
Abstract
Background:
Hypothyroidism is common, and in iodine-sufficient areas, it is primarily caused by autoimmune destruction of the thyroid gland. Observational studies have consistently shown an inverse association between serum 25-hydroxyvitamin D concentration and autoimmune diseases; however, there is a lack of evidence from randomized controlled trials to support a benefit of vitamin D supplementation, particularly for autoimmune thyroid diseases. We, therefore, aimed to assess the effect of vitamin D supplementation on the incidence of hypothyroidism.
Methods:
We analyzed data from the D-Health Trial (n = 21,315), a randomized double-blind placebo-controlled trial of 60,000 international units per month of supplemental vitamin D3 among Australians aged 60 years and over. Hypothyroidism, a tertiary outcome of the D-Health Trial, was defined by treatment with levothyroxine, ascertained through linkage with the Australian Pharmaceutical Benefits Scheme. The outcome was time to first prescription of levothyroxine. We began follow-up at 12 months after randomization; people who had died or who had been dispensed levothyroxine during the first year were excluded. Flexible parametric survival models were used to assess the effect of vitamin D supplementation on hypothyroidism, overall and within strata defined by age, sex, body mass index, and predicted baseline vitamin D status.
Results:
We included 17,851 participants in the main analysis (vitamin D = 8939; placebo = 8912). During a median follow-up of 4.1 years (interquartile range 4.1–4.1), 293 participants developed hypothyroidism (vitamin D = 138 [1.5%]; placebo = 155 [1.7%]). Vitamin D supplementation did not significantly reduce the incidence of hypothyroidism (overall hazard ratio [HR] 0.89; 95% confidence interval [CI] 0.71–1.12). There was some suggestion of an effect in females (overall HR 0.78; CI 0.58–1.06) but not in males (overall HR 1.06; CI 0.74–1.50; p interaction 0.20).
Conclusions:
Vitamin D supplementation did not reduce the incidence of hypothyroidism overall; however, the possible beneficial effect observed in females warrants further investigation.
Clinical Trial Registration:
Australian New Zealand Clinical Trials Registry: ACTRN12613000743763.
Introduction
Hypothyroidism is common. In iodine-sufficient countries, its prevalence ranges from 1% to 2%, 1 and the most common cause is autoimmune thyroid disease. The prevalence of hypothyroidism increases with age, and females have greater risk of developing it than males.
Vitamin D may play a role in autoimmune diseases, including those of the thyroid. Many experimental studies have shown that vitamin D downregulates proinflammatory responses, 2 and vitamin D and the thyroid hormone bind to similar nuclear receptors. Moreover, certain vitamin D gene polymorphisms may be associated with risk of autoimmune thyroid diseases. 3
A 2021 systematic review and meta-analysis of observational studies found inverse associations between serum 25-hydroxyvitamin D [25(OH)D] concentration and risk of certain thyroid diseases. 4 These included hypothyroidism (9 studies, n = 1174), autoimmune thyroid diseases (13 studies, n = 12,916), and Hashimoto's thyroiditis (12 studies, n = 2440). However, there was significant heterogeneity, and the associations may have been due to reverse causality or residual confounding. Indeed, in a Mendelian randomization study, where confounding bias is less likely, there was no association between genetically predicted 25(OH)D concentration and hypothyroidism (n = 326,409, odds ratio was 1.00). 5 However, the study assumed a linear association.
Few randomized controlled trials (RCTs) have investigated the effect of vitamin D supplementation on autoimmune thyroid diseases. The VITamin D and OmegA-3 TriaL (VITAL, n = 25,871) found that daily supplementation with 2000 international units (IU) of vitamin D for ∼5 years reduced the incidence of a combined group of autoimmune diseases (hazard ratio [HR] 0.78; 95% confidence interval [CI] 0.61–0.99). 6
However, vitamin D supplementation did not reduce the incidence of confirmed autoimmune thyroid diseases (HR 1.63; CI 0.77–3.45). 6 Two meta-analyses of RCTs found that vitamin D supplementation reduced the level of thyroid peroxidase antibodies in patients with Hashimoto's thyroiditis (6 studies, n = 258) 7 and autoimmune thyroiditis (6 studies, n = 344), 8 suggesting it might be useful in the treatment of autoimmune thyroiditis.
The D-Health Trial was conducted to determine the effect of vitamin D supplementation on the health of older Australians. The primary outcome of the trial was all-cause mortality, for which we found no beneficial effect of vitamin D supplementation. 9
The aim of this study was to determine the effect of vitamin D supplementation on incidence of hypothyroidism in older Australians, where new prescription of levothyroxine was used as surrogate for diagnosis.
Materials and Methods
Trial design, participants, and intervention
The D-Health Trial was a randomized placebo-controlled double-blind trial, conducted from 2014 to 2020 among 21,315 Australians aged 60–84 years, using a population register as the sampling frame. Details of the trial methods have been published. 10 The intervention was monthly oral doses of either 60,000 IU of cholecalciferol (vitamin D3) or placebo for up to 5 years. Hypothyroidism was a prespecified tertiary outcome. 11
We used automated computer-generated permuted block randomization (1:1), stratified by age (60–64, 65–69, 70–74, ≥ 75 years), sex, and state of residence. Staff and investigators did not have access to the allocation list.
The D-Health Trial is registered on the Australian New Zealand Clinical Trials Registry: ACTRN12613000743763.
Ethics approval
The QIMR Berghofer Medical Research Institute Human Research Ethics Committee (HREC) approved this study (P1519). Data linkage was approved by ACT Health HREC, NSW Population and Health Services Research Ethics Committee, Department of Health WA HREC, and Department of Health Tasmania HREC. Written or online informed consent was obtained from all participants. This research was completed in accordance with the Declaration of Helsinki.
Baseline characteristics
Participants completed a baseline survey that collected sociodemographic, lifestyle, and medical information. We did not measure baseline serum 25(OH)D concentration due to prohibitive cost. Instead we used a binary classifier to predict whether deseasonalized baseline serum 25(OH)D concentration was <50 nmol/L. 12 The classifier was built and internally validated using data collected from a random subset of placebo participants who provided a blood sample during the intervention; its area under the receiver operating characteristic curve for the prediction model was 0.71 (CI 0.63–0.78). 12 We did not ascertain pre-existing hypothyroidism at baseline.
Ascertainment of hypothyroidism
Participants gave optional consent for their records to be linked with Australia's Pharmaceutical Benefits Scheme (PBS) and Medicare Benefits Schedule (MBS) data sets. The PBS data set contains information on prescriptions for medicines that qualify for a government subsidy and for which a claim has been processed. The MBS database captures services provided to private patients in private hospitals, public hospitals, or outside hospital. These data sets were provided by Services Australia.
We ascertained hypothyroidism using prescription of levothyroxine as a surrogate for diagnosis. Levothyroxine (Anatomical Therapeutic Chemical [ATC] classification code “H03AA01”) is mainly prescribed for the treatment of hypothyroidism or used in conjunction with surgery or radioactive iodine therapy to treat thyroid cancer. We defined participants who had at least one prescription of levothyroxine dispensed within 12 months after randomization as having pre-existing hypothyroidism, and those whose first prescription was >12 months after randomization as having incident hypothyroidism. We, therefore, began follow-up at one year after randomization. The outcome of this study was time to first prescription of levothyroxine as a surrogate for incident hypothyroidism.
Follow-up, eligibility, and sample size
Follow-up ended at the earliest of (1) first prescription of levothyroxine, (2) thyroidectomy, (3) thyroid cancer diagnosis, (4) date last known to be alive, or (5) 5 years and 1 month after randomization.
Deaths were ascertained primarily through linkage to state death registries. 9 We ascertained thyroidectomy and thyroid cancer using MBS data, hospital admitted patient data, and linked cancer registry data (Supplementary Table S1).
In the main analysis, we excluded people who did not give consent to linkage with both MBS and PBS data sets, who did not have hospital data, who were diagnosed with thyroid cancer before randomization, who had pre-existing hypothyroidism, who had a thyroidectomy and/or thyroid cancer within 12 months after randomization, or whose last known date alive was within 12 months of randomization (see Supplementary File S1).
The sample size for the D-Health Trial was chosen to enable 80% power to detect a difference of 9% in the mortality rate with a type 1 error rate of 0.05. 10 Before commencing the current analyses, we performed an effect size calculation to determine whether the detectable effect size was small enough to warrant proceeding with the planned analyses. Assuming that the available sample size (n = 17,853) would be split equally between the vitamin D and placebo groups, and assuming incidence rates of 2.5 per 1000 person-years at risk (PYAR) for males and 8.2 PYAR for females based on a previous study, 13 we estimated that 176 events would be experienced in the placebo group, resulting in 80% power to detect a difference of 28% in the hazard of hypothyroidism.
Monitoring adherence and adverse events
We used annual surveys to ascertain the number of study capsules taken in the previous year; intake of off-study supplements containing vitamin D; and new diagnoses of hypercalcemia, kidney stones, and hyperparathyroidism. Participants were also asked to contact study staff through phone or email if they experienced an adverse event at any time during the intervention. Serum 25(OH)D concentration was measured in blood samples of a subset of participants randomly selected each year. Full details of adherence and adverse events have been published. 9
Blinding
During the intervention period, all participants, investigators, study staff, and analysts were blinded to group allocation. In March 2020, after all participants had completed the intervention, participants were informed of their study group allocation. Blinding was maintained for investigators, analysts, and study staff until analyses of the primary outcome (mortality) 9 were completed.
Code for the current study was written using a blinded data set (i.e., the randomization and participant identification codes had been removed, and participants were randomly assigned to two equal-sized groups). The analyst was not supplied with the “true” data set (i.e., data set with the real randomization code) until after the analysis plan was finalized and saved on a read-only server.
Statistical methods
We analyzed the data using SAS version 9.4 (SAS Institute, Inc., Cary, NC), R version 4.1.1 (R Foundation for Statistical Computing, Vienna, Austria), and Stata (StataCorp LLC, TX) Version 18. Analyses estimating the effect of vitamin D supplementation followed the intention-to-treat principle.
We used flexible parametric survival models to estimate the effect of vitamin D supplementation on incidence of hypothyroidism (Supplementary File S1); these models included randomization group, age, sex, and state of residence at randomization. We fitted 2 models: 1 assumed proportional hazards, and the other allowed the HR for randomization group to vary with time. For the latter, we included an interaction between randomization group and time since follow-up. We assessed the interaction between time and randomization group using a likelihood ratio test comparing the two models.
Treating death, thyroidectomy, and thyroid cancer (without prior hypothyroidism) as competing risks, we plotted the cause-specific cumulative incidence of hypothyroidism for each randomization group (Supplementary File S1). We also estimated standardized cause-specific cumulative incidence; the cumulative incidence functions were standardized to the distribution of age at randomization, sex, and state of residence at randomization (Supplementary File S1).
We examined the associations between selected baseline characteristics and the prevalence and incidence of hypothyroidism using logistic regression and flexible parametric survival models. All models included randomization group, age at randomization, and sex, and we assumed proportional hazards when fitting survival models.
We used a significance level of p < 0.05 with no adjustment for multiple testing. 14,15
Subgroup analyses
We tested for effect modification by selected baseline characteristics of (1) age (<70; ≥70 years), (2) sex (males; females), (3) body mass index (BMI) (<25; 25–<30; ≥30 kg/m2), and (4) predicted baseline serum 25(OH)D concentration (<50; ≥50 nmol/L). We assumed proportional hazards for all covariates in the survival models and report the overall HR for each subgroup. We used a likelihood ratio test to assess the interaction between randomization group and each variable.
Sensitivity analyses
We conducted two sensitivity analyses. In 1 analysis we started follow-up from 7 months after randomization to allow for some flexibility in the definition of pre-existing hypothyroidism (another 133 participants were included in this analysis). The other sensitivity analysis was to consider medical treatment of hyperthyroidism as a competing risk, using prescription of carbimazole or propylthiouracil (ATC codes “H03BB01” and “H03BA02”) as a surrogate for hyperthyroidism (44 participants were excluded from this analysis due to having at least 1 prescription of carbimazole or propylthiouracil dispensed within 12 months after randomization). Further details are described in Supplementary File S1.
Exploratory analyses
We plotted cause-specific cumulative probability of hypothyroidism according to randomization group separately for each sex. We also estimated time-varying HRs separately for each sex.
Results
We included 17,851 participants (vitamin D, n = 8939; placebo, n = 8912) in the main analysis (Fig. 1). Females were more likely to be excluded than males (Supplementary Table S2) due to their higher prevalence of pre-existing hypothyroidism (Supplementary Table S3). The baseline characteristics of included participants were well balanced between the randomization groups (Table 1).
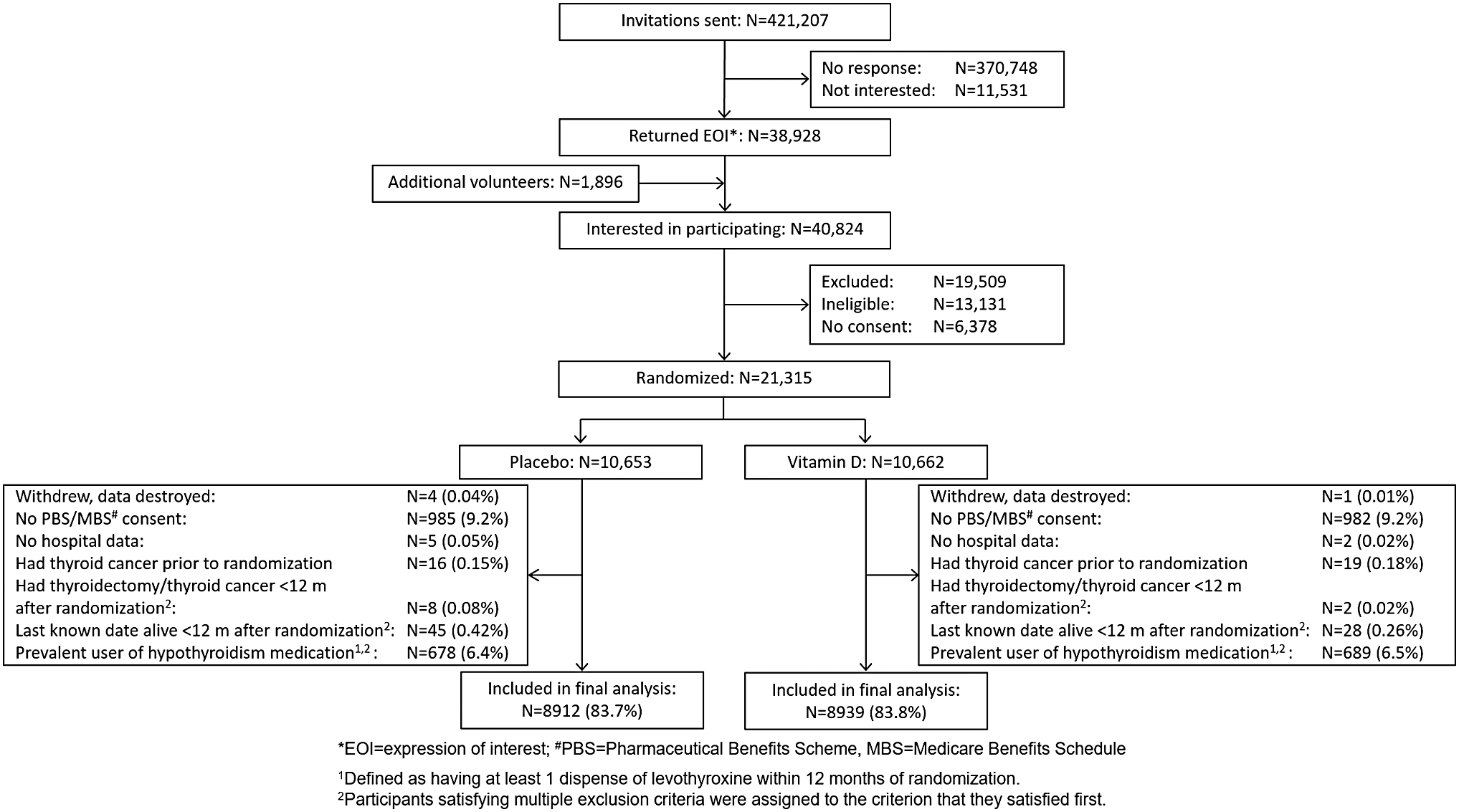
Participant CONSORT flow diagram.
Baseline Characteristics of Participants Included in the Analysis According to Randomization Group
25(OH)D, 25-hydroxyvitamin D; BMI, body mass index.
During a median follow-up of 4.1 years, 293 (1.6%) participants developed hypothyroidism. Females, those in older age groups, who were obese, or who had poorer self-rated overall health and/or quality of life, had greater prevalence and incidence of hypothyroidism (Supplementary Table S4). People with predicted baseline serum 25(OH)D concentration ≥50 nmol/L had lower incidence of hypothyroidism (Supplementary Table S4).
Effect of vitamin D supplementation on hypothyroidism
We observed 11% lower incidence of hypothyroidism in the vitamin D group compared with the placebo group, although the confidence bounds were consistent with a null finding or up to a 12% increased risk (HR 0.89; CI 0.71–1.12, Table 2). When we allowed the HR to vary with time, there was a suggestion of stronger benefit early in follow-up, although the p-value for the interaction between randomization group and follow-up time was not significant (p = 0.30, Fig. 2).

Effect of vitamin D supplementation on incidence of hypothyroidism.
The Effect of Vitamin D Supplementation on the Incidence of Hypothyroidism a
Follow-up began 1 year postrandomization and ended at the earliest of (1) first prescription of levothyroxine (used as a surrogate for diagnosis of hypothyroidism), (2) thyroidectomy, (3) thyroid cancer diagnosis, (4) date last known to be alive, (5) 5 years and 1 month after randomization.
Estimates produced using flexible parametric survival models that included randomization group, age, sex, and state of residence at baseline.
Cause-specific standardized cumulative incidence estimated treating death (without prior hypothyroidism) and thyroidectomy and/or thyroid cancer (without prior hypothyroidism) as competing risks. Incidence, expressed as a percentage, is standardized to the distribution of age, sex, and state of residence at baseline for all participants included in this study.
Estimates from a model that also included an interaction between randomization group and time since randomization. p-Value for interaction = 0.30.
Overall estimate from a model that assumed proportional hazards.
CI, 95% confidence interval; HR, hazard ratio.
The difference in standardized cause-specific cumulative incidence after 4 years of follow-up was 2.0 per 1000 lower (CI 5.6 per 1000 lower to 1.7 per 1000 higher) (Supplementary Fig. S1); 500 people would need to be treated to avoid 1 case of hypothyroidism. The effect was similar when we considered hyperthyroidism as a completing risk (Supplementary Table S5, Supplementary Figs. S2 and S3). When follow-up started from 7 months after randomization, we observed a somewhat stronger effect, with confidence bounds consistent with 1–34% lower risk (n = 17,984; HR 0.81; CI 0.66–0.99; Supplementary Table S6, Supplementary Figs. S4 and S5).
Vitamin D supplementation reduced the incidence of hypothyroidism in females (HR 0.78; CI 0.58–1.06) but not in males (HR 1.06; CI 0.74–1.50; p-interaction = 0.20) (Fig. 3). In exploratory analyses, the cumulative probability of hypothyroidism was higher in the placebo group than in the vitamin D group in females and the HR remained <1 at all timepoints; however, the confidence intervals were consistent with no effect or a ∼10% to ∼50% increased risk (Supplementary Fig. S6). This was not the case for males (Supplementary Fig. S7).
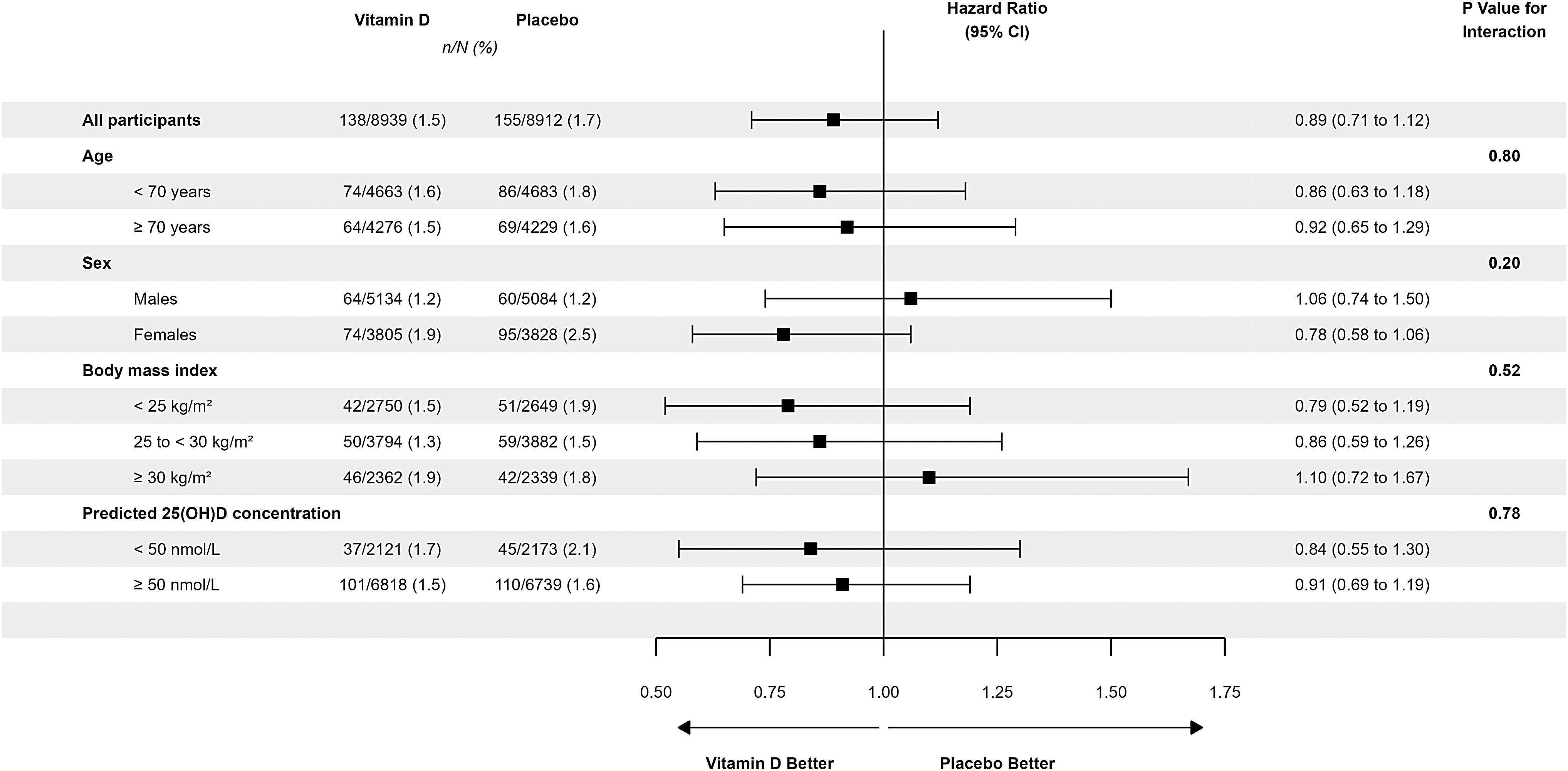
The effect of vitamin D supplementation on incidence of hypothyroidism overall and in subgroups of participants. HRs (CI) comparing vitamin D with placebo are from flexible parametric survival models. All models include randomization group, age, sex, and state of residence at baseline. Models producing estimates by levels of age, sex, BMI, and predicted baseline 25(OH)D concentration include the characteristic of interest and an interaction between randomization group and the characteristic of interest. p-Values were from likelihood ratio tests that compared models with and without the interaction term. Follow-up began 1 year postrandomization and ended at the earliest of (1) first prescription of levothyroxine (used as a surrogate for diagnosis of hypothyroidism), (2) thyroidectomy, (3) thyroid cancer diagnosis, (4) date last known to be alive, and (5) 5 years and 1 month after randomization. 25(OH)D, 25-hydroxyvitamin D; BMI, body mass index; HR, hazard ratio.
Discussion
In our main analysis of the D-Health Trial data, we did not find a significant effect of vitamin D supplementation on the incidence of hypothyroidism. However, there was a suggestion of benefit in females, and in a sensitivity analysis in which follow-up commenced at 7 months rather than at 12 months postrandomization.
In the D-Health Trial, the prevalence of pre-existing hypothyroidism was 12.2% in females and 2.8% in males (overall 7.1%). The cumulative incidence was 1.6% (2.2% in females and 1.2% in males) over a median 4.1 years. Consistent with the literature, these were strongly associated with age, BMI, self-rated overall health, and quality of life. 1,16 –18
The prevalence of pre-existing hypothyroidism in females was higher than in a cohort of Australians aged ≥49 years but was similar in males (5.0% in females and 2.7% in males, overall 6.8% n = 2665), 17 and incidence was lower than that observed over 5 years in analyses restricted to participants aged ≥55 years (6.0% in females and 2.1% in males). 18 The incidence of autoimmune thyroid disease reported in the VITAL trial was somewhat lower than in our study (0.75% over a median 5.3 years), 6 which may have been driven by the younger population in the VITAL trial and reliance on self-report of hypothyroidism in surveys.
The VITAL trial did not find a benefit of vitamin D supplementation on autoimmune thyroid diseases (HRs [CI] for confirmed and confirmed plus probable autoimmune thyroid diseases were 1.63 [0.77–3.45] and 1.05 [0.78–1.41], respectively). 6 Although our effect estimate is within VITAL's confidence intervals for autoimmune thyroid disease, differences in the approaches used to ascertain outcomes mean that our result is not directly comparable with those of VITAL trial. Indeed, the VITAL trial classified only 33 participants as having confirmed autoimmune thyroid disease. Of note, however, the VITAL trial did find evidence of benefit on incidence of combined autoimmune diseases, 6 which in combination with our result in females suggests that vitamin D might play a role in autoimmune diseases.
We observed a strong and statistically significant effect in the sensitivity analysis in which follow-up commenced at 7 months rather than 12 months postrandomization. This may have been a function of sample size (i.e., these analyses included an additional 133 people and an additional 98 incident hypothyroidism events). Assuming this evidence of a benefit earlier in the follow-up period reflects a true effect, it may be that there was a pool of people with preclinical hypothyroidism who benefitted from vitamin D. These people would have been excluded from the at-risk population in our main analysis, resulting in less benefit subsequently.
The suggestion of a difference between males and females may be a chance finding. However, it is plausible that there is a greater effect of vitamin D in females than in males since there are large differences in incidence between females and males, suggesting that the pathogenesis of the disease is influenced, at least in part, by sex.
A previous study found that among patients with relapsing-remitting multiple sclerosis (n = 42), another autoimmune disease, the immune-modulatory effects of 1,25(OH)2D (as measured by the inhibition of T cell proliferation, reduction in interferon-γ- and interleukin [IL]-17- producing cell number, and increase in T cell anti-inflammatory cytokine production IL-10) were stronger in females (n = 25) than in males (n = 17). 19 The study also found that estrogens modulated vitamin D metabolism by downregulating the expression of the CYP24A1 gene that encodes the catabolic 24-(OH)ase enzyme and increased uptake of vitamin D binding protein in T cells. 19
Our study has some limitations. First, we did not assess hypothyroidism at baseline. Instead, we used prescription of levothyroxine within 12 months postrandomization as a surrogate measure for prevalent hypothyroidism. Importantly, the estimated prevalence at baseline was similar between the vitamin D and placebo groups. Second, we defined incident hypothyroidism using treatment with levothyroxine instead of measuring thyroid-stimulating hormone. We acknowledge there is no one clinical or laboratory threshold for commencing levothyroxine for hypothyroidism, and there is evidence for overprescription in many countries. 20
Therefore, some people without persistent hypothyroidism may have been defined as having incident hypothyroidism. Conversely, we may not have captured all events of actual hypothyroidism, particularly subclinical cases. Both scenarios potentially reduced our ability to detect an effect. Finally, we did not measure baseline serum 25(OH)D concentration. The model we used to predict whether baseline serum 25(OH)D concentration was <50 nmol/L had a modest positive predictive value (23%).
Hence, many participants will have been misclassified as having low serum 25(OH)D concentration when they did not, and this nondifferential misclassification may have attenuated any effect of vitamin D in people with low predicted baseline 25(OH)D concentration. Consequently, analyses stratified by predicted baseline 25(OH)D concentration should be interpreted with caution.
The D-Health participants were largely vitamin D replete and the prevalence of vitamin D deficiency in the placebo group was slightly lower than in Australians aged ≥65 years (13% vs. 16% 21 ). While our findings are likely generalizable to the Australian population, they should not be extrapolated to populations with greater prevalence of vitamin D deficiency.
In conclusion, vitamin D supplementation did not reduce the incidence of hypothyroidism overall. There was, however, a possible protective effect in females, which is consistent with previous studies suggesting vitamin D might protect against some autoimmune diseases.
Footnotes
Acknowledgments
We thank: The D-Health Trial staff and members of the Data and Safety Monitoring Board (Patricia Valery, Ie-Wen Sim, Kerrie Sanders). The D-Health Trial participants who committed to this research. The State and Territory health departments (Western Australia, Victoria, South Australia & Northern Territory, New South Wales, Queensland, and Tasmania) for the provision of inpatient hospital data, State cancer registries for cancer notifications data, the State Registries of Births, Deaths and Marriages for death data, and State and Territory Data Linkage Units for undertaking linkage of these data sets. Services Australia for supplying MBS and PBS data. This study was approved by the following HRECs: QIMR Berghofer HREC, ACT Health HREC, NSW Population and Health Services Research Ethics Committee, Department of Health WA HREC.
Authors' Contributions
M.W. contributed to data curation (equal), conceptualization (supporting), methodology (equal), formal analysis (equal lead), writing—original draft (equal lead), and writing—review and editing (equal). H.P. was involved in conceptualization (supporting), methodology (equal), formal analysis (equal lead), writing—original draft (equal lead), and writing—review and editing (equal). S.T.R. carried out formal analysis (supporting) and writing—review and editing (equal).
C.B. was in charge of trial design (supporting), recruitment (equal), data collection (equal), data curation (equal), and writing—review and editing (equal). B.D.R. took charge of trial design (supporting), recruitment (equal), data collection (equal), data curation (equal), and writing—review and editing (equal). B.K.A. took charge of trial design (supporting) and writing—review and editing (equal). P.R.E. carried out trial design (supporting) and writing—review and editing (equal).
D.R.E. was involved in trial design (supporting) and writing—review and editing (equal). G.H. was involved in trial design (supporting) and writing—review and editing (equal). J.C.v.d.P. carried out trial design (supporting) and writing—review and editing (equal). A.J.V. carried out trial design (supporting) and writing—review and editing (equal). P.M.W. took charge of trial design (supporting) and writing—review and editing (equal).
D.C.W. took charge of trial design (supporting) and writing—review and editing (equal). D.S.A.M. was in charge of trial design (supporting), data collection (equal), conceptualization (supporting), methodology (equal), writing—original draft (supporting), writing—review and editing (equal), and supervision (equal). R.E.N. was in charge of trial design (lead), recruitment (equal), data collection (equal), data curation (equal), conceptualization (lead), methodology (equal), formal analysis (supporting), writing—original draft (supporting), writing—review and editing (equal), and supervision (equal).
Author Disclosure Statement
M.W., H.P., S.T.R., C.B., B.D.R., B.K.A., D.R.E., G.H., J.C.v.d.P., A.J.V., D.C.W., and D.S.A.M. have nothing to disclose. P.R.E. received grants and other from Amgen, other from Sanofi, grants and other from Novartis, grants from Eli-Lilly, and grants from Alexion. P.M.W. received funding from Astra Zeneca for an unrelated study of ovarian cancer. R.E.N. received funding from Viatris for an unrelated study of pancreatic cancer.
Funding Information
The D-Health Trial is funded by National Health and Medical Research Council (NHMRC) project grants (APP1046681; APP1120682). The vitamin D assays were performed at the University of Western Australia, supported by infrastructure funding from the Western Australian State Government in partnership with the Australian Federal Government, through Bioplatforms Australia and the National Collaborative Research Infrastructure Strategy (NCRIS). M.W., H.P., S.T.R., C.B., B.D.R., B.K.A., D.R.E., G.H., J.C.v.d.P., and A.J.V. received no funding. P.R.E. received NHMRC fellowship (GNT1197958). P.M.W. received NHMRC fellowship (GNT1173346). D.C.W. received NHMRC fellowship (GNT1156072). D.S.A.M. was supported by a Metro North Clinician Research Fellowship and the Queensland Advancing Clinical Research Fellowship. R.E.N. was supported by an NHMRC fellowship (GNT1060183).
Supplementary Material
Supplementary File S1
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Figure S7
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6