
Abstract
Background:
Although recent studies have introduced antibiotics as a potential risk factor for thyroid cancer, further studies are necessary. We examined the association between long-term antibiotic usage and thyroid cancer risk.
Methods:
This nationwide cohort study investigated 9,804,481 individuals aged 20 years or older who participated in health screening (2005–2006) with follow-up ending on December 31, 2019, using the Korean National Health Insurance Service database. Multivariable Cox proportional hazards regression was used to estimate adjusted hazard ratios (aHRs) and 95% confidence intervals (CIs) for thyroid cancer risk according to the cumulative days of antibiotic prescription and the number of antibiotic classes, respectively. A 1:1 propensity score (PS) matching was also performed for analysis.
Results:
Compared with nonusers of antibiotics, participants prescribed ≥365 days of antibiotics showed an increased risk of thyroid cancer (aHR, 1.71; CI, 1.66–1.78) after adjusting for covariates including age, smoking status, comorbidities including thyroid-related diseases, and the number of head and neck computed tomography scans. Participants prescribed ≥365 days of antibiotics also had a significantly increased risk of thyroid cancer (aHR, 1.37; CI, 1.34–1.40) compared with participants prescribed 1–14 days of antibiotics. Association remained significant in the 1:1 PS-matched cohort. Moreover, compared with nonusers of antibiotics, the 5 or more antibiotic class user group had a higher thyroid cancer risk (aHR, 1.71; CI, 1.65–1.78).
Conclusions:
Long-term antibiotic prescriptions and an increasing number of antibiotic classes may be associated with a higher risk of thyroid cancer in a duration-dependent manner. The effects of long-term antibiotic exposure on thyroid cancer should be further investigated.
Introduction
Thyroid cancer is the most commonly diagnosed malignancy in South Korea. Widespread thyroid cancer screening in South Korea may be one of the major causes of the high incidence of thyroid cancer. 1,2 Nevertheless, although several factors, such as radiation exposure, 3 –6 computed tomography (CT) scans, 6 and thyroid-related diseases, 6 –8 have been revealed to be possible causative factors of thyroid cancer, evidence regarding the other risk factors remains insufficient. Furthermore, recent advances in genetic sequencing technologies enabled the discovery that microbiota may be associated with thyroid cancer development, adding to genetic and environmental factors. 9 –11
Gut microbiota plays an integral role in inflammation and tumorigenesis. 12,13 The thyroid–gut axis is currently considered an important linkage between the immune system and thyroid diseases. 14 Gut microbiota dysbiosis promotes the production of cytotoxins and genotoxicity and, as a result, strongly affects the protection against and susceptibility to the development of cancer. 15 Therefore, antibiotic-induced dysbiosis of the gut microbiota and the interaction between the gut and the thyroid may lead to the development of thyroid cancer. 16,17
Multiple studies have shown alterations in the composition of intestinal and thyroid microbiota in individuals diagnosed with thyroid cancer. 18 –20 Antibiotic usage reduces the diversity of gut microbes, especially by depleting the gut microbiome, and as a result, the microbial antitumor activity within the thyroid is impaired. 21 Various studies have reported that antibiotic use is associated with a higher risk of cancers such as colorectal cancer and lung cancer. 22,23
However, there is currently limited evidence about the association between thyroid cancer and antibiotic exposure. A Finnish study, comprising 1769 identified thyroid cancer cases among 3,112,624 participants, has shown a higher risk of thyroid cancer incidence related to antibiotic prescription. The age- and sex-adjusted relative risk (RR) for thyroid cancer participants with six or more antibiotic prescriptions was 1.67 (1.41–1.99). 16 However, the potential confounding variables were not adjusted when performing statistical analysis.
In this retrospective cohort investigation, we explored the relationship between antibiotic usage and the incidence of thyroid cancer by analyzing data from the Korean National Health Insurance Service (KNHIS) database.
Methods
Data source
The nationwide cohort study was identified from the National Health Insurance Service (NHIS) database of South Korea. The NHIS provides mandatory health insurance for the entire Korean population covering a wide range of health services. 24 Citizens over the age of 20 are qualified to participate in a biannual health checkup program, which includes a self-reported questionnaire on lifestyle habits, laboratory tests, and anthropometric measurements. 25
The NHIS database includes comprehensive sociodemographic information, results of health checkups, records of both inpatient and outpatient health care visits, and medication prescriptions. This database has been employed in numerous epidemiological research studies, 26 –28 and its validity has been well demonstrated elsewhere. 24,25,29
This study was approved by the Institutional Review Board (IRB) of Seoul National University Hospital (IRB No. E-2204-023-1312). Since this retrospective cohort study utilized the database, which is anonymized by strict confidentiality guidelines, the requirement for informed consent was waived. This study followed Strengthening the Reporting of Observational Studies in Epidemiology reporting guideline. 30
Study population
Among a total of 12,163,324 participants aged 20 years or older who participated in health screening between 2005 and 2006, individuals were excluded if (1) they were diagnosed with cancer before the index date of January 1, 2007 (n = 1,884,138), (2) they died before the index date (n = 11,302), or (3) they had any missing values for covariates (n = 463,403). Finally, 9,804,481 individuals were included in the analyses (Fig. 1). All participants in the cohort were followed up until the date of cancer diagnosis, death, or December 31, 2019, whichever happened first.
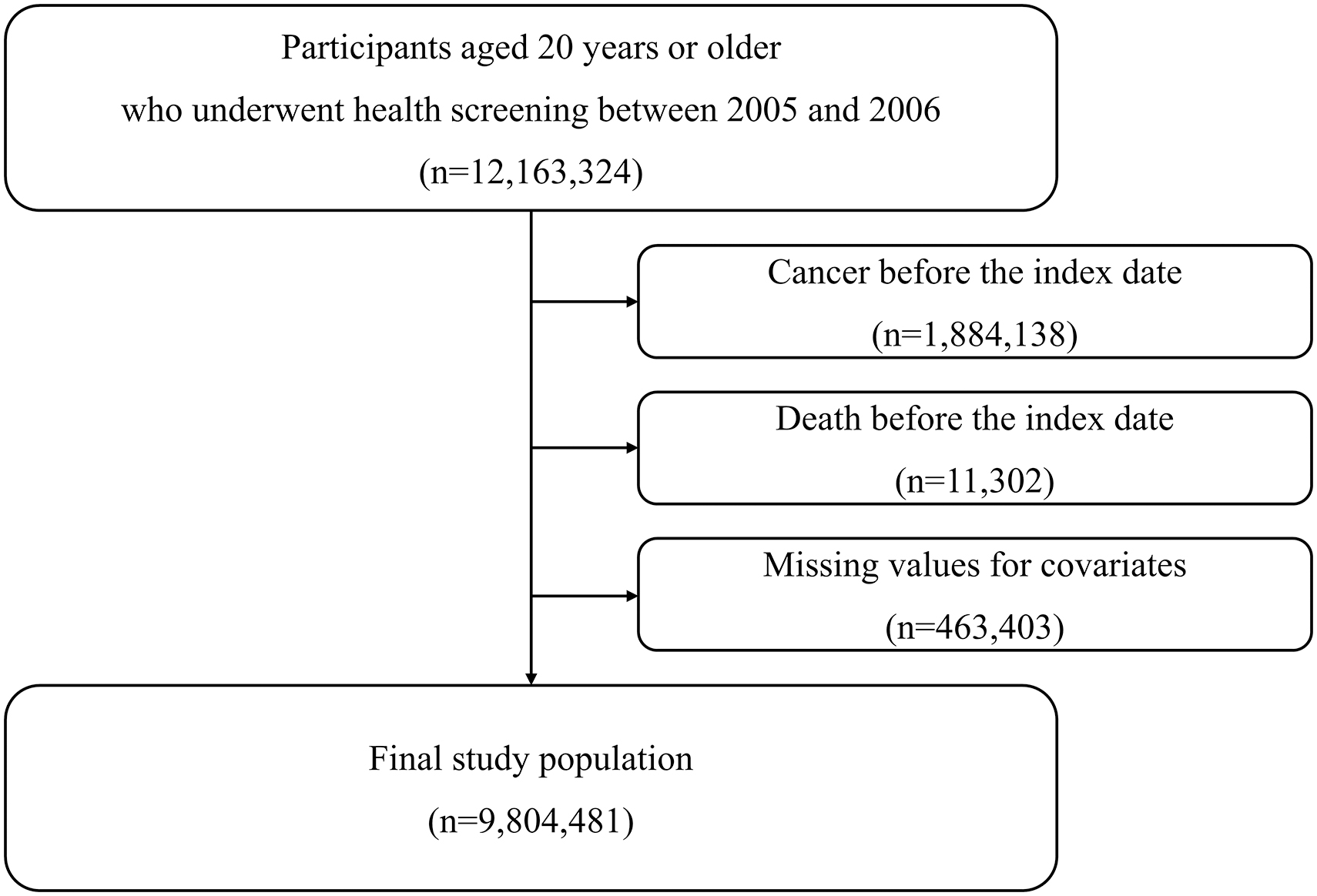
Identification of the study cohort.
Exposure
Antibiotic exposures were defined as the cumulative total days of prescription, the number of antibiotic classes, and a single specific antibiotic use for 5 years before the index date from the database. In other words, antibiotic exposure was considered in the main analyses between January 1, 2002 and December 31, 2006. The KNHIS database includes prescription records consisting of the drug code, prescription date, days prescribed, and medication dosage.
The database would contain all antibiotic prescriptions, since antibiotics are prescribed by physicians in South Korea. We identified antibiotics, such as sulfonamides, lincosamides, cephalosporins, macrolides, tetracyclines, penicillins, fluoroquinolones, vancomycin, and others, based on the World Health Organization (WHO) Anatomical Therapeutic Chemical (ATC) classification (eTable 1in Supplementary Data). 31,32
The number of cumulative days was classified into six categories: 0 (nonusers), 1–14, 15–90, 91–180, 181–364, and 365 or more days. The number of classes was classified into six categories: 0 (nonusers), 1, 2, 3, 4, or 5 or more classes. We also assessed the single-class impact of antibiotics by comparing antibiotic nonusers to users of a single-specific class exclusively.
Covariates
For multivariable regression analyses, we extracted information on age, sex, household income, Charlson comorbidity index (CCI), smoking status, alcohol intake, physical activity, body mass index (BMI), total cholesterol (TC), systolic blood pressure (SBP), fasting serum glucose (FSG), thyroid nodules, Hashimoto's thyroiditis, hypothyroidism, hyperthyroidism, Graves' disease, and the number of head and neck CT scans 33 (eMethod 1 in Supplementary Data). Household income was obtained from the insurance premiums of each individual. CCI was calculated in line with previous research. 34
Outcome
The primary outcome was thyroid cancer, which occurred between January 1, 2007 and December 31, 2019. The operational definition was defined as the diagnosis code for thyroid cancer (C73) based on the International Classification of Diseases, Tenth Revision (ICD-10) with the critical condition code for cancer (V193 and V194). 35,36 The government subsidizes 95% of the medical costs for 5 years for cancer patients who registered with the NHIS and received V codes. 37 The physicians register patients with V codes for carcinoma based on strict pathological confirmation after biopsy or surgical removal. 38 This method is well-known for its high accuracy in identifying newly diagnosed cancer patients. 36 –38
Statistical analysis
Categorical variables were presented as number (percentage), and continuous variables were presented as mean (standard deviation [SD]). Participants' baseline characteristics are also presented using the chi-square test for categorical variables and the analysis of variance for continuous variables. Cox proportional hazards regression was used to calculate the crude hazard ratios (cHRs) or adjusted hazard ratios (aHRs) and 95% confidence intervals (CIs).
Covariates considered in the model included age, sex, household income, CCI, smoking status, alcohol intake, physical activity, BMI, TC, SBP, FSG, thyroid nodules, Hashimoto's thyroiditis, hypothyroidism, hyperthyroidism, Graves' disease, and the number of head and neck CT scans. Analyses were conducted using two reference groups, such as the antibiotic nonusers and the individuals who were prescribed antibiotics for 1–14 days.
We performed the additional analysis using the cumulative days of antibiotics as a continuous variable to examine the linear trend of this research. In addition, we examined the hazard ratios of the covariates adjusted and RR by covariates. In the sensitivity analyses, we did not consider patients who were diagnosed with thyroid cancer within the first 1, 3, or 5 years of follow-up to minimize protopathic bias. 26,27
We also performed sensitivity analyses by lengthening the antibiotic exposure duration from 5 years to 7 or 9 years. Shifting the index date was to check for any potential confounding caused by drug use after the index date of the main analyses. 27,39 In the sensitivity analysis of changes in exposure and follow-up duration, all covariates were re-extracted and adjusted based on the changed index date, respectively.
Variables related to health checks, including lifestyle behaviors, were extracted from information for the 2 years before the index date. We also excluded individuals with thyroid-related diseases, such as thyroid nodules, Hashimoto's thyroiditis, hypothyroidism, hyperthyroidism, and Graves' disease, when performing sensitivity analysis. Moreover, we performed subgroup analyses stratifying by age, sex, CCI, BMI, smoking status, alcohol intake, physical activity, thyroid nodules, Hashimoto's thyroiditis, hypothyroidism, hyperthyroidism, Graves' disease, and the number of head and neck CT scans.
Finally, propensity score (PS) matching was used to minimize confounding effects between the antibiotic nonuser and the antibiotic user groups. The PS was generated using baseline characteristics such as age, sex, household income, CCI, smoking status, alcohol intake, physical activity, BMI, TC, SBP, FSG, thyroid nodules, Hashimoto's thyroiditis, hypothyroidism, hyperthyroidism, Graves' disease, the number of head and neck CT scans, and infectious diseases.
Infectious diseases, which are causes of antibiotic prescription, were defined into six variables: respiratory diseases, urinary tract infections, skin, soft tissue, bone, and joint infections, intra-abdominal infections, intestinal infectious diseases, and other infectious diseases (eTable 2 in Supplementary Data). A matching ratio of 1:1 was employed to match participants from two different groups using a caliper of 0.1 SD of the logit PS.
Covariates in multivariable Cox proportional hazards regression analysis using PS included age, sex, household income, CCI, smoking status, alcohol intake, physical activity, BMI, TC, SBP, FSG, thyroid nodules, Hashimoto's thyroiditis, hypothyroidism, hyperthyroidism, Graves' disease, and the number of head and neck CT scans. We also conducted subgroup analyses stratified by age and sex. Statistical significance was determined using a two-sided manner with a threshold of p < 0.05. Data mining and statistical analyses were conducted using SAS Enterprise Guide 8.3 (SAS Institute, Cary, NC).
Results
Baseline characteristics
A total of 9,804,481 individuals were included in our analysis, including 109,144 thyroid cancer cases during the mean follow-up of 10.52 years. Characteristics of the study population based on antibiotic cumulative days are presented in Table 1. Individuals with longer cumulative days of antibiotic exposure were more likely to be older and to have a higher BMI, less alcohol intake, more never-smokers, more physical activity, thyroid-related diseases, and a high number of head and neck CT scans.
Characteristics of the Study Population
The p-values were calculated using the χ 2 test for categorical variables and an analysis of variance for continuous variables.
BMI, body mass index; CCI, Charlson Comorbidity Index; CT, computed tomography; FSG, fasting serum glucose; SBP, systolic blood pressure; SD, standard deviation; TC, total cholesterol.
Association between antibiotic cumulative prescription days and thyroid cancer
Association of antibiotic cumulative prescription days with thyroid cancer is presented in Table 2. Greater cumulative days of antibiotic exposure were associated with an increased risk of thyroid cancer (p trend<0.001). In the crude model, ≥365 days of antibiotic use were associated with a higher thyroid cancer risk (cHR, 2.47; CI, 2.38–2.55) than antibiotic nonusers.
Risk of Thyroid Cancer According to Antibiotic Cumulative Prescription Days
Model 1 adjusted for age and sex.
Model 2 adjusted for model 1 plus household income, CCI, smoking status, alcohol intake, physical activity, BMI, TC, SBP, FSG, thyroid nodules, Hashimoto's thyroiditis, hypothyroidism, hyperthyroidism, Graves' disease, and the number of head and neck CT scans.
aHR, adjusted hazard ratio; cHR, crude hazard ratio; CI, 95% confidence intervals; ref., reference; PY, person-years.
The longer duration of antibiotic exposure was associated with the risk of thyroid cancer (aHR, 1.71; CI, 1.66–1.78 for ≥365 days of exposure) in model 2. Compared with those who used antibiotics for 1–14 days, ≥365 days users (aHR, 1.37; CI, 1.34–1.40) had a higher risk for thyroid cancer in model 2. Thyroid cancer risk remained elevated when analyzing antibiotic cumulative days as a continuous variable (aHR, 1.084; CI, 1.080–1.089; p < 0.001) in model 2 (eTable 3 in Supplementary Data).
Sensitivity analysis
The results from all sensitivity analyses were mostly consistent with the primary findings (Table 3). First, we performed analyses with a washout period of 1, 3, or 5 years. After a 1-year washout period, those who were prescribed antibiotics for ≥365 days had a significantly increased risk of thyroid cancer compared with antibiotic nonusers (aHR, 1.72; CI, 1.66–1.78) or those who were prescribed antibiotics for 1–14 days (aHR, 1.37; CI, 1.34–1.40).
Sensitivity Analysis for the Association of Antibiotic Exposure with Thyroid Cancer
Model 1 adjusted for age, sex, household income, CCI, smoking status, alcohol intake, physical activity, BMI, TC, SBP, and FSG, thyroid nodules, Hashimoto's thyroiditis, hypothyroidism, hyperthyroidism, Graves' disease, and the number of head and neck CT scans.
Model 2 adjusted for age, sex, household income, CCI, smoking status, alcohol intake, physical activity, BMI, TC, SBP, and FSG, and the number of head and neck CT scans.
The antibiotic exposure period in analyses was set from 2002 to 2006, five years in total. The shifting index date indicates that the antibiotic exposure period was set from 2002 to 2008, seven years in total, and 2002–2010, nine years in total.
Thyroid-related diseases included thyroid nodules, Hashimoto's thyroiditis, hypothyroidism, hyperthyroidism, and Graves' disease.
Further results for washout periods of 3 or 5 years were also consistent. Second, we conducted analyses by shifting the index date from January 1, 2007 to January 1, 2009, or January 1, 2011. In other words, antibiotic exposure was defined as use for 7 or 9 years before the index date. The longer the total days of antibiotic exposure, the greater the risk of thyroid cancer (p trend<0.001) in all analyses.
In a 9-year exposure period, those who received antibiotic prescriptions for ≥365 days had an elevated risk for thyroid cancer compared with antibiotic nonusers (aHR, 1.78; CI, 1.70–1.85) or those who have prescribed antibiotics for 1–14 days (aHR, 1.40; CI, 1.37–1.43). After the exclusion of thyroid-related disease patients, those who received antibiotic prescriptions for ≥365 days had an increased risk for thyroid cancer compared with antibiotic nonusers (aHR, 1.74; CI, 1.68–1.81) or those who have prescribed antibiotics for 1–14 days (aHR, 1.39; CI, 1.36–1.42).
Subgroup analysis
Among the adjusted variables in statistical models, female sex (HR, 3.33; CI, 3.27–3.39), CCI (HR, 1.03; CI, 1.03–1.04), BMI (HR, 1.02; CI, 1.02–1.02), physical activity, thyroid nodules (HR, 2.75; CI, 2.67–2.82), Hashimoto's thyroiditis (HR, 1.21; CI, 1.11–1.31), hypothyroidism (HR, 1.08; CI, 1.03–1.13), hyperthyroidism (HR, 1.21; CI, 1.15–1.27), and Graves' disease (HR, 1.10; CI, 1.02–1.19) were determined to be independent risk factors for thyroid cancer (eTable 4 in Supplementary Data).
There was a significantly increased RR for thyroid cancer patients with age ≥40 years (RR, 1.15; CI, 1.14–1.17), female (RR, 3.77; CI, 3.72–3.82), CCI ≥1 (RR, 1.17; CI, 1.15–1.18), thyroid nodules (RR, 4.60; CI, 4.48–4.72), Hashimoto's thyroiditis (RR, 2.96; CI, 2.73–3.21), hypothyroidism (RR, 2.42; CI, 2.31–2.52), hyperthyroidism (RR, 2.17; CI, 2.07–2.28), Graves' disease (HR, 2.11; CI, 1.96–2.27), and the number of head and neck CT scans ≥1 (RR, 1.06; CI, 1.03–1.09) (eTable 5 in Supplementary Data).
We also observed interactions of antibiotic exposure with baseline age, sex, household income, CCI, BMI, smoking status, alcohol intake, thyroid nodules, Hashimoto's thyroiditis, hypothyroidism, or hyperthyroidism on thyroid cancer (P interaction<0.05) (eTable 6 in Supplementary Data). We did not find a significant interaction between antibiotic exposure with physical activity, Graves' disease, or the number of head and neck CT scans on thyroid cancer risk (P interaction>0.05).
During the follow-up period, 6243 individuals were diagnosed with thyroid cancer out of 138,813 patients with thyroid nodules. Thyroid nodules were estimated to be an independent risk factor and associated with a high RR in our analysis. However, in the stratified analyses, the association between antibiotic exposure and thyroid cancer risk was more pronounced in the group without thyroid-related disease, including thyroid nodules.
Analysis before and after PS matching
In the unmatched cohort, 639,429 individuals were antibiotic nonusers, and 9,165,052 individuals were antibiotic users. Among the 1:1 PS-matched cohort, 638,379 individuals were antibiotic nonusers and antibiotic users, respectively. Baseline characteristics, including the standardized mean difference for all covariates, are presented in eTable 7 in Supplementary Data. With a fully adjusted model, antibiotic use was associated with a greater risk of thyroid cancer (aHR, 1.48; CI, 1.43–1.53) compared with antibiotic nonuse in the unmatched cohort.
After 1:1 PS matching, the association between antibiotics and thyroid cancer was maintained. Antibiotic use was associated with a higher risk of thyroid cancer (aHR, 1.20; CI, 1.15–1.25) compared with antibiotic nonuse (Table 4). After stratifying by sex and age, antibiotic exposure was linked to an increased risk of thyroid cancer in individuals of each different age group (eTable 8 in Supplementary Data) as well as in both male and female (eTable 9 in Supplementary Data).
Risk of Thyroid Cancer Associated with Antibiotic Exposure Before and After 1:1 Propensity Score Matching
Propensity score matching was conducted using age, sex, household income, Charlson comorbidity index, smoking status, alcohol intake, physical activity, body mass index, total cholesterol, systolic blood pressure, fasting serum glucose, thyroid nodules, Hashimoto's thyroiditis, hypothyroidism, hyperthyroidism, Graves' disease, the number of head and neck CT scans, and infectious diseases (respiratory diseases, urinary tract infections, skin, soft tissue, bone, and joint infections, intra-abdominal infections, intestinal infectious diseases, and other infectious diseases).
Model 1 adjusted for age and sex.
Model 2 adjusted for model 1 plus household income, CCI, smoking status, alcohol intake, physical activity, BMI, TC, SBP, FSG, thyroid nodules, Hashimoto's thyroiditis, hypothyroidism, hyperthyroidism, Graves' disease, and the number of head and neck CT scans.
PS, propensity score.
Association between the number of antibiotic classes and thyroid cancer
In analyses examining thyroid cancer risk according to the number of antibiotic classes (eTable 10 in Supplementary Data), increasing the number of antibiotic classes was associated with an increased risk of thyroid cancer (p trend<0.001). In the adjusted model, individuals who used five or more antibiotic classes had a higher risk of thyroid cancer than the antibiotic nonuser group (aHR, 1.71; CI, 1.65–1.78). Individuals who took five or more antibiotic classes had a greater risk of thyroid cancer than those who took only one class (aHR, 1.37; CI, 1.34–1.41).
Association between a particular class of antibiotics and thyroid cancer
Thyroid cancer risk according to a specific class of antibiotics is shown in eTable 11 in Supplementary Data. In comparison with the antibiotic nonuser group, sulfonamide-only group (aHR, 1.31; CI, 1.12–1.53), cephalosporin-only group (aHR, 1.12; CI, 1.09–1.15), macrolide-only group (aHR, 1.11; CI, 1.06–1.17), tetracycline-only group (aHR, 1.11; CI, 1.03–1.20), penicillin-only group (aHR, 1.10; CI, 1.08–1.13), or fluoroquinolone-only group (aHR, 1.08; CI, 1.05–1.12) were, respectively, associated with a higher risk of thyroid cancer.
Discussion
The results of this longitudinal study suggest that the cumulative days of antibiotic prescription may be associated with thyroid cancer incidence in a duration-dependent manner. This association is maintained after adjustments for possible confounding factors and in multiple sensitivity analyses. To our best knowledge, this is the first nationally representative study in Asia to report that long-term antibiotic use may be one of the risk-enhancing factors for thyroid cancer using real-world data.
In a previous study that studied stool microbial composition among patients with thyroid cancer, the microbial composition in thyroid cancer patients significantly differed from the control group. 18 In detail, thyroid cancer samples showed reduced fecal microbiota richness and diversity, which suggests an imbalance in the gut microbiota in thyroid cancer patients. 18 Moreover, the abundance of Proteobacteria in the gut was higher in thyroid cancer patients compared with healthy controls. 18
Another study reported that the gut microbiota of thyroid cancer patients was dominated by Prevotella, Roseburia, Coprococcus, Anaerostipes, Ruminococcus, Neisseria, Streptococcus, and Porphyromonas characteristically. 19 Lactobacillus, which promotes the uptake of selenium and is thus greatly important in maintaining intracellular selenium levels, was found to be significantly reduced in the gut among thyroid cancer patients. 40
Selenium contributes to the production of thyroid hormones and the avoidance of oxidative damage to the thyroid gland. Reduced selenium level was associated with a higher thyroid cancer stage. 41 Therefore, many studies that exhibited qualitative and quantitative changes in the gut bacteria in thyroid cancer patients elucidated the existence of the gut–thyroid axis and the connection between gut dysbiosis and thyroid cancer. Imbalances in the intestinal microbiota can also affect the uptake of iodine, and iodine deficiency can induce the appearance of thyroid nodules, thus increasing the risk of thyroid cancer development. 42
A previous study reported that an increased number of inflammatory and carcinogenic bacterial strains were found in thyroid cancer patients. 11 In our study, the correlation between antibiotics and thyroid cancer risk could potentially be attributable to the alteration of gut and thyroid microbiota. Antibiotic accumulation may have induced dysbiosis of the gut microbiota, leading to systemic inflammation and the formation of toxic metabolites in the thyroid. 20
Thyroid had long been regarded as sterile. As next-generation sequencing developed, the presence of robust microbiota in the thyroid was revealed. Thyroid tumor tissues were found to have lower thyroid microbiota diversity and richness compared with peritumoral tissues. 9 In particular, the genus Acinetobacter was enriched in thyroid cancer tissues. 9 Acinetobacter is generally known as an important pathogen, and various studies have proposed its relevance to the carcinogenesis of multiple malignancies. 21,43 Similar to the gut microbiome, increased pathogenic bacteria in thyroid microbiota may promote chronic inflammation within the thyroid. A chronic inflammatory environment induces carcinogenesis by causing cell proliferation, mutation, and apoptosis. 44
There are other potential explanations that could support our results. First, antibiotics may act as a carcinogen. 16 Antibiotics could serve as both physical and chemical carcinogens by altering the normal microbiota to a carcinogenic environment, consequently inducing cancer. 45 In our study, most of the antibiotic classes were independently associated with an increased risk of cancer, except for lincosamides and vancomycin.
Second, diseases caused by gut and thyroid dysbiosis in accordance with prolonged antibiotic use may have led to a higher risk of thyroid cancer. Gut dysbiosis is known to elicit inflammation and thyroid diseases such as Hashimoto's thyroiditis, Graves' disease, and thyroid nodules. 46 –50 Moreover, the association of Hashimoto's thyroiditis and Graves' diseases with thyroid cancer provides evidence that gut dysbiosis due to long-term antibiotic prescription causes thyroid cancer. 51 –53
A recent study has also discovered that gut microbiota correlated with the presence of thyroid nodules and the carcinogenesis that can lead thyroid nodules to thyroid cancer. 50 Thus, antibiotics may have played a role in both initiating tumorigenesis and stimulating the proliferation of formerly existing tumor sites.
There are limitations to this study. First, we did not have the specific detailed clinical states of each patient, including cancer stage and histopathological type, due to the limitations of the administrative database. Second, although adjustments were conducted for various potential confounding factors regarding thyroid cancer in the statistical models, residual confounders that are not accounted for analysis may exist as an inherent limitation of retrospective studies.
The underlying diseases of the patients that were not included as confounders in our analyses could have led to systemic inflammation and gradually induced thyroid cancer. We also could not consider the change over time of variables such as smoking status and alcohol intake. Instead, we tried to minimize these limitations by re-extracting and analyzing information at each time point through sensitivity analyses that accounted for changes in exposure and follow-up periods. Third, there can be limitations in generalizing our findings to other ethnicities or countries.
Furthermore, South Korea is known for the overdiagnosis of thyroid cancer. 54,55 Therefore, the context of overdetection in South Korea should be carefully considered when interpreting thyroid cancer risk according to antibiotic exposure. Finally, although the relationship between the usage of antibiotics and the risk of thyroid cancer was discovered through our study, this retrospective cohort study could not conclude causation but only association because of the observational study design.
However, we tried to interpret our study using Bradford Hill criteria for establishing a causal link. 56 In the authors' opinion, this study could meet the criteria, including strength (effect size), consistency (same association in different populations), temporality (antibiotic exposure precedes the incidence of thyroid cancer), biological gradient (duration-dependent relationship), and plausibility (biological mechanisms).
However, this study could not meet the criteria of specificity (residual contribution), coherence (need for compatibility with epidemiological and experimental studies), experimental evidence (need for clinical and experimental studies), and analogy (need for other potential exposure variables). Therefore, further experimental and epidemiological research is necessary to confirm a clear causal effect.
Several strengths of this research include the reasonable approach to investigating the relationship between antibiotic exposure and thyroid cancer. The large sample size raises the credibility of our study and may enable us to perform the stratified analysis with sufficient power. The prolonged thyroid cancer follow-up also supports the validity of this study. Moreover, we aimed to conduct a comprehensive study by adjusting for an extended range of confounders, including sociodemographic factors, health-related habits, health status, thyroid-related diseases, and the number of head and neck CT scans. Finally, the robustness of major findings was maintained in multiple sensitivity analyses.
This nationwide cohort study suggests a possible duration-dependent association between antibiotic prescription days and the risk of thyroid cancer. Future biological studies that elucidate the relationship between antibiotic exposure and the incidence of thyroid cancer, which could potentially be linked to alterations of the thyroid and gut microbiota, are needed to validate our conclusions and understand the underlying pathophysiology.
Footnotes
Authors' Contributions
Concept and design by S.J.P., M.K., S.J., Y.J.P., S.C., J.C., and S.M.P. Acquisition, analysis, or interpretation of data by S.J.P., M.K., S.J., and Y.J.P. Drafting of the article by S.J.P. and M.K. Critical revision of the article for important intellectual content by Y.J.P., S.C., J.C., Y.H.O., S.W.C., Y.J.P., and S.M.P. Statistical analysis by S.J.P., M.K., and S.J. Funding obtained by S.J.P. and S.M.P. Administrative, technical, or material support by S.J., Y.J.P., S.C., and J.C. Supervision by Y.H.O., S.W.C., Y.J.P., and S.M.P.
Data Availability
The KNHIS provides access to the data; however, confidential data are only available to researchers who meet specified conditions. The database is accessible to any researcher who has been authorized by the KNHIS.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
S.J.P. received a scholarship from the BK21 FOUR education program from the National Research Foundation of Korea (NRF). The funding sources had no role in design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the article.
Supplementary Material
Supplementary Data