
Abstract
Background:
The objective of this study is to evaluate the diagnostic accuracy of 18F-fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT) in detecting recurrence in patients with differentiated thyroid cancer (DTC) who have negative whole-body scans (WBSs) but elevated serum thyroglobulin (Tg) or thyroglobulin antibody (TgAb) levels.
Methods:
This systematic review/meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis for Diagnostic Test Accuracy criteria (International Prospective Register of Systematic Reviews registration number: CRD42022340924). A comprehensive search of the MEDLINE, EMBASE, and Cochrane databases identified articles reporting the diagnostic accuracy of FDG PET/CT for the detection of recurrence in patients with DTC with negative WBS and elevated serum Tg or TgAb levels published between January 2012 and June 2023. Meta-analyses were performed to determine the diagnostic accuracy of FDG PET/CT on the total target population as well as on subgroups stratified by serum Tg or TgAb, and thyrotropin (TSH) stimulation status at the time of FDG PET/CT. The Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) framework was applied to evaluate the quality of evidence and the strength of recommendations to facilitate translation of the meta-analysis results into practical recommendations for clinical guidelines.
Results:
A total of 24 studies involving 1988 patients were included for analysis. The overall pooled sensitivity and specificity values were 0.87 (95% confidence interval [CI] = 0.83–0.92; I 2 = 75%) and 0.84 (CI = 0.80–0.89; I 2 = 44%), respectively. Subgroup analyses revealed no significant differences in the diagnostic accuracy of FDG PET/CT in patients stratified by serum Tg or TgAb levels, and TSH stimulation status at the time of PET/CT. Treatment plans were changed following FDG PET/CT imaging in 40% (CI = 34–47%; I 2 = 39%) of cases. The quality level of evidence for using FDG PET/CT was moderate in both sensitivity and specificity according to the GRADE system.
Conclusion:
There is moderate quality evidence demonstrating the high diagnostic accuracy of FDG PET/CT in detecting recurrence in patients with DTC with negative WBS and elevated serum Tg or TgAb levels. This evidence corroborates the current guidelines' endorsement of FDG PET/CT as a diagnostic tool in such patients.
Introduction
18
F-
In particular, a negative radioiodine whole-body scan (WBS) raises the suspicion of persistent or recurrent DTC without obvious clinical presentation of disease. 1 Thus, appropriate diagnostic imaging is essential to facilitate accurate diagnosis and guide suitable treatment planning.
Most current guidelines recommend FDG PET imaging for the diagnosis of patients with DTC with suspected recurrence. 2 –5 However, the evidence cited by these guidelines was based on earlier clinical studies that were conducted using PET-dedicated imaging systems with a wide range of reported diagnostic accuracy. 6 Recently reported meta-analyses demonstrated the high diagnostic accuracy of FDG PET imaging for the detection of recurrence. 7 –11 Nonetheless, in the previous meta-analyses, the criteria for the use of FDG PET may have varied regarding Tg or TgAb levels and thyrotropin (TSH) stimulation status.
The current meta-analysis was conducted to assess the diagnostic accuracy of FDG PET/CT in detecting recurrence in patients with DTC with negative WBS and elevated serum Tg or TgAb levels. The Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) framework was applied to facilitate the translation of the study results into practical recommendations for clinical guidelines. 12
Materials and Methods
We performed this systematic review/meta-analysis following the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analysis for Diagnostic Test Accuracy guidelines. 13 The protocol was registered a priori in the International Prospective Register of Systematic Reviews (registration number: CRD42022340924).
A comprehensive search of the MEDLINE, EMBASE, and Cochrane databases was conducted to identify relevant articles published between January 1, 2012 and April 29, 2022. We updated the search on June 27, 2023. The search strategy included synonyms and related terms for “thyroid cancer” and “PET/CT” (Supplementary Text S1).
Two investigators (J.-I.B. and S.W.O) independently examined the titles and abstracts of the initial search results and selected studies for full-text review. The inclusion criteria were as follows: (a) patients with DTC who underwent thyroidectomy followed by radioiodine therapy and had negative WBS and elevated serum Tg or TgAb levels, (b) FDG PET/CT was used as the index test, (c) pathologic confirmation and/or clinical follow-up was used as the reference standards, and (d) adequate data were available for the construction of a 2 × 2 contingency table required for calculation of diagnostic accuracy.
The exclusion criteria were (a) duplicated articles; (b) case reports, abstracts, letters, editorials, review, or guideline; and (c) non-English full-text articles. If there were insufficient data for the construction of 2 × 2 contingency tables, the researchers contacted the corresponding authors of the relevant articles to request additional data.
One investigator extracted descriptive data from the included studies, and another investigator corroborated the extracted data. The following study characteristics were extracted: criteria for elevated serum Tg/TgAb levels and the FDG PET/CT protocols; and the following patient characteristics were extracted: age at diagnosis, histological type and stage of DTC, cumulative activity of radioiodine patient received previously, pathological results, and clinical follow-up outcomes, as well as location of recurrence and change in treatment plans based on FDG PET/CT findings.
Several studies conducted comparative evaluations of the diagnostic accuracy of neck magnetic resonance imaging (MRI) or neck ultrasonography (US) for the detection of recurrence. 14 –16 Data pertaining to 2 × 2 contingency tables for neck MRI or neck US were also collected.
Two independent investigators assessed the methodological quality of the included studies, utilizing the Quality Assessment of Diagnostic Accuracy Studies-2 tool. 17 Any disagreements that arose during the assessment were resolved through discussion. Further, we employed the GRADE framework to evaluate the strength and certainty of the body of evidence. 12
Statistical analysis
Pooled sensitivity and specificity with corresponding 95% confidence intervals (CIs) were calculated using bivariate statistical models. A hierarchical summary receiver operating characteristic (HSROC) plot was produced using pooled data. A random-effects model was used for analyses with more than four articles, and a fixed-effects model was used for analyses with only three articles.
Subgroup analyses of sensitivity and specificity were conducted in groups with (a) TSH-stimulated status, (b) TSH-suppressed status, (c) elevated serum Tg levels and normal serum TgAb levels, (d) elevated serum TgAb levels, and (e) TSH-stimulated serum Tg level above 10 ng/mL. Deeks' Funnel Plot Asymmetry Test was conducted to evaluate potential publication bias. 18 The rate of change in treatment plans following FDG PET/CT was calculated. The relative sensitivity and specificity were calculated to compare the diagnostic accuracy of FDG PET/CT and neck MRI or US. 19 A p-value of 0.05 was considered significant.
All statistical analyses were performed using R 4.0.2 software (R Foundation for Statistical Computing, Vienna, Austria) and Stata 17.0 (StataCorp LP, College Station, TX, USA). Assessment of the quality of each article was conducted using Review Manager software version 5.4 (The Cochrane Collaboration, London, UK). Summaries of research evidence were generated using GRADEpro GDT (GRADEpro Guideline Development Tool, McMaster University and Evidence Prime, 2022).
Results
Characteristics of included studies
The database search yielded 1988 articles, and a total of 24 articles were ultimately included in the review and meta-analysis (Fig. 1). 14 –16,20 –40 There were two articles with overlapping patient cohorts. 25,39 The study with the larger cohort 25 was selected for the main analysis; the study with the smaller cohort, 39 which included patients with elevated serum TgAb only, was included in a subgroup analysis. The characteristics of the included studies, patient populations, PET/CT protocols, and details of reference standard are summarized in Tables 1 and 2 and Supplementary Tables S1–S3.
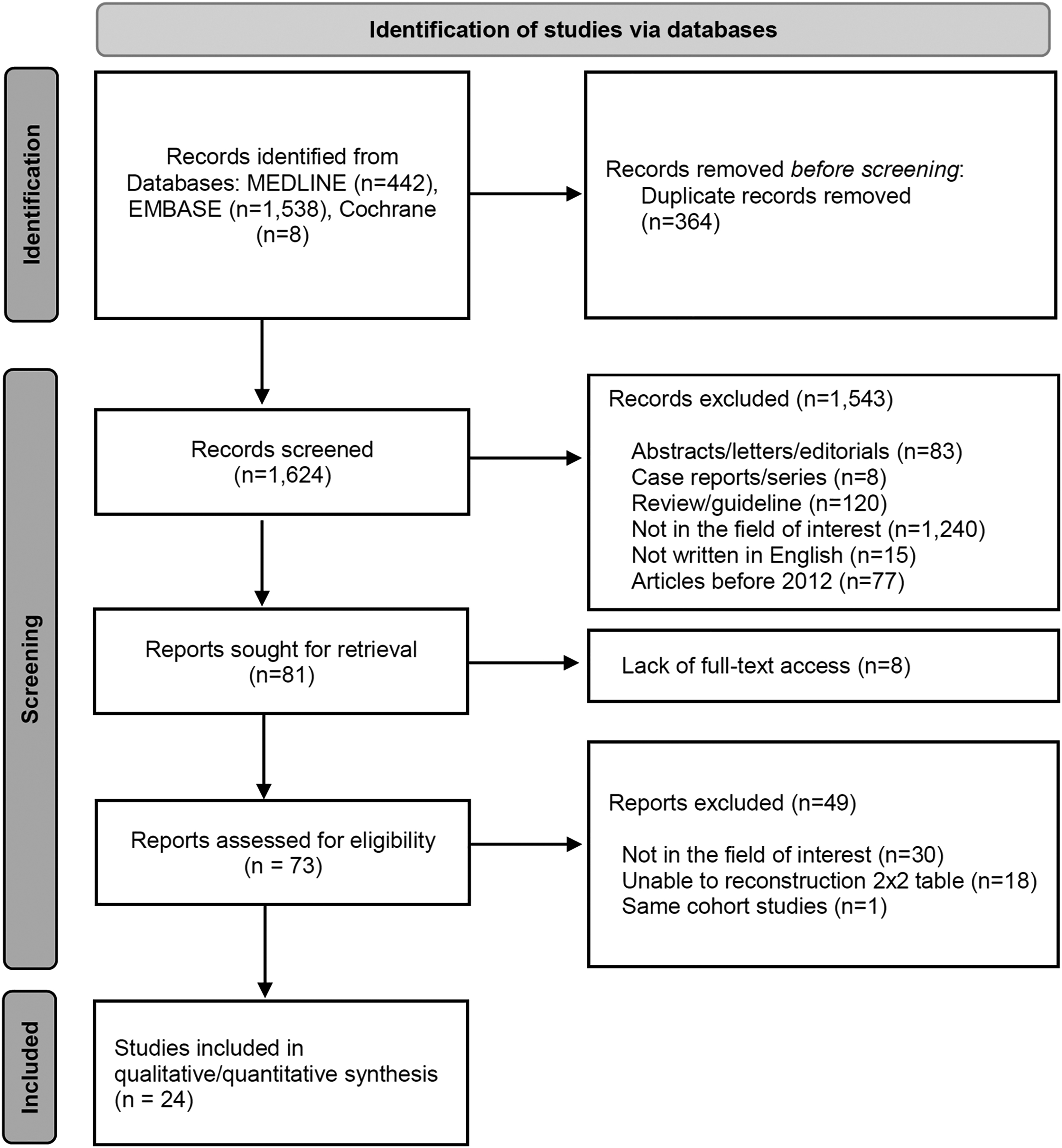
Preferred Reporting Items for Systematic Reviews and Meta-Analysis flow diagram depicting the study selection process.
Characteristics of the Included Studies
Normal ragne of TgAb is 0–115 IU/mL.
Some patients overlap between studies. Ozkan et al. 25 were included in the meta-analysis of total studies; Ozkan et al. 39 were included in the subgroup analysis.
CT, computed tomography; sTg, stimulated thyroglobulin; sTgAb, stimulated anti-thyroglobulin antibody; supTg, suppressed serum thyroglobulin; supTgAb, suppressed serum anti-thyroglobulin antibody; Tg, thyroglobulin; TgAb, anti-thyroglobulin antibody; US, ultrasonography.
Demographic Data and Clinical Characteristics of Study Populations
Data were presented as mean ± standard deviation; meana or medianc or (range).
Suppressed TgAb for 27 patients; sTgAb for 13 patients.
Total number of included patients were 84; the demographic data were only for 75 patients who showed elevated serum Tg level. The nine patients showed elevated serum TgAb level.
Serum TSH levels were between 0 and 100 (63.86 ± 38.98).
60 Patients with 68 FDG PET/CT cases, 65 cases with elevated stimulated serum Tg, and 3 cases with elevated stimulated serum TgAb and stimulated serum Tg <2 ng/mL.
Patients with increased stimulated serum Tg levels.
Patients with increased stimulated serum TgAb levels.
One patient had an increase in both Tg and TgAb.
Aggre.variant, aggressive variant; FDG, 8 F-fluorodeoxyglucose; FTC, follicular thyroid cancer; FV-PTC, follicular-variant papillary thyroid cancer; IQR, interquartile range; n/a, not available; PD, poorly differentiated; PET/CT, positron emission tomography/computed tomography; PTC, papillary thyroid cancer; rhTSH, recombinant human thyrotropin; TSH, thyrotropin.
Fifteen of the studies 14 –16,20,21,26 –28,30,33 –38 employed specified but heterogenous criteria to define elevated serum Tg or TgAb levels, whereas for 8 of the 9 remaining studies, 22 –25,29,32,39,40 the criteria were deduced using the mean and standard deviation values provided in the article (Supplementary Table S1). Nineteen studies reported the subtype of DTC, and more than 50% of the cases were classified as papillary thyroid cancer. 14 –16,23 –28,31 –40
Five studies reported information about the stage of DTC or risk of recurrence, although they did not provide specific diagnostic outcomes based on stage or risk. 14,24,31,36,38 Two articles relied solely on pathologic confirmation as the reference standard, 15,26 and the remaining 22 studies employed either pathologic confirmation and/or clinical follow-up.
Three studies 14,16,22 assessed only local tumor recurrence, whereas the remaining 21 studies evaluated both local and distant metastasis. Five studies reported no structural indications of recurrence by conventional imaging techniques at the time of the FDG PET/CT evaluation, 14,16,21,29,30 and one study included some patients with suspicious lesions identified by neck ultrasound or CT. 25
Quality assessment
The results of the quality assessment are summarized in Supplementary Figure S1. Fifteen studies had an indeterminate risk of bias owing to inadequate reporting about patient selection related to consecutive enrollment. 15,22,23,25 –27,29,31 –34,37 –40 Moreover, because of insufficient information about blinding, all studies had an uncertain risk of bias in the domains of the index test or reference standard. However, given the inherent clinical nature of DTC, bias resulting from unblinded index tests or reference standards would likely be minimal.
Diagnostic accuracy of FDG PET/CT
The pooled total sensitivity and specificity values of FDG PET/CT for detecting recurrence in patients with negative WBS and elevated serum Tg or TgAb were 0.87 (CI = 0.83–0.92; I 2 = 75%) and 0.84 (CI = 0.80–0.89; I 2 = 44%), respectively (Fig. 2A). Subgroup analysis of the 20 studies that investigated both local and distant metastasis showed pooled sensitivity and specificity values of 0.88 (CI = 0.84–0.93; I 2 = 74%) and 0.83 (CI = 0.78–0.89; I 2 = 42%), respectively (Fig. 2B). Figure 3 shows the HSROC curve, with an area under the curve of 0.88.
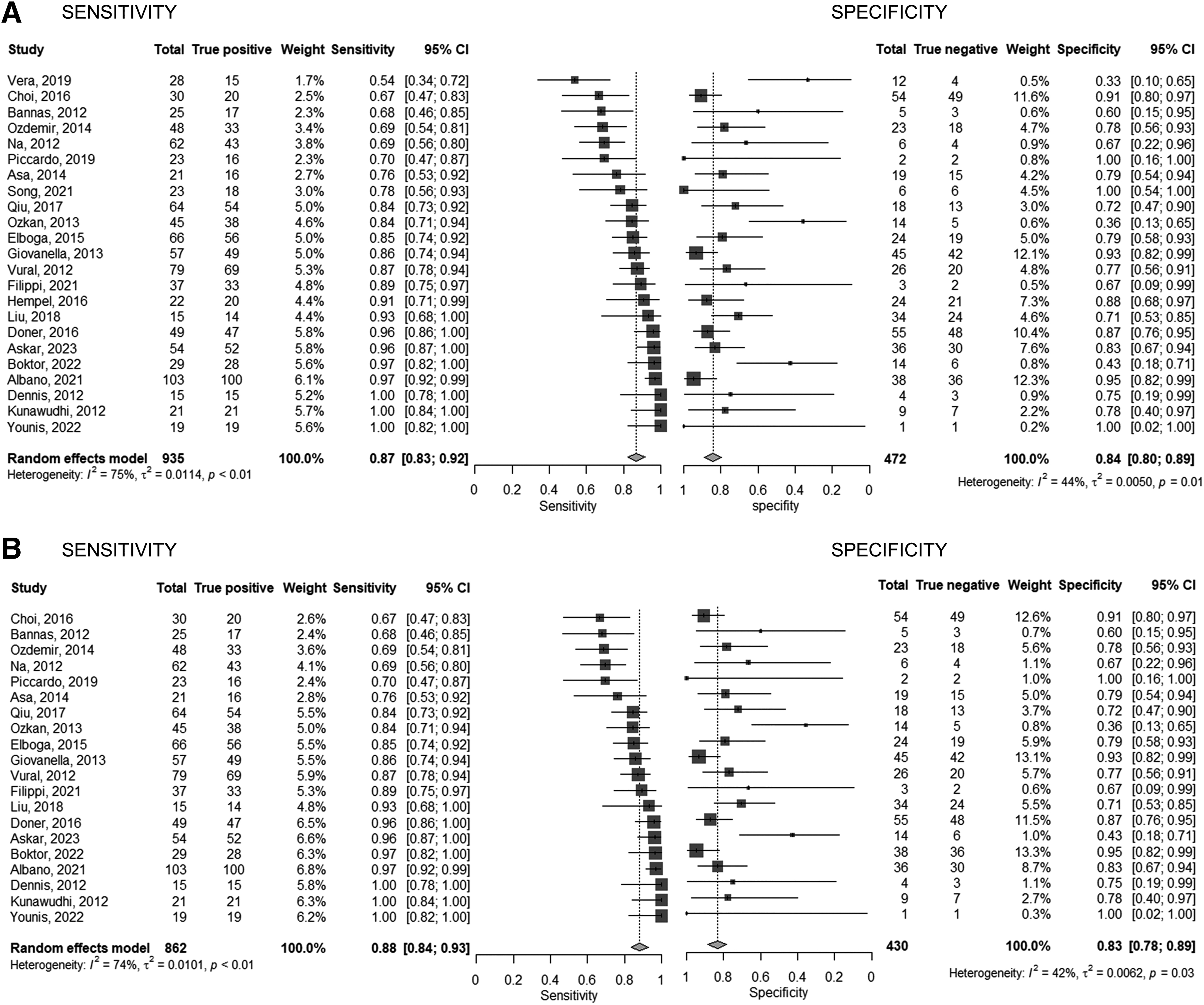
Meta-analysis examining the diagnostic accuracy of FDG PET/CT scans for detecting recurrence in patients with differentiated thyroid cancer with negative radioiodine whole-body scans but elevated serum Tg or TgAb levels. (
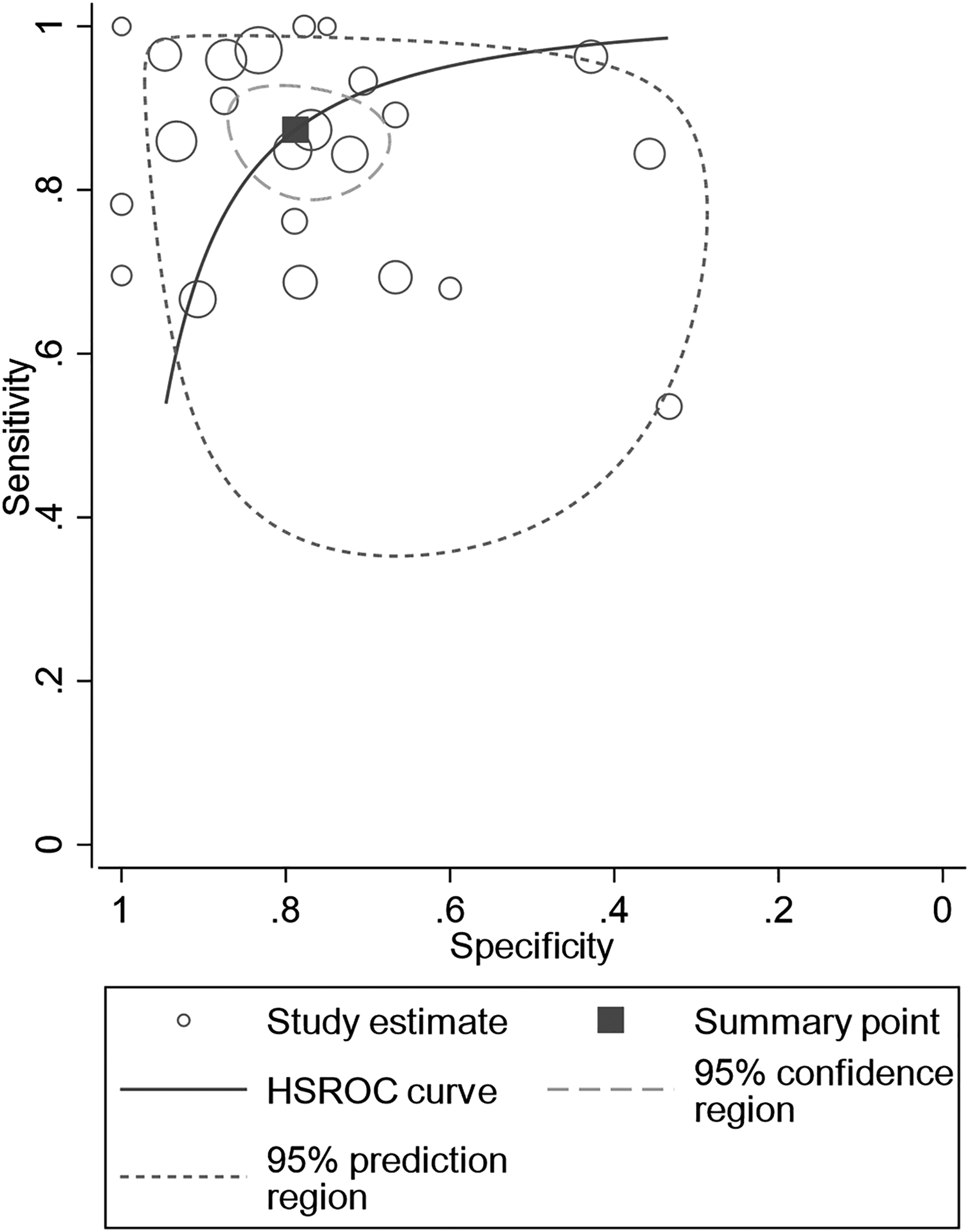
Hierarchical summary receiver operating characteristic curve of FDG PET/CT scan for detecting recurrence in patients with differentiated thyroid cancer with negative radioiodine whole-body scans but elevated serum Tg or TgAb levels.
Subgroup analysis of patients stratified by TSH stimulation status at the time of the scan showed that sensitivity and specificity values for TSH-stimulated patients were 0.84 (CI = 0.72–0.97; I 2 = 78%) and 0.84 (CI = 0.73–0.97; I 2 = 33%), respectively. The corresponding values for TSH-suppressed patients were 0.86 (CI = 0.80–0.92; I 2 = 78%) and 0.87 (CI = 0.82–0.92; I 2 = 31%), respectively (Fig. 4A, B).
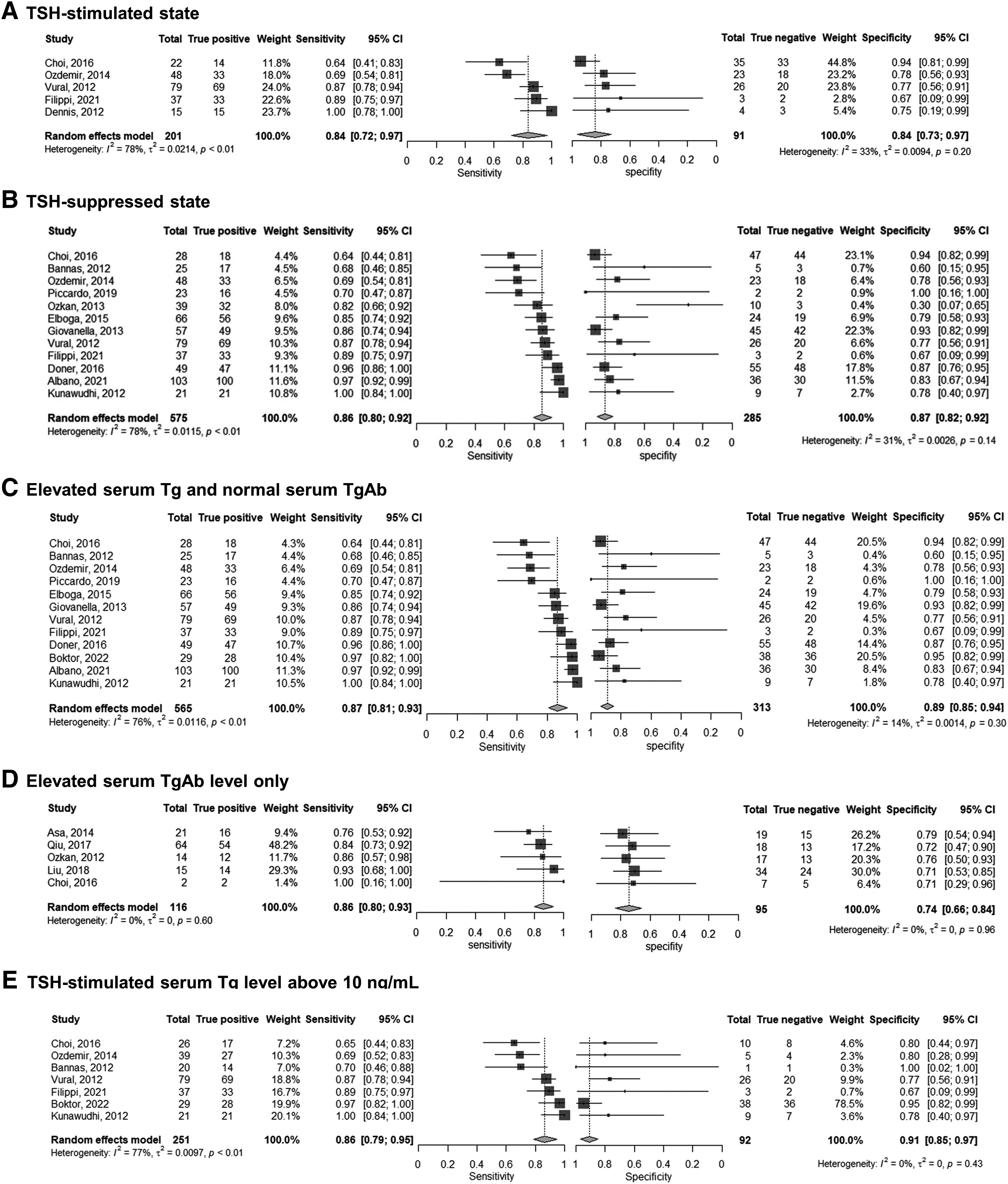
Meta-analyses examining the diagnostic accuracy of FDG PET/CT in detecting recurrence in patients with differentiated thyroid cancer in the following subgroups of patients: (
The pooled diagnostic accuracy of FDG PET/CT was also evaluated in subgroups of patients stratified by elevated serum Tg or TgAb status. In patients with elevated serum Tg, the pooled sensitivity and specificity values were 0.87 (CI = 0.81–0.93; I 2 = 76%) and 0.89 (CI = 0.85–0.94; I 2 = 14%), respectively.
In patients with elevated serum TgAb, the pooled sensitivity and specificity values were 0.86 (CI = 0.80–0.93; I 2 = 0%) and 0.74 (CI = 0.66–0.84; I 2 = 0%), respectively (Fig. 4C, D). To account for the heterogeneity in the criteria for elevated levels of serum Tg or TgAb, only studies that evaluated patients with TSH-stimulated serum Tg levels above 10 ng/mL were included in the analysis. The resulting pooled sensitivity and specificity values were 0.86 (CI = 0.79–0.95; I 2 = 79%) and 0.91 (CI = 0.85–0.97; I 2 = 0%), respectively (Fig. 4E).
Impact on treatment change
Six studies reported the rate of treatment change following FDG PET/CT. 15,21,27,30,34,35 The scope of treatment change was not only limited to alterations in the administration of radioiodine, 15,21,27,34 but also included decisions to pursue curative-intent surgery for recurrent tumors, 15,27,34,35 change from local treatment to systemic treatment, 21,34,35 and conversion to external radiation treatment. 27,34 Pooled analysis revealed that the overall rate of treatment change following FDG PET/CT was 40% (CI = 34–47%; I 2 = 39%) (Fig. 5).
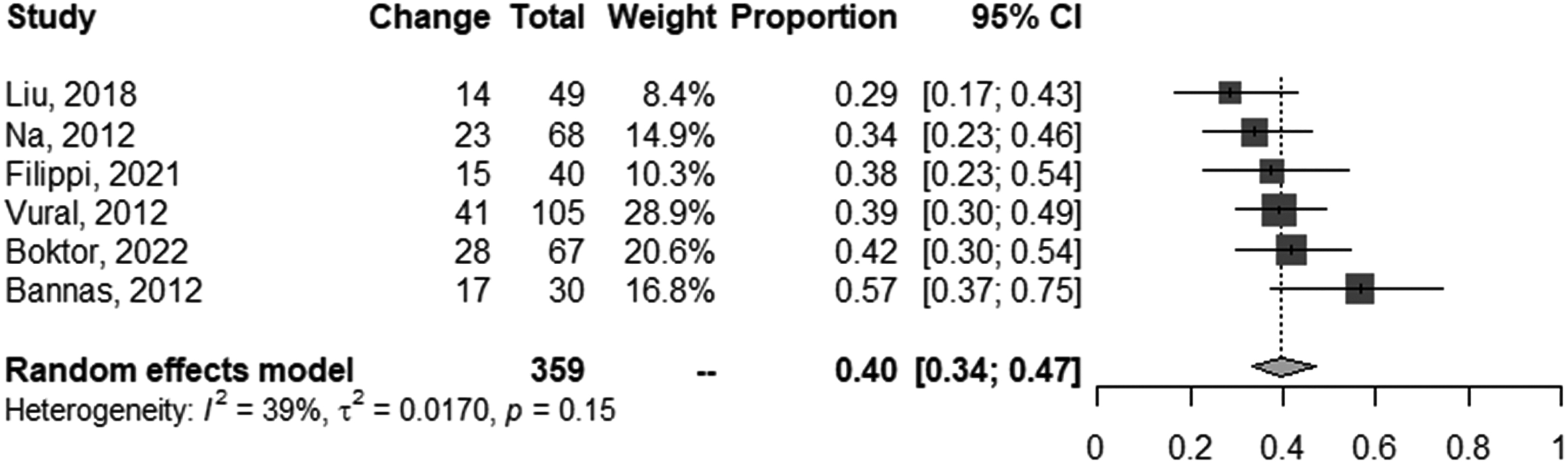
Meta-analysis examining the rate of treatment change following FDG PET/CT.
Location of recurrence detected by FDG PET/CT
Ten studies reported the site of recurrence detected using FDG PET/CT. The most common site of recurrence was the locoregional recurrence only (62.0%), followed by concurrent locoregional recurrence and distant metastases (12.5%), and distant metastases in the absence of locoregional recurrence [mediastinal lymph node metastases (10.5%), pulmonary metastases (8.4%), bone metastases (6.3%), and other distant metastases (1.0%)]. 16,23,25 –27,29,30,32,35 About 38.7% of patients had either distant metastases in the absence of locoregional recurrence or a concurrent locoregional recurrence and distant metastases.
Comparisons with structural imaging
The diagnostic performance of FDG PET/CT and neck MRI in detecting local recurrence compared two paired-design studies using a fixed-effect model. 14,16 The pooled sensitivity and specificity values for FDG PET/CT were 0.70 (CI = 0.56–0.81) and 0.69 (CI = 0.53–0.82), respectively. In contrast, the pooled sensitivity and specificity values of neck MRI were 0.50 (CI = 0.35–0.65) and 0.49 (CI = 0.35–0.63), respectively.
Although the difference in diagnostic performance between FDG PET/CT and neck MRI did not reach statistical significance, the relative sensitivity and specificity values of FDG PET/CT compared with neck MRI were 1.40 (CI = 0.98–2.00, p > 0.05) and 1.42 (CI = 0.98–2.05, p > 0.05), respectively.
Two studies compared the diagnostic performance of FDG PET/CT with neck US in detecting local recurrence. 15,16 However, one study solely reported the diagnostic outcomes of FDG PET/CT for both local and distant metastases. 15 So, pooled sensitivity and specificity estimates were calculated separately for FDG PET/CT 14,16,22 and neck US 15,16 with a fixed-effect model.
The pooled sensitivity and specificity values of FDG PET/CT were 0.73 (CI = 0.61–0.82) and 0.74 (CI = 0.59–0.85), respectively. Conversely, the pooled sensitivity and specificity values of neck US were 0.48 (CI = 0.34–0.62) and 0.67 (CI = 0.52–0.79), respectively. Although the difference in diagnostic accuracy between FDG PET/CT and neck US was not statistically significant, the relative sensitivity and specificity values of FDG PET/CT compared with neck US were 1.49 (CI = 0.85–2.60, p > 0.05) and 1.19 (CI = 0.64–2.23, p > 0.05), respectively.
Grading of evidence quality
The results of the quality of evidence assessment are summarized in Supplementary Table S4. No significant publication bias was detected using Deeks' Funnel Plot Asymmetry test (p = 0.09; Supplementary Fig. S2). As inconsistency was identified, according to the GRADE system, the overall quality of evidence was evaluated to be moderate for both sensitivity and specificity.
Discussion
Several current guidelines advocate the use of FDG PET for diagnosing patients with DTC with suspected tumor recurrence or metastasis, with negative WBS, and elevated serum Tg or TgAb levels. 2,4,5 However, the evidence cited in guidelines included studies with single-modality PET-scanners, which are now outdated and thus, an updated synthesis of the current evidence was necessary.
We conducted a systematic review and meta-analysis of articles published in the past decade that reported the diagnostic accuracy of FDG PET/CT systems in the same target population. The results of the present study align with the results of previous analyses, including single-modality PET-scanners, 7 –11 and demonstrate that FDG PET/CT has a moderate-to-high degree of sensitivity and specificity in this population.
Subgroup analyses of patients stratified by serum Tg or TgAb, serum Tg level, and TSH stimulation status at the time of the FDG PET/CT scan consistently indicated that the diagnostic performance of FDG PET/CT had sensitivity and specificity rates of ∼85%. There were no significant differences in the diagnostic accuracy of FDG PET/CT when stratifying patients based on their TSH stimulation status at the time of the scan.
These findings are consistent with an earlier meta-analysis investigating FDG PET/CT diagnostic accuracy in patients with DTC with negative WBS and elevated serum Tg levels. 11 However, considering that the methods of TSH stimulation (endogenous vs. recombinant human TSH) varied among the studies, methods of TSH stimulation could impact the results. Further, the diagnostic accuracy of FDG PET/CT did not vary significantly in groups of patients stratified by either elevated serum Tg or elevated TgAb.
The included studies did not provide sufficient data to determine an optimal cutoff value for serum Tg or TgAb elevation to indicate when FDG PET/CT should be performed. Some studies reported an association between the diagnostic performance of FDG PET/CT and higher serum Tg levels, 26,33,35 which could potentially signify a greater tumor burden. 41
However, most studies arbitrarily suggested cutoff values of 2, 5, or 10 ng/mL for serum Tg, either stimulated or suppressed, and the evidence for these values was not robust. We performed a subgroup analysis in studies that specified stimulated serum Tg levels exceeding 10 ng/mL as the cutoff, which represented the largest number of eligible studies in our dataset. 21,26,28,30,33,35 However, further research is needed to establish an optimal cutoff value for serum Tg or TgAb levels to effectively guide the use of FDG PET/CT in patients with DTC with suspected tumor recurrence or metastasis.
We found that treatment plans were changed following FDG PET/CT in 39% of patients with DTC with suspected tumor recurrence. However, these results should be cautiously interpreted because we did not include this clinical condition as a primary search term in the initial literature search. Although conducted in a different patient population with different clinical circumstances, Filippi et al. reported that the rate of treatment change following FDG PET/CT was 50% in patients with DTC and suspicion of structural recurrence. 30
We found no significant differences in the diagnostic accuracy of the FDG PET/CT, neck MRI, or neck sonography in patients with DTC and suspicion of recurrence. Nevertheless, due to limitations of small sample sizes and study designs that lacked clear indications of index test blindness, the current evidence is insufficient to provide conclusive results.
The American Thyroid Association's (ATA) 2015 guidelines for DTC in adults indicate that FDG PET/CT may be beneficial following neck CT, chest CT, or neck sonography, 4 but to date, no studies have directly compared the diagnostic accuracy of FDG PET/CT with that of neck CT or chest CT. Although a limited number of studies have reported negative findings detected by neck US or chest CT, their sample sizes were small, and the patient groups did not receive the same imaging modalities. 14,16,21,25,29,30,39
Although direct evidence to prioritize imaging modalities for the detection of tumor recurrence is limited, given the potential coexistence of local and distant metastasis, whole-body evaluation using FDG PET/CT may confer an advantage in patients with DTC with suspected tumor recurrence. Further, the FDG-avidity of the tumor may provide supplementary information to help determine an appropriate treatment plan and predict prognosis. 42 –44
We employed the GRADE system to assess both the methodological and overall quality of evidence for using FDG PET/CT. The level of evidence was determined to be moderate for both sensitivity and specificity owing to inconsistency, as indicated by high heterogeneity. It is important to note that in considering the slow glowing nature of thyroid cancer, confirmation of true negative could be subject to bias, as the follow-up duration may be insufficient. Also, as the diagnostic accuracy was measured by patient-based, rather than lesion-based, analysis, the sensitivity estimate could be inflated. 9
The ATA 2015 guidelines recommend FDG PET imaging in patients with structurally complete but biochemically incomplete response to initial therapy, or with indeterminate serum Tg levels and negative WBS, or with high-risk features for recurrent or persistent disease. 4
Although these guidelines specify the use of FDG PET in patients with a high risk of recurrence, these recommendations lacked adequate evidence to specify the group of patients best suited for FDG PET/CT imaging. 6 More research is needed to inform the cut-offs for serum Tg/TgAb levels that may guide more efficient utilization of FDG PET/CT. In future, the diagnostic accuracy of FDG PET/CT should be stratified according to the risk parameters of DTC in patients with suspected recurrence.
Conclusion
This systematic review and meta-analysis offers compelling evidence of the high diagnostic accuracy of FDG PET/CT in detecting recurrence in patients with DTC with negative WBS but elevated serum Tg or TgAb levels.
Footnotes
Authors' Contributions
J.-I.B. contributed to design/acquisition of data/analysis, interpretation of data, and participated in drafting/writing/editing the article. S.P. contributed to conceptualization and reviewing/editing the article. K.K. contributed to conceptualization/design of the study and reviewing/editing the article. Y.S. contributed to conceptualization/design of the study and reviewing/editing the article. A.C. contributed to conceptualization/design of the study and reviewing/editing the article. C.M.H. contributed to conceptualization/design of the study and reviewing/editing the article. M.C. contributed to interpretation of the data and editing the article. S.-W.L. conceived and designed the study and provided a critical revision to the article. S.W.O. contributed to design/acquisition of data/analysis, interpretation of data, participated in writing/editing the article, and provided critical revisions to the article.
Author Disclosure Statement
J.-I.B., S.P., K.K., Y.S., A.C., C.M.H., M.C., S.-W.L., and S.W.O. declare that they have no conflict of interest.
Funding Information
This work was supported by the National Cancer Center Grant (NCC-2112570-1).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Text S1