
Abstract
Background:
Corticosteroid therapy is often employed in thyroid eye disease (TED), but its efficacy is variable. Teprotumumab and tocilizumab have been considered as effective alternatives. This study aims to evaluate their clinical outcomes and safety in patients with steroid-resistant TED.
Methods:
A retrospective case–control study was conducted between 2018 and 2022 within a national multicenter health system. Thirty-seven patients with moderate to severe steroid-resistant TED treated with teprotumumab or tocilizumab (cases) were compared with steroid-naïve patients treated with similar therapy (controls). Due to lack of steroid-naïve patients treated with tocilizumab, a control subgroup for tocilizumab was not included in the analysis. Demographic and clinical characteristics were described. Proptosis, diplopia, clinical activity score (CAS), and disease severity (European Group on Graves' orbitopathy classification) were evaluated at weeks 0, 12, 24, and 52 after therapy initiation.
Results:
Thirty-one patients received teprotumumab (13 cases and 18 controls) and 6 received tocilizumab (cases). The mean age was 57 years (standard deviation ±14.3), median duration of TED was 11.5 months (interquartile range [IQR]: 7.2–17.7), and median excess proptosis was 4 mm (IQR: 2–8) above the upper limit of normal for sex and race. At week 24, in the teprotumumab cases, 81% had proptosis response (reduction of ≥2 mm), 45.5% resolution of diplopia, 85.7% disease inactivation (CAS <3), and 58.3% reverted to mild disease severity. There were comparable results in teprotumumab controls, with no significant differences between subgroups. In the tocilizumab cases, 50% had a proptosis response, 16.7% resolution of diplopia, 100% disease inactivation, and 75% returned to mild disease. In the teprotumumab cases, there was a trend toward worsening proptosis and diplopia between weeks 24 and 52. In the same time frame, the tocilizumab cases had a trend toward worsening diplopia, disease activity, and severity. In the teprotumumab subgroup, 46.2% experienced otic changes and 23.1% hyperglycemia. In the tocilizumab subgroup, there were no reported adverse events.
Conclusions:
Teprotumumab and tocilizumab improved inflammation in patients with moderate to severe TED who had failed previous steroid therapy. Additionally, the teprotumumab cases demonstrated similar improvement in proptosis and diplopia to the teprotumumab controls. Further evaluation, particularly regarding the long-term response and side effect profile, of these medications in steroid-resistant TED is needed.
Introduction
Thyroid eye disease (TED) is the most common extrathyroidal manifestation of Graves' disease with a prevalence of 25–50% depending on race. 1 It is an inflammatory disease of the orbital tissues that can cause disfigurement and debilitation. Clinical presentation ranges from mild dry eye symptoms with foreign body sensation to sight-threatening exposure keratopathy or optic neuropathy. 2
While most patients have mild symptoms, 20–30% have moderate to severe disease and 3–5% develop sight-threatening disease. 3,4 Diplopia and exophthalmos are among the hallmarks of TED and are some of the features most difficult to treat.
Glucocorticoids have been the first-line treatment for TED since the 1980s. 5 –7 Previous studies demonstrated superior effectiveness and tolerability of high-dose intravenous over oral glucocorticoids in the treatment of TED. 8 However, treatment has shown mixed results, from complete response to steroid resistance. 5 –7,9
Moreover, patients might experience relapse following glucocorticoid discontinuation, 9 and the high dose and chronicity of glucocorticoid therapy could lead to unwanted side effects such as glucose intolerance, urinary tract infections, and Cushingoid features. 8 Given limitations to the effectiveness and safety profile of glucocorticoid therapy for TED, there has been ongoing research on alternative therapies.
In the last few decades, better understanding of the pathophysiology of TED has led to the pursuit of novel agents to treat it. Insulin-like growth factor receptor (IGF-1R) is coexpressed on orbital fibroblasts along with the thyrotropin receptor (TSH-R). 10 Binding of autoantibodies to TSH-R leads to cross-linking of the two receptors, orbital fibroblast activation, 11 and secretion of interleukin-6 (IL-6) and other cytokines that stimulate extracellular matrix production, 10 which is responsible for most manifestations of TED.
Teprotumumab, an IGF-1R inhibitor originally developed for cancer treatment, has shown efficacy in improving proptosis, diplopia, disease severity, and disease activity in patients with steroid-naïve TED and is the first advanced therapy approved by the Food and Drug Administration (FDA) to treat TED. 12
Tocilizumab, an IL-6 inhibitor that is FDA approved for other inflammatory conditions, has been used off-label for treatment of patients with steroid-resistant TED, with improvement in clinical activity and severity. 13
Importantly, the two pivotal trials for teprotumumab excluded patients with TED who had received glucocorticoid treatment, 12,14 and previously reported retrospective cohorts have not stratified their experience by exposure or response to systemic corticosteroids. 15,16 Thus, there are no reported data on efficacy of teprotumumab specifically in patients with steroid-resistant TED.
Furthermore, while previous studies of tocilizumab included patients with steroid-resistant TED, their numbers were small and follow-up was limited to 40 weeks. 13,17 In this retrospective study, we analyzed the clinical outcomes and safety of teprotumumab and tocilizumab in patients with moderate to severe steroid-resistant TED up to 52 weeks after therapy initiation.
Methods
Sample
This was a retrospective case–control study conducted in a major, multicenter health system in the United States. The electronic medical records of all patients with TED who received care between 2018 and 2022 were screened. Adult patients (18 years or older) who received treatment with teprotumumab (10–20 mg/kg every 3 weeks for a total of eight intravenous infusions) or tocilizumab (4 mg/kg for the first infusion, followed by 8 mg/kg every month, for a total of four intravenous infusions) were identified.
Those who had previously failed treatment (lack of improvement or worsening disease activity or severity) with a 4-g cumulative dose of intravenous methylprednisolone or a 6-week course of oral prednisone (with a starting dose of 40–80 mg daily) were deemed to be steroid resistant.
Clinical outcomes
Proptosis response (reduction of ≥2 mm without an increase in the contralateral eye); median excess proptosis (above normal for patients' sex and race); presence of diplopia; disease activity, as determined by the clinical activity score (CAS 0–7) 18 ; and disease severity based on the European Group on Graves' orbitopathy (EUGOGO) classification 19 were evaluated at baseline and at weeks 12, 24, and 52 after the first medication infusion.
Proptosis was assessed by an ophthalmologist and/or endocrinologist using a Hertel exophthalmometer. Adverse events were extracted from providers' documentation and medication administration records.
Statistical analysis
The total sample was divided into the teprotumumab and tocilizumab subgroups. Both subgroups were further subdivided into steroid-naive patients as controls and steroid-resistant patients as cases. Given the lack of steroid-naïve patients who received tocilizumab, only tocilizumab cases were characterized in the analysis. The evaluation of clinical and safety outcomes was performed for each subgroup separately.
Continuous variables are summarized using mean, median, and standard deviation (SD), and categorical variables are described with counts and percentages. At each of the study time points, the outcomes between the teprotumumab cases and controls were compared with Fisher exact tests for categorical variables and Kruskal–Wallis tests for continuous variables. A p-value <0.05 was used as the cutoff for statistical significance.
Ethical considerations
This study adheres to the Declaration of Helsinki and was performed in accordance with the Health Insurance Portability and Accountability Act. The study's protocol was reviewed by the Institutional Review Board at Mayo Clinic (22-002189), and the requirement for study-specific informed consent was waived. All participants who were treated in Minnesota had previously provided the required Minnesota Research Authorization. Participants' information, confidentiality, and integrity were respected throughout the duration of the study.
Results
Sample and baseline characteristics
A total of 41 patients with TED who were treated with teprotumumab or tocilizumab between 2018 and 2022 were screened. Patients without available follow-up data were excluded. Thirty-one patients treated with teprotumumab (13 cases and 18 controls) and 6 patients treated with tocilizumab (cases) were included in the analysis (Fig. 1). Table 1 summarizes the baseline demographic and clinical characteristics.
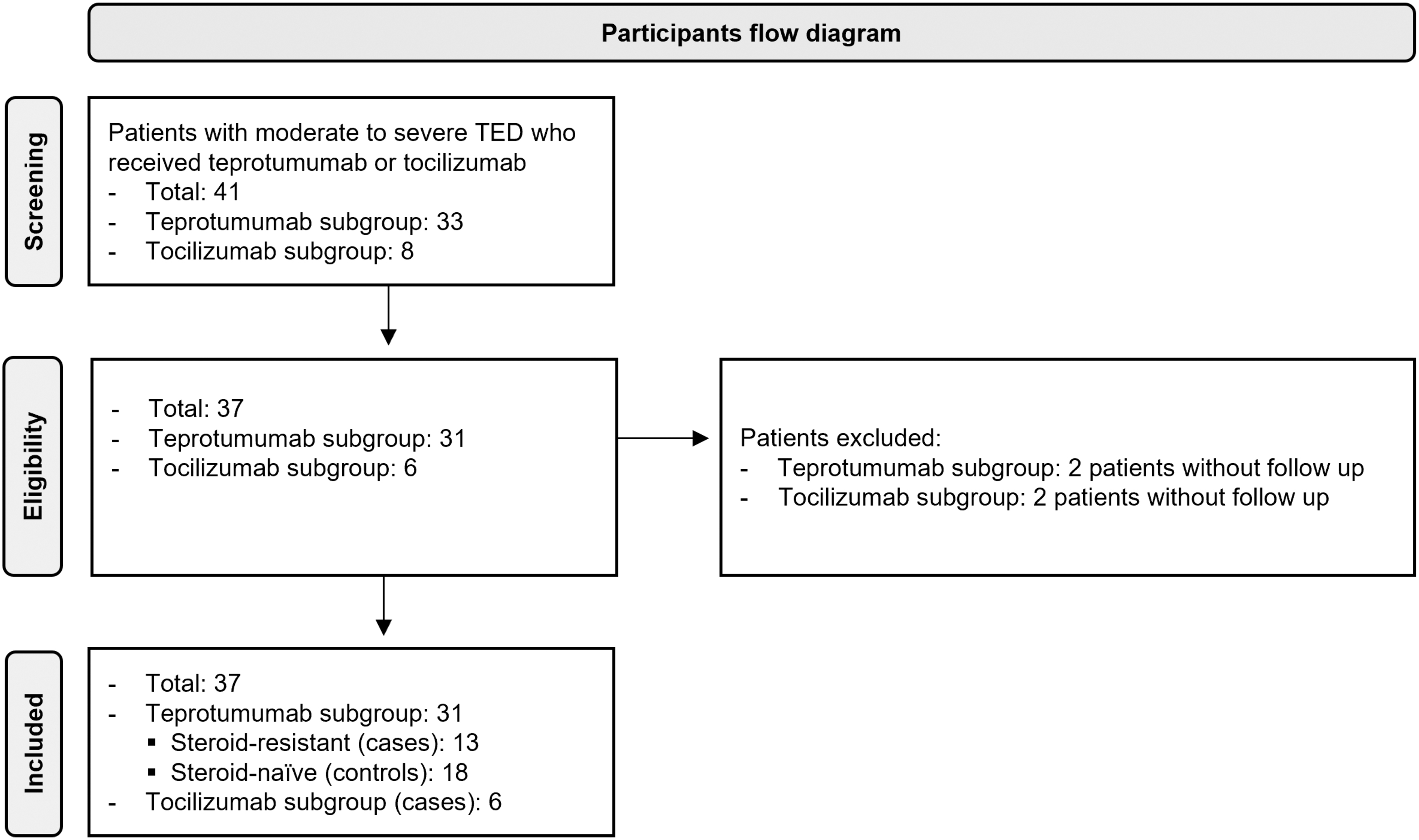
Participant flow diagram. TED, thyroid eye disease.
Baseline Characteristics
Above normal for patients' sex and race.
CAS, clinical activity score; IQR, interquartile range.
Most patients had Graves' disease (89.1%), and all patients had active moderate to severe TED based on the CAS and EUGOGO classification. In the total sample, the mean age was 57 years (SD ±14.3) and there was female and White predominance (72.9% and 89.1%, respectively). In the teprotumumab cases, the median duration of TED was 11 months (interquartile range [IQR]: 8–17.5), most were euthyroid (92.3%), 100% had diplopia, median excess proptosis was 4.5 mm (IQR: 1.8–8), and median CAS was 4 (IQR: 4–5).
In the teprotumumab controls, the median duration of TED was 10 months (IQR: 4.5–37.8), 44.4% were euthyroid, 72.2% had diplopia, median excess proptosis was 5 mm (IQR: 3–7), and median CAS was 4 (3–4.7). There were no statistically significant differences for these baseline characteristics between the teprotumumab cases and controls.
In the tocilizumab cases, the median duration of TED was 14.5 months (IQR: 12.5–21.7), all were euthyroid, 66.7% had diplopia, median excess proptosis was 2 mm (IQR: 2–7.3), and median CAS was 4 (IQR: 4–4.8). The median time from completion of systemic steroids was 3 months (IQR: 0.25–6) for teprotumumab cases and 7.8 months (IQR: 3.6–11.9) for tocilizumab cases.
Clinical outcomes
In the teprotumumab cases, by week 24, most patients experienced proptosis response (reduction of ≥2 mm) (83.3%) (Fig. 2A), the median excess proptosis decreased to 2 mm (IQR: −3.5 to 2) (Fig. 2B), 91.7% were deemed to have inactive TED (CAS of <3) (Fig. 2C), presence of diplopia decreased to 54.5% (Fig. 2D), and 58.3% improved to mild TED severity (as classified by the EUGOGO criteria) (Fig. 2E).
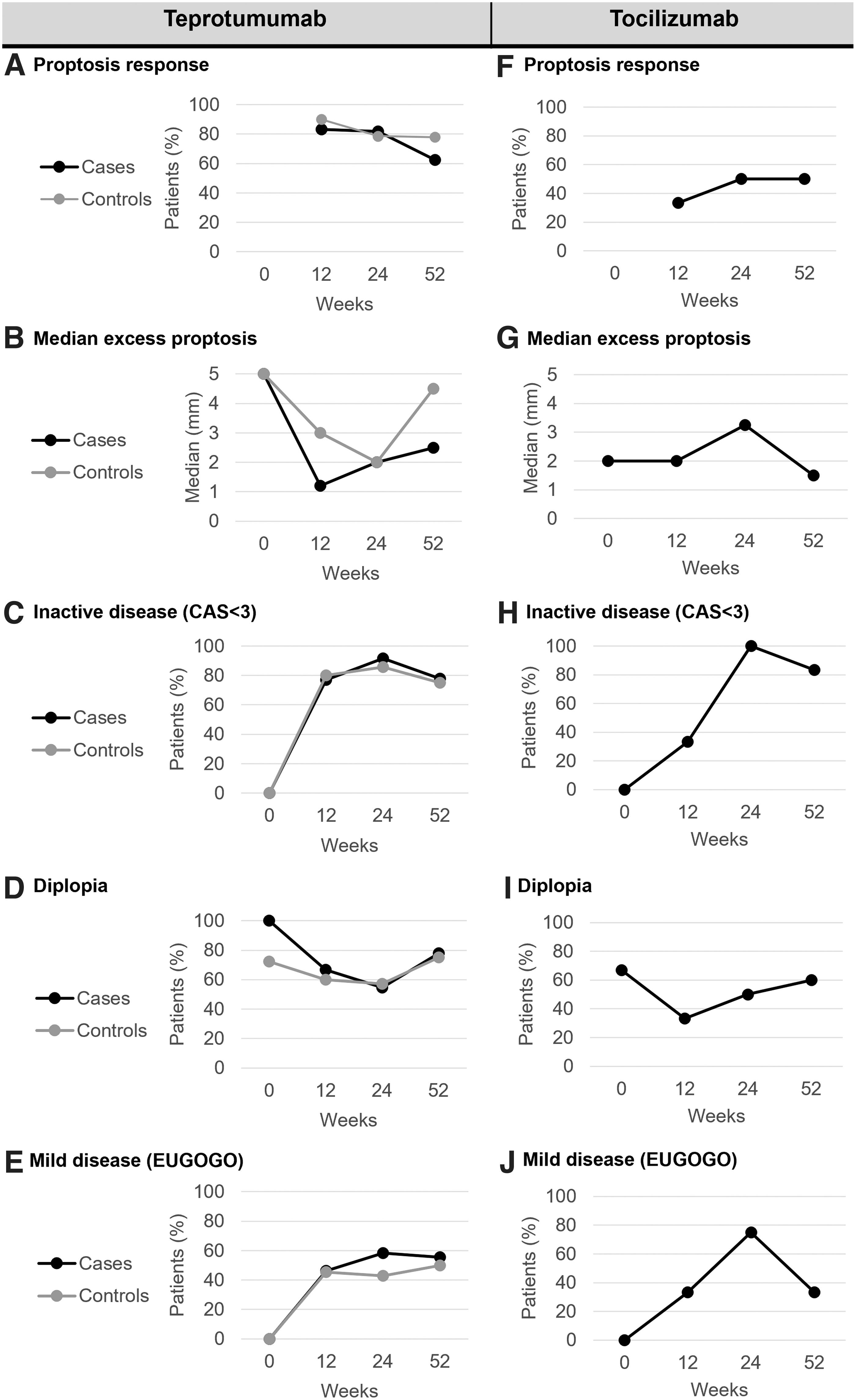
Clinical treatment outcomes. Chronological representation of clinical outcomes of teprotumumab and tocilizumab at 0, 12, 24, and 52 weeks from therapy initiation. (
All the outcomes remained improved at week 52 compared with baseline. However, from week 24 to 52, there was a trend toward increasing prevalence of excess proptosis >2 mm (18.2–37.5%), active disease (8.3–22.2%), and diplopia (54.5–77.8%). In the teprotumumab controls, by week 24, most patients experienced proptosis response (78.6%), the median excess proptosis decreased to 2 mm (IQR: −1.1 to 2), 85.7% were deemed to have inactive disease, the presence of diplopia decreased to 57.1%, and 42.9% improved to mild severity.
From week 24 to 52, there was a trend toward decreasing frequency of inactive disease (85.7–75%) and increasing frequency of diplopia (57.1–75%). No statistically significant differences were found when comparing any of the outcomes between the teprotumumab cases and controls at weeks 12, 24, and 52.
In the tocilizumab cases, by week 24, half of the patients (50%) experienced proptosis response (Fig. 2F). However, overall, the median excess proptosis did not exhibit clinically relevant trends through the different study time points (Fig. 2G). In all cases, TED became inactive (Fig. 2H), prevalence of diplopia decreased by 16.7% (Fig. 2I), and overall, 75% of patients improved to mild disease severity (Fig. 2J).
At week 52, diplopia, disease activity, and severity remained improved compared with baseline. However, from week 24 to 52, there was a trend toward a disease flare with increased frequency of active disease (0–16.7%) and return to moderate severity (25–66.7%).
One of the tocilizumab cases experienced overall improvement in proptosis, disease severity, and activity, but experienced disease reactivation with progressive inflammatory features and diplopia seven months after completing the tocilizumab infusions and required further treatment with teprotumumab.
In the teprotumumab cases, one patient experienced improvement in diplopia, proptosis, severity, and disease activity, but developed severe disease reactivation with bilateral optic neuropathy and required bilateral orbital decompression 11 months after completing teprotumumab therapy. Another patient required orbital decompression due to persistence of proptosis and a second course of teprotumumab due to disease reactivation at 6 and 22 months, respectively, after completing initial teprotumumab therapy.
In the teprotumumab controls, therapy was discontinued in one patient after the fourth infusion as significant TED improvement was already achieved, combined with a troublesome adverse effect (hair thinning). However, this patient experienced disease reactivation and worsening diplopia and proptosis around a year after the first infusion. Subsequently, the patient completed the remaining four infusions and had a positive response in disease activity, diplopia, and proptosis.
In addition, six different patients had surgery within 18 months of initiating teprotumumab, of which two patients had orbital decompression for worsening or persistent proptosis and four patients had strabismus surgery for worsening diplopia.
Safety
As depicted in Table 2, 76.9% of patients in the teprotumumab cases, 72.2% in the teprotumumab controls, and none in the tocilizumab cases experienced any adverse reaction. The most common adverse effects in the teprotumumab cases were otic changes (including 7.7% hearing loss and 38.4% tinnitus, ear fullness, or other nonhearing loss symptoms).
Safety
Number of patients. Some patients may have had more than one adverse event.
Includes ear fullness, tinnitus, and other nonhearing loss symptoms.
CI, confidence interval.
In this subgroup, only three patients underwent baseline audiology evaluation; one patient had mild to moderate sensorineural hearing loss and two patients had normal hearing. After 52 weeks of teprotumumab initiation, the patient with pre-existing sensorineural hearing loss was noted to have worsened hearing and was recommended for a hearing aid.
The second most common adverse effect was hyperglycemia (23.1%). In the teprotumumab controls, the most common adverse effects were muscle spasms (27.8%) and otic changes (16.7% hearing loss and 5.6% tinnitus, ear fullness, or other nonhearing loss symptoms).
Only one patient underwent baseline audiology evaluation, which revealed mild to moderate sensorineural hearing loss. This patient reported transient worsened hearing during the medication infusions, but audiology reevaluation at 40 weeks remained unchanged compared with baseline.
Noteworthy, there were no statistically significant differences in the frequency of individual adverse events between teprotumumab cases and controls.
Additionally, two patients experienced serious adverse reactions. One of the teprotumumab cases experienced a retropharyngeal abscess complicated by severe sepsis due to Escherichia coli after the fourth dose of teprotumumab, after which the medication was discontinued. Another teprotumumab control developed acute pancreatitis complicated by peripancreatic necrosis and abscess requiring inpatient care. In this patient, teprotumumab was discontinued after the third infusion.
Discussion
Teprotumumab has emerged as an FDA-approved therapeutic alternative for TED with promising efficacy and safety profile. 20,21 In phase 3 clinical trials of teprotumumab conducted in steroid-naïve patients, 12,22 teprotumumab showed efficacy in proptosis reduction, disease activity, and diplopia. Similar results were noted in a small retrospective series with mixed disease activity and severity at baseline. 15
Furthermore, case reports and case series of teprotumumab use in patients with TED complicated by optic neuropathy have found resolution or improvement of neuropathy along with proptosis reduction and disease inactivation. 23 None of the post-FDA approval, clinical practice studies have stratified their findings by previous use or response to systemic corticosteroid therapy and their duration of follow-up has been limited to up to 30 weeks.
In contrast, tocilizumab remains an off-label medication used to treat TED, with limited data that originate from a single-center open-label series and a single randomized clinical trial in a steroid-resistant population only. 13,24 Our retrospective study reassuringly found teprotumumab and tocilizumab to be beneficial to various degrees for up to 52 weeks, even in patients with TED who had failed prior steroid therapy.
Similar to the results of trials conducted in steroid-naïve TED patients, 12,22 in our teprotumumab controls, there were clinical improvements in proptosis, diplopia, disease activity, and disease severity at week 24 compared with baseline. However, as opposed to the randomized clinical trials, our patients had a longer duration of TED (4–6 months in clinical trials vs. 10 months in our series).
Furthermore, similar to the long-term efficacy outcomes reported by Kahaly et al., 20 the improvements in disease activity and severity remained evident at week 52. In addition, the clinical outcomes of the teprotumumab cases were consistent with those of the controls, with no statistically significant differences between them. Noteworthy, while all clinical outcomes at week 52 had some degree of clinical improvement compared with baseline, from week 24 to 52, there was a trend toward disease reactivation and worsening severity, reflected in CAS, proptosis, and diplopia changes.
While these findings might be related to the small sample size, further study is needed to evaluate these trends. Furthermore, in our series, at least four patients experienced severe disease progression/reactivation, which required orbital decompression after an initial successful response to teprotumumab. Similar to the Optic-X extension trial, 14 our findings further inform on the durability of initial results and potential need for retreatment with teprotumumab in a subgroup of patients.
In our tocilizumab subgroup, there was clinically meaningful improvement in disease activity and severity by week 24, which was explained by improvement of inflammatory features such as soft tissue involvement (eyelid swelling, eyelid erythema, and lid retraction), orbital pain, chemosis, and conjunctival erythema. These findings are consistent with those reported by Perez-Moreiras et al. 13
In contrast, in our series, there was also mild improvement in diplopia at weeks 12 and 24 compared with baseline, but the benefit was less apparent by week 52, even though both disease activity and severity at this point remained improved compared with baseline.
Furthermore, one of our patients who initially responded to tocilizumab later experienced disease reactivation and was treated with teprotumumab. Despite our series being small, these findings highlight the need for additional research to understand the long-term efficacy of tocilizumab and the predictors of successful therapy to facilitate individualized TED management strategies.
In our series, the adverse event profile in the teprotumumab cases was similar to that of controls. In both subgroups, otic changes and hyperglycemia were among the most frequent adverse effects. The incidence of otic changes was higher than in prior randomized controlled trials 12,22 and similar to what has been reported in clinical case series. 14,25 –27
However, only a few patients underwent audiology assessment before therapy initiation, and it is not possible to determine whether some of the reported otic changes corresponded to new onset versus worsening baseline otic impairment. Similar to prior studies, otic changes presented in a spectrum from tinnitus to hearing loss, many were mild and transient, and did not require treatment discontinuation. 14,20,25
In concordance with the larger series by Amarikwa et al., in our series, hyperglycemia was persistent, with most affected patients being ultimately diagnosed with diabetes and started on oral antihyperglycemic agents by week 24. Measurement of hemoglobin A1C (HbA1C) or fasting glucose after initiation of teprotumumab was conducted at the discretion of each provider, thus our results might underestimate the true prevalence of hyperglycemia in real practice. 28
Furthermore, while one of our teprotumumab cases experienced severe sepsis, there is no readily available explanation, and only one other similar case has been previously reported by Smith et al. 22 Similarly, it was unclear whether the acute pancreatitis with complications in one control patient was related to teprotumumab therapy as no similar event had been reported in the past. Nevertheless, teprotumumab was discontinued out of caution.
Perez-Moreiras et al. have previously reported that hypercholesterolemia is the most common adverse effect and that other serious reactions, such as liver injury and acute pyelonephritis, can be seen with the use of tocilizumab in patients with TED. 13,17 In our series, no clinically relevant liver impairment, hypercholesterolemia, sepsis, or other milder infectious processes were documented.
The results of this study should be considered in the context of its limitations. Our series is relatively small, particularly the tocilizumab subgroup, substantially limiting its statistical power and likely leading to underestimation of its outcomes. Moreover, for the tocilizumab subgroup, there were no controls, thus our analysis was limited to descriptive statistics and comparisons could not be established.
Furthermore, given the retrospective design, missing data could have affected the accuracy of the findings (for instance, at week 52, only 61.5% of the data for teprotumumab controls were available for review). The severity of certain variables could not be graded and their evaluation had to be done in a dichotomized way, which might have limited our ability to detect subtle changes in features such as diplopia.
Moreover, the intensity, duration, and reversibility of some adverse effects could not be fully assessed from the available data. Our findings highlight the need for a more standardized screening and monitoring process to facilitate early identification and management of potential adverse events and a more precise evaluation of clinical outcomes.
In addition, a major limitation with regard to the tocilizumab group is the selection of patients—the drug lacks FDA approval for TED, hence most of these patients had to pay for the treatment out of pocket, leading to a selection bias and impairing the generalization to the broad TED population. Despite these limitations, our results may inform current clinical practice and guide the design of future randomized prospective studies to revise and strengthen the current findings.
In conclusion, teprotumumab and tocilizumab appear to be beneficial in improving disease activity and severity even in patients with TED who have failed previous steroid therapy. In addition, teprotumumab use resulted in considerable improvement in proptosis and diplopia in these patients, while tocilizumab had a very appealing safety profile.
However, more research is needed to strengthen these findings and inform on the comparison between these drugs and their long-term efficacy, as well as the potential need for subsequent treatments.
Footnotes
Authors' Contributions
D.T.-T. and K.N.R. were involved in conceptualization, methodology, data collection, statistical analysis, and manuscript preparation (initial draft, review, and editing). M.N.S. was involved in conceptualization, methodology, and manuscript preparation (review and editing). E.A.B., L.H.W., A.A.T., and J.K.S. were involved in manuscript preparation (review and editing).
Author Disclosure Statement
M.N.S. declares that within the last two years, his institution has received research support from Horizon Therapeutics, Immunovant, ValenzaBio, Lassen Therapeutics, and Sling Therapeutics and he is a consultant for Septerna Inc., Third Rock Ventures LLC, Genentech, ArgenX US Inc., Tourmaline Bio, Ortho Clinical Diagnostics, OSE Immunotherapeutics, and Roivant Sciences. The other authors have no relevant disclosures.
Funding Information
No funding was received for this article.