
Abstract
Background:
Patients with metastatic medullary thyroid cancer (MTC) who progressed under tyrosine kinase inhibitors can benefit from an alkylating agent such as dacarbazine or temozolomide.
Patient Findings:
We describe two patients with metastatic MTC who developed a hypermutant phenotype after alkylating agent treatment. This phenotype was characterized by a high tumor mutational burden (TMB) and a mutational signature indicative of alkylating agent mutagenesis (single-base substitution 11). Both patients received immune checkpoint inhibitors, with partial morphological responses, clinical benefit, and progression-free survival of 6 and 9 months, respectively.
Summary and Conclusions:
Based on the described observations, we suggest that a hypermutant phenotype may be induced after alkylating agent treatment for MTC and the sequential use of immunotherapy should be further explored as a treatment option for MTC patients with increased TMB.
Introduction
Medullary thyroid cancer (MTC) is a rare neuroendocrine cancer arising from the parafollicular C cells of the thyroid, characterized by frequent molecular alterations in the RET oncogene. 1 The current standard treatment for metastatic patients requiring systemic therapy is multikinase inhibitors (MKi) vandetanib or cabozantinib, whatever their RET status, following the results of the two phase III trials, ZETA and EXAM, respectively. 2,3 For RET-altered MTC, the selective RET inhibitors (RETi), selpercatinib and pralsetinib, have demonstrated promising results in phase I/II studies 4,5 and are being evaluated in phase III trials compared with MKi.
MKi and RETi have replaced conventional chemotherapy for the treatment of MTC patients. However, alkylating agents may still be useful for patients who experience disease progression under these drugs and/or have contraindications and/or experience toxicities. 1 Although evidence supporting the use of conventional chemotherapies for MTC is limited to small retrospective studies, dacarbazine (DTIC), an alkylating agent, combined with 5-fluorouracil (5-FU), can provide partial responses (PRs) in 15–60% of the cases. 6 –10 Temozolomide (TMZ), the oral form of DTIC, although commonly used in neuroendocrine tumors (NETs), 11 was reported to be used in combination with capecitabine, in only one MTC patient to date. 12 DTIC or TMZ is known to have the ability to deposit methyl groups at the O6 position of guanine on DNA, causing mismatch pairing during replication, leading to genomic instability and eventually cell death. 13
More recently, TMZ has been reported to be associated with a hypermutant phenotype in different type of cancers, including NET, with some reported response to immune checkpoint inhibitors. 14 –18
In this study, we describe two patients with metastatic MTC who developed an alkylating agent-associated hypermutant phenotype with high tumor mutational burden (TMB) and response to immune checkpoint inhibitors. Both patients provided written consent for genomic analyses, and the patient still alive agreed for utilization of clinical data for research purpose after oral and written information in the context of TUTHYREF clinical research database. Further ethical review and approval were waived for this study.
Patients
Patient 1 was a 56-year-old female with a familial, germ line RET C611W mutated, metastatic MTC. The patient underwent a total thyroidectomy and lymph node dissection in 2009 for a 35-mm low-grade (WHO 2022) MTC with 37 metastatic lymph nodes, staged pT2(m)N1bM0. Follow-up revealed multiple bone and pulmonary metastases 1 year after the diagnosis, and liver metastases 4 years later. Multiple locoregional treatments to the bone (radiation, cryotherapy, and/or radiofrequency ablations) were performed throughout the patient's history. Systemic treatment was introduced 2 years after diagnosis for progressive and symptomatic metastatic disease (Fig. 1).
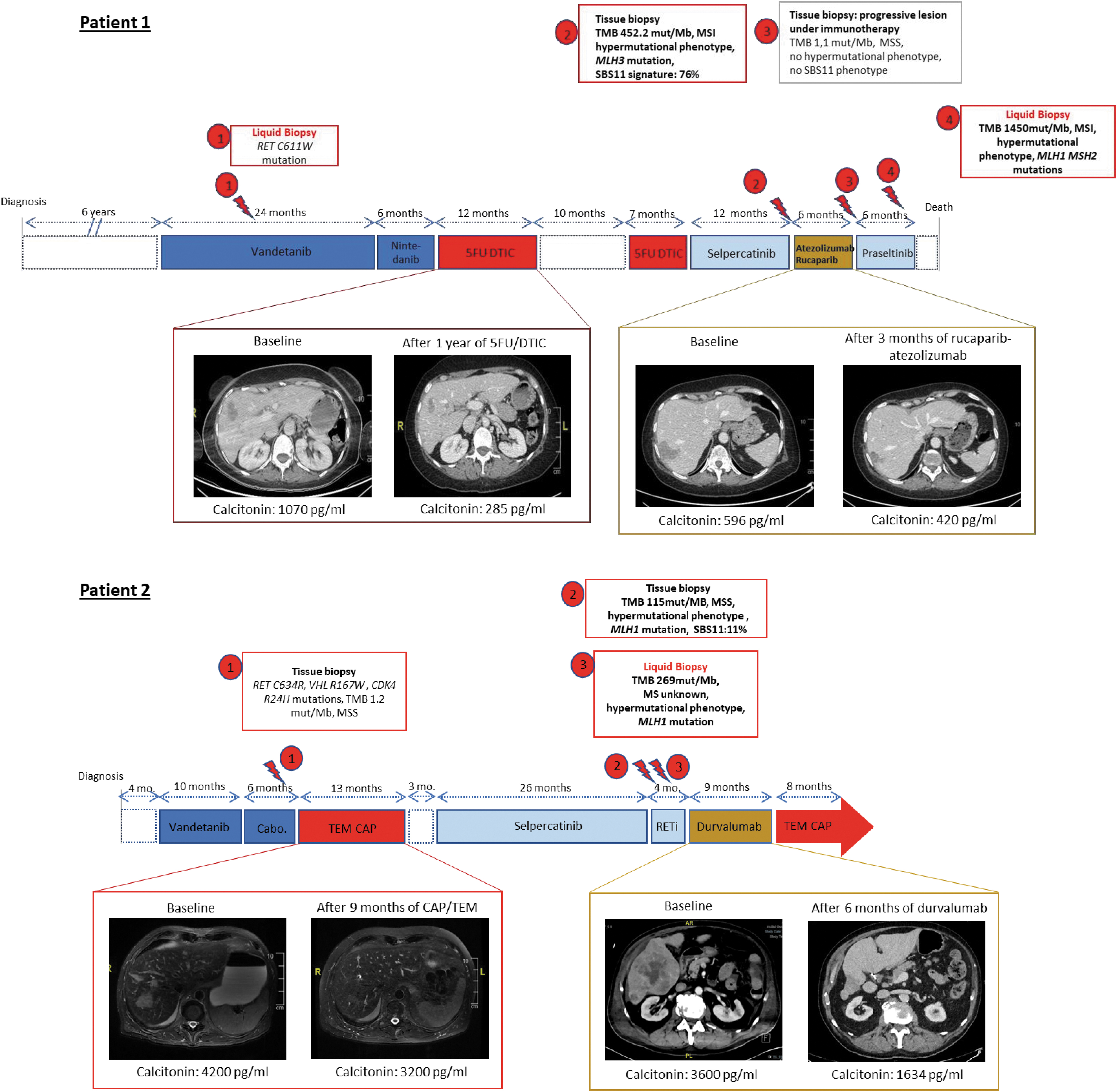
Time line of biopsies and treatments. For patient 1: biopsy number 1: liquid biopsy, Ion AmpliSeq™ Cancer Hotspot Panel v2 (50 genes); biopsy 2: tissue biopsy, WES, PFMG 2025; biopsy 3: tissue biopsy, WES, PFMG 2025; biopsy 4: liquid biopsy, FoundationOne Liquid CDx (324 genes, including TMB and MS-S). For patient 2: biopsy number 1: tissue biopsy, FoundationOne DX1 (324 genes, including TMB and MS-S); biopsy 2: tissue biopsy, WES, PFMG 2025; biopsy 3: liquid biopsy, FoundationOne Liquid CDx. Cabo., cabozantinib; DTIC, dacarbazine; MS, microsatellite; MS-I, MS-instable; MS-S, MS-stable; PFMG, Plan France Médecine Génomique; SBS, single-base substitution; TEM-CAP, temozolomide–capecitabine; TMB, tumor mutational burden; WES, whole-exome sequencing.
At that time, liquid biopsy revealed only the RET C611W mutation (Fig. 2). The patient sequentially received vandetanib for 26 months (best response: PR according to RECIST 1.1) and nintedanib (in the clinical trial NCT01788982) for 6 months (best response: PR). At the time of progression under nintedanib, she was found to have massive, painful bony metastatic spread of disease. The patient was then treated by fluorouracil and DTIC (5-FU: 400 mg/m2 for 5 days, DTIC 200 mg/m2 for 5 days, 28-day cycle) for 12 cycles. The O6-methylguanine-DNA methyltransferase (MGMT) H-score performed by immunohistochemistry was low on two different pathological samples (10 and 0/300). Importantly, she experienced major clinical benefit with pain relief and a drastic reduction in painkiller use, thereby enabling a return to normal activity. This PR (−31% according to RECIST 1.1) lasted for 10 months (Fig. 1).
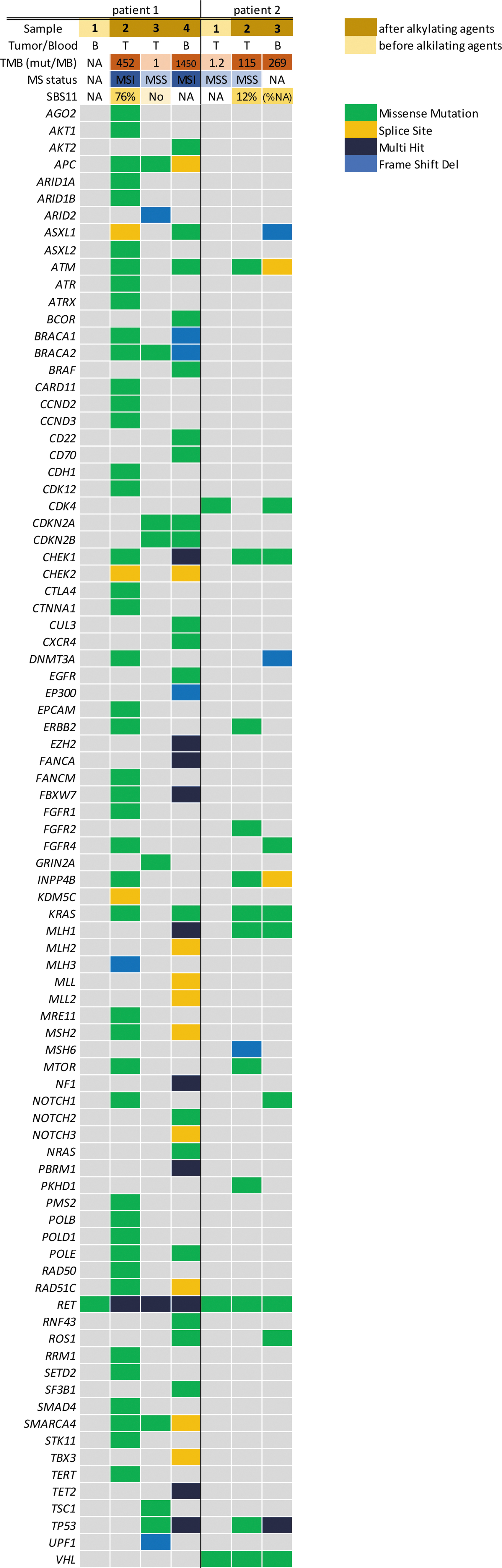
Oncoplot with TMB and MS-status before and after alkylating agents. For patient 1: biopsy number 1: liquid biopsy, Ion AmpliSeq Cancer Hotspot Panel v2 (50 genes); biopsy 2: tissue biopsy, WES, PFMG 2025; biopsy 3: tissue biopsy, WES, PFMG 2025; biopsy 4: liquid biopsy, FoundationOne Liquid CDx (324 genes, including TMB and MS-S). For patient 2: biopsy number 1: tissue biopsy, FoundationOne DX1 (324 genes including TMB and MS-S); biopsy 2: tissue biopsy, WES, PFMG 2025; biopsy 3: liquid biopsy, FoundationOne Liquid CDx. B, liquid biopsy; NA, nonavailable; T, tissue biopsy.
After a rechallenge of 7 cycles of 5-FU/DTIC with stable disease (SD) only and no clinical benefit, the patient started on compassionate selpercatinib, with major clinical benefit and PR. Twelve months after selpercatinib initiation, a dissociated response was observed. The patient underwent a cryotherapy of a progressive costal metastatic site. Tumor analysis with whole-exome sequencing (WES) under the Plan France Médecine Génomique (PFMG) 2025 program 19 revealed a very high TMB of 452.2 mutations/megabase with mutations in a large number of genes, including KRASG12D (resistance to selpercatinib) and mismatch repair (MMR) genes, resulting in a microsatellite (MS) instability (MS-I) status (Fig. 2). This molecular profile revealed a single-base substitution (SBS) mutational signature related to alkylating agent chemotherapy (SBS 11), suggesting that this high TMB was related to previous DTIC treatment.
Following selpercatinib discontinuation because of disease progression, the patient was enrolled in the ARIANES trial (NCT04276376, EudraCT: 2018-001744-62) and received atezolizumab and rucaparib. A dissociated response was observed, with PR in the liver (−60% according RECIST 1.1) for 6 months (Fig. 1). Biopsy analysis of a bony progressive lesion under rucaparib–atezolizumab did not reveal the alkylating agent mutational signature with high TMB (Fig. 1). Following progression under immunotherapy, she had another 6-month period of disease stabilization under pralsetinib. At this time, a new CtDNA molecular profile (FoundationOne liquid CDx) revealed a high TMB (1450 mutations/megabase) and an MS-I status (Fig. 2), but her condition worsened, and she passed away 11 years after the initial diagnosis.
Patient 2 was a 72-year-old male patient with a sporadic RET C634R-mutated high-grade pT3(m)N1bM1 (WHO 2022) MTC, with synchronous metastasis to bone, mediastinal lymph nodes, and the liver. After initial surgery in 2015, he received several systemic therapeutic lines for symptomatic metastatic progressive disease concomitantly to locoregional treatments: vandetanib for 10 months (best response: PR), followed by cabozantinib for 6 months (best response: PR) (Fig. 1). As third line, he received 13 cycles of TMZ (Tem 200 mg/m2/day, 5 days, 28-day cycle and capecitabine (Cap) 750 mg/m2 BID, 14 days, 28-day cycle). The MGMT H-score was low on three different pathological samples (0, 0, and 60/300). He experienced a major clinical benefit with reduction of bone pain and diarrhea together with a −31% RECIST response lasting 16 months (Fig. 1).
The baseline molecular profile before TemCap revealed RET C634R, VHL R167W, and CDK4 R24H mutations, TMB 1.2 mutations/megabase, and MS-stable (MS-S) status (FoundationOne DX1) (Fig. 2). At progression under TemCap, he received selpercatinib during 26 months (best response: SD) and another investigational RETi (NCT03780517) for 4 months (best response: progressive disease). At progression, the patient developed paraneoplastic adreno corticotropic hormone-dependent hypercortisolism with major clinical deterioration. At that time, the molecular profile by WES (PFMG 2025) of a progressive liver metastasis revealed a KRAS G12D mutation responsible for resistance to RET inhibition, a hypermutational phenotype with an MLH1 mutation, a high TMB at 115 mutations/megabase (without MS-I), and an SBS mutational signature related to alkylating agents' chemotherapy (SBS11) (Fig. 2). Liquid biopsy (FoundationOne CDx) performed at the same period also founded this hypermutational phenotype and the high TMB at 269 mutations/megabase (Fig. 2).
Therefore, the patient was started on anti PD-L1 durvalumab (individual request as compassionate use, 1500 mg every 28 days) for 9 months with a complete response of the Cushing syndrome and a partial morphologic response (−50% according RECIST 1.1) (Fig. 1). After further disease progression, rechallenge of TEM/CAP was initiated and is currently ongoing, with stabilization of the disease and decrease in bone pain for 8 months.
Discussion
Chemotherapy and particularly alkylating agents are not the preferred systemic treatment options for metastatic MTC. However, alkylating agents may still be relevant, for some patients, especially in the case of progression under MKi and/or RETi. In this study, we report two patients who experienced a clear prolonged clinical benefit under alkylating agents: DTIC, as described in small retrospectives studies 6 –10 and TMZ, the oral form of DTIC. As illustrated here, MGMT expression, assessed by immunohistochemistry and H-score may be a relevant predictive test as described in NET. 20
These two cases reveal, for the first time in MTC, a hypermutated phenotype with high TMB and an SBS mutational signature (SBS11) related to their prior alkylating agents' chemotherapy. 21 This WES analysis was made possible by the implementation, at the national level of the “Plan France Médecine Génomique,” the French genomic initiative, which aims to change methods for diagnosis, prevention, and treatment of patients with rare diseases by 2025. 22
The concept of alkylating agent-associated hypermutated phenotype was first described in gliomas treated by TMZ. 23 Data obtained from several longitudinal observational studies in gliomas treated by TMZ have revealed two distinct genomic outcomes at progression: the hypermutant-one and the nonhypermutant-one. 23,24 The hallmark of hypermutation progression includes the following: (1) a marked increase in TMB across the whole genome, (2) an enrichment of the C:G>T:A mutational signature indicative of alkylating mutagenesis (also called SBS 11), and (3) a gain of inactivating mutations in DNA MMR pathway components. 21,23,24 A preliminary study failed to prove immunotherapy efficacy in these hypermutant tumors, but several studies are currently underway (NCT04145115 and NCT02658279). 23
Moreover, there are some promising results in colorectal cancer (CRC), as shown by the MAYA trial, with durable clinical benefit in patients with metastatic MS-S CRC treated by TMZ followed by a combination with low-dose anti-CTLA4 ipilimumab and anti PD-1 nivolumab. 15,16 Several case reports of NET with high TMB, including one high-grade cervical NET, one carcinoid tumor, and one pituitary carcinoma, have also been described in the literature with responses to immune checkpoint inhibitors. 14,17,18
The two patients described here received in the 5th and 6th line of treatment with anti PD-L1 immune checkpoint inhibitors, either atezolizumab or durvalumab, with clinical benefit and partial morphologic responses during 6 and 9 months, respectively. In patient 1, we have been able to observe the heterogeneity of tumor evolution and resistance to different therapeutic lines with two tumoral contingents after 5-FU/DTIC, one hypermutated with high TMB and the other one not hypermutated with low TMB that was progressive to immunotherapy. This result is concordant with the inter- and intrametastasis heterogeneity of response to TMZ observed in the clinical study of CRC. 15 This also suggests that in the context of tumor heterogeneity, we should not expect an “immune priming” by a hypermutated tumor site to drive response to other tumor sites.
In addition, it is not known why some tumors develop a hypermutant phenotype, whereas others do not. This may occur despite stable MGMT expression, as reported in primary and recurrent glioma cases. 25 However, in our two patients, MGMT expression was low and may have driven the response to alkylating agents. Alkylating agents' mutational signature is associated with the presence of variant of the MMR gene, such as MSH6 or MLH1-MLH3, without necessarily being associated with MS-I, which is similar to what we observed. Currently, we do not know if the hypermutant phenotype in MTC is associated with better or worse patient outcomes, but it suggests the hypothesis that alkylating treatment could modify these tumors from immunologically “cold” to “hot.”
Moreover, high TMB has been associated with a greater therapeutic benefit from immune checkpoint inhibitors across multiple cancer types, 26,27 as confirmed in a recent real-life study 28 and in an extensive clinical study. 29 Pembrolizumab was recently approved by the Food and Drug Administration for use in TMB-high tumors, regardless of histology, based on KEYNOTE-15826 and might, in this setting, also be beneficial to MTC. 30 We believe that liquid biopsy and circulating tumor DNA sequencing are an effective and a minimally invasive tool to determine alkylating agent-associated hypermutated phenotype, with high TMB as a complementary to a tissue-based strategy.
We recognize some limitations of our report, such as incomplete data before initiating alkylating agents (e.g., no TMB for patient 1 and no SBS signature analyses for both patients). Both liquid and tissue biopsies were used with different techniques that could impact the concordance of the results, although a recent study has shown that liquid biopsy enables identification of clinically relevant alterations with high accuracy. 31 Importantly, there is currently no standardization for the ctDNA-based evaluation of hypermutational phenotype associated with alkylating agents.
To conclude, we report two cases of patients with a clear, prolonged clinical benefit of MGMT-deficient MTC under alkylating agent-based chemotherapy, the identification of an alkylating agent-induced hypermutant phenotype with high TMB after progression, and a clinical benefit with immune checkpoint inhibitors that led to PR for several months. Our observations warrant further exploration of the role of alkylating agents in both treatment and hypermutant phenotype induction, as a novel treatment strategy for progressive MTC patients, after standard-of-care kinase inhibitors.
Footnotes
Acknowledgments
This report was made possible through access to the data generated by the France Genomic Medicine Plan 2025. We thank “Gustave Roussy Promoteur” as well as ROCHE and CLOVIS for their participation in the ARIANES study (NCT04276376, EudraCT: 2018-001744-62). We are grateful to the precision medicine and the endocrine oncology teams of Gustave Roussy.
Authors' Contributions
S.M.: conceptualization, writing original draft, writing—review and editing; M.-A.B.: data curation and review; L.L., A.A.G., L.F., A.I., L.L., S.P.V., L.T., F.D., B.B., F.P., and E.B.: writing—review and editing; J.H.: data curation, conceptualization, writing original draft, writing—review and editing, and supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article. Funding for the clinical trials that are mentioned in these case reports are as follows: ROCHE and CLOVIS for NCT04276376, Boehringer Ingelheim for NCT01788982, and Boston Pharmaceuticals for NCT03780517.