
Abstract
Background:
Preterm infants presented a high prevalence of congenital hypothyroidism (CH), while the optimal screening pattern is still under debate. This study aimed at evaluating the characteristics of thyroid function by conducting weekly screening during the first month of life in very preterm infants (VPIs) to achieve timely diagnosis and treatment of CH.
Methods:
A prospective cohort study was carried out on VPIs born with gestational age (GA) <32 weeks (w) and admitted to the participating institutes from January 1, 2019 to December 31, 2022. Serial serum thyroid hormone levels were measured weekly within the first month after birth, and at 36 w of corrected age, or before discharge. Datasets for serial thyroid hormone levels and general information were obtained.
Results:
A total of 5992 VPIs were enrolled in this study, of which 456 (7.6%) [95% confidence interval (CI), 6.9–8.3%] were diagnosed with CH. The incidence of CH increased with lower GA, moving from 4.8% [CI, 3.4–6.1%] at GA 31 w to 16.9% [CI, 8.3–25.4%] at GA <26 w. Among the CH subjects, 57.7% [CI, 53.1–62.2%] were identified after the first screening and classified as delayed thyrotropin elevation (dTSH). With the decrease of GA, the proportion of dTSH also increased, moving from 38.1% [CI, 27.5–48.7%] at GA 31 w to 82.6% [CI, 65.8–99.4%] at GA <26 w. Through conducting weekly screening of thyroid function, it was remarkable that only 42.3% [CI, 37.8–46.9%] of CH subjects were diagnosed during the first screening. The cumulative rate of CH identified by rescreening performed at the second, third, and fourth week was 76.1% [CI, 72.2–80.0%], 90.6% [CI, 87.9–93.3%], and 98.9% [CI, 97.9–99.9%], respectively.
Conclusion:
The incidence of CH and dTSH both increase with lower GA in VPIs. Dynamic screening of thyroid function by weeks within the first month of life is crucial for the timely diagnosis and treatment of CH in VPIs, and it might effectively reduce the implications of missed diagnosis and delayed treatment.
Clinical Trials Registration:
ChiCTR1900025234 and ChiCTR2000037918 (Registration number).
Introduction
Maintaining normal thyroid function from fetus to neonate has a profound impact on the long-term growth and neurocognitive development of infants. 1,2 Congenital hypothyroidism (CH) is defined as insufficient secretion of thyroid hormones in neonates after birth, which can cause mental disability, and is preventable by timely diagnosis and replacement therapy. 3 Therefore, newborn screening for CH in the early days of life, typically performed by measuring thyrotropin (TSH) concentration between the third and seventh days of life, has been widely advocated around the world. 4 –6
Over the past two decades, an increase of preterm infants with lower gestational age (GA) and birth weight (BW) have survived due to the improvement of treatment ability. Every year, about 14.9 million neonates are born prematurely worldwide. 7 –9 More and more clinical research has shown that the incidence of CH in preterm infants is significantly higher than in normal term infants, and it is closely associated with GA. 10 –12
Infants with lower GA face a uniquely high risk of comorbidities and significant challenges of catching up with normal growth and development, making them more vulnerable to abnormal levels of thyroid hormones. 13
Preterm infants usually present with unique thyroid function patterns, such as a high proportion of delayed elevation of TSH concentration (dTSH) and transient hypothyroxinemia of prematurity, which requires repeat screening after the first neonatal screening. 14 –16 Our previous study also proposes the necessity of repeat screening in preterm infants due to the dynamic change of serum TSH and free thyroxine (fT4) in accordance with postmenstrual age after birth. 17,18
In recent years, the optimal time and adequate cut-offs for repeat screening of thyroid function in preterm infants has been widely debated. 19 As suggested by the 2020–2021 updated European CH consensus guideline, retesting at the second week of postnatal age (PNA) or 2 weeks (w) after the first screening is recommended in preterm and low BW infants. 11,20
However, it is found that 48% of the infants with dTSH might be missed if rescreening is performed only at the second week of PNA or before. 21 Besides, for those who undergo retesting only after the third week of PNA, the level of TSH might have reached a very high level, even up to 100 mU/L; thus, these neonates are neither able to obtain timely diagnosis nor able to obtain early treatment. 13
In addition, the recommendations of current guidelines lack high-quality evidence from large prospective cohort studies. Therefore, there is an urgent need for large clinical data from the early postnatal life to further explore the optimal screening pattern of CH in preterm infants, so as to prevent missed or delayed diagnosis.
This study was based on a prospective multicenter cohort with the specific primary objective of investigating the unique characteristics of thyroid function in very preterm infants (VPIs). Dynamic weekly screening of thyroid function within the first month after birth, and at 36 w of corrected age or before discharge was performed in each participant. This study aimed at providing reliable clinical real-world evidence for the early and timely diagnosis of CH, so as to avoid missing or delaying replacement therapy in preterm infants with different GA.
Participants and Methods
Study design and participants
This cohort was embedded in the Chinese Adverse Prognosis of Very Preterm infants (CARE-Preterm) cohort, a prospective multicenter cohort based on the clinical research database, Sino-northern Neonatal Network (SNN). SNN was initiated by Shandong Provincial Hospital affiliated to Shandong First Medical University on January 1, 2018, and it was authorized and managed by the Shandong Health Committee and the National Institute of Health Data Science of China.
As of 2022, up to 52 neonatal intensive care units across 6 provinces and autonomous regions with high geographical coverage, population base, and fertility rates in Northern China have joined the database. All VPIs born with GA <32 w or very low-birth-weight infants with BW <1500 g admitted to the participating institutes of SNN after January 1, 2018 were enrolled into the CARE-Preterm cohort.
In this study, we only included the VPIs admitted to the 52 participating institutes from January 1, 2019 to December 31, 2022. Infants who died or were discharged within the first week after birth without thyroid hormone results, or with apparent congenital malformations, or with incomplete data of thyroid hormones were excluded from this study.
Weekly measurement of serum thyroid function was performed within the first 4 w after birth, and at 36 w of corrected age or before discharge for each participating neonate, as reported in our previous study. 17 Information on the clinical characteristics, including maternal demographics data, pregnancy, delivery, infant hospitalization information, and serial thyroid hormone values of the included participants, was collected from the SNN database. The required data could be extracted by the corresponding author. The data were checked by specific SNN database staff to ensure the data quality submitted by each institute.
Detection procedure and explanatory variables
Serum was obtained to detect the concentration of serum thyroid hormones, including TSH, fT4, and free triiodothyronine (fT3). About 1–2 mL of blood was drawn weekly in the morning to perform thyroid function tests and other tests, depending on the medical needs of the infant. Electrochemiluminescence and chemiluminescence immunoassay assays were used for the measurement of serum TSH, fT4, and fT3 concentrations. Detailed detection strategies have been previously described. 17
In this study, the definition of thyroid dysfunction was taken from the European Society for Paediatric Endocrinology. 11 Infants with a serum TSH concentration exceeding 20 μIU/mL at any PNA during hospitalization were diagnosed with CH, and they were treated with levothyroxine even if fT4 concentrations were within the normal range.
If the infant showed normal TSH concentration during the initial thyroid function screening within the first week of PNA, but the concentration increased to more than 20 μIU/mL when retested in the subsequent weeks, a diagnosis of dTSH was made, with the initiation of treatment immediately.
Based on their peak serum TSH concentrations in serial measurements, infants were categorized into three groups: TSH <6, 6 ≤ TSH <20, and TSH ≥20 μIU/mL. The TSH <20 μIU/mL group comprised infants from both the TSH <6 and 6 ≤ TSH <20 μIU/mL groups, all of whom had a peak serum TSH concentration less than 20 μIU/mL.
Ethical approval
This study has been approved by the Ethics Committee of Shandong Provincial Hospital affiliated to Shandong First Medical University by appropriate processes (LCYJ: NO.2019-132 and SWYX: NO.2020-129). Informed consents is obtained from all the parents or guardians of the participants. Based on the SNN database, the cohort has been registered on the Chinese Clinical Trial Registry (registration number: ChiCTR1900025234 and ChiCTR2000037918).
This study is completed in accordance with the Declaration of Helsinki as revised in 2013. The clinical data of each participant are anonymous and encrypted, which conforms to the data protection law.
Statistical analysis
The categorical data were expressed by the number of cases and percentage (n, %), and the comparison between groups was carried out using the Chi-square test. The continuous data that did not conform to the normal distribution were expressed as median (interquartile range, Q1–Q3), and the Mann–Whitney U test was used for the comparison between the two groups. p < 0.05 was considered statistically significant. SPSS version 23.0 software was used for the statistical analysis of this study.
Results
A total of 6254 VPIs admitted to the 52 participating institutes from January 1, 2019 to December 31, 2022 were enrolled. After exclusions, 5992 VPIs were included and a total of 14,141 thyroid function test results were collected, averaging of 2.4 TSH values per infant. Among the participants, 956 (15.9%) infants were born with GA <28 w, 1921 (32.1%) were born with 28 w ≤ GA <30 w, and 3115 (52.0%) were born with 30 w ≤ GA <32 w (Fig. 1).
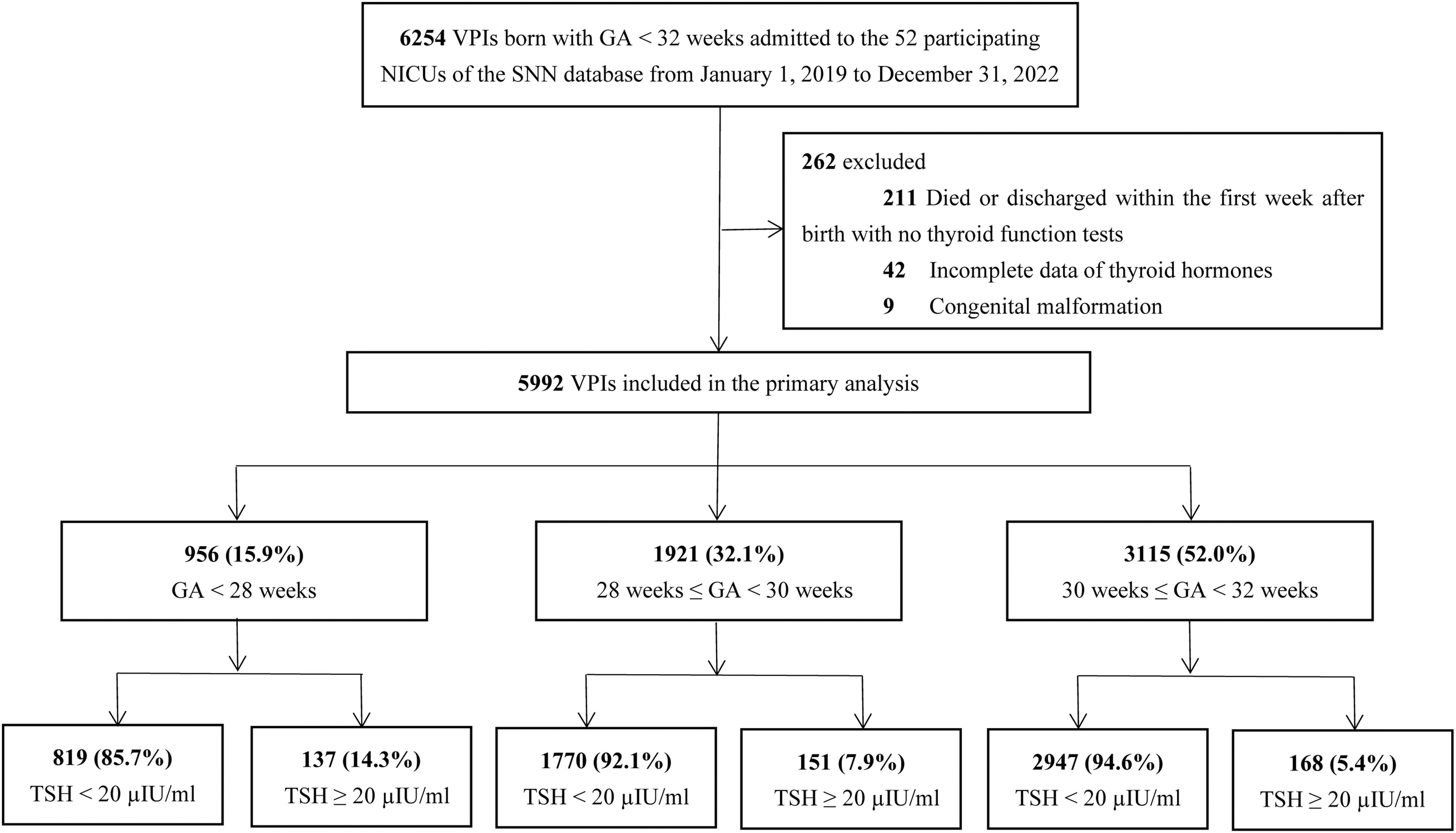
Flowchart of the study population. GA, gestational age; NICU, neonatal intensive care unit; SNN, Sino-northern Neonatal Network; TSH, thyrotropin; VPI, very preterm infant.
In this cohort, a total of 456 (7.6%) [95% confidence interval (CI), 6.9–8.3%] infants presented serum TSH ≥20 μIU/mL during hospitalization and were diagnosed with CH. When stratified by GA, 14.3% (137/956) with GA <28 w, 7.9% (151/1921) with 28 w ≤ GA <30 w, and 5.4% (168/3115) with 30 w ≤ GA <32 w were diagnosed with CH, respectively. Among the infants with CH, their BW was significantly lower compared with those with TSH <20 μIU/mL (non-CH). Moreover, among the infants with 28 w ≤ GA <30 w and 30 w ≤ GA <32 w, the serum fT4 concentration in the CH group was significantly lower than that in the non-CH group.
However, no statistical difference was found between the CH and non-CH group among the infants with GA <28 w. In addition, mothers in the CH group also presented a higher proportion of maternal hypertensive disorder of pregnancy (HDP) compared with the non-CH group (Table 1).
Infant and Maternal Characteristics by Gestational Age and Thyroid-Stimulating Hormone Concentrations (<20 vs. ≥20 μIU/mL)
Data are expressed as n (%) or median (IQR, Q1–Q3). Infants were categorized into <20 versus ≥20 μIU/mL groups according to their peak serum TSH concentrations in serial measurements.
There are significant differences between the TSH <20 μIU/mL group and TSH ≥20 μIU/mL group in the same GA groups by using Chi-square test or Mann–Whitney U Test. p < 0.05 is considered statistically significant.** p < 0.01.
AGA, appropriate for gestational age; BPD, bronchopulmonary dysplasia; BW, birth age; fT3, free triiodothyronine; fT4, free thyroxine; GA, gestational age; IQR, interquartile range; IVH, intraventricular hemorrhage; LGA, large for gestational age; M, median; PNA, postnatal age; PPROM, preterm premature rupture of membrane; ROP, retinopathy of prematurity; SGA, small for gestational age; TSH, thyrotropin; w, weeks.
After stratification according to GA, the proportion of infants with TSH ≥20 μIU/mL decreased gradually with the increase of GA from 16.9% (13/77) [CI, 8.3–25.4%] at GA <26 w to 4.8% (46/964) [CI, 3.4–6.1%] at GA 31 w. In contrast, the proportion of infants with serum TSH <6 μIU/mL increased significantly with advancing GA, rising from 26.0% (20/77) [CI, 16.0–36.0%] at GA <26 w to 52.0% (501/964) [CI, 48.8–55.1%] at GA 31 w (Fig. 2).
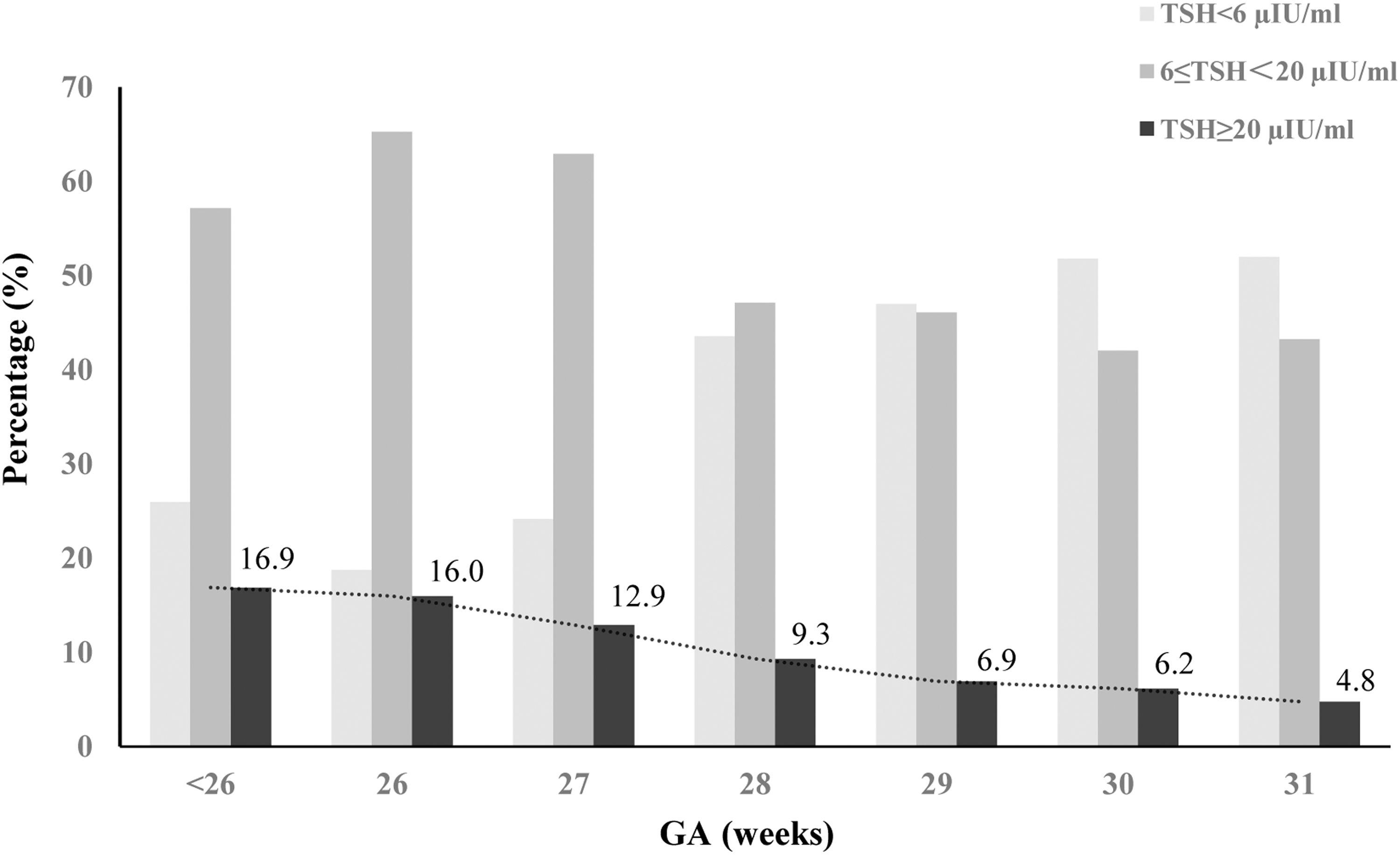
Categorization of TSH level into <6, ≤6–< 20, and ≥20 μIU/mL, and the percentage of each TSH group by GA among the whole cohort of VPIs. According to the peak serum TSH levels in serial measurements, infants were categorized into three groups: TSH <6, 6 ≤ TSH <20, and TSH ≥20 μIU/mL.
Among the infants with CH, our results showed a significantly high proportion of dTSH in each GA group, which was also closely associated with GA. For the infants with GA <26 w, only 17.4% (4/23) [CI, 0.6–34.2%] were diagnosed with CH during the first thyroid function screening within the first week after birth (PNA 1 w), while 82.6% (19/23) [CI, 65.8–99.4%] were diagnosed during the second and subsequent rescreening and were thus defined as dTSH. The proportion of dTSH decreased gradually with the increase of GA. Until GA 31 w, 38.1% (32/84) [CI, 27.5–48.7%] of the infants were diagnosed as dTSH (Fig. 3).
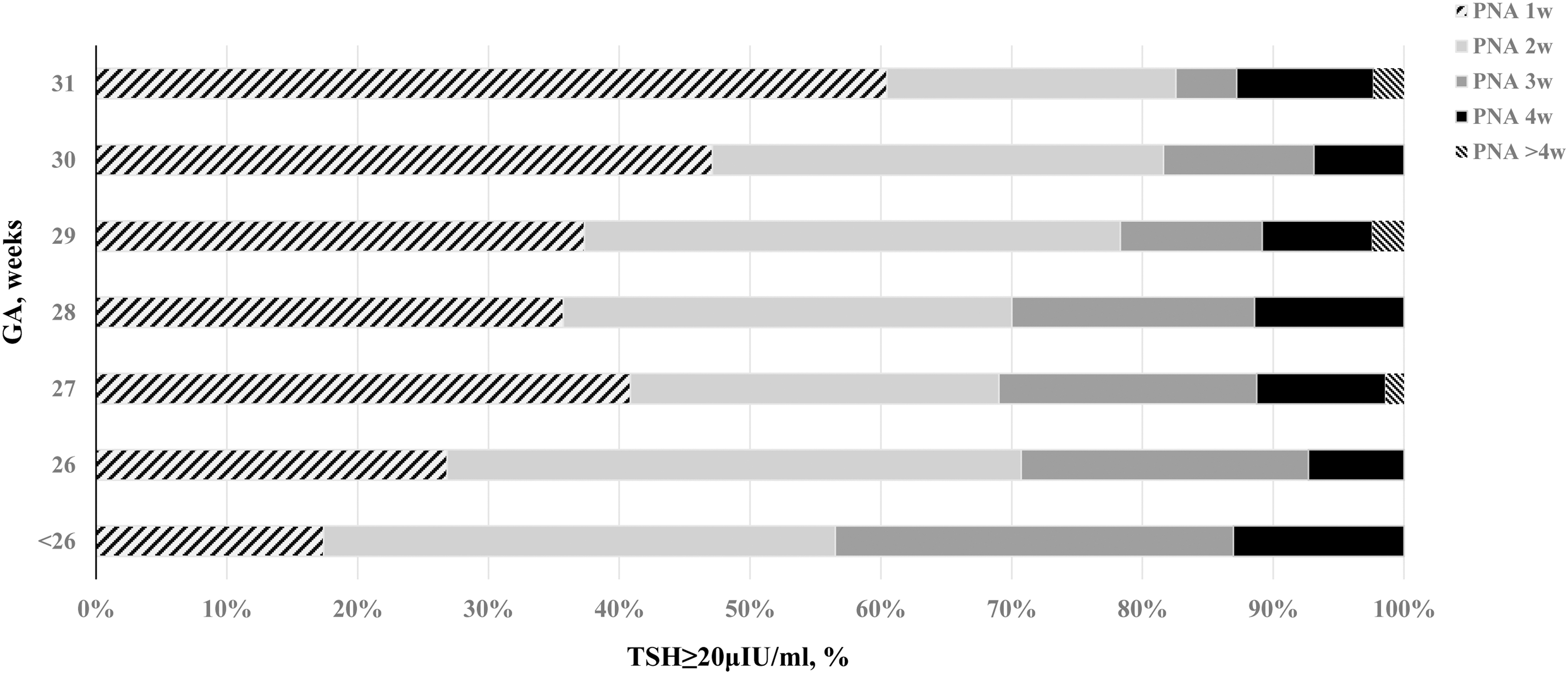
Proportion of CH diagnosed by weekly GA and PNA. CH, congenital hypothyroidism; PNA, postnatal age.
With weekly testing of thyroid function, only 42.3% (193/456) [CI, 37.8–46.9%] of CH cases were identified during the first week of PNA, and up to 57.7% (263/456) [CI, 53.1–62.2%] were diagnosed as dTSH after the first week. During the second, third, and fourth week of PNA, the cumulative rate of CH identified by rescreening was 76.1% (347/456) [CI, 72.2–80.0%], 90.6% (413/456) [CI, 87.9–93.3%], and 98.9% (451/456) [CI, 97.9–99.9%], respectively. Only 1.1% (5/456) [CI, 0.1–2.1%] were diagnosed after the fourth week of PNA (Fig. 4).
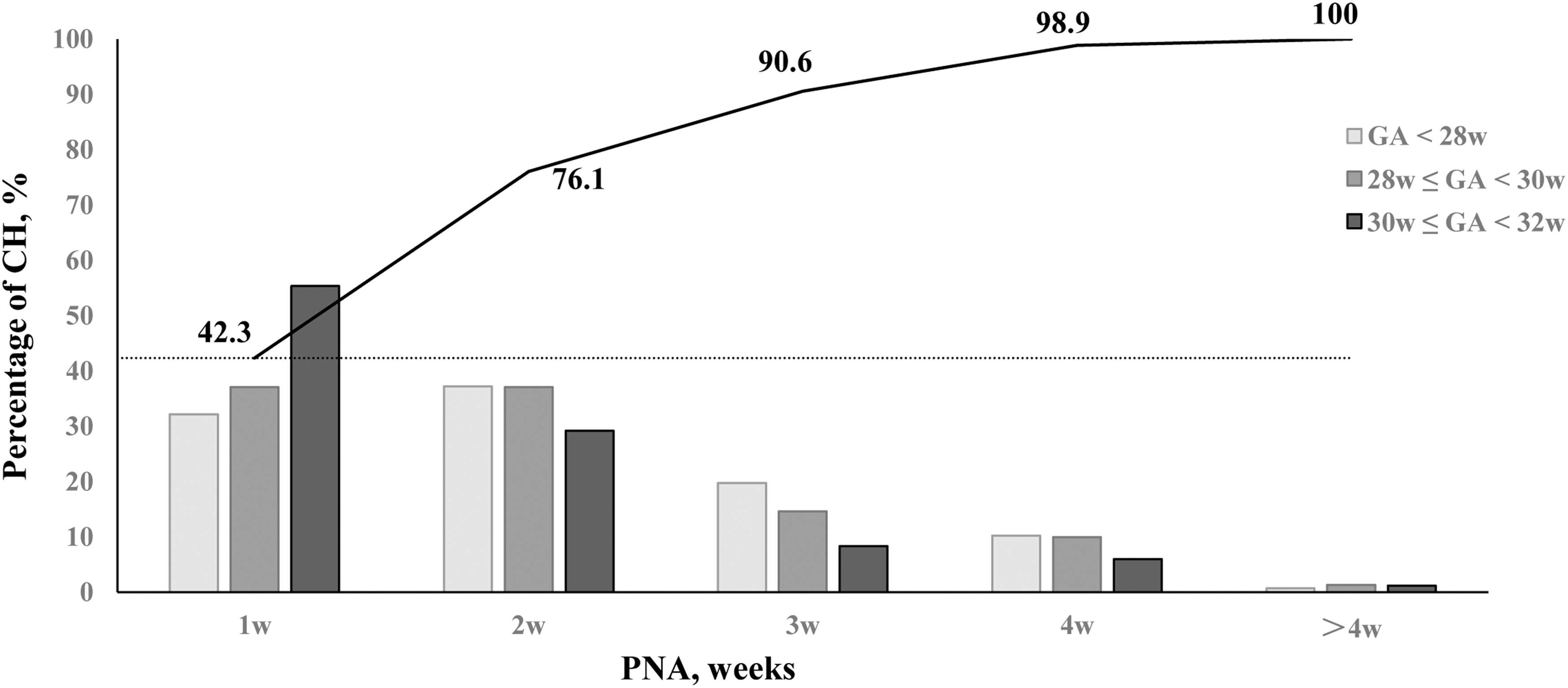
Percentage of CH identified by weekly PNA in different GA groups. Dashed line represents 42.3% of the CH subjects identified at the first week of PNA. Solid line represents the cumulative percentage of the whole CH group identified at different PNA by weeks. Space between the dashed line and the solid line represents the cumulative proportion of dTSH identified after the first week. dTSH, delayed TSH elevation; w, weeks.
Among the infants diagnosed with dTSH, 40.3% (106/263) [CI, 34.3–46.3%] and 13.7% (36/263) [CI, 9.5–17.9%] showed serum fT4 < 15 pmol/L and <10 pmol/L respectively at the initial screening before treatment, while none of them showed serum fT4 < 5 pmol/L.
Discussion
In this large prospective multicenter cohort study embedded in the CARE-Preterm cohort of the SNN database, we explored the unique characteristics of thyroid function pertaining to the diagnosis of CH in VPIs with different GA through weekly testing. Our observations unveiled a significant high prevalence of both CH and dTSH within preterm infants, both exhibiting a strong correlation with GA.
Moreover, our findings revealed an incremental growth in the cumulative diagnosis proportion of CH with the increase of PNA by weeks. Therefore, dynamic screening for CH by weeks within the first month post-birth was necessary to achieve timely diagnoses and early replacement therapy in VPIs with CH, especially those with lower GA.
In our study, the prevalence of CH is up to 7.6% among the VPIs cohort, which is significantly higher than that in term infants (0.05%). The prevalence of CH in preterm infants varies widely in different studies. 18,22,23 In the study reported by Kaluarachchi and colleagues, the overall prevalence of CH in 3137 VPIs is only 1.56%. 15
On the other hand, in the study reported by Kim and colleagues, the prevalence of CH is up to 19.4% among 180 VPIs, which is significantly higher than that in our study. 24 However, the exact prevalence of CH in preterm infants is still uncertain due to the un-unified cutoff value, screening method, and rescreening time for the diagnosis of CH, as well as the characteristics of the preterm population with different GA and BW. 5,18,25,26
Thus, large multicenter real-world studies with broad geographical and population coverage, such as our study, are needed urgently to obtain the accurate prevalence of CH in preterm infants with different GA around the world, and to formulate diagnosis and treatment guidelines applicable to the VPIs globally.
The CH of VPIs presented unique patterns in our study, which are different from term infants. First, the lower the GA and BW, the higher the prevalence of CH. The BW of the infants with CH is significantly lower than those with non-CH, and the proportion of CH in each GA group increases gradually with lower GA from 4.8% at GA 31 w to 16.9% at GA <26 w, which is consistent with previous studies. 13
In addition, before therapy, the serum fT4 concentrations in the CH group is statistically lower than those in the non-CH group with GA 28–30 w and GA 31–32 w. However, among the infants with GA <28 w, the fT4 concentrations in both the CH and non-CH groups are quite low. This indicates differing maturity levels of the hypothalamic-pituitary-thyroid (HPT) axis, especially the immaturity of the thyroid gland, in infants with birth GA <28 w and those with GA >28 w.
Further, the infants of the CH group also present a higher rate of maternal HDP than the non-CH group. Likewise, a high incidence of CH is also found in preterm infants born to mothers who suffered from HDP. In prior studies, we employed univariate and multivariate analyses to investigate the risk factors for CH in preterm infants, and we found that HDP might be an independent risk factor for CH. 27,28
These findings emphasize the importance of dynamic screening of thyroid function for preterm infants exposed to maternal HDP during pregnancy. Moreover, animal experiments are also needed to investigate the effect of maternal intrauterine exposure factors, such as HDP, on the development of the HPT axis in their offspring and the related mechanism.
Another unique pattern of CH in VPIs is the high ratio of dTSH, which accounts for 57.7% of the CH subjects in our study, and the rate increases with lower GA. Many studies have also reported a high ratio of dTSH in preterm infants with different GA. In another study report on 286 preterm infants with GA <30 w, 19 out of 26 (73.1%) infants with CH are diagnosed as dTSH, which is much higher than the VPIs in our study. 29
The high rate of dTSH could be attributed to the immature status of the HPT axis at different GA in preterm infants. 11,20,30 Therefore, optimized CH rescreening programs are crucial to prevent missed diagnoses of CH in preterm infants, especially for those with lower GA.
At present, the optimal time for retesting is still controversial. Retesting only once before the second week of PNA or after the third week may lead to missed or delayed diagnosis. 13,21 In our study, through weekly screening of thyroid function during the first 4 w of life, only 42.3% of the CH cases are identified by the first screening within the first week of PNA.
During the second, third, and fourth week of PNA, the cumulative detection rate of CH is 76.1%, 90.6%, and 98.9%, respectively. Among them, the ratio of dTSH identified by rescreening from the second to the fourth week of PNA is 33.8%, 14.5%, and 8.3%, respectively. Therefore, if the rescreening is only performed during the second week, about 23.9% of cases might be missed.
Similarly, for those only retested during the fourth week, about 33.8% may experience delayed treatment for at least 2 w, potentially leading to subtle neurocognitive disability. Thus, dynamic screening of thyroid function by weeks within the first month of life is of great significance to prevent missed and delayed diagnosis of CH in VPIs, especially in those with lower GA.
Currently, the approach to treating dTSH in VPIs is a debated topic. 31 Our study showed that 40.3% of VPIs with dTSH had low fT4 levels, indicating overt hypothyroidism that requires immediate treatment. On the other hand, the 59.7% with normal fT4 levels face uncertain treatment options. Some research sees dTSH as a mild and temporary condition that does not impact their long-term outcomes, hence negating the need for treatment. 32,33
However, other studies discovered that the TSH level in preterm infants with dTSH could rise to more than 100 μIU/mL, with some infants even demonstrating permanent TSH elevation, indicative of relatively deficient in thyroid hormones. 34 Moreover, some studies also assert that even mild abnormality in TSH concentration may lead to poorer neurodevelopment. 1,35
Given these findings, there is significant merit in conducting longitudinal studies to further investigate the beneficial effect of repeat screening and early therapy on growth and neurocognitive outcomes in VPIs with dTSH.
There are strengths in this study. Weekly screening of thyroid function was performed on each participant to provide data from a large cohort of VPIs. In addition, this study was designed as a prospective multicenter cohort study underpinned by a clinical research database.
This framework ensured the authenticity, accuracy, and reliability of our data under strict data quality control, so as to provide trustworthy evidence for the investigation of the unique patterns of thyroid function in preterm infants. Thus, this study could provide high-quality and reliable baseline data on thyroid hormones from a large preterm cohort, thereby enhancing our understanding of the unique thyroid function patterns in preterm infants with different GA, so as to achieve timely diagnosis of CH in these infants.
There are also limitations. This study was a multicenter study including 52 participating institutes with different measurement methods, agents, and instruments for the testing of thyroid function, which could cause heterogeneity on the results. In our previous study, we had analyzed the impact of different measurement methods on the overall result of thyroid function, and no significant difference was found in the results. 17
In addition, our study was an observational real-world study, leading to the problem of missing data. Not every participant managed to complete the four tests within the first month post birth. However, the large sample size of this cohort could effectively reduce the bias caused by the missing data.
Further, weekly testing of thyroid function was only performed for the first 4 w after birth and again at 36 w of corrected age or discharge. This left a possibility that additional transient CH cases, occurring between the first 4 w and discharge, might have been missed. Therefore, further studies with larger sample size are required to explore the natural history of CH beyond the first month of life in preterm infants.
Conclusion
Based on the large real-world data, our study confirms that dynamic screening of thyroid function by weeks within the first 4 w after birth might effectively avoid missed and delayed diagnoses of CH in VPIs. However, the selection of specific screening methods and therapeutic protocols should be tailored based on their clinical conditions, especially for critically ill preterm infants.
These findings may provide reliable high-quality evidence for the assessment of thyroid function in preterm infants with different GA. Further, it is also expected to steer clinicians toward making timely diagnosis and early initiation of replacement therapy of CH, so as to avoid adverse prognosis.
Footnotes
Acknowledgments
The authors sincerely appreciate all the clinical medical experts, epidemiological experts, statistics experts, and study participants of the SNN database and the CARE-Preterm cohort study group for their contributions to data collection and quality control, research design, and data analysis.
Authors' Contributions
Y.Y. and J.Z.: review and editing—directed the study, analyzed the data, and revised the article (equal). R.S.: writing—collected and analyzed the data (equal), and drafted the article (lead). S.R.: writing—edited the language and grammar, and drafted the article (equal). J.J., B.W., F.L., X.L., D.Y., Z.L., H.H., X.S., Q.L., H.L., J.H., J.Y., and M.Z.: contributed to data collection, submission, and verification to Shandong Neonatal Network database (equal). All authors have contributed equally to this work and share the first authorship, and approved the submitted version for publication.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by a cross-disciplinary project, “Impact of Pulmonary Surfactant on Preterm Infants with Neonatal Respiratory Distress Syndrome,” sponsored by Beijing Yaoling Information Technology Co., Ltd. The funder was not involved in study design, execution, data collection/storage, data analysis, or the writing of the article.