
Abstract

T
A 35-year-old woman presented with a suspicious 13 mm thyroid nodule and right laterocervical nodes. Calcitonin and carcinoembryonic antigen (CEA) levels were 2300 pg/mL (N < 10) and 21 ng/mL (N < 3.5), respectively, in favor of MTC. 18F-dihydroxyphenyl-alanine positron emission tomography showed high uptake in the thyroid nodule and laterocervical nodes, while millimetric lung nodules did not show any uptake. Total thyroidectomy with neck dissection revealed a pT3N1bMx MTC. Ki-67 was 10%. Germline genetic screening identified a RET-L790F pathogenic variant. During the follow-up, she presented with a locoregional progression with laterocervical nodes. Both calcitonin and CEA increased with a doubling time of 12 and 15 months, respectively.
Imaging identified a suspicious left iliac bone lesion 23 months after the diagnosis, treated by cryoablation. As the patient progressed with distant metastases, somatic analysis was performed on the thyroid specimen, showing a somatic RET-M918T. No variations were founded on cancer-related genes ALK, FGFR1, FGFR2, FGFR3, HRAS, KRAS, JAK1, JAK2, JAK3, and MET. At last follow-up, 6 years after surgery, calcitonin and CEA were 6566 pg/mL and 84.2 ng/mL, respectively (Fig. 1). As imaging showed a stable metastatic disease, the multidisciplinary team recommended a wait-and-watch approach with no systemic treatment. Catecholamines, calcium, and parathormon levels all remained normal. Family screening revealed four RET-L790F carriers aged 12–68 years, with normal calcitonin and neck ultrasound. No thyroidectomy was performed.
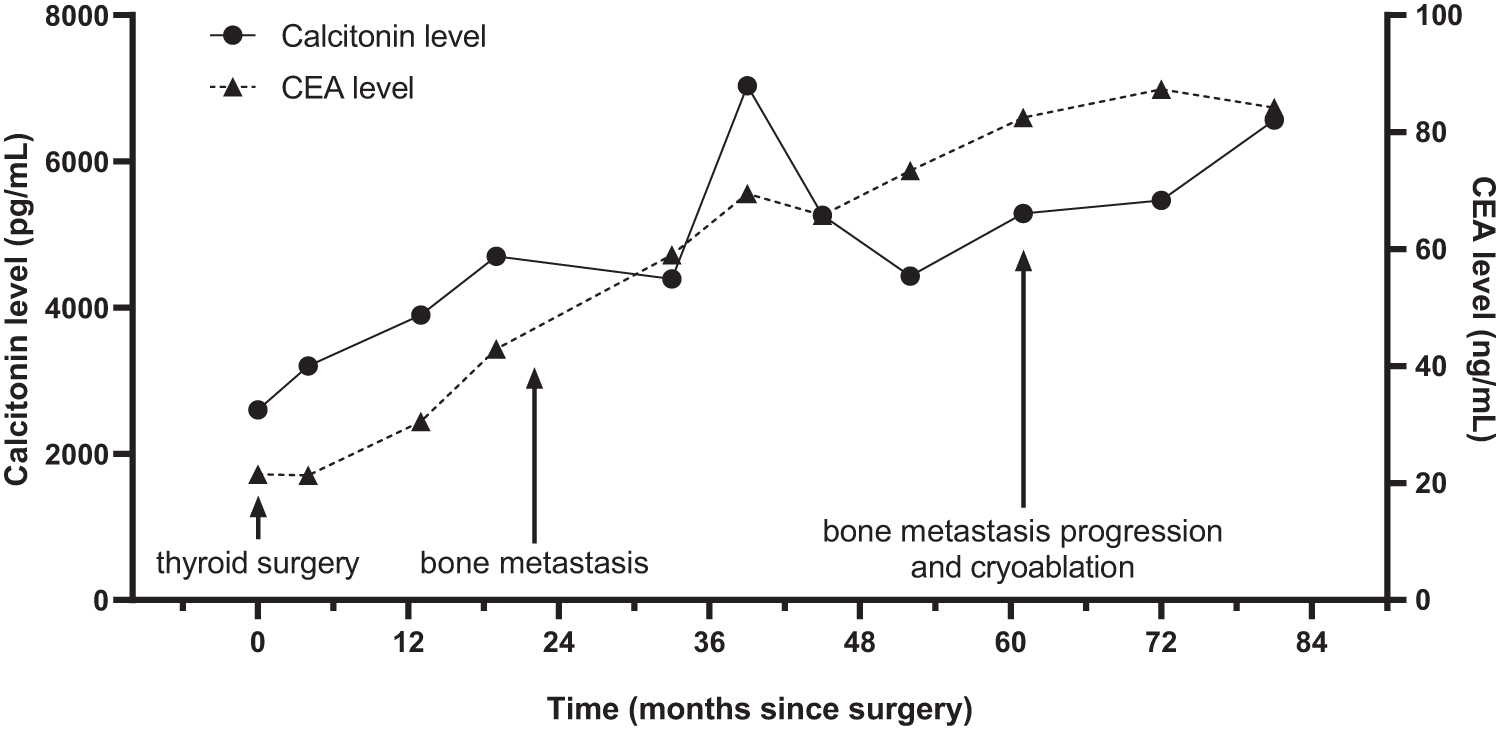
Evolution of calcitonin and CEA levels and treatments from the time of diagnosis to last follow-up. CEA, carcinoembryonic antigen.
Most studies reporting the natural history of RET-L790F-related MTC suggested an indolent disease. A French multicentric study involving 77 RET-L790F MEN2A patients reported no distant metastases, and lymph node invasion in only 10/55 (18.2%) operated patients (mean age 32 years). After a follow-up of 89 months, most patients were cured. 2 In contrast, several studies reported that somatic RET-M918T is a main driver of tumorigenesis in nonhereditary MTC, leading to a more advanced stage at diagnosis and a worse outcome. 3
Concomitant somatic and germline RET mutations in MEN2-related MTC have been rarely reported. Lombardo et al. described a 12-year-old girl exhibiting an extensive and invasive MTC despite a germline moderate risk 804 RET variant, leading to the identification of a somatic RET-M918T. 4 A somatic RET-M918T was also identified in 4 MEN2A MTCs with germline 634, 618, and 620 variants. 5 More recently, while no somatic RET mutation had been identified, a somatic variant in FTL3 (a transcription factor involved in growth and differentiation) was reported in a RET-L790F carrier with metastatic progression few years after the diagnosis of a locoregionally advanced MTC. 6
To our knowledge, this is the first report highlighting the potential additional role of a somatic RET-M918T in a patient with a germline RET-L790F, who rapidly developed metastases. Further studies should determine whether MEN2 patients with an atypical MTC phenotype should be tested from a somatic viewpoint, and how this could individualize our follow-up strategies in MEN2 patients.
Footnotes
Acknowledgments
We thank Pr. Taieb, Pr. Sebag, Dr. Guerin, Pr. Brue, and Dr. Morange for fruitful discussion. We thank Dr. Isabelle Nanni for somatic cancer-related genes sequencing. And we thank Ian Darby (Editing BioMed) for English editing.
Authors' Contributions
Writing—original draft (lead) and review and editing (equal) by N.S. Writing—original draft (supporting) and review and editing (equal) by P.R. Review and editing (equal) by D.M.-P. and N.C.P. Conceptualization (lead) and review and editing (equal) by A.B. Writing—review and editing (lead) by F.C.
Patient Statement
The research was completed in accordance with the Declaration of Helsinki as revised in 2013 and was approved to the APHM RGPD IRB. The patient has given consent for the publication of this case report.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
N.S. received financial support from the French Endocrine Society (Société Française d'Endocrinologie, SFE). The other authors have no funding information to declare.