
Abstract
Background:
Graves' disease has been associated with adverse pregnancy, labor and delivery, and neonatal outcomes. Thyroid function levels, assessed during newborn screening (NBS), can serve as indicators of the adaptation in the hypothalamic–pituitary–thyroid axis. We utilized data from the national thyroid NBS program to investigate the characteristics of the mother–infant dyad of term infants born to mothers with past or active Graves' disease.
Methods:
The dataset of the Israeli NBS for thyroid function was linked with the electronic records of a tertiary medical center to generate a unified database of mothers and their term infants born between 2011 and 2021. The MDClone big data platform extracted maternal, pregnancy, disease course, labor and delivery, and neonatal characteristics of the mother-infant dyads.
Results:
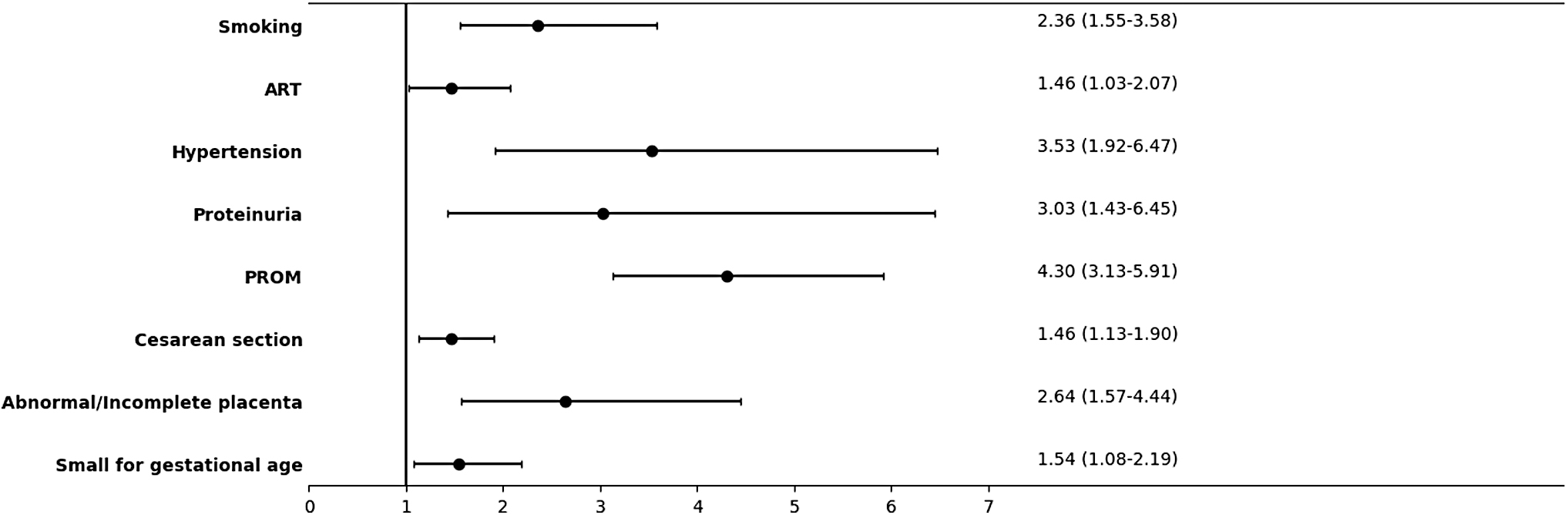
Out of 103,899 registered mother–infant dyads, 292 (0.3%) mothers had past or active Graves' disease. A forward multivariate linear regression demonstrated that Graves' disease did not significantly affect NBS total thyroxine (tT4) levels (p = 0.252). NBS tT4 levels in infants born to mothers with active Graves' disease were higher than those observed in the general Israeli population (p < 0.001). Mothers with Graves' disease more frequently used assisted reproductive technology (12.7% vs. 9.0%, respectively, p = 0.012; odds ratio [OR] = 1.46 [CI 1.03–2.07], p = 0.031), and had more gestational hypertension (3.9% vs. 1.1%, p < 0.001; OR = 3.53 [CI 1.92–6.47], p < 0.001), proteinuria (2.5% vs. 0.9%, p < 0.001; OR = 3.03 [CI 1.43–6.45], p = 0.004), cesarean sections (26.4% vs. 19.7%, p = 0.029; OR = 1.46 [CI 1.13–1.90], p = 0.004), prelabor rupture of membranes (15.4% vs. 4.1%, p < 0.001; OR = 4.3 [CI 3.13–5.91], p < 0.001), and placental abnormalities (5.1% vs. 2.0%, p < 0.001; OR = 2.64 [CI 1.57–4.44]; p < 0.001). Their infants had lower adjusted birthweight z-scores (−0.18 ± 0.94 vs. −0.03 ± 0.90, p = 0.007) and were more likely to be small for gestational age (12.0% vs. 8.1%, p = 0.005; OR = 1.54 [CI 1.08–2.19], p = 0.018).
Conclusions:
Neonatal thyroid function levels were affected by maternal Graves' disease only when the disease was active during gestation. Moreover, maternal Graves' disease was also associated with an increased risk of adverse outcomes for the mother–infant dyad.
Introduction
Hyperthyroidism due to Graves' disease is estimated to occur in 0.2% of all pregnancies, and inadequate management of hyperthyroidism has been associated with an increased risk of adverse outcomes, such as preterm delivery, low birthweight, miscarriage, and stillbirth. 1 –3 Neonatal hyperthyroidism in the offspring of mothers with active or a past history of Graves' disease, may be associated with higher rates of fetal or neonatal morbidity, particularly if left untreated. 4,5 Elevated levels of thyroid hormones in the mother has been suggested as a potential risk factor for neurocognitive problems in the offspring, such as seizure disorders, behavioral difficulties, and lower intelligence quotient. 6,7
Newborn screening (NBS) programs comprise an essential element of public health, with the primary aim of improving health outcomes and reducing neonatal morbidity and mortality. 8,9 Congenital hypothyroidism (CH), is typically detected through routine NBS programs, and treatment is promptly initiated based upon confirmatory measurements of serum thyrotropin (TSH) and free thyroxine (fT4) levels. 10,11 Banigé et al. recently conducted a proof-of-concept study for population-based neonatal hyperthyroidism screening utilizing TSH levels, 12 but it has not yet been implemented into common practice.
The intrauterine environment has significant impact upon the offspring, and fetal characteristics may also influence maternal health throughout pregnancy and delivery. 13,14 As such, the bidirectional nature of health characteristics calls for an integrated approach that views the mother–infant relationship as a dyad rather than two independent entities. In this study, we utilized data from the thyroid NBS program to investigate the characteristics of the mother–infant dyad of term infants born to mothers with Graves' disease without the confounding effect of prematurity. We hypothesized that total thyroxine (tT4) levels as detected by NBS in infants born to mothers with Graves' disease will be higher than those of infants of mothers in the general population.
Materials and Methods
Study outcomes
The primary outcome was NBS thyroid function levels in term infants born to mothers with Graves' disease in comparison to mothers in the general population. We also explored secondary outcomes in two dimensions: maternal characteristics (assisted reproduction, pregnancy weight gain, comorbid conditions, prelabor rupture of membranes [PROM], anesthesia, and cesarean section) and neonatal characteristics (sex, adjusted birthweight, APGAR score [appearance {skin color}, pulse, grimace {reflex}, activity {muscle tone}, and respiration], and hospitalization in a neonatal intensive care unit) in mother–infant dyads with Graves' disease compared with the general population.
Sample size calculation
The sample size calculation was based on the expected mean (standard deviation [SD]) change of 0.75 μg/dL in NBS tT4 levels, the primary outcome of this study, using WinPepi software version 11.65. 15 The required sample size of 192 cases of Graves' disease and 63,803 cases from the general population was calculated to achieve a significance level (α) of 5% and a power of 80%. The calculation considered the proportion of Graves' disease cases (0.3%) among all study cases.
Study design and population
The Israeli NBS program's thyroid dataset was queried to identify all neonates born at the Tel Aviv Sourasky Medical Center (TASMC) between 2011 and 2021. The MDClone platform was utilized to access the medical records of mothers and their infants and to link pertinent data with the thyroid dataset to generate a unified mother–infant dyad database. Included were liveborn infants with available NBS thyroid test results. Excluded from the analysis were infants with conditions that could significantly impact the hypothalamic-pituitary-thyroid axis function, such as being preterm (gestational age [GA] <37 weeks), having been diagnosed with chromosomal abnormalities, and maternal thyroid disorders other than Graves' disease.
Dyads were categorized into two groups: the maternal Graves' disease (study cohort) and the general population (control group). The MDClone system searched the mother's records for the terms “Graves' disease,” “thyroid eye disease,” “thyroid ophthalmopathy,” “goiter,” “hyperthyroidism,” “thyrotoxicosis,” “toxic thyroid nodule,” “propylthiouracil,” “mercaptizol,” and “methimazole.” A broad search term approach was implemented to ensure the inclusion of all potential cases of Graves' disease.
The study group was then manually validated to ensure that only dyads in which the mothers who had Graves' disease were included. The control group underwent data preprocessing steps, including data wrangling, filtering, and subsetting, as well as correction of obvious inconsistencies. The Graves' disease mother–infant dyads were stratified into two categories based upon whether the disease was active or inactive during gestation. Active Graves' disease during pregnancy was defined by the fulfillment of at least one of the following conditions: the use of antithyroid drugs (ATDs) during pregnancy, elevated thyroid function tests in a trimester-specific approach, 16,17 elevated TSH receptor antibody (TRAb) levels during pregnancy, or the clinical judgment of the practicing physician. Any value above the normal range of the specific assay as documented in the medical files was considered elevated.
The NBS program search yielded 124,238 tT4 results of infants born at the TASMC Lis Maternity Hospital. The MDClone platform (MDClone© Ltd, Beer Sheva, Israel) was utilized to link these results to the medical records of the mother–infant dyads. Five-hundred fourteen dyads were initially identified as having a history of maternal hyperthyroidism, while 195 mothers and 27 infants did not fulfill inclusion criteria, leaving a final study cohort of 292 mother–infant dyads. Out of the 123,724 mother–infant control population dyads, 103,607 mother–infant dyads fulfilled inclusion criteria and comprised the final control group (Fig. 1).
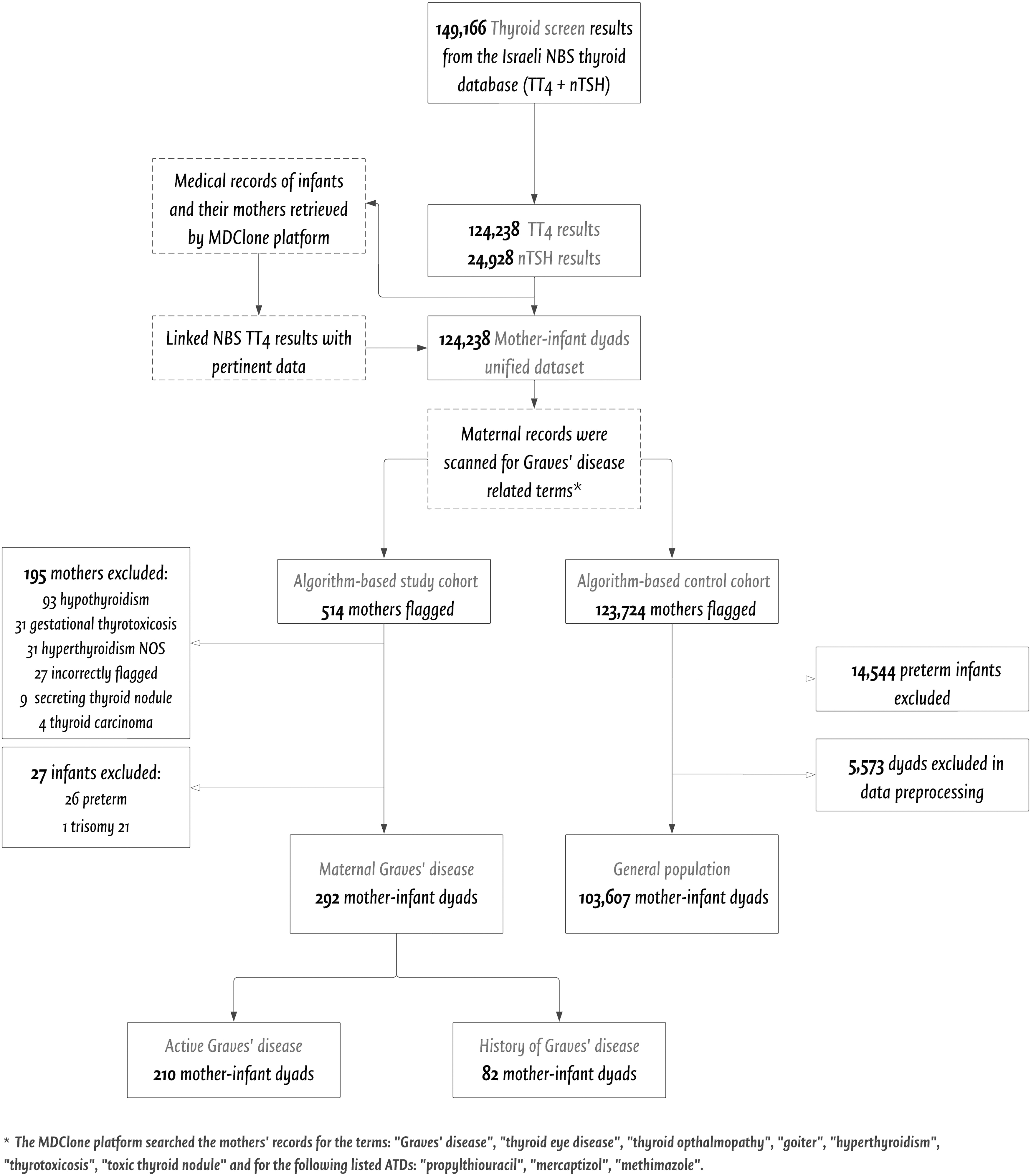
Flow diagram showing study design and patient selection. The MDClone system searched the mother's records for the terms “Graves' disease,” “thyroid eye disease,” “thyroid ophthalmopathy,” “goiter,” “hyperthyroidism,” “thyrotoxicosis,” “toxic thyroid nodule,” and for the following listed ATDs: “propylthiouracil,” “mercaptizol,” “methimazole.” ATDs, antithyroid drugs; NBS, newborn screening; NOS, not otherwise specified; tT4, total thyroxine; TSH, thyrotropin.
The Israeli NBS program is a national effort with all samples being handled and analyzed at a single laboratory. The program's strategy for early detection of CH in term infants utilizes an initial single screen of tT4 at 36–72 hours of age, with a follow-up TSH assay if the tT4 value falls below the 10th percentile of the reference. 18
Data acquisition
Data on mother–infant dyads were gathered from conception and throughout the pregnancy and perinatal periods. Body mass index (BMI) was calculated as weight (in kilograms) divided by height (in meters squared). 19 Gestational diabetes mellitus (GDM) was defined according to the Carpenter and Coustan diagnostic thresholds. 20 Cases in which part of the placenta persisted and required gynecological intervention were labeled “incomplete placenta,” while “abnormal placenta” referred to cases of an abnormal size, color, shape, and/or general appearance of the placenta. Birthweight and head circumference z-scores were calculated based upon the World Health Organization growth chart for term infants. 21,22 Appropriate birthweight (AGA) was defined as birthweight z-scores of −1.28 to 1.28, small (SGA) as birthweight z-scores of −1.28 or lower, and large (LGA) as birthweight z-scores of 1.28 or higher. 21
Ethics
Our Institutional Review Board approved the study protocol (approval number TLV-0030-22) and waived the need for informed consent. The research has been conducted in accordance with the Declaration of Helsinki, the guidelines of good clinical practice, and the Strengthening the Reporting of Observational studies in Epidemiology guidelines.
Statistical analysis
Data were analyzed with the Statistical Package for the Social Sciences software version 28 (IBM Corp., Armonk, NY, USA). Violin plots were created using R-studio 4.2 (R Project for Statistical Computing). The Kolmogorov–Smirnov test was applied to assess the normality of continuous data. Continuous data are reported as either mean ± SD for normally distributed data, or median and interquartile range (IQR) for skewed data. Categorical variables are reported as number and percentage. Differences in continuous data between groups were studied using independent-sample t-tests for normally distributed data or by Mann–Whitney U-tests for skewed data. Chi-square tests were performed to compare the distribution of categorical variables.
Contingency tables were performed to explore associations between maternal Graves' disease dyads and selected outcomes through the estimation of odds ratios (ORs) and 95% confidence intervals (CIs). A post hoc subanalysis, excluding twin pregnancies, was also performed. A forward multivariable linear regression model was used (entry stepping method criteria p < 0.05) to investigate the influence of various factors (maternal, labor- and delivery-related, and infant characteristics) on NBS tT4 levels.
A multivariable logistic regression model was performed to evaluate the abovementioned contributory factors for NBS tT4 levels in the ≥90th percentile (19.9 μg/dL). We addressed the effect of active maternal Graves' disease on NBS tT4 levels by performing an identical post hoc model in which the variable “active maternal Graves' disease” replaced “maternal Graves' disease” (past and active). All linear regression models fulfilled the following conditions: linear relationship between the dependent variable and all the numerical independent variables, normality of the regression residuals, little or no multicollinearity between the independent variables, no autocorrelation, and homoscedasticity of the regression residuals. A p-value of ≤0.05 was considered significant, and Bonferroni corrections were used for multiple comparisons.
Results
Mother and pregnancy
Out of 103,899 mother–infant dyads, 292 (0.3%) had a diagnosis of maternal Graves' disease. The maternal and pregnancy characteristics of the mother–infant dyads of the Graves' disease group compared with the general population are presented in Table 1 and Figure 2. Mothers with Graves' disease were older (mean age 34.6 ± 4.8 years vs. 32.6 ± 4.8 years, respectively, p < 0.001), and fewer of them were nulliparous (34.2% vs. 42.0%, p = 0.007) as compared with mothers in the general population. Anthropometric parameters of height, pregestational BMI, and gestational weight gain were similar between groups. Methods of conception differed significantly, with more mothers in the Graves' group having undergone assisted reproduction (12.7% vs. 9.0%, p = 0.012; OR = 1.46 [CI 1.03–2.07], p = 0.031) and higher rates of twin pregnancies (5.5 vs. 2.1%, p < 0.001). The prevalence of smoking in mothers with Graves' disease was also significantly higher (8.2% vs. 3.7%, p < 0.001; OR = 2.36 [CI 1.55–3.58], p < 0.001).
Selected outcomes of mother
Maternal and Pregnancy Characteristics of Mother–Infant Dyads in Mothers with Graves' Disease Compared with the General Israeli Population, 2011–2021
The data are expressed as mean ± SD, median [IQR], and number and (%). Rates of conditions affecting gestation are based upon the number of cases with valid documentation for the control and study groups, respectively; hypertension = 77,882 (75.2%) and 281 (96.2%); and proteinuria = 73,363 (70.8%) and 275 (94.1%). Bold indicates statistical significance at the p ≤ 0.05 level. All variables retained their significance after Bonferroni correction (p < 0.013 for obstetric history and p < 0.010 for conditions affecting gestation).
BMI, body mass index; IQR, interquartile range; IVF, in-vitro fertilization; SD, standard deviation.
Pregnancies of mothers with Graves' disease were complicated by comparatively increased rates of hypertension (3.9% vs. 1.1%, p < 0.001; OR = 3.53 [CI 1.92–6.47], p < 0.001) and proteinuria (2.5% vs. 0.9%, p < 0.001; OR = 3.03 [CI 1.43–6.45], p = 0.004). There were no significant differences in the rate of GDM between the groups: a post hoc subanalysis that excluded twin pregnancies revealed that the rates of GDM were higher in mothers with Graves' disease compared with the general population (7.2% vs. 4.6%, p = 0.04; OR = 1.63 [CI 1.01–2.57], p = 0.036).
Labor and delivery
The labor- and delivery-related characteristics of the mother–infant dyads with maternal Graves' disease in comparison to the general population are shown in Table 2 and Figure 2. The administration of medications during labor and the type of anesthesia were similar between the two groups. However, there was a significant group difference in the mode of delivery, with higher rates of cesarean section observed in women with Graves' disease (26.4% vs. 19.7%, p = 0.029; OR = 1.46 [CI 1.13–1.90], p = 0.004). Notably, a post hoc subanalysis that excluded twin gestations revealed no significant differences in the rates of cesarean section between the groups. Furthermore, increased rates of PROM (15.4% vs. 4.1%, p < 0.001; OR = 4.3 [CI 3.13–5.91], p < 0.001) and abnormal or incomplete gross placental appearance (5.1% vs. 2%, p < 0.001; OR = 2.64 [CI 1.57–4.44]; p < 0.001) were observed in mothers with Graves' disease compared with the general population.
Labor and Delivery Characteristics of Mother–Infant Dyads in Mothers with Graves' Disease Compared with the General Israeli Population, 2011–2021
The data are expressed as mean ± SD and number and (%). Bold indicates statistical significance at a p ≤ 0.05 level. PROM remained significant after Bonferroni correction (p < 0.025).
The variable “antibiotics” includes usage of prophylactic antibiotics.
PROM, prelabor rupture of membranes.
Newborns
Infant characteristics stratified according to maternal Graves' disease are presented in Table 3 and Figure 2. The infants in the Graves' disease group had significantly lower birthweights, with lower birthweight z-scores (−0.18 ± 0.94 vs. −0.03 ± 0.90, p = 0.007), and a higher proportion of infants categorized as SGA (12% vs. 8.1%, p = 0.005; OR = 1.54 [CI 1.08–2.19], p = 0.018), compared with the control group. A graphic visualization of birthweight z-scores showed that the two groups had a dissimilar center, spread, and distribution (Fig. 3A). There were no significant group differences in presentation at delivery, APGAR scores, and newborn hospitalization parameters (department and duration of stay). The median tT4 and TSH levels did not differ between the groups, with similar proportions of newborns requiring TSH testing due to relatively low tT4 levels (9.1%). A post hoc subanalysis, which excluded twin pregnancies showed no significant difference in tT4 levels among newborns in either group. The graphic visualization of the NBS tT4 level distribution revealed similarity between the two groups (Fig. 3B).
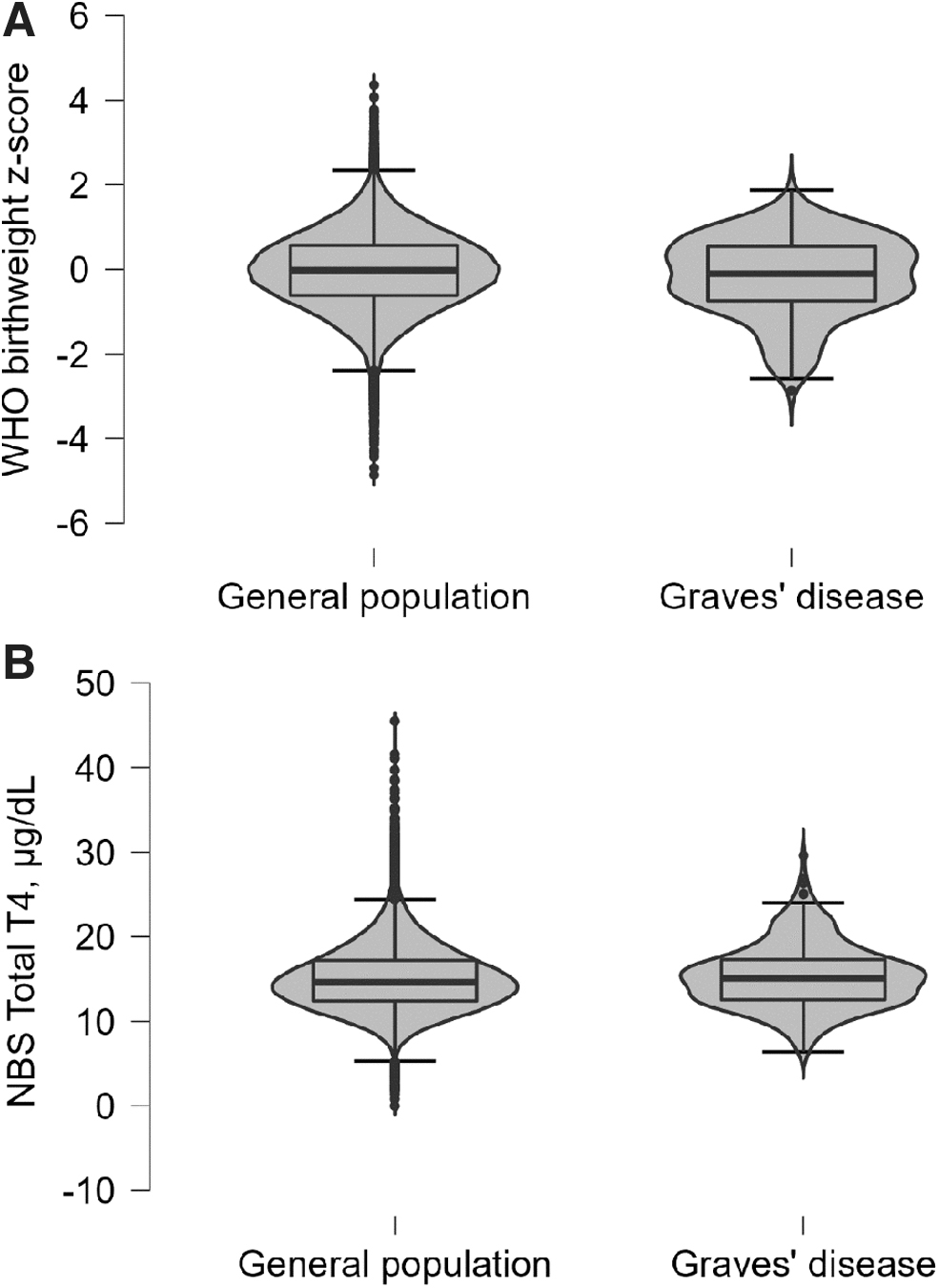
Birthweight z-scores and NBS tT4 levels of newborns to mothers with Graves' disease compared with the general population. Violin plots (distributions of numeric data using probability density curves) illustrating the distribution of: (
Newborn Characteristics of Mother–Infant Dyads in Mothers with Graves' Disease Compared with the General Israeli Population, 2011–2021
The data are expressed as number and (percent), mean ± standard deviation, median [IQR]. Bold indicates statistical significance at a p ≤ 0.05 level. Gestational age is presented in standardized decimal form. All variables retained their significance after Bonferroni correction (p < 0.013 for newborn characteristics).
APGAR, appearance (skin color), pulse, grimace (reflex), activity (muscle tone), and respiration; NICU, neonatal intensive care unit; tT4, total thyroxine; TSH, thyrotropin; WHO, World Health Organization.
Disease course
According to the American Thyroid Association guidelines, managing maternal Graves' disease requires close monitoring of maternal hyperthyroidism and adjusting the dose of ATDs to maintain normal thyroid function. Figure 4 illustrates the variability of TSH, fT4, and free triiodothyronine values by trimester, displaying their center, spread, and distribution. While the median thyroid function test levels were all within the normal range for each trimester, the distribution of values in the first trimester was wide. Table 4 presents an overview of the medical treatments administered to pregnant women diagnosed with Graves' disease in our cohort. The data showed that 10.3% of the women had previously undergone definitive thyroid treatment, with 6.5% having received radioiodine ablation and 3.8% having undergone thyroidectomy. More than one-half (52.4%) of those women were treated with medication aimed at regulating thyroid function, such as propylthiouracil, methimazole, or levothyroxine. Additionally, around one-fifth of the women received other prescribed medications, most commonly cardiovascular medication.
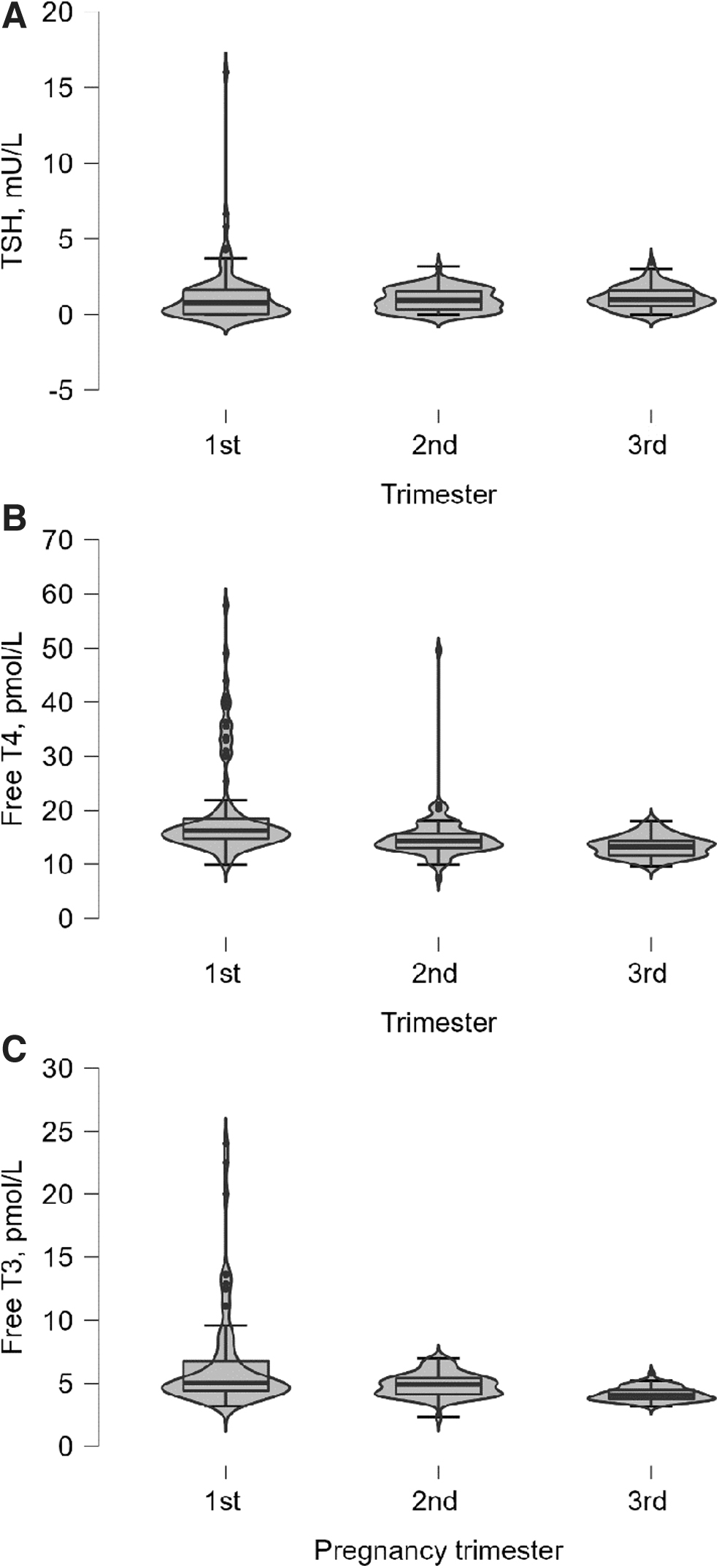
Trimester-specific thyroid function tests for pregnant women with Graves' disease. Violin plots (distributions of numeric data using probability density curves) illustrating the distribution of trimester-specific thyroid function tests. (
Medical Treatments in Pregnant Women with Graves' Disease
Thyroid treatment refers to the administration of any thyroid medication during pregnancy, regardless of trimester or dosage.
Active Graves' disease and regression models
We compared newborns from dyads with active maternal Graves' disease to those with a history of the disease. That subgroup analysis revealed that the former had significantly lower birthweight z-scores (−0.19 [IQR −0.82, 0.47] vs. 0.13 [IQR −0.58, 0.61], p = 0.05). In addition, newborns from dyads with active Graves' disease had higher NBS tT4 levels (μg/dL) compared with those with a history of the disease (15.6 [IQR 13, 18.1] vs. 13.4 [IQR 11.8, 16.1], p < 0.001) (Fig. 5; Supplementary Table S1).

Birthweight z-scores and NBS tT4 levels of newborns to mothers with active Graves' disease compared with those with a history of Graves' disease. Violin plots (distributions of numeric data using probability density curves) illustrating the distribution of: (
Forward multivariable linear regression models were applied to evaluate contributing factors for NBS tT4 levels. The final model for higher NBS tT4 levels (p < 0.001; Table 5) included younger maternal age (p < 0.001), lower pregestational BMI (p = 0.017), administration of any type of anesthesia (p < 0.001), administration of oxytocin (p < 0.001), newborn female sex (p < 0.001), older GA (p < 0.001), and higher birthweight z-scores (p < 0.001). Past and active maternal Graves' disease, gestational weight gain, and cesarean delivery did not show any significant association with NBS tT4 levels. Of note, the multivariable logistic regression model (Table 6) that was performed to evaluate the contributory factors for NBS tT4 levels in the ≥90th percentile (19.9 μg/dL) revealed essentially the same contributory factors for the primary outcome with the exception of maternal pregestational BMI.
Forward Multivariable Linear Regression Model Assessing Contributory Factors for Newborn Screen Total Thyroxine Levels
Multivariable linear regression models were applied to evaluate explanatory variables for NBS tT4 levels (μg/dL). The following independent variables were included in the model: maternal Graves' disease, maternal age at delivery, pregestational body mass index, gestational weight gain, gestational age, administration of any type of anesthesia, administration of oxytocin, cesarean section (elective or urgent), newborn male sex, and birthweight z-scores. A p-value of ≤0.05 was considered significant. Bold indicates significant.
CI, confidence interval analyzed at a level of 95%; NBS, newborn screening; SE, standard error.
Forward Multivariable Logistic Regression Model Assessing Contributory Factors for Newborn Screen Total Thyroxine Levels in the ≥90th Percentile
Multivariable logistic regression models were applied to evaluate explanatory variables on NBS tT4 levels (μg/dL) in the 90th percentile. The following independent variables were included in the model: maternal Graves' disease, maternal age at delivery, pregestational body mass index, gestational weight gain, gestational age, administration of any type of anesthesia, administration of oxytocin, cesarean section (elective or urgent), newborn male sex, and birthweight z-scores. A p-value of ≤0.05 was considered significant. Bold indicates significant.
OR, odds ratio.
A hypothesis-generating model was performed post hoc to isolate the effect of active maternal Graves' disease on NBS tT4 levels. The final model for higher NBS tT4 levels (p < 0.001; Supplementary Table S2) included active maternal Graves' disease (p = 0.001) in addition to the other abovementioned contributory factors.
Discussion
This large-scale cohort study explored characteristics of the mother–infant dyads of mothers with past or currently active gestational Graves' disease. We especially focused upon the effect of the mother's disease history on the newborn's thyroid function as measured by a NBS program. We found that neonatal thyroid function levels were affected by maternal Graves' disease only when the disease was considered active. The mothers with Graves' disease were older, fewer were nulliparous, and more of them conceived through in-vitro fertilization (IVF) compared with the general population. They had higher rates of gestational morbidity and instrumental delivery, and gave birth to smaller infants.
Israel has the highest utilization rates of assisted reproductive technology (ART) in the world, 23 with 9% of term infants having been born after ART compared with the reported 2–6% of births in European countries. 24 Noteworthy, the percentage increased 1.5 times among our study women with past or active Graves' disease. Hyperthyroidism has been linked to various fertility problems, including oligomenorrhea, and amenorrhea in women with uncontrolled severe hyperthyroidism. 25 More mothers with Graves' disease in our study used ART, which suggests a possible association between the disease and infertility. Twin pregnancies were more common in mothers with Graves' disease, possibly due to the higher rates of ART utilization in this population. Importantly, Israel's high ART rates may limit the generalizability of our findings.
Interestingly, mothers with past or active Graves' disease had a significantly higher proportion (∼2.2 times) of gestational smoking compared with the general population. A recent study has suggested a gene–environment interaction between smoking and genetic factors associated with Graves' disease. 26 Previous studies have also reported a dose-dependent relationship between Graves' disease and smoking intensity. 26,27 The influences of past and present smoking and family history of Graves' disease were beyond the scope of this study.
Several studies conducted in Scandinavia and the United States found various obstetric complications among hyperthyroid mothers. 28 –31 Our analysis indicates that pregnant women with past or active Graves' disease are at an increased risk of hypertension and proteinuria (3.5 and 3.0, respectively) compared with the general population. Previous studies have also reported an increased risk of gestational hypertensive disorders among mothers with Graves' disease, 2,31 but a lesser one compared with ours. We also found lower rates of gestational hypertensive disorders in the Israeli general population compared with other countries. 30,31 An earlier study hypothesized that thyroid hormones may enhance various processes, such as gluconeogenesis, glycogenolysis, and insulin degradation. 32 Another study has suggested a negative correlation between TSH levels and hemoglobin A1c levels in pregnant women. 33 While our primary analysis did not confirm this latter relationship, a post hoc analysis, excluding twin pregnancies indicated an increased risk of gestational diabetes in mothers with Graves' disease during pregnancy (OR = 1.6).
Cesarean section rates have increased to 18.6% of all births globally, with Israel having the lowest rate among the Organization for Economic Cooperation and Development countries. 34 In our study, mothers with past or active Graves' disease were at a higher risk of cesarean section (OR = 1.46) compared with the general Israeli population occurring in 26.4% of term deliveries. This finding is consistent with previous research from other countries. 30,31 However, a recent study reported that the risk of cesarean section in mothers with Graves' disease who were not administered ATDs was similar to that of euthyroid mothers. 35 This suggests that there may be a link between serum thyroid levels and delivery outcomes. 2 Previous publications have also demonstrated higher rates of PROM and placental abnormalities among mothers with gestational hyperthyroidism, 30,31 and our analysis revealed a similar trend (4.30 and 2.64, respectively). Hyperthyroidism was shown to modulate immunological and morphological placental aspects and induce fetal phenotypic changes in an animal model. 36
Gestational age at delivery and birthweight are significant indicators of neonatal morbidity and mortality. Some complications associated with maternal thyroid disease have been proposed to be due to preterm birth. 29 Our study focused solely upon mother–infant dyads of liveborn term infants, thus, the findings cannot be attributed to the confounding effects of prematurity. Prior research consistently demonstrates an association between maternal hyperthyroidism and an increased likelihood of SGA infants. 2,29 –31,37 Our study corroborates this finding (OR = 1.54), but the underlying mechanisms that contribute to this association remain unclear.
One theory suggests that hyperthyroidism-induced metabolic changes in the mother may affect the placenta and fetal growth. 3,29 Additionally, in mothers with Graves' disease, TRAbs that cross the placenta may induce fetal hyperthyroidism. 4,37 –39 Previous studies have emphasized the significance of gestational levels of TRAbs in predicting clinical outcomes in the newborn. 37,39 It is crucial to measure TRAbs during midgestation in women with active Graves' disease, but this analysis is often neglected. Moreover, it is essential to monitor TRAb levels in women with a history of prior surgical or radioactive iodine-131 treatment for Graves' disease since they may still have circulating TRAbs, even if they are euthyroid during pregnancy. 3,39 We acknowledge that the lack of Graves’-related data on the levels of TRAbs during pregnancy as well as dosage and adherence of ATDs present limitations to this analysis. Maternal smoking is a known risk factor for low birthweight 29 and also constitutes a potential risk factor for thyroid dysfunction. 26,27 Thus, a higher smoking rate among the Graves' disease group may be one plausible explanation for their increased risk of SGA.
Although TSH-based NBS for neonatal hyperthyroidism may be within reach, 12 population-based screening that uses TSH or tT4 for neonatal hyperthyroidism is currently not recommended. 8,9,40,41 Our findings of increased tT4 levels in newborns of mothers with active Graves' disease suggest that NBS could have the potential to identify both neonatal hypothyroidism and hyperthyroidism. Notably, however, our study design does not enable us to draw definitive conclusions or provide recommendations regarding tT4 levels and thresholds in newborns born to mothers with Graves' disease.
Our study is not without limitations. First, the data we used relied upon self-reported information, including obstetric history, health conditions affecting pregnancy, consumption of ATDs, and pregestational weight. Second, the observational design of the study prevented us from establishing a causal relationship between Graves' disease and the distinct characteristics observed in mother–infant dyads. The general applicability of the study's findings may be limited to countries that employ tT4 as the marker for assessing NBS thyroid function and, as such, might underdiagnose cases with isolated hyperthyrotropinemia. The primary strengths of this study include the uniform obstetric protocol of a single medical center and the rigorous validation process, which involved manually reviewing all hospital medical records of pregnant women with Graves' disease.
In conclusion, this observational study offers valuable insights into the impact of Graves' disease on the mother–infant dyad across multiple dimensions. Our findings suggest that term newborns of mothers with active gestational Graves' disease exhibit higher NBS tT4 levels. Moreover, Graves' disease was associated with an increased risk of adverse outcomes for the mother–infant dyad. Our study primarily focuses upon short-term outcomes, and we recommend future prospective longitudinal studies to assess the long-term effects of maternal Graves' disease on offspring in later years.
Footnotes
Acknowledgments
The authors thank Esther Eshkol for editorial assistance. This work was performed by ECS in partial fulfillment of the MD thesis requirements of the Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel. Parts of this work were presented in abstract form at ESPE 2023 (97 P1-588).
Authors' Contributions
E.C.-S. made a substantial contribution to the curation of data, data analysis, interpretation of data, and drafting of the article. A.B. made a substantial contribution to the conception and design of the study, interpretation of data analysis, and revised the article for important intellectual content. O.R. made a substantial contribution to the curation of data, interpretation of data, and revised the article for important intellectual content. M.Y.-G. performed the statistical analysis, interpreted the data, and revised the article for important intellectual content. S.A., R.M., M.A., and L.H. made a substantial contribution to the curation of data and revised the article for important intellectual content. Y.L. made a substantial contribution to the conception and design of the study, interpretation of data analysis and drafting of the article, and critically revised the article, incorporating contributions from the coauthors. Y.L. is the guarantor of this work, and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors approved the final version.
Ethics Statement
All authors confirm that the research meets the ethics guidelines, including adherence to the legal requirements of the State of Israel.
Author Disclosure Statement
The authors have nothing to declare. None of the authors has conflicts of interest that could be perceived as prejudicing the impartiality of the research reported.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2