
Abstract
Background:
The optimal extent of surgery for unilateral papillary thyroid carcinoma (PTC) with contralateral nodules remains unclear. This study evaluated the long-term outcomes in a large cohort of patients with unilateral PTC and contralateral low-to-intermediate suspicious nodules who underwent lobectomy.
Methods:
This retrospective cohort study included patients with unilateral PTC who underwent lobectomy between January 2016 and December 2017 at Asan Medical Center in Korea. Patients were divided into two groups, those with and without contralateral nodules at the time of lobectomy: the Present group and the Absent group. All contralateral nodules observed at the time of surgery and during follow-up were evaluated.
Results:
The study cohort consisted of 1761 patients (1879 nodules), including 700 (39.8%) with and 1061 (60.2%) without contralateral nodules. The median size of the contralateral nodules was 0.5 cm. After a median follow-up of 59 months, the median growth of the contralateral nodules in the Present group was 0.1 cm (range, −3.4 to 4.7 cm). Of the contralateral nodules present at the time of lobectomy, 54.7% remained unchanged, decreased in size, or disappeared; whereas 14.8% increased ≥0.3 cm. Of the 700 patients with contralateral nodules, 20 (2.9%) were diagnosed with contralateral PTC. The 5-year contralateral PTC disease-free survival rates in patients with and without contralateral nodules were 98.2% and 99.3% (p = 0.003), respectively, whereas the 5-year recurrence-free survival rates did not differ significantly in these two groups. Of the 39 patients who underwent completion thyroidectomy, 2 (5.1%) experienced permanent hypocalcemia.
Conclusions:
Lobectomy may be a safe and feasible initial treatment option for patients with unilateral low-risk PTC and contralateral low-to-intermediate suspicious nodules.
Introduction
Papillary thyroid carcinoma (PTC) has an indolent clinical course and excellent prognosis. 1 The increased use of highly sensitive ultrasonography has increased the incidental detection of PTCs and small thyroid nodules worldwide. 2 –4 This has increased the economic burden of PTC and treatment-related side effects, 5 –7 making it important to consider both oncologic safety and quality of life when determining the appropriate extent of surgery for patients with PTC.
Understanding the long-term outcomes of patients with PTC and nodules in the contralateral lobe is essential for optimizing patient care and making informed decisions about the extent of surgery. The 2015 American Thyroid Association (ATA) guidelines 8 and the National Comprehensive Cancer Network guidelines (version 2.2023) 9 have recommended completion or total thyroidectomy in patients with PTC and contralateral nodules due to the possibility of bilateral disease and to facilitate follow-up monitoring. Previous studies have evaluated the natural course of nonsuspicious contralateral nodules, but less is known about the natural course of disease in patients with contralateral intermediate suspicious nodules, 10,11 which have a malignancy risk of 10–50%. 12 Comparable recurrence rates and survival after lobectomy have been observed in patients with PTC with and without intermediate suspicious contralateral nodules. 13 Nevertheless, determining the appropriate surgical approach for patients with PTC and low-to-intermediate suspicious nodules in the contralateral lobe remains unclear.
This study was designed to evaluate the long-term outcomes after lobectomy in a large cohort of patients with PTC and contralateral nodules, including intermediate suspicious nodules. This study also analyzed the risk factors associated with the diagnosis of contralateral PTC and the progression of contralateral nodules.
Materials and Methods
Study design and data collection
The electronic medical records of Asan Medical Center, a tertiary referral center in Seoul, South Korea, were retrospectively searched to identify patients with unilateral PTC who underwent lobectomy between January 2016 and December 2017. All contralateral nodules observed at the time of surgery and during follow-up were evaluated. Patients were divided into two groups, those with and without contralateral nodules at the time of surgery: the Present group and the Absent group. We excluded patients with involved resection margins after lobectomy, patients followed-up for <24 months, and patients who underwent immediate completion thyroidectomy. This study was approved by the institutional review board of Asan Medical Center (No. 2022-0707), and the institutional review board waived the requirement for informed consent due to the retrospective nature of this study.
Variables obtained from patients' medical records included demographic and clinical characteristics, such as age at diagnosis, sex, and duration of follow-up; histopathologic findings, such as tumor size, PTC variant, multifocality, microscopic/gross extrathyroidal extension (ETE), vascular invasion, co-occurrence of Hashimoto thyroiditis, lymph node metastasis, involvement of resection margins, tumor stage, and ATA initial risk classification; operation records; and follow-up outcomes, including diagnosis of contralateral PTC, tumor recurrence, progression of contralateral nodules, and postoperative complications. Multifocality was defined as the presence of two or more PTC tumor foci in one lobe. Tumor stage was classified according to the American Joint Committee Cancer (AJCC) 8th tumor-node-metastasis (TNM) staging system. 14 ATA initial risk was classified according to the 2015 ATA risk stratification guidelines. 8 Information on contralateral nodules, including their presence or absence at the time of surgery, as well as their size, number, and sonographic features, was also recorded.
Determining the extent of surgery and evaluation of contralateral nodules
The decision on the extent of initial surgery, either total thyroidectomy or lobectomy, was based on several factors, such as primary tumor size and location; clinical risk factors, including gross ETE, lymph node metastasis, and the presence of contralateral nodules; patient factors, including age, comorbidities, and history of radiation exposure, and patient preference. Total thyroidectomy or immediate completion thyroidectomy after initial lobectomy was considered for patients with primary tumors >4 cm in size, bilateral disease, gross ETE, or clinically apparent cervical lymph node metastasis, especially lateral lymph node metastasis.
Nodules detected in the contralateral lobe before the initial surgery were subject to fine needle aspiration biopsy and cytologic examination, depending on the size and category of these nodules, as described by the 2016 Korean Thyroid Imaging Reporting and Data System (K-TIRADS). 15 Intermediate suspicion (K-TIRADS 4) nodules were cytologically examined if they were ≥1 cm in size; low suspicion nodules (K-TIRADS 3) were examined if they were ≥1.5 cm in size; and benign nodules (K-TIRADS 2) were examined if they were ≥2 cm in size. Additionally, cytological examinations were performed upon patient request or if there was strong clinical suspicion. The extent of surgery was determined based on the Bethesda system for Reporting Thyroid Cytopathology. Patients with contralateral nodules classified as Bethesda category IV to VI underwent total thyroidectomy. If the contralateral nodules were classified as Bethesda category I to III, the decision to perform total thyroidectomy was based on sonographic pattern and patient preference.
Monitoring and management following initial lobectomy
Patients were initially followed-up 3–6 months after initial lobectomy, with examinations every 6–12 months thereafter. Serum concentrations of thyrotropin (TSH), free thyroxine (fT4), thyroglobulin, and anti-thyroglobulin antibody were measured as described. 16,17 The reference ranges for TSH and fT4 were 0.4–4.5 mIU/L and 0.80–1.90 ng/dL, respectively. Levothyroxine supplementation or TSH suppression was not routinely performed following lobectomy in our institution. 18,19
Neck ultrasound (US) was performed within the first 6–12 months after the initial operation, and every 12 or 24 months thereafter. Abnormal findings on neck US were further evaluated by cytologic examination, with the preoperative cytological criteria applied to any newly developed contralateral nodules. Additional cytological examinations were performed if existing contralateral nodules became highly suspicious, if nodule size increased continuously, if the patient requested further examination despite the nodule remaining stable, or if there were clinical suspicion of malignancy. Treatment plans according to ATA guidelines were based on biopsy results of the contralateral nodules. Other imaging modalities, such as neck and chest computed tomography and 18F-fluorodeoxyglucose-positron emission tomography, were performed if indicated.
Study endpoints
The primary study endpoint was the diagnosis of contralateral PTC and the progression of contralateral nodules. Contralateral PTC was confirmed by fine needle aspiration (FNA) or core needle biopsy. The progression of contralateral nodules was defined by an increase of ≥0.3 cm in the maximal dimension or a change to a highly suspicious appearance.
Key secondary endpoints included tumor recurrence after lobectomy and postoperative complications following completion thyroidectomy. Recurrence after lobectomy was defined as loco-regional recurrence (operative site and cervical lymph node metastasis) or distant metastasis. Contralateral PTC disease-free survival (DFS), recurrence-free survival (RFS), and disease-specific survival (DSS) were calculated.
Statistical analysis
Continuous variables were expressed as median (range), and categorical variables as numbers (n) and percentage (%). Contralateral PTC DFS was calculated from the date of lobectomy to the date of last follow-up, the date of diagnosis of contralateral PTC, or the date of completion thyroidectomy, whichever occurred first. DFS, RFS, and DSS were estimated using the Kaplan–Meier method and compared across subgroups using log-rank tests. Risk factors associated with contralateral PTC, the progression of contralateral nodules, and recurrence were evaluated using univariate and multivariable Cox proportional hazards regression models. The results were presented as hazard ratios (HRs) and 95% confidence intervals (CIs). All tests of significance were two-sided, and p-values <0.05 were considered statistically significant. Statistical analyses were performed using IBM SPSS Statistics for Windows, version 18.0 (IBM Corp., Armonk, NY, USA) and SAS version 9.3 (SAS Institute, Inc., Cary, NC, USA).
Results
Patients and tumor characteristics
The 1761 patients in this study (Fig. 1) included 1393 (79.1%) females and the median age of the study population was 46 years at diagnosis (Table 1). The median tumor size was 0.8 cm, and 1166 (66.2%) patients had papillary microcarcinomas, defined as tumors <1 cm in diameter. Multifocality was observed in 410 (23.3%) patients, microscopic ETE in 780 (44.3%), and pathological lymph node metastasis in the ipsilateral central neck in 618 (35.1%). According to the TNM staging system, 1639 (93.1%) patients were classified as stage I and 122 (6.9%) as stage II. Based on ATA risk stratification, 805 (45.7%) patients were classified as low risk, 949 (53.9%) as intermediate risk, and only seven (0.4%) as high risk.
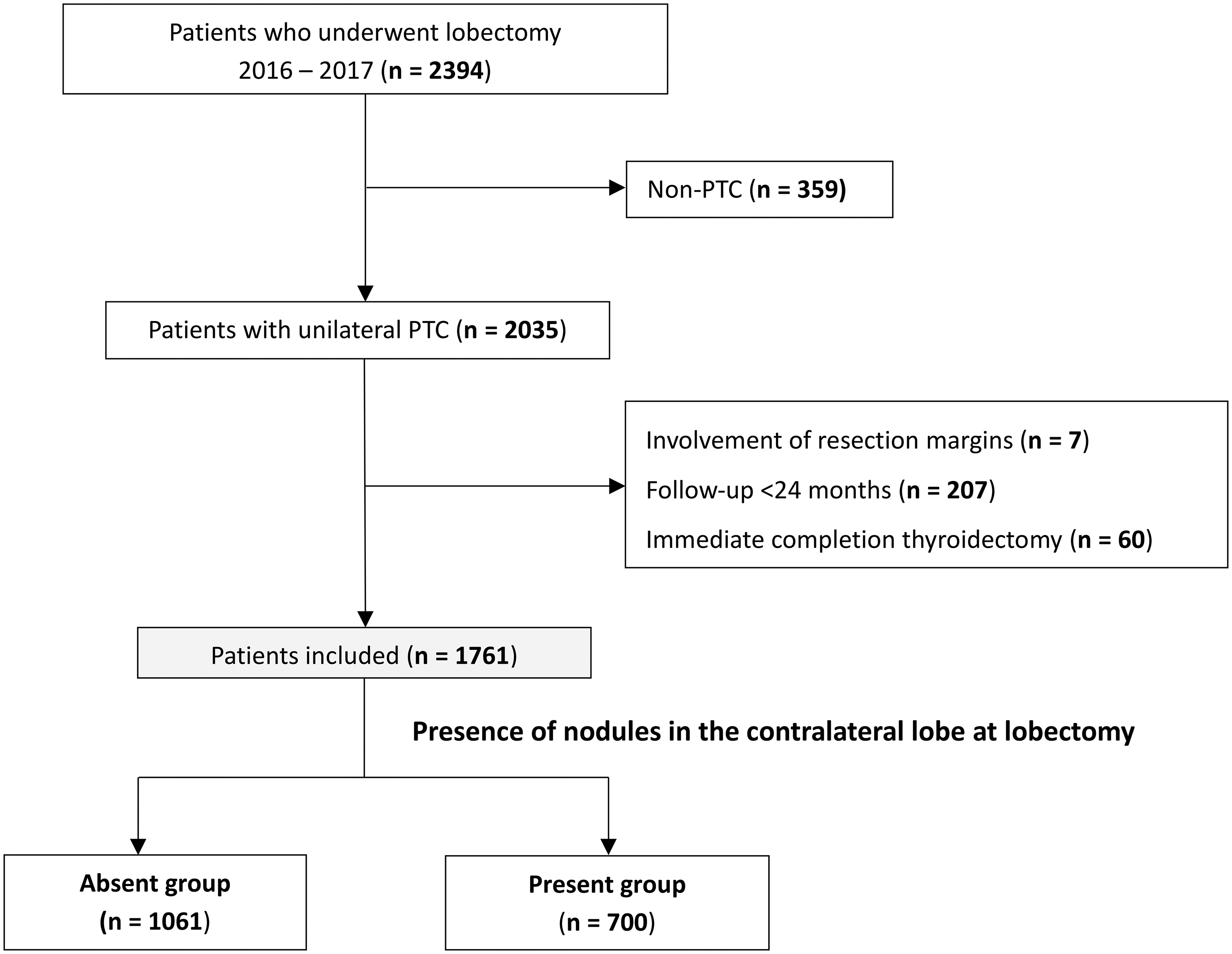
Flow chart of patient selection. PTC, papillary thyroid carcinoma.
Clinical Characteristics of Patients and Changes in Contralateral Nodules During Follow-Up
AJCC, American Joint Committee on Cancer; ATA, American Thyroid Association; ETE, extrathyroidal extension; PTC, papillary thyroid carcinoma; TNM, tumor-node-metastasis.
These 1761 patients included 700 (39.8%) in the Present group and 1061 (60.2%) in the Absent group. There were no between-group differences in sex distribution, primary tumor size, PTC variant, microscopic ETE, and ATA risk of recurrence. However, the Present group was older, exhibited greater multifocality, had a lower incidence of Hashimoto thyroiditis, and was more likely to be classified as AJCC TNM stage II than the Absent group (Table 1).
Contralateral nodules at the time of lobectomy
The median nodule size in the 700 (39.8%) patients who presented with contralateral nodules at the time of lobectomy was 0.5 cm (range, 0.1 to 4.5 cm). Of these 700 patients, 239 (34.1%), 175 (25.0%), and 245 (35.0%) had contralateral nodules classified as of intermediate, low, and benign suspicion, respectively, with 169 patients (24.1%) having multiple nodules in the contralateral lobe. Cytologic examination of the contralateral nodules in 88 patients (12.6%) before surgery found that 7, 71, and 10 patients could be classified as Bethesda categories I, II, and III, respectively.
Changes of contralateral nodules after lobectomy
Table 1 summarizes the changes in nodules detected in the contralateral lobe after lobectomy, including changes in their size, number, and characteristics. During a median follow-up period of 59 months, a total of 1879 nodules were detected, including 565 nodules in the 1061 patients without nodules at lobectomy (Absent group) and 1314 nodules in the 700 patients with nodules at lobectomy (Present group). The median growth of contralateral nodules in the Present group was 0.1 cm (range, −3.4 to 3.1 cm. Of the contralateral nodules in the Present group, 54.7% were unchanged, decreased in size, or disappeared during the follow-up period, whereas 14.8% increased ≥0.3 cm in size. Additionally, 401 new nodules were detected, with 24 (5.9%) being categorized as highly suspicious, similar to the rate observed in the Absent group. Of the 26 contralateral nodules at lobectomy reclassified as highly suspicious, 24 had been initially classified as of intermediate suspicion. Detailed information is provided in Supplementary Table S1.
During the follow-up period, 57 (3.2%) of the 1761 patients underwent cytological examinations; of these 57 patients, 31 presented with newly developed contralateral nodules. Nine patients underwent cytologic examinations due to an increase in the size of their contralateral nodules. Thirteen patients showed a change in their contralateral nodules to a state of high suspicion. Although four patients were found to have stable nodules, cytologic examinations were performed due to clinical suspicion or at the patient's request. Two patients whose nodules were clinically suspicious underwent FNA before their initial surgery for intermediate suspicion contralateral nodules. Preoperative cytologic examination of the nodules of these two patients showed that one had a benign nodule (Bethesda II), whereas the other had atypia of undetermined significance (Bethesda III) (Fig. 2).
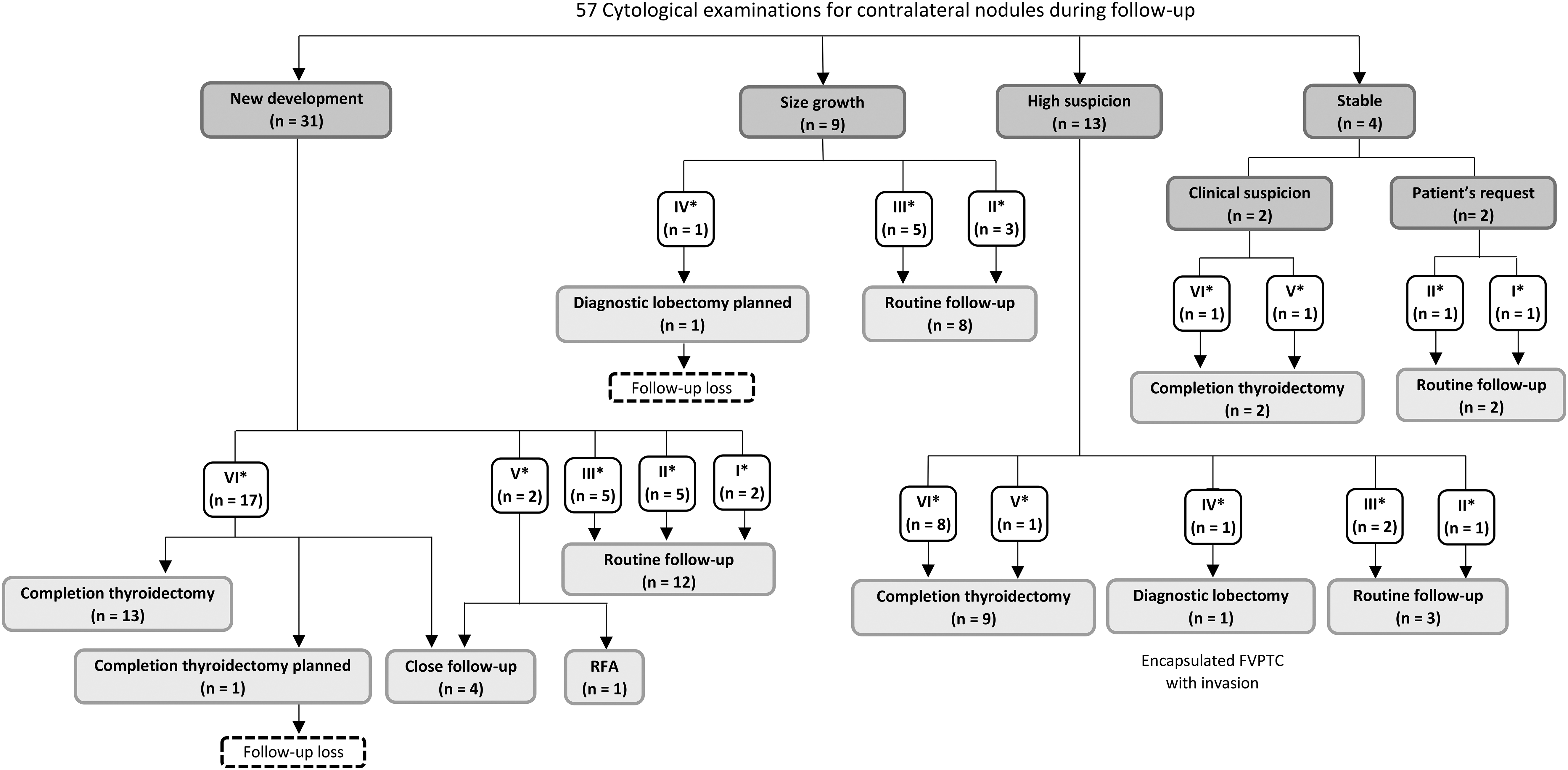
Results of cytologic examinations of contralateral nodules following lobectomy in 57 patients. *Results of cytologic examination based on the 2017 Bethesda system for reporting thyroid cytopathology. 25 FVPTC, follicular variant papillary thyroid carcinoma; RFA, radiofrequency ablation.
Outcomes of contralateral PTC and tumor recurrence
During the follow-up period, 31 patients (1.8%) were newly diagnosed with contralateral PTC. Contralateral PTC was significantly more common in the Present group than the Absent group (2.9% [20/700] vs. 1.0% [11/1061], p = 0.004) (Table 1). Of the 31 patients diagnosed with contralateral PTC, 24 underwent completion thyroidectomy, and one underwent radiofrequency ablation. Surgery was planned in two other patients, but both were lost to follow-up; and four patients preferred close follow-up without surgery (Fig. 2). Twenty-four patients (1.4%) experienced loco-regional recurrence, including cervical neck lymph node metastasis or operative site recurrence, whereas only one patient experienced distant metastasis (Table 1). There were no disease-related deaths.
The 5-year contralateral PTC DFS rates in the Present group and the Absent group were 98.2% and 99.3% (p = 0.003), respectively (Fig. 3A). The 5-year RFS rates did not differ significantly in these two groups (98.7% vs. 98.7%, p = 0.724; Fig. 3B), and the DSS rates were 100% in both groups. Neither the presence of contralateral nodules nor the presence of intermediately suspicious contralateral nodules at the time of lobectomy were identified as statistically significant risk factors for recurrence, as in univariate and multivariable analyses (Supplementary Table S2). Completion thyroidectomy was performed in 39 patients (2.2%), with two experiencing permanent hypoparathyroidism and none having recurrent laryngeal nerve injury.
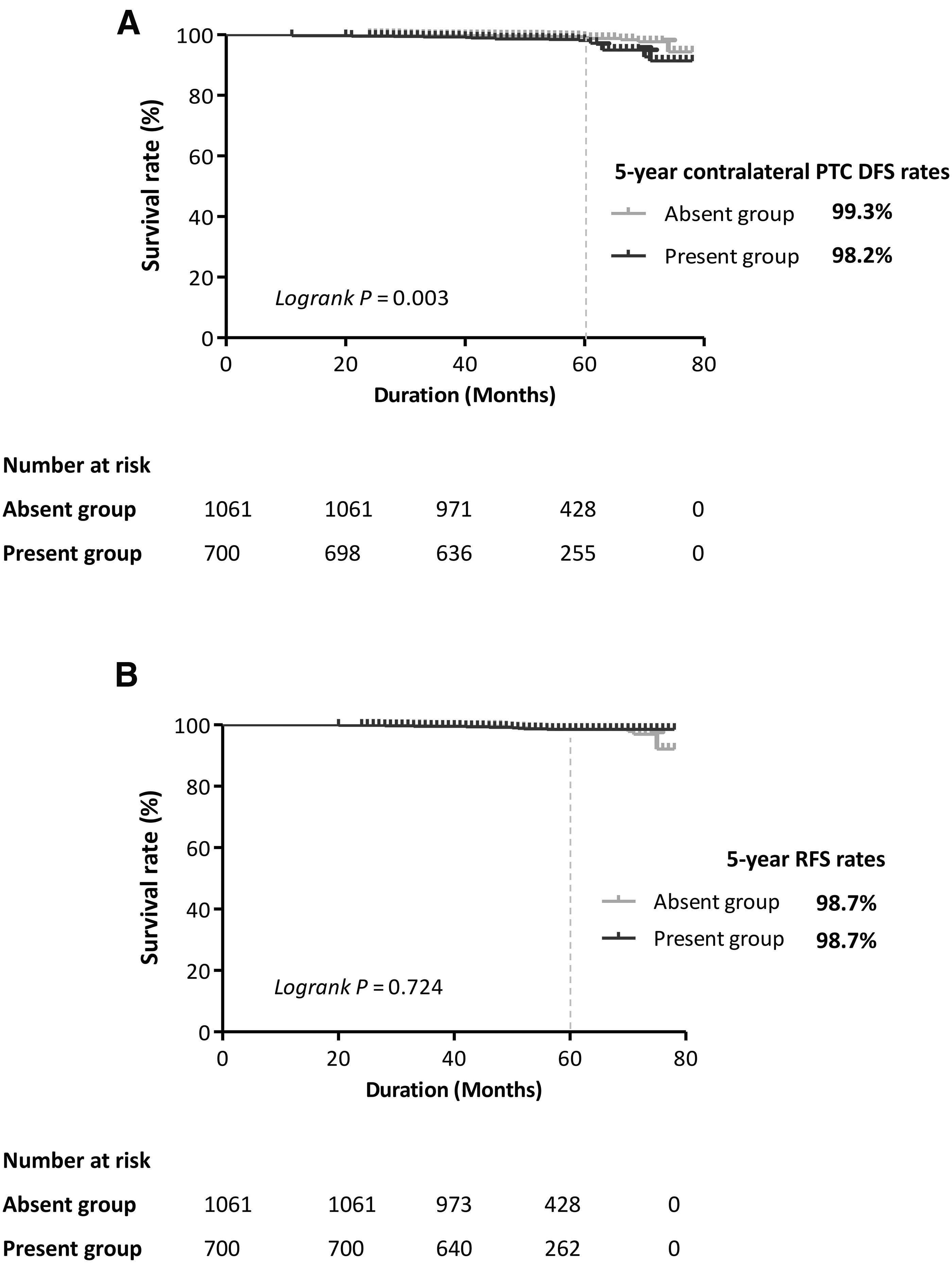
Kaplan–Meier analysis of the 5-year rates of (
Risk factors for contralateral PTC and progression of contralateral nodules
Univariate and multivariable regression analyses were performed to identify the factors associated with contralateral PTC in patients who underwent lobectomy (Table 2). Univariate analyses showed that multifocality, pathologic lymph node metastasis (pN1a), and ATA intermediate risk were significantly associated with contralateral PTC. Multivariable analysis showed that multifocality (HR 2.25, p = 0.026) and pN1a (HR 2.28, p = 0.032) were independently associated with contralateral PTC.
Univariate and Multivariable Regression Analyses of Risk Factors Associated with Contralateral Papillary Thyroid Carcinoma in All Patients
CI, confidence interval; HR, hazard ratio.
The presence of contralateral nodule(s) (HR 2.74, p = 0.008), particularly those nodules classified as intermediately suspicious (HR 6.03, p < 0.001), was significantly and independently associated with contralateral PTC (Table 2). Moreover, the presence of contralateral nodules ≥1 cm in size was significantly associated with nodule progression (HR 2.06, p < 0.001) (Table 3).
Univariate and Multivariable Regression Analyses of Risk Factors Associated with Progression of Contralateral Nodules in Patients with Contralateral Nodules at the Time of Lobectomy (Present Group)
OR, odds ratio.
Discussion
This retrospective cohort study investigated the long-term outcomes following lobectomy in a large cohort of patients with unilateral PTC and low-to-intermediate suspicious contralateral nodules. During the follow-up period, more than half of contralateral nodules present at the time of lobectomy were stable or disappeared, although a few became highly suspicious. The incidence of newly diagnosed contralateral PTCs was higher (2.9% vs. 1.0%), and the 5-year contralateral PTC DFS rate (98.2% vs. 99.3%) was lower in the Present group than the Absent group. However, the 5-year RFS and DSS rates did not differ significantly in these two groups. Reducing the extent of surgery in patients with low-risk unilateral PTC and low-to-intermediate suspicious contralateral nodules could therefore allow most patients to avoid unnecessary total thyroidectomy and its associated complications, as well as lifelong medication use.
Of the 1314 contralateral nodules observed at the time of lobectomy, 194 (14.8%) showed a ≥0.3 cm increase during follow-up. By contrast, approximately half of the contralateral nodules observed at lobectomy did not change, decreased in size, or disappeared. Of the 401 (30.5%) nodules that newly developed following lobectomy, 24 (5.9%) were highly suspicious (K-TIRADS 5). About 80% of the nodules that appeared after lobectomy were either benign or of low suspicion nodules (K-TIRADS 2 or 3). A study of the natural history of nonsuspicious contralateral nodules after lobectomy in patients with PTC showed that, after a median follow-up of 6 years, the median growth of contralateral nodules was zero, with 41% being stable and 26% decreasing in size. 10 A second study reported similar outcomes of nonsuspicious contralateral nodules after lobectomy in patients with PTC, finding that, after a median follow-up of 51 months, the median change in size of contralateral nodules was 0 mm, with 78.8% of patients having stable or decreased nodules, and 18.4% having no detectable nodules. 11
These findings, along with the results of this study, suggest that most nodules in the contralateral lobe after lobectomy in patients with PTC do not progress. However, this study found that contralateral nodule size ≥1 cm was significantly associated with nodule progression, with multivariable analysis yielding a HR of 2.06 ([CI 1.40–3.05]; p < 0.001). These results suggest the need for close surveillance or total thyroidectomy in patients with contralateral nodules ≥1 cm at the time of surgery, as this factor may be associated with an increased risk of progression.
We found that contralateral intermediately suspicious nodules were associated with an increased risk of contralateral PTC (HR = 6.03 [CI 2.80–13.02]; p < 0.001). The incidence of contralateral PTC was slightly higher in patients with (2.9%) than without (1.0%) contralateral nodules at the time of lobectomy, suggesting that the contralateral nodules at initial surgery may be undetected PTCs. However, neither the presence of contralateral nodules nor of contralateral intermediately suspicious nodules was a statistically significant risk factor for recurrence (Supplementary Table S2). This suggests that undetected PTCs, even in the presence of contralateral intermediately suspicious nodules, do not significantly affect the rates of loco-regional recurrence and distant metastasis. Small occult carcinomas are rarely associated with distant metastasis or death. 20 –22
Furthermore, only 2 (5.1%) of the 39 patients who underwent completion thyroidectomy experienced postoperative complications, with both having permanent hypocalcemia. Total thyroidectomy may result in postoperative complications, such as hypocalcemia, hematoma, vocal cord paralysis, and respiratory complications, making lifelong postoperative thyroid hormone replacement mandatory. 7,23 To avoid overtreatment and potential complications that negatively affect patient quality of life, total thyroidectomy may not be necessary to determine bilaterality, as the rate of diagnosis of contralateral PTC is low, and completion thyroidectomy did not increase the complication rate. Rather, close surveillance and salvage surgery may be a more appropriate approach.
This study had several limitations. First, it was a retrospective cohort study involving patients at a single tertiary center. Most of these patients had microscopic PTCs and low-risk disease, which may have led to selection bias and limited the generalizability of the study results. Second, the limited numbers of patients diagnosed with contralateral PTC and recurrence limited the ability to assess risk factors for these outcomes. Third, at the time of this study, molecular or genetic testing, such as BRAF and telomeratse reverse transriptase mutation analyses, was not performed routinely. Therefore, there may have been insufficient information to accurately classify the risk of recurrence according to ATA guidelines and to predict recurrence in these patients. Fourth, because the concept of noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) did not exist at the time of the initial pathologic classification, some patients now classified as having NIFTP may have been categorized as having encapsulated follicular variant without invasion. Fifth, because US was performed by several radiologists during the follow-up period, their interpretation of results may have differed, potentially affecting accuracy. Stratification of the risk of malignancy associated with thyroid nodules may depend on the level of expertise of the radiologists. 24 However, because all radiologists who evaluated the nodules were properly trained, interobserver variability was not likely to be significant. In addition, nodules that changed in size by <0.3 cm were excluded from the statistical analysis to minimize this potential limitation. Sixth, the study follow-up period (median 59 months) may have been insufficient to determine the lifelong risk of contralateral nodules. Further long-term follow-up studies are needed.
Nevertheless, this study highlights the natural course of contralateral nodules after lobectomy in a large patient cohort. These findings provide meaningful insights into the potential progression and management of contralateral nodules after lobectomy.
In conclusion, lobectomy may be a safe and reliable initial treatment option for low-risk unilateral PTC with contralateral low-to-intermediate suspicious nodules. Close surveillance and salvage surgery may be effective in patients with contralateral intermediate suspicion nodules.
Footnotes
Acknowledgments
The authors thank Seonok Kim, MSc, for statistical analyses and Bioedit Ltd for English language editing. The authors are profoundly grateful to Dong Eun Song, MD, PhD, for her invaluable contributions to the pathologic diagnosis of the patients involved in this study.
Authors' Contributions
S.J.P.: Writing—original draft (lead), formal analysis (lead). D.K., B.-C.K., J.W.C., W.W.K., Y.-m.L., and T.-Y.S.: Conceptualization (supporting), writing—review and editing (equal). J.H.B., W.G.K., and W.B.K.: Conceptualization (supporting), methodology (supporting), writing—review and editing (equal). K.-W.C.: Conceptualization (lead), methodology (lead), writing—original draft (supporting), wiring—review and editing (equal). All the authors had full access to the data, take responsibility for the accuracy of the data analysis, and approved the final version of the manuscript.
Author Disclosure Statement
None of the authors has anything to disclose.
Funding Information
None of the authors has any funding information to declare.
Supplementary Material
Supplementary Table S1
Supplementary Table S2