only 6.3% (54/856) reported to experience side effects of LT4, with palpitations (n = 13), weight gain (n = 10), fatigue (n = 8), and nervousness (n = 7) being most common. Use of LT3 and desiccated thyroid extracts was very rare in our sample (0.6%, 5/856 and 0.5%, 4/856, respectively).
Levothyroxine Use
Data are presented as n (%) of patients, unless indicated otherwise.
Most frequently reported side effects: palpitations (n = 13), weight gain (n = 10), fatigue (n = 8), nervousness (n = 7).
A total score <25 was considered as non-adherence.
Item 1 reflects non-intentional non-adherence, items 2–5 reflect intentional non-adherence.
An item score <5 was considered as non-adherence.
Total N = 632 since MPR was not calculated in case of recent dose change and/or if observation period was <1 year.
Represents n (%) of patients agreeing or strongly agreeing with the statement.
Denominator represents number of patients using this complexing agent; numerator represents number of patients not applying the recommended dose separation.
BMQ, Beliefs about Medicines Questionnaire; LT4, levothyroxine; MARS-5, 5-item version of the Medication Adherence Report Scale; MPR, medication possession ratio.
Adherence to LT4
Based on MARS-5, we identified one quarter of participants as non-adherent (total MARS-5 score <25), which was mainly due to non-intentional non-adherence (i.e., forgetting to take LT4) (Table 4).
Based on pharmacy dispensing data, the median MPR was 88.4% (IQR 77.6–95.8). About 28% (178/632) of participants were considered as non-adherent (MPR <80%) (Table 4). This implies that these participants had at least 73 cumulative days per year without LT4 intake (365–0.8 × 365 days).
Regarding patient beliefs about LT4, the median BMQ Necessity score was 17 (IQR 15–20) and the median BMQ Concerns score was 10 (IQR 8–14), resulting in a positive necessity-concerns differential of 6 (IQR 2–10) (Table 4). For the majority of participants (86.0%, 727/856), the necessity beliefs about LT4 outweighed the concerns. With respect to necessity of LT4 treatment, participants showed the highest level of agreement with the item “My LT4 protects me from becoming worse” (65.1% [557/856] agreed or strongly agreed). The highest level of concern was expressed for the item “My LT4 is a mystery to me” (37.0% [316/856] agreed or strongly agreed).
The medians of the BMQ Necessity score, the BMQ Concerns score, and the BMQ necessity-concerns differential did not differ significantly between adherent (MPR ≥80%) and non-adherent (MPR <80%) participants (p = 0.230, p = 0.343 and p = 0.230, respectively).
Timing of LT4 intake
To maximize drug absorption, clinical practice guidelines recommend intake of LT4 at least 30 minutes before food or at least 3 hours after the last meal. However, only 39.4% (329/836) of participants complied with this recommendation (Table 4). In our study, the most common deviation was taking LT4 < 30 minutes before food (48.1%, 402/836). Nevertheless, participants appeared to be very consistent in their scheduling of LT4 intake as they reported a median of 7.0 days (IQR 7.0–7.0) of consistent timing over the past week.
Drug interactions with complex forming agents
In almost 7% (58/856) of participants, we found an interaction with a complex forming agent, meaning that these participants used a complex forming agent but did not apply the recommended dose separation (Table 4). These interactions most commonly occurred with iron (n = 32).
Is correct LT4 use associated with better thyroid health?
TSH level
The percentage of participants with within-range TSH levels did not differ between adherent (MPR ≥80%) and non-adherent participants (82.5%, 241/292 vs. 78.8%, 89/113; p = 0.381), between participants administering LT4 ≥ 30 minutes before food and participants not administering LT4 ≥ 30 minutes before food (75.1%, 172/229 vs. 75.3%, 244/324, p = 0.957), and between participants reporting an interaction with a complexing agent and those without an interaction (72.3%, 34/47 vs. 72.3%, 391/516, p = 0.600).
Health-related quality of life
The linear regression analysis showed that ThyPRO-39 composite scores were not significantly associated with MPR-based adherence (estimate, −0.17; confidence interval [CI] −2.2 to 1.8; p = 0.866), timing of LT4 administration (estimate, −1.04; CI −2.91 to 0.83; p = 0.274), or presence of an interaction with a complexing agent (estimate, 3.50; CI −0.06 to 7.07; p = 0.054). However, all three covariates added to the model significantly impacted ThyPRO-39 composite scores: worse ThyPRO-39 composite scores were associated with use of psycholeptics/psychoanaleptics (estimate, 4.43; CI 2.48 to 6.38; p < 0.001), a major life event in the past 6 months (estimate, 4.56; CI 2.34 to 6.78; p < 0.001), and diagnosis of a major illness in the past 6 months (estimate, 2.99; CI 0.09 to 5.89; p = 0.043).
Discussion
This community pharmacy study investigated LT4 use and thyroid health in patients with hypothyroidism. We found that almost 30% of participants had an MPR below 80%, which corresponds to at least 73 cumulative days without LT4 intake per year. The clinical impact of these days without dose is not yet clear. Single missed doses are probably less impactful than longer gaps in LT4 use, but unfortunately our data did not allow determination of whether the missed doses occurred consecutively or not. Relevant to note, LT4 has a long half-life (7 days 4 ), suggesting that its therapeutic outcomes are robust for single missed doses because the duration of action greatly exceeds the dose interval, and therefore, LT4 can be considered as having a high level of “forgiveness.” 40,41
There is a paucity of data reported on adherence to LT4. A large retrospective analysis of claims data among patients with hypothyroidism initiating LT4 treatment found that less than half were adherent over the first 12 months post-initiation. 19 Other studies investigated adherence through self-report and found adherence rates ranging between 59% and 87%. 18,20,21,42 Interestingly, a cohort study by Hepp et al. found lower all-cause and hypothyroidism-related costs and resource utilization as well as significantly lower rates of many comorbid diagnoses (e.g., depression, diabetes, obesity) in adherers compared with non-adherers. 43 Given that hypothyroidism is a prevalent disease that most often requires lifelong LT4 treatment, this suggests that the economic and clinical impact of non-adherence to LT4 could be substantial.
Non-adherence should therefore be proactively followed up so that timely intervention is possible (i.e., identifying reasons for non-adherence and providing patient-tailored solutions), preferably by a physician–pharmacist collaborative approach. Forgetfulness was the most frequently reported reason for missing doses in our sample. There are several management strategies available to tackle this, for example, use of reminder systems. 44 Importantly, our sample showed a positive attitude toward LT4 treatment, with necessity beliefs outweighing concerns. However, almost 40% (strongly) agreed with the statement “My LT4 is a mystery for me” indicating the need for improved patient education about LT4, tailored to patients' health literacy.
Only 39% of our study population complied with the recommendation of ingesting LT4 at least 30 minutes before eating or at least 3 hours after the last meal. Nevertheless, compliers did not differ from non-compliers in TSH or ThyPRO scores, which might be due to the fact that our study participants were very consistent in their timing for LT4 intake. Probably day-to-day consistency in timing of LT4 intake is more important than the exact timing itself as LT4 dose will be titrated in function of TSH levels. Moreover, a previous study found that taking LT4 with breakfast can be a reasonable alternative regimen for patients who have adherence difficulties due to delaying breakfast.
However, this regimen is more likely to cause variability in TSH levels, so for patients for whom a stable serum TSH level is important, fasting LT4 ingestion is still the preferred choice. 45 Based on our study findings, it may be appropriate to make less stringent recommendations about timing of intake of LT4 in clinical practice for patients in whom a stable TSH is not considered critically important. This could potentially enhance patient convenience and adherence, as long as patients are adequately educated about the importance of maintaining a consistent schedule for taking LT4.
Seven percent of participants in our study concurrently used molecules that bind to LT4, without applying the recommended dosing interval. In the case of long-term use of such interacting minerals (e.g., calcium), the physician may notice eventual increases in TSH levels during routine follow-up and adapt LT4 dosing accordingly. However, short courses might remain undetected and could cause TSH fluctuations, especially in patients who are completely dependent on exogenous LT4 (e.g., following total thyroidectomy). Moreover, most of these interacting minerals are available without prescription and may thus be used without knowledge of the physician. This highlights the importance of the role of community pharmacists in advising patients about how to avoid these interactions.
Although our study participants were treated with LT4 for at least 2 years, about one in four patients had TSH levels outside the reference range, which is somewhat lower than in previous reports (37–44% out-of-range). 46,47 These patients could be at increased risk of adverse health outcomes, particularly for TSH concentrations above the upper reference limit. 47 Nonetheless, our study population was observed to generally have ThyPRO scores that were largely very similar to the general population. 48 Our finding is in contrast with previous reports of impaired QoL among LT4-treated patients. 6 –8 For example, online patient surveys by the American Thyroid Association 8 and the British Thyroid Foundation 7 revealed a remarkable dissatisfaction with hypothyroidism treatment. However, as acknowledged by the authors, 8 such surveys might be subject to sampling bias as they might have mainly attracted dissatisfied patients. Overall, our study suggests that the vast majority of LT4-treated patients with hypothyroidism who are sampled through community pharmacies appear to be doing fine.
We did not observe a significant correlation between LT4 use (adherence, timing of intake, and interaction with complex forming drugs) and TSH or HR-QoL. The reason why suboptimal LT4 use was not reflected in TSH levels could be that physicians adjusted LT4 doses based on TSH levels, in cases where poor adherence, concomitant food intake, or drug interactions may have impacted LT4 efficacy. However, if suboptimal use is not reported by the patient, such dose increases can lead to a low TSH if LT4 administration is later corrected. Regarding HR-QoL, this is a complex matter with several influencing factors at play. For example, we found that use of pyscholeptics/psychoanaleptics and a recent major life event or new major diagnoses significantly affected HR-QoL.
The main strength of this study is that we reported real-life data about how patients with hypothyroidism use their LT4 and how they perceive HR-QoL, by combining questionnaire data with pharmacy dispensing data and by using well-validated measures (MPR, MARS-5, ThyPRO-39) in conjunction with review of recent TSH measurements. Moreover, our study appears to have captured a representative sample of participants with hypothyroidism, with the cause of hypothyroidism confirmed by contact of their primary care physicians. Our sample included 6.4 times more females than males (hypothyroidism is 5–8 times more common in women than in men), and the most commonly reported cause of hypothyroidism was Hashimoto's disease, which is in line with the literature. 25 Furthermore, our study population included a substantial number of participants with low educational levels. Those with low educational levels are often underrepresented in survey studies, which may introduce bias. 49
This study also has some limitations. First, we only included experienced LT4 users (due to the inclusion criterion of “using LT4 for at least 2 years”). This implies that our findings cannot be generalized to patients who recently started taking LT4. Adherence, for example, may be different in the latter group. Second, the findings are also not applicable to thyroid cancer patients and survivors, who were excluded from the study. Third, 23% of eligible participants declined study participation, which may have contributed to potential selection bias. Fourth, we collected data through a patient-completed questionnaire, which may be subject to recall bias. Fifth, TSH values were not determined specifically for this study since this was not practically feasible, given the high number of study centers (n = 183).
Instead, we used recent routine TSH measurements retrieved via the patient's primary care physician. Furthermore, TSH levels measured >6 months before patient inclusion in the study were excluded from analysis of TSH data. This implies that our findings about TSH should be interpreted with caution since participants may have lacked a recent TSH measurement with their primary care physician for reasons that may affect TSH levels. This may include patients with poor adherence skipping laboratory tests or doctor visits, patients on a stable dose for several years who feel well and therefore avoid general practitioner (GP) visits, or patients whose TSH is measured by the endocrinologist (of note, in Belgium, most patients with hypothyroidism are treated by primary care physicians).
We also have no information about TSH at diagnosis, and the cause of hypothyroidism is patient-reported. Finally, the level of adherence was estimated based on pharmacy dispensing data. Purchasing medication does not necessarily mean actual use by the patient. However, pharmacy data reflect actual use better than data obtained from prescription records since the patient already bought the medication (suggesting the intention of actual use).
In conclusion, we discovered that in Belgium, many community pharmacy patients with hypothyroidism do not use their LT4 according to guidelines, particularly with attention to taking it regularly and at the right time. Despite this, our study population's level of HR-QoL seemed largely satisfactory, and there was no significant correlation between correctly using LT4 and thyroid health.
Footnotes
Acknowledgments
The authors would like to thank the participating participants and pharmacists.
Authors' Contributions
All authors contributed to the concept and design of the study. E.M. performed the data analysis, interpretation, and writing under the supervision of K.B. All authors revised the article critically and approved the final version of the article.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
No funding was received for this study.
Supplementary Material
Supplementary Appendix SA1