
Abstract
Background:
The optimal cutoff value of calcitonin (Ctn) levels measured using an electrochemiluminescence immunoassay (ECLIA) obtained from the washout fluid of fine needle aspiration (FNA-Ctn) for the diagnosis of medullary thyroid carcinoma (MTC) is currently not established. We evaluated the diagnostic accuracy and clinical utility of FNA-Ctn for the diagnosis and location of MTC in patients with nodular or multinodular goiters.
Methods:
This was a case–control study nested on a prospective multicenter cohort of patients with nodular or multinodular goiter, normal or elevated serum Ctn, and thyroidectomy indications. Ctn and FNA-Ctn were measured using ECLIA methodology before surgery. From this nested cohort, MTC cases and controls (non-medullary pathology) were identified from the final pathological analysis. Cumulative incidence sampling of controls was randomly performed at a ratio of 1:2. Sensitivity, specificity, and area under the receiver operator curve (AUROC) were calculated for patients and the total number of thyroid nodules.
Results:
From 1272 patients included in the prospective cohort, 50 MTC cases and 105 controls were included. In this study, 286 thyroid nodules were evaluated (63 MTC and 223 non-MTCs). The median serum Ctn value was significantly higher in cases (525 pg/mL [interquartile range (IQR), 162.5–1.200]) than in controls (1.6 pg/mL [IQR, 0.5–5.6]; p < 0.001). The median FNA-Ctn value was significantly higher in MTC nodules (3.100 pg/mL [IQR, 450–45,200]) than in non-MTC nodules (0.5 pg/mL [IQR, 0.5–0.5]; p < 0.0001). In 11 MTC patients with multinodular goiter, the FNA-Ctn value was significantly higher in non-medullary nodules located in the same lobe where an MTC nodule was diagnosed (p = 0.0002). Overall, the FNA-Ctn AUROC was 0.99 [95% confidence interval, 0.98–1.0], and a threshold of ≥220 pg/mL showed 100% sensitivity and 98% specificity for MTC diagnosis.
Conclusions:
The use of FNA-Ctn measured by ECLIA showed adequate diagnostic accuracy for MTC diagnosis. Moreover, it may be clinically useful for localization in multinodular goiter when lobectomy is considered.
Clinical Trial Registration:
Introduction
Medullary thyroid carcinoma (MTC) is a thyroid tumor of C cell or parafollicular origin that accounts for 1–6% of all thyroid tumors. 1,2 MTC can be sporadic or hereditary in multiple endocrine neoplasia (MEN) type 2 due to germline mutations of the rearranged during transfection (RET) oncogene. 2 –4 Hereditary MTC is usually a bilateral multicentric process. 5,6 The need for total thyroidectomy in hereditary MTC is well established. In contrast, sporadic MTC tends to be unifocal and confined to one lobe. 5 –7 The prognosis of MTC depends on various factors including age, sex, tumor genotype, and initial extension. Also, the presence of necrosis, high expression of Ki-67, high pre- and postoperative calcitonin (Ctn) levels, and the presence of distant metastases are associated with less favorable prognosis. 8,9 Up to 15–20% of patients will present with distant metastatic disease, and retrospective series report a 10-year survival of 10–40% from the time of detection of the distant metastatic disease. 10
The diagnosis of MTC presents significant challenges. 11,12 Ultrasonographic assessment is important in the initial evaluation as certain patterns indicate varying malignancy risks, but characteristics of MTC in ultrasonography are generally heterogeneous. 11,12 In fact, ultrasound has been shown to correctly identify only ∼50% of cases. 12 –14 As MTC derives from C cells that produce Ctn, a 32-amino acid peptide, its measurement remains the most reliable marker for diagnosing MTC. However, there is no fixed diagnostic cutoff point and its routine testing is not universally accepted. 11,12 The cytological appearance of MTC on fine needle aspiration (FNA) can be variable, causing it to be misdiagnosed. 11,12 The measurement of Ctn in the washout fluid of FNA biopsy (FNA-Ctn) can be used as a complementary test to confirm the diagnosis of MTC. 15,16 Indeed, a meta-analysis on the use of FNA-Ctn for the diagnosis of MTC showed that sensitivity was higher than 95% in most of the studies, but the authors highlighted methodology limitations due to the lack of well-established cutoff points. 17
To establish a diagnosis, baseline serum Ctn levels higher than 100 pg/mL are frequently indicative of MTC, but lower levels have unclear clinical implications. 2 Moreover, to improve diagnostic specificity, due to the low sensitivity of cytology, FNA-Ctn is relevant as an auxiliary and cost-effective approach. 18 FNA-Ctn is usually performed using a chemiluminescent method, 17 which is now being replaced by an electrochemiluminescence immunoassay (ECLIA), 19 as it has occurred at our three centers. However, adequate data regarding the appropriate cutoff value of Ctn in FNA-Ctn using ECLIA are lacking. Consequently, in this study, we aimed to assess the diagnostic accuracy of FNA-Ctn using ECLIA for the confirmation and localization of MTC, searching for a fixed FNA-Ctn threshold.
Methods
Study design and participating centers
This was a case–control study nested in a prospective multicenter cohort conducted in three centers in Argentina from March 2018 to May 2022. The participating centers were the Hospital Universitario Austral and the Sanatorio Las Lomas from Buenos Aires and the Hospital Alta Complejidad in Formosa. This article followed the STARD guidelines for observational and diagnostic studies. 20,21
Study design and case selection
In all three institutions, the diagnostic workup for thyroid nodules adhered to the recommendations provided by the American Thyroid Association (ATA) guidelines for the management of thyroid nodules. 22 This comprehensive approach included a combination of personal and family medical history assessment, physical examination, evaluation of thyroid function, and thyroid ultrasonography. The ultrasound criteria for fine needle aspiration biopsy (FNAB) were as follows: nodules larger than 1 cm with intermediate or high suspicious sonographic patterns, nodules larger than 1.5 cm with low suspicion sonographic patterns, and nodules larger than 2 cm with very low suspicion sonographic patterns. FNAB was not indicated for purely cystic thyroid nodules. 22 Surgery was also recommended in accordance with the current ATA guidelines. 22 Systematic determination of Ctn levels was performed for all patients.
Medullary carcinoma was excluded in individuals with Ctn levels of ≤9.8 pg/mL for women and ≤14.3 pg/mL for men. Those with Ctn levels above this threshold but ≤50 pg/mL were categorized as having a low risk of developing MTC. Patients with Ctn levels between ≥50 and ≤100 pg/mL were considered to be at moderate risk for MTC, while those with levels exceeding 100 pg/mL were classified as having a high risk for MTC. 23
In all cases of hypercalcitoninemia, other causes of non-medullary hypercalcitoninemia were ruled out. First, we repeated the serum Ctn levels twice throughout the study to minimize the risk of false positives and false negatives attributable to the biochemical test. We conducted a comprehensive medical history assessment to identify any underlying conditions that could be responsible for elevated Ctn levels. This assessment involves the use of a checklist designed for medications and diseases. To evaluate these conditions, we requested laboratory tests, clinical evaluation, FNA, and pathological examinations. 24 Cytological diagnosis was performed by an expert pathologist blinded to the clinical information according to our standardized protocol. A calcium stimulation test was conducted following the strategy reported by Mian et al. 25 It was performed in patients with Ctn measurements ≥9.8 pg/mL for women and ≥14.3 pg/mL for men, and ≤100 pg/mL (reconfirmed in a second assessment), and with a cytological report non-suspicious for malignancy.
Eligibility criteria: nested prospective cohort
Subjects included in the prospective cohort consisted of adult patients (≥18 years of age) with nodular or multinodular goiter, normal or elevated serum Ctn, with an indication for thyroidectomy. Thyroidectomy was recommended for patients presenting with at least one of the following criteria: toxic multinodular goiter; benign growing nodules >4 cm causing compressive or structural symptoms; FNA suggestive or indicative of thyroid malignancy; serum Ctn ≥100 pg/mL; and serum Ctn ≤100 pg/mL associated with a stimulation calcium test >100 pg/mL. In Ret-positive patients, the surgical decision was in accordance with the recommendations of the ATA guidelines. 22 We excluded patients who did not meet the surgical criteria, presented with chronic renal failure, and/or had a history of MEN previously operated.
Before surgery, all nodules were evaluated using ultrasound for number, diameter, location, composition, echogenicity, margins, types of calcifications, and pattern of vascularization. Based on these characteristics, nodules were classified according to the ATA guidelines. 22 To assess the diagnostic prediction of FNA-Ctn in patients with hypercalcitoninemia undergoing surgery, our plan was to conduct FNA-Ctn on all nodules ≥8 mm; benign and very low-risk nodules were excluded from analysis. In cases where patients had negative Ctn levels in the surgical plan, FNA-Ctn was only performed on nodules that met the ATA guidelines criteria. 22 In addition, the following determinations were performed in all patients before surgery: thyrotropin, antiperoxidase antibodies, antithyroglobulin antibodies, calcium, parathormone. The presurgical clinical routine included a physical examination and detailed inquiry regarding the patient's medication history.
Definition and selection of cases and controls
Cases were defined as MTC if they were histologically confirmed after total thyroidectomy. Pathological diagnosis was performed on the surgical specimens by an expert pathologist according to standardized procedures. To obtain anatomical, cytological, and anatomopathological correlates, each surgical piece was analyzed according to the ultrasound data of each patient. C cell hyperplasia (CCH) or microscopic MTC foci were evaluated immunohistochemically, as previously reported by Kaserer et al. 26 We used the eighth edition of the TNM staging system. 27 There was no central revision. Instead, expert pathologists independently reviewed each specimen at all three centers. Any discrepancies were resolved through consensus among three pathologists from each institution. Cumulative incidence sampling of controls (non-medullary pathology) was randomly performed from the nested prospective cohort in a ratio of 1:2.
Total thyroidectomy was indicated for all patients with a high pretest probability of medullary carcinoma. Central compartment lymphadenectomy was performed systematically in all cases, and lateral lymphadenectomy was indicated only when the involved lymph nodes were suspected or demonstrated clinically by ultrasound or cytology after FNA. To exclude sporadic or familial cases, a presurgical study of the RET proto-oncogene was performed, and the entire family was studied.
Exposure of interest: Ctn measurement and other related procedures
Ctn was measured using the ECLIA method, blinded to the pathology reports from all centers. Ctn determination was performed on a Cobas e601 autoanalyzer using the Elecsys® calcitonin test (Roche Diagnostics, Basel, Switzerland). According to the manufacturer, this test has a detection limit of 0.5 pg/mL, reference interval of up to 9.8 pg/mL for women and 14.3 pg/mL for men, and interval measurement range of 0.5–200,000 pg/mL. Harmonization of the preanalytical stage for the determination of serum Ctn in the three centers was ensured (morning blood extraction with 8 hours of fasting and obtaining fresh serum from a centrifugation protocol according to the specifications of each laboratory). All centers used the same assay for analysis.
The FNA-Ctn analysis was performed on the same sample by ultrasound-guided FNA, and all related procedures were performed uniformly across all patients at the three centers using a 23-gauge needle attached to a 10-mL plastic syringe. The aspirated fluid was partially expelled, smeared directly onto loaded microscope slides, fixed, and subjected to May-Grunwald–Giemsa and/or Papanicolaou staining. Cytological specimen adequacy was defined as the presence of at least 6 groups of 10 well-preserved epithelial cells. After smear preparation of specimens for cytological examination, the needle was rinsed with a standardized amount (0.5 mL) of Ctn-free normal saline. The samples were then processed for FNA biopsy using a standardized method for Ctn measurement from the washout fluid. 28 Cytological nodule samples were classified by an experienced pathologist in each center, blinded to serum Ctn and FNA-Ctn values. The Bethesda System was used for reporting thyroid cytopathology. 29 Each nodule was labeled during ultrasound screening to compare the findings. Lymph nodes FNA-Ctn were excluded from the analysis.
Statistical analyses
Continuous variables are described as mean ± standard deviation or median (interquartile range [IQR]), according to their distribution, and were compared using Student's T-test or the Wilcoxon test, respectively. For categorical data, numbers and proportions are shown, and comparisons were performed using chi-square or Fisher's exact test, as appropriate. The sensitivity, specificity, positive predictive value, negative predictive value, and accuracy were evaluated for FNA-Ctn in patients and in each thyroid nodule. The area under the receiver operator curve (AUROC) and likelihood ratios were estimated, and the best threshold or cutoff value according to sensitivity and 1 − specificity was selected using the Liu method. Using FNA-Ctn thresholds, the net reclassification index (NRI) was estimated to evaluate and quantify the agreement between the two cutoff points. Statistical analyses were performed using STATA v15 (College Station, TX). For all comparisons, statistical significance was set at p < 0.05.
Ethical aspects
The study complied with international ethical statements, the standards of Good Clinical Practice, and the Declaration of Helsinki and Argentine Act 25326/Habeas Data. The study was approved by the ethics committees of all centers, and written informed consent was obtained from all patients.
Results
In the prospective cohort (n = 7664), 5565 participants met the criteria for FNA biopsy for cytological examination (FNA cytology). Within this group, 1272 patients met the surgical criteria, from which cases and controls were selected. From the nested cohort, cumulative incidence sampling of controls (non-medullary pathology) was randomly performed at a 1:2 case:control ratio. Ultimately, 155 patients were included in the study (Fig. 1). No differences were found in sex or age between the two groups (Table 1). The mean age of the patients was 50 ± 14.9 years, and 62.6% (n = 97) were females. The median serum Ctn level was 5.5 pg/mL (IQR 0.5–2550 pg/mL). Regarding the number of nodules, 52.3% (n = 81), 18.1% (n = 28), 22.3% (n = 35), and 7.1% (n = 11) had only one, two, three, and four nodules, respectively.
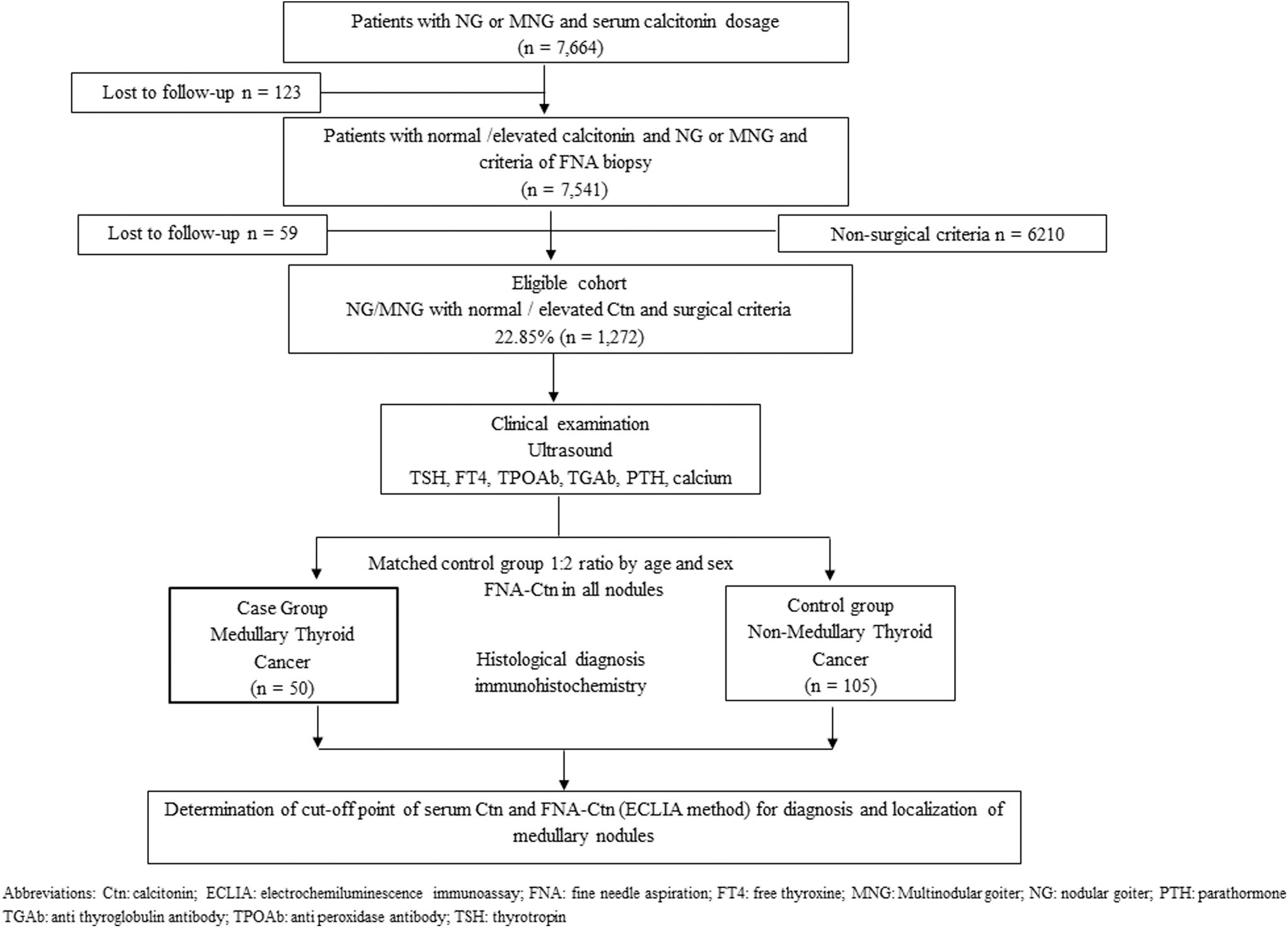
Flowchart showing the selection of patients from the nested prospective cohort study.
Baseline Characteristics of the Included Patients
Ctn, calcitonin; IQR, interquartile range; SD, standard deviation.
Table 2 shows the characteristics of MTC and non-medullary (non-MTC) nodules (Ctn level, location, and ultrasound pattern risk). Post-surgery, we identified 50 cases of MTC (32.3%); 105 controls (67.7%) with non-MTC were randomly selected. Baseline serum Ctn was significantly higher in patients with a diagnosis of MTC (median 525 pg/mL [IQR, 41.5–2550 pg/mL]) compared with non-MTC (1.6 pg/mL [IQR, 0.5–54.5 pg/mL], p = 0.001). In the MTC group, 40% (n = 20/50) of patients had a germline RET proto-oncogene mutation (Table 1). In the group of patients diagnosed with MTC (n = 50), 34% (n = 17) also presented with multinodular goiters (Table 3).
Characteristics of Medullary Thyroid Carcinoma Nodules and Non-Medullary Thyroid Carcinoma Nodules (Calcitonin Level, Location, and Ultrasound Pattern Risk)
FNA-Ctn, calcitonin in washout fluid of fine needle aspiration; MTC, medullary thyroid carcinoma; US, ultrasound.
Characteristics of Medullary Thyroid Carcinoma Nodules Associated with Non-Medullary Thyroid Carcinoma Nodules
This nodule was a post-surgery finding, which was not seen in ultrasound examination. RL/6 (no FNA-Ctn post-surgical finding).
H, high risk; I, intermediate risk; Isth, isthmus; L, low risk; LL, left lobe; RL, right lobe.
A total of 286 nodules detected on ultrasound in both groups (MTC and non-MTC) were analyzed. Of these, 22.0% (n = 63) were diagnosed with MTC, with a medullary nodule/non-medullary nodule ratio of 1:3. Table 4 shows the cytological characteristics of MTC and non-MTC nodules; among the 30 patients with sporadic MTC, a single focus of medullary carcinoma was observed in all cases. The characteristics of the patients with non-medullary hypercalcitoninemia are shown in Table 5. Only two patients presented with FNA-Ctn >220 with a calcium stimulation test of >100 pg/mL. The characteristics of all the patients with MTC are shown in Supplementary Table S1.
Cytological Diagnosis of Pathological Confirmed Medullary Thyroid Carcinoma Nodules and Non-Medullary Thyroid Carcinoma Nodules Using the Bethesda Classification System *
Reference. 29
AUS, atypia of undetermined significance.
Characteristics of Thyroid Nodules from Non-Medullary Thyroid Carcinoma Patients with Hypercalcitoninemia
F, female; CCH, C cell hyperplasia; LT, lymphocytic thyroiditis; M, male; N/A, not applicable; TT, total thyroidectomy; USR, ultrasound risk.
Accuracy of FNA-Ctn for diagnosis of MTC
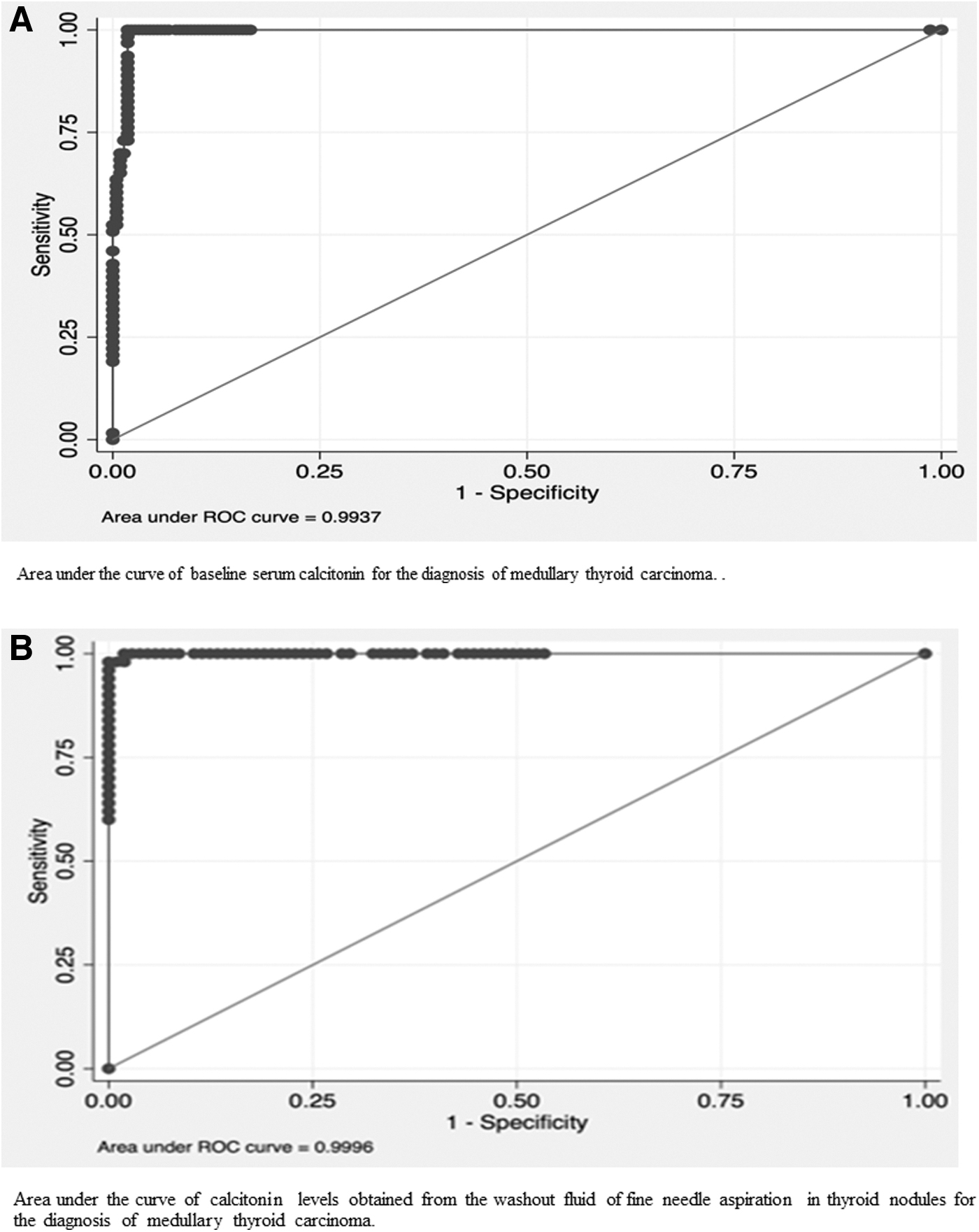
The median FNA-Ctn values in cases and controls were significantly different: 3100 pg/mL (IQR, 450–45,200 pg/mL) in medullary nodules versus 0.5 pg/mL (0.5–0.5 pg/mL) (p < 0.001) in non-medullary nodules. Among non-medullary nodules, the FNA-Ctn value was significantly higher in nodules located in the same lobe as the medullary tumor than in those located in the contralateral lobe: 41 pg/mL (IQR, 11–110 pg/mL) versus 0.5 pg/mL (IQR, 0.5–0.95 pg/mL) (p = 0.0002) (Fig. 2). When analyzing the diagnostic performance of FNA-Ctn for the identification of MTC nodules, the AUROC was 0.99 [95% confidence interval, 0.98–1.0], with the best cutoff point or threshold set at 220 pg/mL, 100% sensitivity, and 98% specificity (Table 6). Figure 3 shows the performance of baseline serum Ctn (Fig. 3A) and FNA-Ctn (Fig. 3B) in diagnosing MTC in thyroid nodules. The NRI of this new threshold, compared with the previously published cutoff point of 21 pg/mL, 17 was −0.026 (p = 0.007), showing a 2.7% increase in specificity with similar sensitivity.
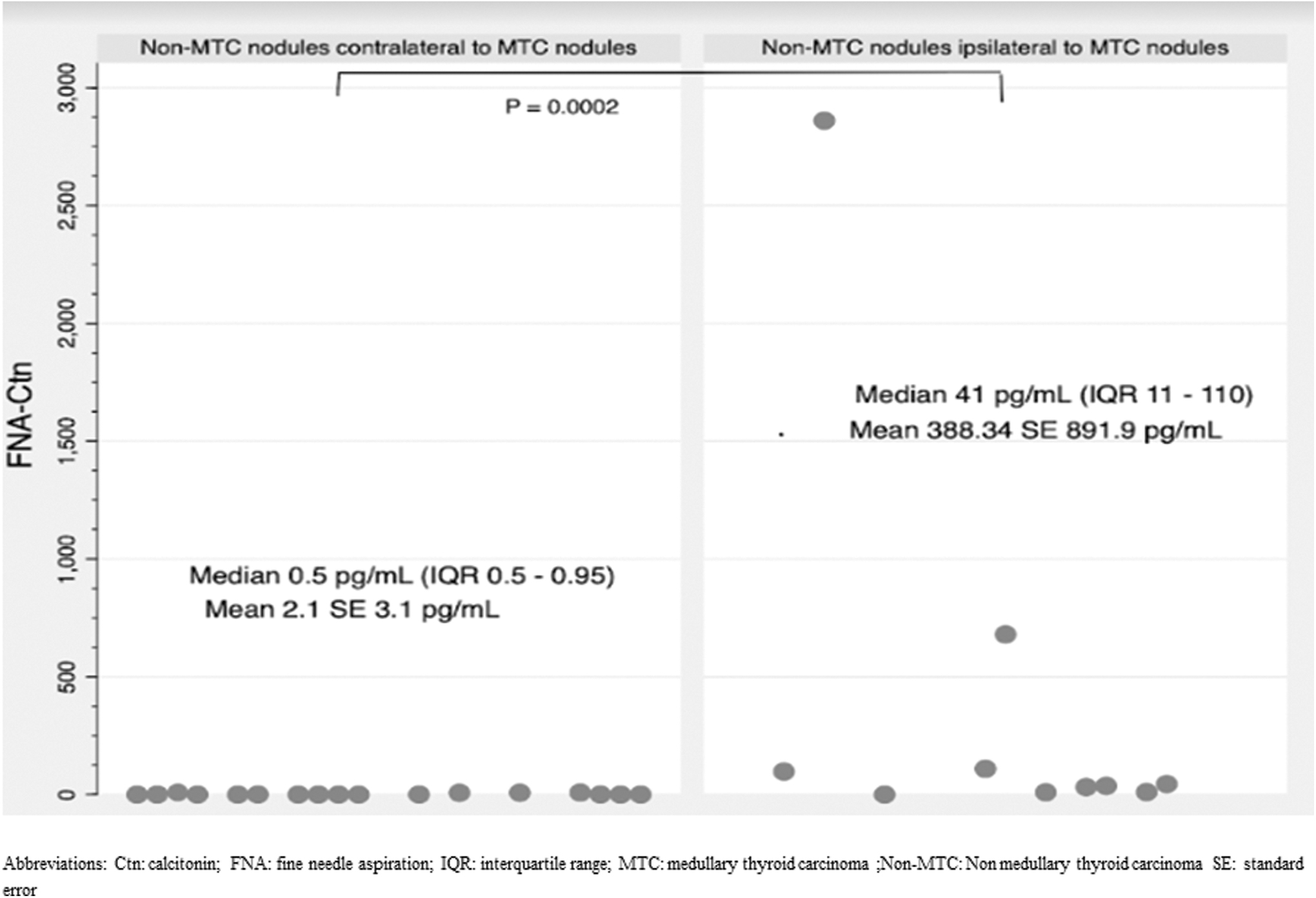
Comparison of Ctn values in washout fluid of FNA values in non-MTC nodules contralateral and ipsilateral to MTC nodules. Ctn, calcitonin; FNA, fine needle aspiration; MTC, medullary thyroid carcinoma.
Proposed Cutoff Points for Calcitonin Levels in Fine Needle Aspiration Biopsy Washout Fluid, Measured by Electrochemiluminescence Immunoassay, in the Diagnosis of Medullary Thyroid Carcinoma
Bold means best cutoff point.
Discussion
In this study, we assessed the diagnostic accuracy of FNA-Ctn in the identification of MTC. Using ECLIA, we observed a high sensitivity and specificity for the diagnosis of MTC. Moreover, we observed that FNA-Ctn values were significantly higher in medullary nodules than in non-MTC nodules. In this regard, within the subgroup of patients presenting with multinodular goiter and MTC, nodules sharing a lobe with MTC had significantly higher levels of Ctn than those located in the contralateral lobe. This finding has implications for the clinical utilization of FNA-Ctn as it may facilitate the localization of MTC nodules and enable individualized surgical approaches for these patients.
Clinical guidelines recommend the use of FNA-Ctn to increase the diagnostic reliability of MTC, 2,29 but only a small number of published series used ECLIA. 18,19 In this study, we propose a higher FNA-Ctn cutoff point than previously reported thresholds using the same methodology. 19 By applying this proposed cutoff point, we observed an improvement in specificity, as indicated by the NRI. The presence of CCH associated with non-medullary pathologies can lead to false-positive results in FNA-Ctn. 17,18,30 –33 We were able to demonstrate this in two cases of nonhereditary MTC. Neither of these patients was using GLP-1 receptor agonists. The first case involved a patient with Hashimoto's thyroiditis associated with a multinodular goiter and multicentric papillary carcinoma.
The second case featured a patient with a colloid goiter, and the cause of hypercalcitoninemia was not evident. Importantly, in the context of hereditary MTC, CCH should always be considered a precancerous lesion. Therefore, a comprehensive and conservative approach should be adopted to avoid misdiagnosis when addressing patients with borderline hypercalcitoninemia. We also observed false-positive results in patients with non-medullary nodules located in the same lobe as the medullary nodule. The relevance of this information depends on whether the final approach is a thyroid lobectomy. If the surgical plan is for a total thyroidectomy, then this information is not relevant.
FNA-Ctn has some possible constraints; although rare, there have been case reports of patients with MTC with undetectable serum Ctn. 34,35 However, to the best of our knowledge, no cases of negative serum Ctn and positive FNA-Ctn have been reported. The number of cases with undetectable serum Ctn was negligible, and most of these cases were microcarcinomas or undifferentiated tumors. 34,35 Serum Ctn is a useful screening test that confirms the presence of MTC when values are >100 pg/mL. 12,36 In our centers, we perform routine Ctn assays in all patients with thyroid nodules based on current evidence. 36 –38
Based on our findings, cytology associated with FNA-Ctn would be a useful approach in cases in which serum Ctn levels are >40 pg/mL. Upon confirmation of an MTC diagnosis, the main concern for advocating total thyroidectomy is the incidence of bilateral disease and the potential hereditary nature of this condition.
In our study, approximately half of the patients had hereditary MTC. It is possible that the high proportion may have resulted from referral bias, as the three participating centers were highly specialized institutions. We further studied the complete family members of each patient with hereditary MTC. Interestingly, most of these cases (70%) were multicentric, and 50% of them were bilateral, matching previous descriptions. 39 –41 In our sporadic forms of MTC, the prevalence of multifocality was 0%, although a prevalence of 6% of multifocality is described. 39 In those cases of hereditary MTC resulting from a germline mutation in the RET oncogene, 40,41 almost all patients are susceptible to bilateral and multifocal disease, thus making total thyroidectomy the preferred approach. 2,36,38,40
Another implication of our findings is related to the potential utility of FNA-Ctn in the localization of MTC nodules in patients with bilateral multinodular goiter. The standard of care for MTC is total thyroidectomy with central compartment lymph node dissection. 2,38,42 Although this approach may diminish MTC recurrence, 2,43 localizing MTC nodules that may be associated with non-medullary nodules is critical for determining the feasibility of lobectomy in patients with sporadic MTC and bilateral multinodular goiter. As most of the patients with early-stage localized MTC have a favorable prognosis, the suitability of this surgical approach is being revisited. 44 –46 In addition, total thyroidectomy may present some disadvantages such as lifelong thyroid hormone replacement and increased surgical complications. 47
Lobectomy may be an appropriate treatment option for patients with MTC who do not have germline RET mutations and have a limited primary lesion without evidence of local invasion or cervical lymph node metastasis, consistent with the Japanese guidelines. 44 In addition, patients with contralateral nodules where FNA-Ctn is undetectable may also be included in this treatment approach. This approach is feasible in institutions where serum Ctn is routinely measured and patient management and follow-up are performed by the same multidisciplinary team.
This study has limitations that need to be considered. First, we only included patients who underwent thyroidectomy, which may overestimate the accuracy of FNA-Ctn for diagnosing MTC. However, we restricted this selection of patients to have a more specific pathological diagnosis, either for cases and controls. Indeed, selection of cases was nested on the same prospective cohort in which cases arose. Second, we evaluated a single diagnostic method for measuring Ctn (ECLIA), which may limit the generalizability of our findings. Nevertheless, this may open further clinical use in the daily practice, underlying the multicenter study design that helped us to generalize our findings, and allowed us a comprehensive assessment of FNA-Ctn performance in this patient population.
Third, no false-positive results were observed in the nodules located in the contralateral lobe of the MTC location, which could have been due to the small sample size. Finally, the clinical application of this strategy may be questionable because MTC is rather an infrequent cancer. Nevertheless, we underline that prompt diagnosis is relevant considering the impact over survival outcomes when MTC is diagnosed at early stages.
In conclusion, the use of FNA-Ctn measured by ECLIA showed adequate diagnostic accuracy for MTC diagnosis. Moreover, FNA-Ctn could be a potentially valuable tool for guiding surgical management decisions, particularly in patients with sporadic MTC and multinodular goiter. This may reduce the risk of performing unnecessary total thyroidectomy. The high diagnostic accuracy of FNA-Ctn may improve the early detection of MTC, leading to a better prognosis and a higher likelihood of successful treatment outcomes.
Footnotes
Acknowledgments
We thank the Academic Department of the Austral University Hospital, professionals from all centers: Albarenque, Karina; San Roman, Alberto; Trujman, Alberto; Zorrilla, Mercedes; Prieto, Analia; Carassai, Mónica; Ferronato, Francisco; Damico, Antonela; Posadas, Silvana; Basualdo, Néstor; Nascimento, Cesar; Elortegui, Emiliano; and Arguello, Mauricio.
Authors' Contributions
A.C.C.: Conceptualization (lead), writing—original draft (lead), formal analysis (lead), writing—review and editing (lead). F.P.: Writing—original draft (equal), conceptualization (supporting), writing—review and editing (equal). J.R.: Writing—original draft (equal), formal analysis (lead), software (lead), writing—review and editing (equal), methodology (equal). P.B.: Review and editing (equal). M.L.: Review and editing (equal). M.J.J.: Review and editing (equal). E.S.: Review and editing (equal). A.V.: Review and editing (equal). C.F.: Review and editing (equal). P.S.: Writing—original draft (supporting), conceptualization (supporting), review and editing (equal). F.P.: Writing—original draft (equal), methodology (lead), review and editing (equal), formal analysis (equal). M.N.: Review and editing (equal), conceptualization (supporting).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1