
Abstract

A
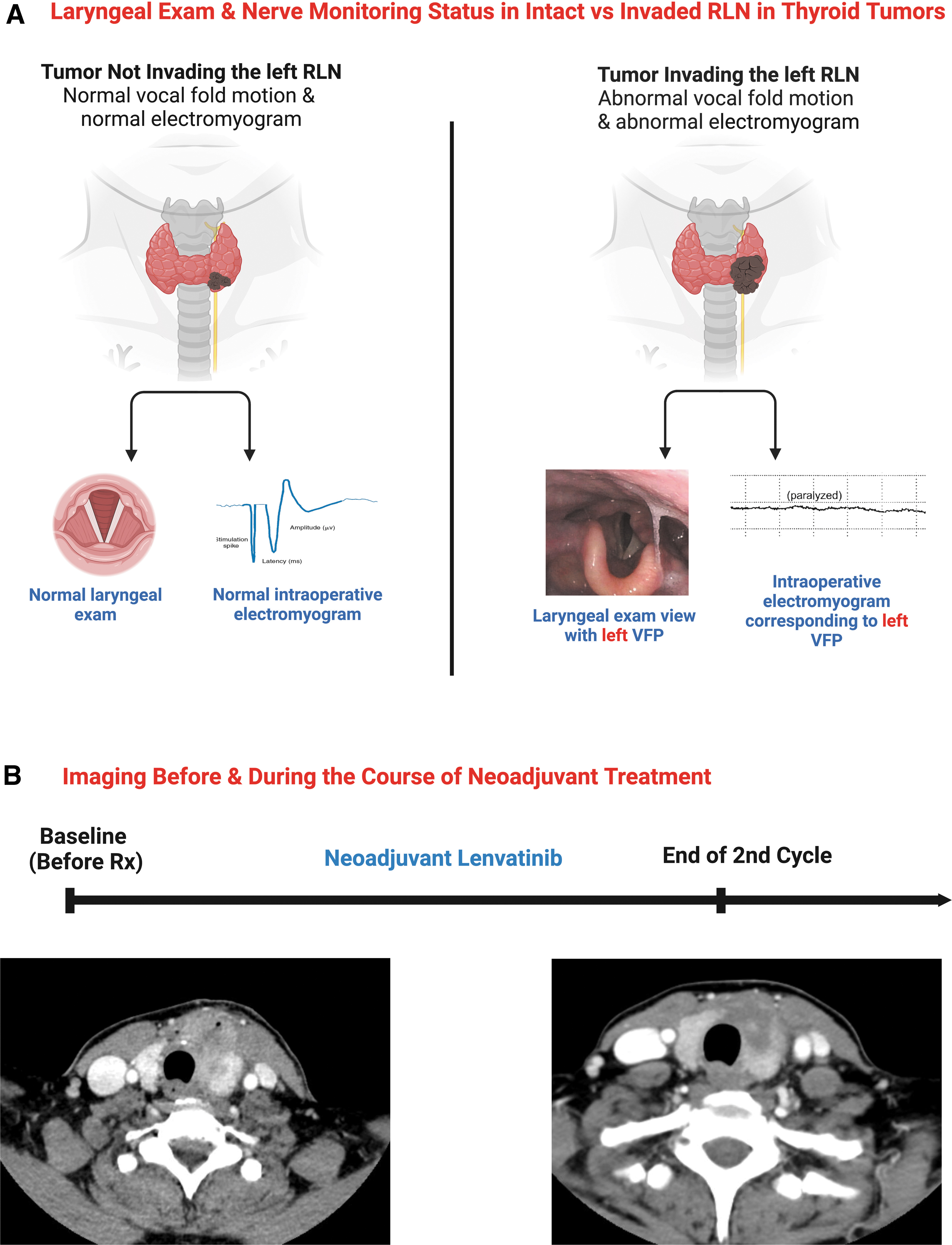
While preoperative VFP is highly suggestive of RLN invasion, normal voice or laryngeal exam does not exclude RLN invasion at surgery. Neural monitoring studies have shown that an invaded RLN may maintain electrophysiologic activity and therefore some degree of laryngeal function. 6 The term “Lazarus Effect” refers to the biblical story of Lazarus who was raised from the dead and given the resumption of vocal function we documented in these advanced thyroid cancer patients undergoing neoadjuvant therapy.
Our aim is to assess if the use of neoadjuvant therapy in patients diagnosed with advanced thyroid cancers and VFP could facilitate the recovery of vocal fold (VF) motion after paralysis, or the surgical preservation of invaded RLNs.
This study is a multicenter, retrospective real-world chart review approved by the Institutional Review Board (Protocol No. 2021P002754) at Mass General Brigham and was determined a minimal risk study due to the de-identified retrospective chart review nature of the study. Study investigators retrospectively abstracted de-identified data separately at each center from Massachusetts Eye and Ear Infirmary/Massachusetts General Hospital, Harvard University, Boston, MA; MD Anderson Cancer Center in Houston, TX; University of Virginia, VA, and University of California, San Francisco, San Francisco, CA.
We evaluated patients' medical records who met our criteria: age ≥18 years; diagnosed with a histologically confirmed advanced thyroid carcinoma (of any histology); had tumor tissues tested for actionable somatic genetic alterations of clinical interest (mutations, fusions, etc.) using academic or commercial next-generation sequencing platforms; underwent a pretreatment transnasal flexible fiberoptic examination (FOE) documenting a VF paresis/paralysis; received systemic anticancer (targeted and/or immune-) therapy (outside of clinical trials); underwent FOE during/after treatment; underwent surgery (January 2017–December 2021) using intraoperative nerve monitoring (Fig. 1A).
(
The primary outcome was the return of VF motion confirmed by FOE as a dichotomous state (normal or abnormal) motion by each site investigator. Secondary outcomes were median time-to-return of laryngeal function after neoadjuvant therapy, frequency of surgical preservation of invaded RLNs, and percentage of patients who experienced clinically significant adverse events (AEs) requiring dose adjustment and/or treatment interruption.
Descriptive statistics were reported as numbers and percentages of patients for categorical variables and mean with standard deviation, or median with range for continuous variables. All analyses were conducted using GraphPad Prism version 9.3.1.
Baseline Patient Characteristics
We identified seven patients who met eligibility criteria for this study. The mean age at diagnosis was 65 (±13) years. Three patients were females (42.9%). Six patients (85.7%) were diagnosed with anaplastic thyroid carcinoma (ATC), and one patient (14.3%) was diagnosed with advanced papillary thyroid carcinoma (PTC). BRAFV600E mutations were detected in all seven patients (100%), TERT promoter mutations were detected in four patients (57.1%), PIK3CA mutations in two patients (28.6%), and TP53 mutations in two patients (28.6%), Supplementary Table S1.
Neoadjuvant Treatment Characteristics
Six patients with ATC received dabrafenib (150 mg twice daily)/trametinib (2 mg daily), and one patient with advanced PTC received lenvatinib (24 mg daily) as the 1st line of therapy. The median number of cycles received in the 1st line of neoadjuvant therapy was 3 cycles (range, 1–13.5). Three patients (42.9%) (all diagnosed with ATC) subsequently received immunotherapy (pembrolizumab, 200 mg intravenously on day 1 of each cycle) in combination with dabrafenib/trametinib for a median of two additional cycles (range, 1–3). Overall, the median number of cycles of all neoadjuvant therapy received per patient regardless of therapy type was 4 cycles/patient. Neoadjuvant treatment was stopped before surgery to decrease intraoperative bleeding risk and allow for appropriate wound healing according to the time window of each targeted therapy used for each patient. One patient received 40 Gy of external beam radiation therapy before receiving dabrafenib/trametinib.
Two ATC patients receiving dabrafenib/trametinib developed AEs requiring treatment interruption and dose reduction: one patient due to suspicion of pulmonary embolism; the other patient due to fever and confusion. Figure 1B compared computed tomography scans before and after receiving 2 cycles of lenvatinib for the PTC patient.
Study Primary Outcome: Return of VF Motion
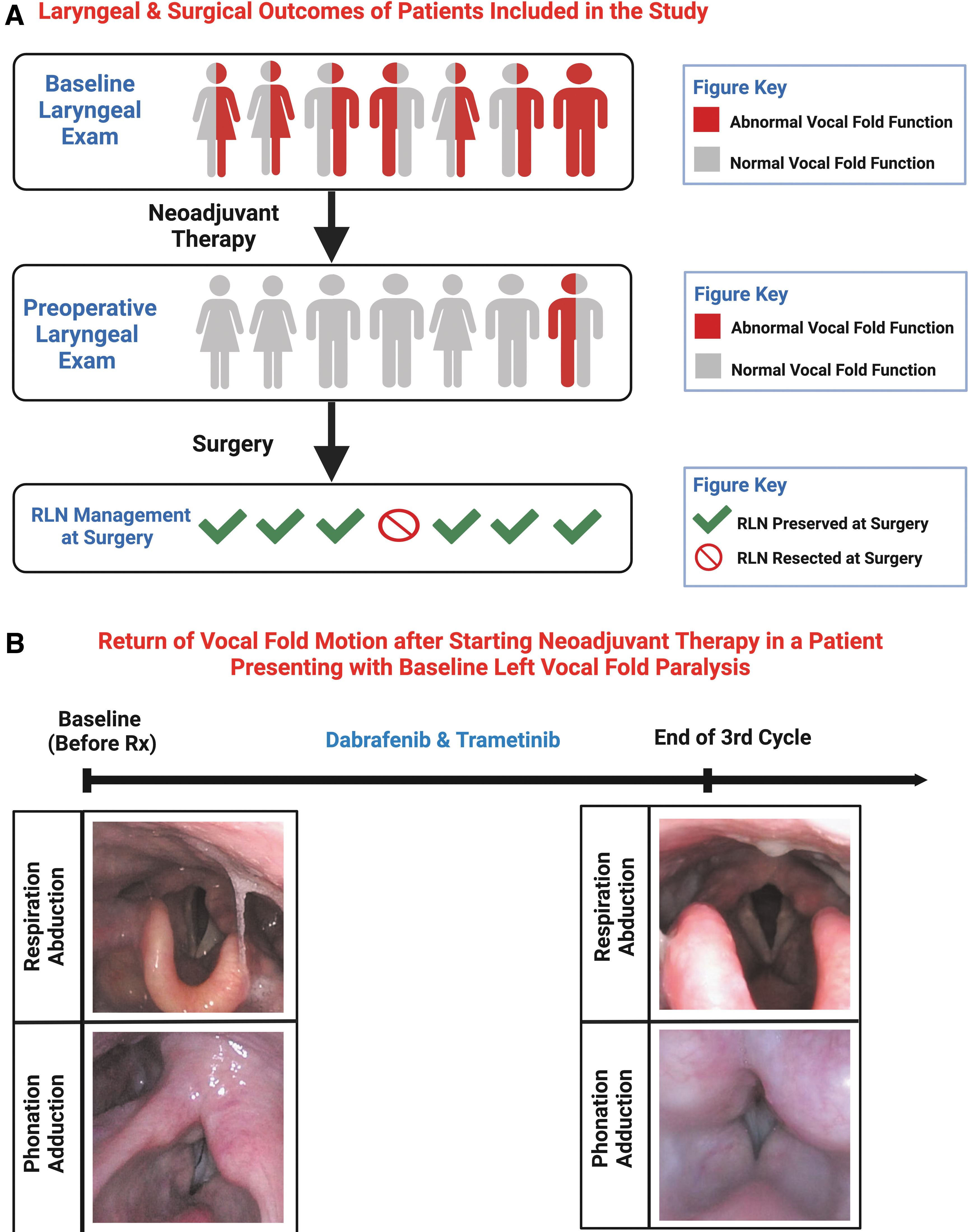
Baseline FOE was performed before initiating neoadjuvant therapy. Six patients had unilateral VFP, while a patient had bilateral VF involvement (right VFP and left VF hypomobility). Figure 2A depicts the side of each VFP for all patients. A total of 2 right VFP and 6 left VFP were included in our study.
(
Subsequent serial FOE was performed during and after neoadjuvant therapy. One patient (14.3%) regained VF mobility within 1 month and five patients (71.4%) regained mobility after 3 months of therapy. By 13.5 months, all patients (100%) regained VF mobility. Median time-to-return of VF mobility was 3 months (range, 1–13.5). Recovered RLNs were surgically preserved in six patients (85.7%). Figure 2B documents the resumption of VF motion after initial paralysis in a patient diagnosed with ATC after receiving 3 cycles of dabrafenib/trametinib.
To our knowledge, this is the first report dedicated to studying the return of laryngeal function as a standalone outcome in patients diagnosed with advanced thyroid cancers with invaded RLNs. Herein, we report the resumption of VF motion in patients who initially presented with VFP due to advanced thyroid cancers and the subsequent preservation of these RLNs when surgery was done regardless of pathology, underlying genetic alterations, or type of neoadjuvant therapy used. Neoadjuvant therapy in the setting of advanced thyroid cancer not only allowed for function-preserving surgery but also allowed for surgery itself to be an option.
There is no formal definition of advanced thyroid cancer. However, size and extrathyroidal extension are important factors in assessing clinical morbidity. Similarly, there is no clear definition of unresectable thyroid cancer, as it depends on the surgical challenge and morbidity associated with the extent of disease that must be resected to achieve the ideal R0 resection (surgical margins free from both microscopic and macroscopic tumor).
Preoperative VFP and/or anticipated RLN involvement meaningfully impact surgical planning and preoperative counseling because of increased risk of bilateral VFP and potential tracheotomy. Strategies to mitigate the risk of bilateral VFP and its associated morbidity warrant special consideration as the benefit of complete oncologic resection (R0 resection) must be weighed carefully against the potential for bilateral VFP. This is especially salient if the resection of an invaded RLN to achieve complete tumor extirpation may not confer survival benefit. 1,7,8
Recent progress in elucidating the oncogenic molecular underpinnings of thyroid carcinomas and the development of targeted therapies has shifted the landscape of advanced thyroid cancer management. Prediction of clinical behavior based on specific molecular features is an active area of interest. 9
At present, R0 surgical resection followed by adjunctive therapy including radioiodine therapy and/or external beam radiation remains the gold standard treatment for advanced thyroid cancer. However, in cases where R0 resection is not feasible or is associated with excessive surgical morbidity, neoadjuvant treatment may lessen surgical morbidity and allow inoperable tumors to become surgically manageable. Neoadjuvant targeted therapy is being increasingly considered for treatment of ATC and advanced MTC and differentiated thyroid cancer with several clinical trials currently underway (NCT04759911, NCT04675710, NCT04739566, and NCT04321954) as examples. 10
Important limitations of our study include the sample size, lack of true denominator, and survival bias (patients who met eligibility criteria may have had a favorable trajectory leading to survival bias, i.e., patients with aggressive disease who did not respond to therapy did not meet the eligibility criteria). Although referral bias may limit our ability to generalize the results, we believe that the multidisciplinary nature of the care provided to the patients provided meaningful change to the outcome of the patients included in this study. Finally, our understanding of the optimal timing of neoadjuvant therapy initiation and the number of cycles to be received before moving to surgery is still nascent.
In conclusion, we report the return of VF motion after initial VFP in seven patients diagnosed with advanced thyroid cancers after receiving neoadjuvant targeted therapy—challenging the assumption that carcinomatous neural invasion is always permanent and suggesting a more dynamic invasive pathophysiology than previously understood. Most patients had return of function within 3 months and had a sufficient clinical response to allow surgical preservation of most RLNs. Serial laryngoscopic examination during neoadjuvant therapy may guide surgical strategy and impact surgical timing. Laryngeal function assessment may be considered as a potential outcome for neoadjuvant clinical trials in thyroid cancers (we are currently testing as a secondary outcome in [NCT04321954]). 10 Future research is needed to further validate our results.
Footnotes
Acknowledgments
G.W.R. would like to acknowledge the ongoing philanthropic support of Mike & Eliz Ruane, John & Claire Bertucci, Ben & Ellen Harvey, and Diana Ryan for his research efforts.
Authors' Contributions
A.S.K.: Conceptualization, methodology, visualization, writing original draft, reviewing, and editing. A.H.A.A.: Conceptualization, ethical approval, methodology, visualization, writing original draft, reviewing and editing, project management. Z.F.: Methodology, visualization, reviewing, and editing. M.R.: Methodology, visualization, writing original draft, reviewing, and editing. D.C.S.Jr., A.I., M.C., J.J.S., N.K., and J.C.P.: Methodology, reviewing, and editing. L.J.W.: Conceptualization, methodology, writing original draft, reviewing, and editing. M.E.Z. and G.W.R.: Conceptualization, methodology, reviewing, and editing.
Author Disclosure Statement
A.S.K., A.H.A.A., Z.F., MR., D.C.S.Jr., A.I., J.J.S., and N.K.: No conflicts of interest to disclose. M.C.: Honoraria: Loxo/Lilly; Consulting or Advisory Role: Loxo, Ignyta; Research Funding: Kura Oncology, Eisai, Roche/Genentech, Exelixis, Merck. J.C.P.: Consulting or Advisory Role: EMD Sorono, Coherus, Selecxine, GC Cell. L.J.W.: Consulting or Advisory Role: Merck, Loxo, Blueprint Medicines, Eisai, Lilly, Bayer, Exelixis; Research Funding: Checkmate Pharmaceuticals, Lilly, Ayala Pharmaceuticals, Eisai; Expert Testimony: Eisai. M.E.Z.: Research Funding: Merck, Eli Lilly. G.W.R.: Research Funding: Eisai, Medtronic, Fluoptics. Administrative roles: President of the International Thyroid Oncology Group (ITOG), President of the World Congress on Thyroid Cancer (WCTC), Chair of the Administrative Division of the American Head and Neck Society (AHNS) and the Governor of the American College of Surgeons (ACS)-Otolaryngology. Other authors have no conflicts of interest to disclose.
Funding Information
This project received no funding.
Supplementary Material
Supplementary Table S1