
Abstract
Background:
GlycA is a novel glycoprotein biomarker of systemic inflammation and cardiovascular risk. Our objective was to assess the levels of GlycA in individuals with hypothyroidism. We also explored whether levothyroxine (LT4)-treated patients had different levels of GlycA, with attention to thyrotropin (TSH) levels.
Methods:
We performed a cross-sectional analysis, using baseline data from the ELSA-Brasil cohort study. We included only participants with serum TSH and GlycA levels measurements, using magnetic resonance spectroscopy (n = 4745). We excluded individuals with endogenous hyperthyroidism and those using drugs impacting thyroid function. Participants not taking LT4 and whose serum TSH was 0.4–4.0 mIU/L were classified as euthyroid (EU) and those with elevated TSH as undiagnosed hypothyroidism (UH). For those on LT4 (n = 345), adequacy of treatment was defined as TSH within the reference range. Those with TSH <0.4 mIU/L were considered over-treated (OT), and those >4.0 mIU/L, under-treated (UT). Both (UT+OT) were considered inadequately treated (IT). Group comparisons were performed by Kruskal-Wallis, adjusted Chi-square, and the post hoc Dunn test. Additional subgroup analysis were performed in patients with circulating thyroperoxidase antibodies (TPO-Ab+). Respective multivariable analyses were performed to evaluate the relationship between thyroid-related variables and GlycA levels (Generalized Linear Model), as well as an abnormal GlycA (>400 μmol/L; Logistic Binary Regression).
Results:
The prevalence rate of UH was 9.8% (467/4745) and, among those on LT4, only 61.7% (213/345) were adequately treated (AT). GlycA levels were higher in IT in comparison to EU (429 vs. 410 μmol/L, p < 0.01) but did not differ between UH (413 μmol/L) and euthyroidism. However, the subgroup analysis of those TPO-Ab+ showed that not only those with IT, but also those with UH, had higher levels of GlycA in comparison to euthyroidism (423 and 424 vs. 402 μmol/L, p = 0.04). This association between higher levels of GlycA and IT was maintained even in multivariable analysis (odds ratio 1.53, confidence interval 1.03 to 2.31) Lower levels of GlycA were detected in AT (405 μmol/L,) compared with OT (432 μmol/L, 0.04) and UT (423 μmol/L, p = 0.02).
Conclusions:
Patients with IT, both OT and UT, had higher GlycA levels, which may be associated with low-grade systemic inflammation and, possibly, increased cardiovascular risk.
Introduction
Both hypo- and hyperthyroidism are associated with increased cardiovascular risk. 1,2 This elevated risk may be related not only to traditional cardiovascular risk factors, such as metabolic syndrome, but also to non-classic risk factors that are associated with low-grade inflammation and endothelial dysfunction. 1,2
Excessive thyroid hormone action augments both cardiac chrono and inotropism, enhances the risk of arrythmias, leads to diastolic hypertension, impaired vascular function, and increased carotid intima hyperplasia. 1,2 All these conditions may impact risk for premature cardiac mortality. 1,2 Conversely, a reduction in thyroid hormone action is associated with impairment of peripheral vascular resistance and reduction of cardiac chrono and inotropism. 1,2
In addition, dyslipidemia and metabolic syndrome are well-known consequences of hypothyroidism. 1,2 There is compelling evidence linking overt and subclinical hypothyroidism to increased cardiovascular risk, including changes in blood pressure, endothelial function, and cholesterol levels. 3,4 All these conditions may result in higher cardiovascular event risk. 3,4
Abnormal levels of thyroid hormones may be induced by under- or over-treatment of hypothyroidism with levothyroxine (LT4), which may also impact cardiovascular risk and mortality. 5 –7 It has been reported that patients taking LT4 replacement with thyrotropin (TSH) above or below the reference range (RR) may have an increased risk of mortality, 8 especially when TSH is under the RR. 5 –10 Both exogenous hypothyroidism and hyperthyroidism have been associated with a higher risk of atrial fibrillation and stroke. 11 Moreover, it has been reported that ∼40% of patients on LT4 replacement are inadequately treated (IT) in Brazil 12 and worldwide. 13
The main cause of hypothyroidism is autoimmune thyroiditis. 14 Thyroid dysfunction and autoimmunity may be associated with low-grade inflammation, which may potentiate increased cardiovascular risk. Studies have reported higher levels of traditional inflammatory markers in patients with hypothyroidism and hyperthyroidism. 15,16
Chronic heightened systemic inflammation potentiates endothelial dysfunction and accelerated atherogenesis, resulting in subclinical cardiovascular disease, which can progress to ischemic heart disease and mortality. Some traditional inflammatory markers are increased during this process, such as high-sensitivity C-reactive protein (hsCRP), interleukin-6 (IL-6), homocysteine, and fibrinogen. 17
All of them were also elevated in other situations, exhibiting low specificity and high intra-individual variability. 16 –20 There is ongoing research in discovering new and reliable markers of inflammation, to enable more accurate risk stratification of patients at increased cardiovascular risk.
GlycA is a glycoprotein biomarker that may be measured by nuclear magnetic resonance (NMR) spectroscopy that reflects systemic inflammation by quantifying acute-phase reactant and multiple glycosylated proteins. 21 –24 GlycA is a more reliable inflammatory biomarker because of its lower intra-individual variability and greater analytic precision, as compared with other inflammatory markers. 21 –25 GlycA has been correlated with indolent inflammation in patients with cardiometabolic risk factors such as obesity, insulin resistance, and metabolic syndrome. 23,25,26
Prospective cohort studies have shown that GlycA concentration is associated with both prevalent and incident cardiovascular events, independent of traditional risk factors. 27 –33 Higher GlycA levels have also been reported to be associated with all-cause and non-cardiovascular mortality, even after adjusting for traditional risk factors. 30 GlycA is also associated with chronic inflammatory diseases, such as autoimmune diseases (systemic lupus erythematosus, rheumatoid arthritis, and psoriasis), and is useful as a biomarker of both systemic disease activity and cardiovascular risk. 27 –33
Variations in levels of GlycA in patients with thyroid dysfunction and in those receiving LT4 replacement to treat hypothyroidism are unknown. We also hypothesized that patients with hypothyroidism, especially when caused by autoimmune thyroid disease, have higher levels of GlycA. We also hypothesized that the adequacy of hypothyroidism treatment is related to lower levels of GlycA.
The main objective of this study was to evaluate the levels of GlycA in individuals with hypothyroidism, and to determine whether those receiving LT4 replacement therapy had different levels of this biomarker, with attention to the adequacy of treatment (as determined by TSH levels).
Materials and Methods
Study design
We performed a cross-sectional analysis of baseline data obtained at the ELSA-Brasil study. This is a prospective cohort study conducted in six different Brazilian cities, which aims at determining the incidence of cardiovascular disease and diabetes, and associated risk factors. Classical and nonclassical cardiovascular risk factors are evaluated, including thyroid function.
The cohort enrolled 15,105 active and retired civil servant employees aged 35–74 years between 2008 to 2010. The study design and cohort profile have been published. 34 Clinical and sociodemographic data were collected between August 2008 and December 2010.
This research was conducted in accordance with the Declaration of Helsinki and was approved by the National Review Committee (CAAE:94726218.9.0000.0076). The institutional ethics committee of each enrolled institution approved the study protocol, and written consent was obtained from all participants.
For the present analysis, only participants that had GlycA measurements, which were those from São Paulo, were considered for evaluation (n = 4793). Figure 1 summarizes the cohort and study selection criteria. After excluding those with endogenous hyperthyroidism (n = 48), a total of 4745 participants were evaluated, including 3933 euthyroid (EU), 467 with undiagnosed hypothyroidism (UH), and 345 with treated hypothyroidism (receiving LT4 therapy).
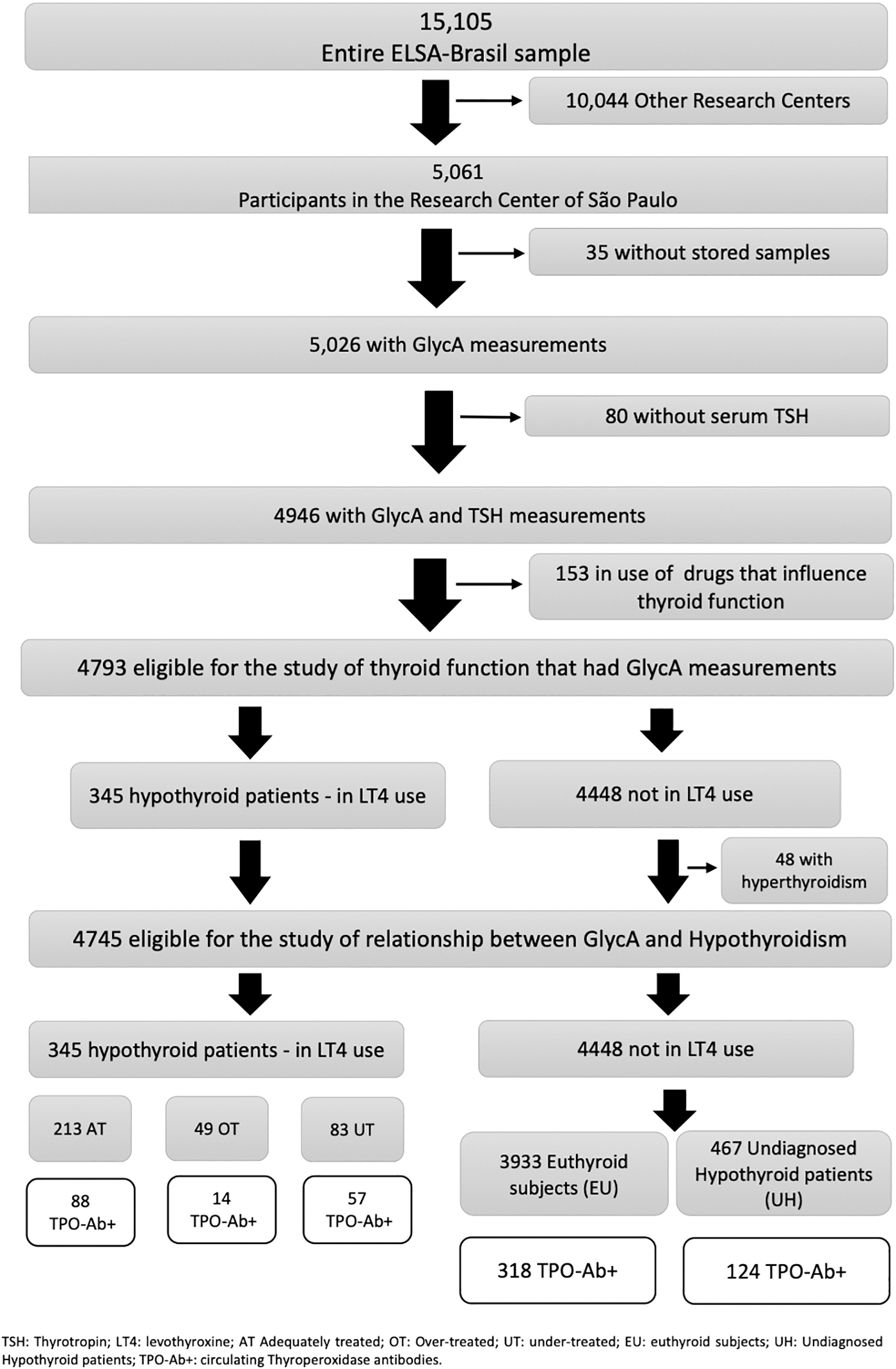
Flowchart of the participants in the study.
Thyroid status
Baseline measurements of thyroid hormone levels were performed for all participants in the study. The levels of TSH and free thyroxine (fT4) were measured using a third-generation immunoenzymatic Elecsys assay (Roche Diagnostics, Mannheim, Germany) in serum obtained from centrifuged venous blood samples obtained after an overnight fast. The RRs were 0.4–4.0 mIU/L for TSH and 0.8–1.9 ng/dL for fT4.
Hypothyroidism was defined by high serum TSH, and further classified as overt hypothyroidism when serum fT4 was below the lower limit of its RR or subclinical hypothyroidism when these levels were in the RR. 14 UH was defined as elevated serum TSH without LT4 replacement.
The adequacy of LT4 replacement was defined based on TSH levels. Patients with serum TSH in the normal range were considered adequately treated (AT). Patients with TSH levels under 0.4 mIU/L were considered over-treated (OT), and those with TSH above 4.0 mIU/L, under-treated (UT). Both (UT+OT) were considered IT.
The levels of thyroperoxidase antibodies (TPO-Ab) were also measured using electrochemiluminescence (Roche Diagnostics) and were considered positive when ≥34 IU/mL.
GlycA
GlycA was measured by NMR spectrometry in plasma of the 5026 Sao Paulo participants. GlycA quantifies acute-phase reactants and a variety of glycoproteins using the NMR signal of their N-acetyl methyl group protons on N-acetylglucosamine (GlcNAc) moieties located on their bi-, tri-, or, tetra-antennary branches (LabCorp, Raleigh, NC).
The intra- and inter-assay coefficients of variation of GlycA were 1.9% and 2.6%, respectively, and biological variability was low (coefficient of variation 4.3% 21,35,36 ). There is absence of an established reference value for serum GlycA, since it is a new biomarker. However, GlycA levels >400 μmol/L have been considered abnormal as this cut-off point is associated with chronic systemic inflammatory states. 33
Statistical analyses
Continuous variables were expressed as median (interquartile range [IQR]), and categorical variables were expressed as percentages. Initially, an exploratory analysis of the factors associated with abnormal GlycA levels (>400 μmol/L) was performed (Supplementary Table S1). To compare continuous variables between two groups, we used the Mann-Whitney U test and to compare dichotomous variables we applied the Chi-square or Exact Fisher Test.
Correlations between two continuous variables were performed by Spearman's correlation index, when necessary. The main exposure groups of interest in this study were initially those with UH and those EU participants. In addition, we evaluated those OT, UT, or AT with LT4. A subgroup analysis of data from patients with circulating TPO-Ab was also performed.
We explored continuous variables among three or more groups by Kruskal-Wallis and thereafter, in a post hoc analysis, we explored continuous variables between them, using the Dunn test for multiple comparisons. 37 In the case of categorical variables, among these groups, we used the adjusted Chi-square test, considering the p-value <0.017 (three groups) or <0.0125 (four groups) as significant, intending to control the alpha error.
Logistic binary regression was applied to explore associates between variables and an elevated GlycA (>400 μmol/L) level. The central exposure group was based on the thyroid status, considering the EU group as the reference for analysis. We used a forward stepwise logistic regression model adding to the model variables related to GlycA levels and to the thyroid status, to be selected for the equation.
The listed variables were: age, sex, diabetes, high blood pressure, smoking habits, body mass index (BMI), sedentary lifestyle, presence of circulating TPO-Ab, and previous thyroid surgery for thyroid cancer. Supplementary Table S2 shows the definitions criteria for the presence or absence of each assessed variable.
A multivariable analysis was performed to explore for factors associated with GlycA levels, as a continuous variable, using a Generalized Linear Model (GLM). The same variables were used in this model as in the logistic binary regression model (described earlier).
However, instead of thyroid status, as previously categorized, we evaluated the serum levels of fT4 (as a continuous variable) and added the categories of serum TSH to the model. The category with serum TSH in the RR was considered as the reference group. This analysis was performed in the whole group and thereafter stratified by LT4 use.
Finally, the serum GlycA levels obtained in the studied population were divided into quartiles of the same size to assess their distribution according to the studied groups.
A p-value <0.05 was considered significant and those ≥0.05 but <0.10 were considered nominally significant. The SPSS software (Version 21.0 for Windows; IBM Corp., Armonk, NY) and the GraphPad Prism (Version 7) were used for the statistical analyses.
Results
The prevalence of UH in the study population was 9.8% (n = 467/4745), with the majority (87.7%, n = 410/467) classified as having subclinical hypothyroidism. In addition, 26.6% of patients with abnormal serum TSH had circulating TPO-Ab in serum (n = 124/467). The clinical and demographic characteristics of the EU participants in comparison to the hypothyroid patients are shown in Table 1.
Characteristics of All Included Participants, and a Subgroup Analysis of Those with Circulating Thyroperoxidase Antibodies, Showing Comparisons Between Groups According to the Presence of Hypothyroidism and Its Treatment
Results are expressed as median (interquartile range) or frequencies. p-Value significant (<0.05) according to Dunn test for multiple comparisons or adjusted Chi-square test: acomparing with EU; bcomparing with AT; ccomparing IT with UH.
AT, adequately treated; BMI, body mass index; DM, diabetes mellitus; EU, euthyroid subjects; fT4, free thyroxine; HBP, high blood pressure; IT, inadequately treated; NE, not evaluated; TPO-Ab+, circulating thyroperoxidase antibodies; TSH, thyrotropin; UH, undiagnosed hypothyroidism.
The median GlycA level in the entire group was 410 μmol/L, and the prevalence of GlycA levels above 400 μmol/L was 56% (n = 2665/4745). GlycA levels were positively associated (Supplementary Table S1) and correlated with hsCRP (r s = 0.610; p < 0.01).
Higher levels of GlycA were found in IT hypothyroid patients in comparison to EU patients, but not in those with UH (Table 1). However, a subgroup analysis of those with circulating TPO-Ab demonstrated that not only those with IT but also those with UH had higher levels of GlycA in comparison to EU patients (423 and 424 vs. 402 μmol/L), as shown in Table 1. In summary, irrespective to being untreated or IT, hypothyroid patients with circulating TPO-Ab had higher levels of the studied biomarker in comparison to EU individuals.
Further, both groups of patients (those with UH and IT) had higher frequencies of GlycA >400 μmol/L in comparison to euthyroidism (61.3%, n = 76/124 and 67.6%, n = 48/71 vs. 50.9%, n = 162/318) and tended to have higher frequencies of GlycA in the highest quartile. This association between higher levels of GlycA and IT hypothyroidism was maintained in a multivariable analysis (odds ratio [OR] 1.53, confidence interval [CI] 1.03 to 2.31), as demonstrated in Table 2.
Binary Logistic Regression Exploring Variables Associated with Abnormal GlycA Levels
Greater than 400 μmol/L. Variables included in the model (equation according to forward stepwise): age, BMI, female sex, diabetes, HBP, smoking habits, TPO-Ab, thyroidectomy by thyroid cancer diagnosis and thyroid status. Reference group in the thyroid status: Euthyroid subjects.
CI, confidence interval; OR, odds ratio.
In addition, independent variables that were positively and independently associated with abnormal levels of GlycA included: BMI, female sex, smoking habits, sedentary lifestyle, diabetes, high blood pressure, and inadequacy of hypothyroidism treatment (Table 2).
There was a positive independent association between serum levels of GlycA and fT4 (OR 10.75, CI 0.74 to 20.75) in the whole group of participants, when performing the GLM (Table 3). A significant association between abnormal serum TSH and GlycA that was observed only occurred in individuals taking LT4 replacement (Table 3). It was detected that both under- and over-treatment, as demonstrated respectively by low and high serum TSH, were positively associated with circulating levels of GlycA (Table 3).
Generalized Linear Model Showing Variables Associated with GlycA Levels in the Whole Group and in the Group of Participants Under Levothyroxine Replacement
Variables included in the model: age, BMI, female sex, diabetes, HBP, smoking habits, TPO-Ab, sedentary lifestyle and thyroidectomy by thyroid cancer diagnosis; fT4 and serum TSH (high: >4.0 mIU/L; low: <0.4 mIU/L).
LT4, levothyroxine.
Of the 345 participants taking LT4, 24.1% (n = 83/345) were UT and 14.2% (n = 49/345) were OT. The median GlycA level in the entire group of patients with hypothyroidism on LT4 replacement was 419 μmol/L (IQR = 84 μmol/L), and the prevalence of GlycA above 400 μmol/L was 58% (n = 201/345).
Lower median levels of GlycA were detected in patients with serum TSH at the target levels, compared with those UT or OT, as shown in Figure 2 and Table 4.
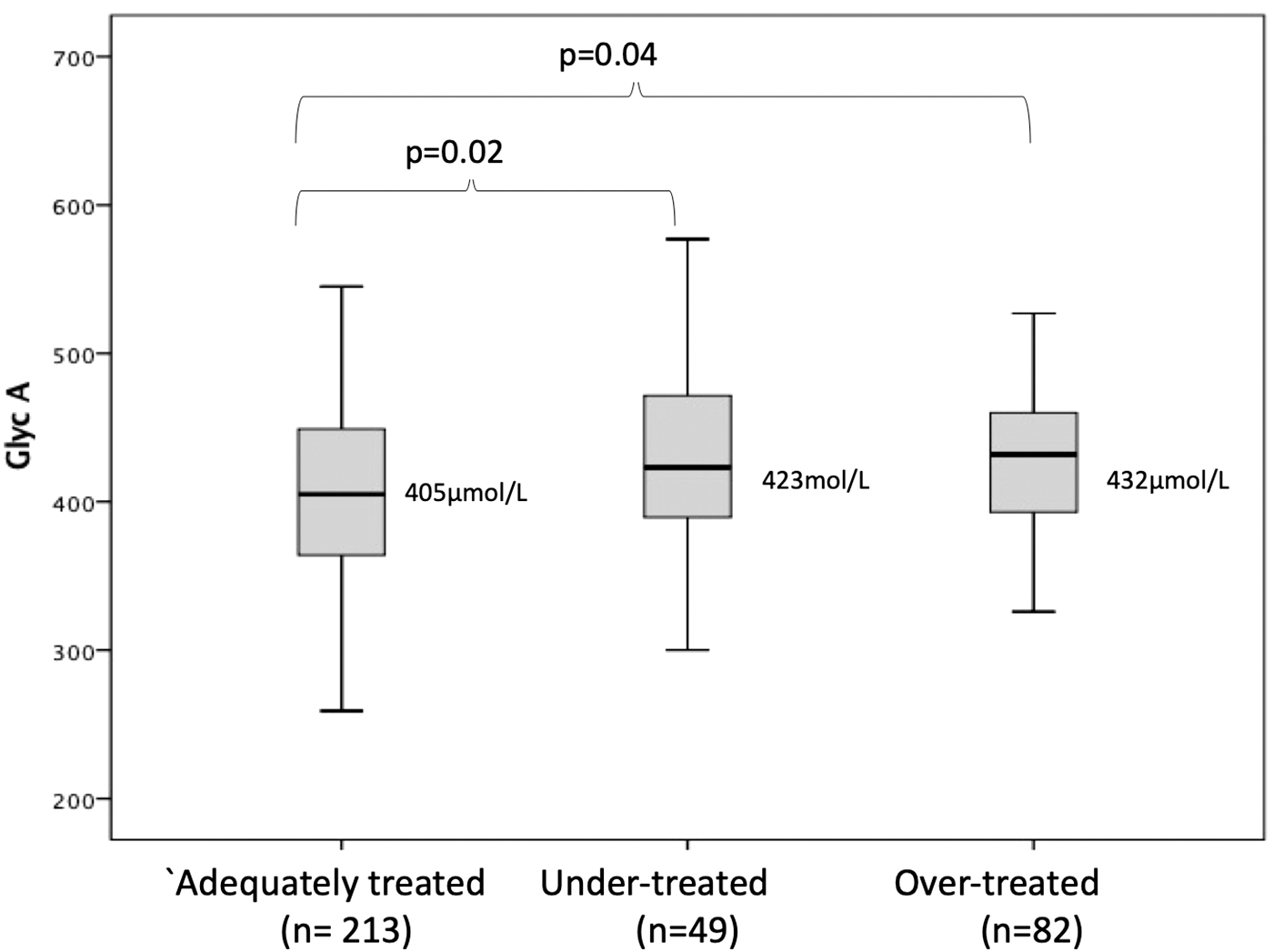
Boxplot showing values of GlycA according to adequacy of hypothyroidism treatment.
Characteristics of All Patients Under Levothyroxine Replacement and Comparisons Between Groups, According to Adequacy of Hypothyroidism Treatment
Results are expressed as median (interquartile range) or frequencies.
p < 0.001 comparing AT vs. UT and also comparing AT vs. OT.
p = 0.02 comparing AT vs. UT.
p = 0.04 comparing AT vs. OT.
p = 0.02 comparing AT vs. UT.
p = 0.03 comparing AT vs. OT.
p < 0.01 only comparing AT with under treated.
p < 0.01 comparing AT with over treated.
OT, over-treated; UT, under-treated.
Considering levels of GlycA >400 μmol/L as abnormal 36 and comparing those UT or OT with the reference group, it was found that those AT had a lower frequency of abnormal GlycA (52%, 111/213) than those OT (69.5%, 34/49) or UT (67%, 56/83) (Table 4).
In examining the levels of GlycA according to quartiles, we found that patients AT with LT4 had a higher prevalence (30.5%, 65/213) of GlycA in the first quartile than patients IT, despite being OT or UT (16.8%, 22/132; p < 0.01). In contrast, they also had a lower prevalence of GlycA in the highest quartile (20.7%, 27/132 compared with 30.5%, 65/213 [p = 0.038]).
Discussion
To the best of our knowledge, this is the first study to evaluate GlycA levels in thyroid disease. Our major finding was that those poorly controlled hypothyroid patients, irrespective of being OT or UT, had higher levels of GlycA and a higher frequency of abnormal GlycA levels than the EU participants or adequately LT4-treated hypothyroid patients.
These findings reinforce the risks of inadequacy of hypothyroidism treatment, since it has been reported that a higher mortality may be related to both under- and over-treatment. 5 –11 Further, the findings were confirmed on examination of data according to GlycA quartiles.
The prevalence of UH observed in the present study is in accordance with that previously reported. 12,13 Further, as expected, the majority of patients with UH had slight elevations of serum TSH and did not fulfill criteria for subclinical hypothyroidism treatment, since the median serum TSH was below 7.0 mUI/mL and <30% had circulating TPO-Ab.
This may explain why those untreated patients, with an elevated TSH, did not have higher levels of serum GlycA in comparison to EU participants, except in the presence of circulating TPO-Ab. The present results suggest that low-grade inflammation may be more frequent in individuals with hypothyroidism requiring treatment or when treatment does not lead to normalization of thyroid indices.
In considering individuals in this study who were taking LT4 replacement, the frequency of inadequacy of treatment was closer to that previously reported in a large study with more than 25,000 participants, 13 and in another study conducted in Brazil. 12 This reinforces the necessity of implementing strategies to improve treatment of hypothyroid patients. 21
It is well documented that poorly controlled hypothyroidism is associated with negative health outcomes such as cardiovascular events, depression, and lower health-related quality of life (HRQoL). 14,38 –41 However, inadequate LT4 replacement occurs worldwide, with >30–40% of patients exhibiting TSH levels outside the normal range in some studies. 12,13,42 –45 Notably, in the National Health and Nutrition Examination Survey (NHANES), the prevalence rate for serum TSH outside the RR was 23% of among the 536 participants with treated hypothyroidism. 46
It is important to acknowledge that the median levels of GlycA in the whole study group were above 400 μmol/L, suggesting that the present study population may have a baseline higher risk for low-grade inflammation due to the presence of confounders. The study sample was composed of participants with a mean BMI compatible with overweight, with a high prevalence of smoking habits and high blood pressure. Previously, GlycA levels have been related to cardiovascular risk factors, which may explain these results. 27 –30
Data from the present cohort (ELSA-Brasil) previously showed that GlycA was positively associated with coronary artery calcium (CAC) score. 47 Higher quartiles of GlycA were associated with higher CAC scores in individuals without metabolic syndrome, allowing those individuals with apparently low cardiovascular risk to be reclassified as having a higher cardiovascular risk. 47
GlycA also appears to be useful as a new cardiovascular risk marker in patients with autoimmune diseases where traditional risk factors and risk scores may not accurately capture cardiovascular risk. In patients with autoimmunity, it has been proposed as a biomarker of both systemic disease activity and cardiometabolic risk. 33,36
In the present study, it was not related to the presence of TPO-Ab or to the diagnosis of other autoimmune diseases, such as Rheumatoid Arthritis or Systemic Lupus Erythematosus. It is important to note the low prevalence of these rheumatologic diseases in the studied population and, as previously highlighted, the inherent high risk for cardiovascular diseases present in the studied group.
In this study, we did not find a high prevalence of TPO-Ab among hypothyroid patients. However, the absence of anti-thyroglobulin antibody (Tg-Ab) measurement was a limitation. Previously, it was reported that the prevalence of TPO-Ab and Tg-Ab was equally important for a diagnosis of Hashimoto's thyroiditis in our population. 48
If we had measured Tg-Ab levels and performed a thyroid ultrasound, we may have found more evidence of thyroiditis. It is also possible that some individuals may have been treated with LT4 for slight TSH elevation, without evidence of associated thyroiditis.
We did not have access to the LT4 amount intake of each patient to estimate a possible excessive, or insufficient, dose prescription and neither to the reasons for LT4 initiation, what might impair the adequate definition of the etiology of the hypothyroidism. We could ascertain the etiology of the hypothyroidism among patients receiving LT4 treatment in only 51% of cases (43.2% were TPO-Ab+, and 7.8% had history of thyroid surgery).
Moreover, the present study demonstrates that the association between GlycA levels and adequacy of treatment is independent of the etiology of hypothyroidism. Neither the presence of TPO-Ab nor the past history of thyroid cancer significantly altered the strength of this association.
In this study, we observed that the presence of circulating TPO-Ab was associated with higher GlycA levels only when thyroid dysfunction was present. An unexpected negative association between TPO-Ab and GlycA levels was found in the entire group of patients with positive TPO-Ab. Reduced inflammatory markers and metabolic parameters in autoimmune thyroiditis have previously been reported by some authors, 49 –51 without a strong mechanistic explanation for this finding.
The cross-sectional design of this study is a limitation that should be noted. However, it has been proposed that higher levels of interferon gamma and estradiol levels may contribute to reduced inflammation in patients with metabolic dysfunction associated fatty liver disease. 50
We have found that although the prevalence of thyroid cancer was higher in OT patients, and in the multivariable analysis, OT patients continued to have higher GlycA levels regardless of the presence of thyroid cancer. Thus, it seems that the increase in GlycA is related to greater TSH suppression and not to the presence of cancer itself.
Despite this, we have to point out an additional limitation of the study, that is, the absence of the determination of the response to cancer treatment of the patients and the absence of data about detailed histological characteristic of the tumors. However, it is well known that most thyroid cancers are well differentiated tumors with a good prognosis, and that it is recommended to avoid overtreatment. 52
The major limitation of the present study was the small number of patients treated with LT4 in the cohort. In addition, the cross-sectional analysis did not permit confirmation of a cause-and-effect relationship between GlycA and hypothyroidism treatment adequacy.
The strengths of the study are related to the robust method of analysis of this new marker, the rigid inclusion and exclusion criteria, and strict quality control in the data collection.
Conclusions
In this study, we observed that patients receiving inadequate treatment for hypothyroidism, both OT and UT, have higher levels of GlycA, which may be associated with greater cardiovascular risk. These findings support the need for more meticulous monitoring of thyroid hormone therapy in patients with hypothyroidism to maintain TSH levels within the normal range to potentially mitigate an increase in cardiovascular risk.
We also found that patients with untreated hypothyroidism only had higher levels of GlycA in the presence of circulating TPO-Ab. It suggests that not all individuals with slight elevations in serum TSH may present a significant thyroid disease potentially related to a risk for low-grade inflammation.
Footnotes
Acknowledgments
The authors thank the ELSA-Brasil participants, staff, and collaborators. Part of the data of this manuscript has been published and was presented at Latin American Thyroid Congress in 2021 as an oral presentation by the name of “GlycA levels as a marker of systemic inflammation in hypothyroid patients under inadequate levothyroxine replacement.” 53
Authors' Contributions
S.G.: conception and design of the work (support), analysis and interpretation of data (lead), and manuscript writing (lead). I.M.B.: funding (lead), data collection (lead), conception and design of the study (lead), interpretation of data, and revision of the manuscript (support). M.J.B.: GlycA analyses (equal), interpretation of data (equal), and editing and revision of the manuscript (equal). S.J.: GlycA analysis (equal), interpretation of data (equal), and editing and revision of the manuscript (equal). P.P.T.: GlycA analyses (equal), interpretation of data (equal), and editing and revision of the manuscript (equal). R.D.S.: conception and design of the study (supporting), GlycA analyses (equal), interpretation, and revision of the manuscript (equal). M.B.: conception and design of the work (supporting), GlycA analyses (equal), and interpretation and revision of the manuscript (equal). P.A.L.: funding (lead), data collection (lead), revision and interpretation of the data, and revision of the manuscript (equal). P.F.S.T.: conception and design of the study (support), analysis and interpretation of the data (lead), manuscript writing, and revision (lead).
Author Disclosure Statement
No conflicts to disclose regarding this manuscript.
Funding Information
I.M.B.: participated in the group responsible for obtaining the ELSA-Brazil baseline study and 4-year follow-up. This study was supported by the Brazilian Ministry of Health (Science and Technology Department) and the Brazilian Ministry of Science and Technology (Financiadora de Estudos e Projetos and CNPq National Research Council; grants of baseline: 01 06 0010.00 RS, 01 06 0212.00 BA, 01 06 0300.00 ES, 01 06 0278.00 MG, 01 06 0115.00 SP, 01 06 0071.00 RJ; grants of 4-year follow-up 01 10 0643-03 RS, 01 10 0742-00 BA, 01 12 0284-00 ES, 01 10 0746-00 MG, 01 10 0773-00 SP, 01 11 0093-01 RJ), and by the FAPESP—Fundação de Amparo à Pesquisa do Estado de São Paulo (2015/17213-2). In addition, she is recipient of a scholarship from the National Research Council (CNPq).
P.A.L.: participated in the group responsible for obtaining the ELSA-Brazil baseline study and 4-year follow-up. This study was supported by the Brazilian Ministry of Health (Science and Technology Department) and the Brazilian Ministry of Science and Technology (Financiadora de Estudos e Projetos and CNPq National Research Council; grants of baseline: 01 06 0010.00 RS, 01 06 0212.00 BA, 01 06 0300.00 ES, 01 06 0278.00 MG, 01 06 0115.00 SP, 01 06 0071.00 RJ; grants of 4-year follow-up 01 10 0643-03 RS, 01 10 0742-00 BA, 01 12 0284-00 ES, 01 10 0746-00 MG, 01 10 0773-00 SP, 01 11 0093-01 RJ), and by the FAPESP (2015/17213-2). In addition, he is recipient of a scholarship from the National Research Council (CNPq). P.F.S.T.: Scholarship of National Research Council (CNPq). All other authors have no funding information to declare.
Supplementary Material
Supplementary Table S1
Supplementary Table S2