
Abstract
Background:
Total thyroidectomy (TT) and hemithyroidectomy (HT) are acceptable surgical options for the treatment of low-risk differentiated thyroid cancer (DTC). While previous data suggest similar disease-free and disease-specific survival regardless of initial surgical treatment, the effect of the extent of surgery on health-related quality of life (HRQOL) is less clear. This systematic review aimed to examine HRQOL in low-risk DTC survivors after TT compared with HT.
Methods:
A search of PubMed, CINAHL, Cochrane, PsycINFO, and Scopus databases was conducted to identify studies published between January 1, 2011, and December 31, 2022, that assessed HRQOL predominantly in patients with low-risk DTC who underwent open thyroid surgery. Covidence™ software was used to apply the inclusion criteria, and a validated instrument was used to assess study quality.
Results:
Sixteen of the 1402 identified studies were included: 5 prospective and 11 retrospective cohort studies. The majority of included studies were of good quality (n = 14) and were from Asia and the Middle East (n = 11). Overall, six studies concluded that HT led to a better HRQOL than TT, two concluded that HT only resulted in better HRQOL compared with TT with central neck dissection (CND), and two concluded HT resulted in better short-term HRQOL that dissipated by 6 months postoperatively. The HRQOL domains found across all studies to be most consistently improved after HT included physical health, psychological/emotional, and social function. Factors found to be associated with HRQOL in more than one study included age, stage, and marital status.
Conclusion:
Differences in HRQOL after HT and TT tended to favor HT particularly when measured <6 months after surgery or when compared with TT with CND. Additional prospective and ideally randomized data are needed to fully determine the impact of the extent of surgery on HRQOL in patients with low-risk thyroid cancer.
Introduction
The incidence of low-risk differentiated thyroid cancer (DTC) has increased globally. However, the optimal extent of surgery for low-risk thyroid cancer remains controversial. The current American Thyroid Association (ATA) guidelines released in 2015 endorse both hemithyroidectomy (HT) and total thyroidectomy (TT) as appropriate options for patients presenting with low-risk disease (e.g., <4 cm without extrathyroidal extension or suspicious lymphadenopathy). 1 While the rate of HT has increased since the publication of these guidelines, 2,3 TT remains the dominant surgery performed for patients with low-risk DTC in the United States even among high-volume and academic surgeons. 4,5 TT is known to have higher rates of complications, but the effect of this surgical procedure on health-related quality of life (HRQOL) is less clear. 6
In the last decade, systematic reviews published on low-risk thyroid cancer have focused on active surveillance compared with surgical intervention, remote access site versus open surgery, cost, complication rates, and overall or recurrence-free survival. 7 –10 Few systematic reviews, however, have focused specifically on HRQOL differences between TT and HT. 11 While oncologic outcomes are similar between both procedures, differences in patient experience may impact HRQOL. For example, TT mandates lifelong thyroid hormone replacement and subjects patients to the risk of postoperative hypoparathyroidism. Conversely, HT patients are not at risk of hypoparathyroidism and may not need thyroid hormone. However, these patients may ultimately require completion thyroidectomy and experience challenges monitoring thyroglobulin levels for recurrence.
Given that long-term survival in patients with low-risk thyroid cancer is close to 100% regardless of initial surgical extent, understanding quality-of-life-related outcomes is of paramount importance to appropriately counsel patients preoperatively. The goal of the current study was to systematically review the contemporary literature examining HRQOL among survivors of low-risk DTC after TT compared with HT. 12
Methods
Literature search strategy
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist was followed for this systematic review. 13 Before conducting the study, we performed a search with the assistance of a medical librarian of all systematic reviews related to this topic to ensure that it added to the literature. A computerized literature search of PubMed, CINAHL, Cochrane, PsycINFO, and Scopus databases was performed by an academic librarian with training in systematic reviews on February 23, 2023, and included articles published online between January 1, 2011, and December 31, 2022. We selected January 1, 2011, as a start date to provide a contemporary view of the literature with recently developed measures and provide an update to one of the most commonly cited systematic reviews on this topic, which included articles published through 2010. 11
The search strategy combined MeSH terms “thyroidectomy,” “thyroid nodules,” or “quality of life” with keyword terms “thyroid lobectomy,” “hemithyroidectomy,” “partial thyroidectomy,” “total thyroidectomy,” “thyroid cancer,” “cancer of the thyroid,” “extent of thyroidectomy,” “thyroid carcinoma,” “QoL,” “health-related quality of life,” “HRQOL,” “health status,” and “well-being.” The full search strategy is provided as Supplementary Data S1. The reference sections of all identified publications were hand searched for additional relevant publications. The search yielded 1402 articles.
Selection criteria
A list of inclusion and exclusion criteria for clinically relevant published peer-review articles was established during a consensus meeting with the senior and all authors involved (Table 1). The initial 1402 articles were uploaded into Covidence™ (Melbourne, Australia) and screened using the described inclusion and exclusion criteria by six authors (K.B., P.A., H.A., N.M.M., D.M.E., and S.C.P.). Based on titles and abstracts, 144 articles met our criteria. The full-text articles were obtained and reviewed by four authors (K.B., P.A., H.A., and N.M.M.). A list of the excluded full-text articles reviewed and their reason for exclusion are provided as Supplementary Data S2. Sixteen articles ultimately fulfilled our selection criteria and were included in this review.
Inclusion and Exclusion Criteria
Studies were included if a small portion of the population had higher risk thyroid cancer. In all but three studies, authors' conclusions reported refer only to the subpopulation of patients with low-risk thyroid cancer. In studies where the subpopulation of thyroid patients with low-risk thyroid cancer was not specified, patients receiving RAI therapy were assumed to be higher risk and patients not receiving RAI therapy were assumed to be low risk, unless tumor stage or histology type was identified. Therefore, studies were included if the population of interest not receiving RAI was >50%.
ATA, American Thyroid Association; HRQOL, health-related quality of life; HT, hemithyroidectomy; RAI, radioactive iodine; TT, total thyroidectomy.
The entire article selection was conducted in duplicates and each article was screened and reviewed by two of the four authors independently to reduce error and biases. If a discrepancy was found between two authors, the decision of whether to include or exclude the article was made by the senior authors (D.M.E. and S.C.P.).
Data collection and synthesis
A list of variables relevant to the objective was generated by the study team and considered variables in previously published systematic reviews. 11 After organizing variables, multiple rounds of data extraction were performed by four authors in duplicates (K.B., P.A., H.A., and N.M.M.). Extraction variables were revised by the study team as needed and the reliability of extraction was ensured among all authors. Discrepancies were resolved by consensus; therefore, a kappa statistic was not computed. The final list of variables is included in Supplementary Data S3.
Quality assessment
The methodological quality of each article was independently assessed by four authors in duplicates (K.B., P.A., H.A., and N.M.M.) using the National Heart, Lung, and Blood Institute's (NHLBI) Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. 14 This quality assessment tool was developed to help reviewers evaluate the internal validity of a study. It includes 14 questions about study population, participation selection, sample size, timing of exposure, study time frame, outcome measures, and more. Studies earned one point for an answer of “Yes” for each NHLBI criterion. The highest possible score was 14 points. Quality was rated as poor (score 0–4), fair (score 5–10), or good (score 11–14) based on prior publications. 15
Results
Study characteristics
Study selection is presented in Figure 1. Sixteen studies performed in seven countries and published between January 2011 and December 2022 met the inclusion criteria and were included in this review (Table 2). 16 –31 Five (31.3%) were prospective cohorts 16,19,21,23,24,30 and 11 (68.8%) studies were retrospective cohort studies. 17,18,22,25 –28 Six HRQOL measurement tools were used in the studies, of which four (66.7%) are validated. The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30) and Thyroid Cancer-Specific Quality of Life questionnaire (THYCA-QOL) were most frequently utilized. Of the 4957 patients with low-risk DTC included in this review, 840 (16.9%) received radioactive iodine (RAI). Patients were treated with RAI after TT in seven studies. 16 –19,22,24,30 Details about study design, country, and patient population are in Table 2.
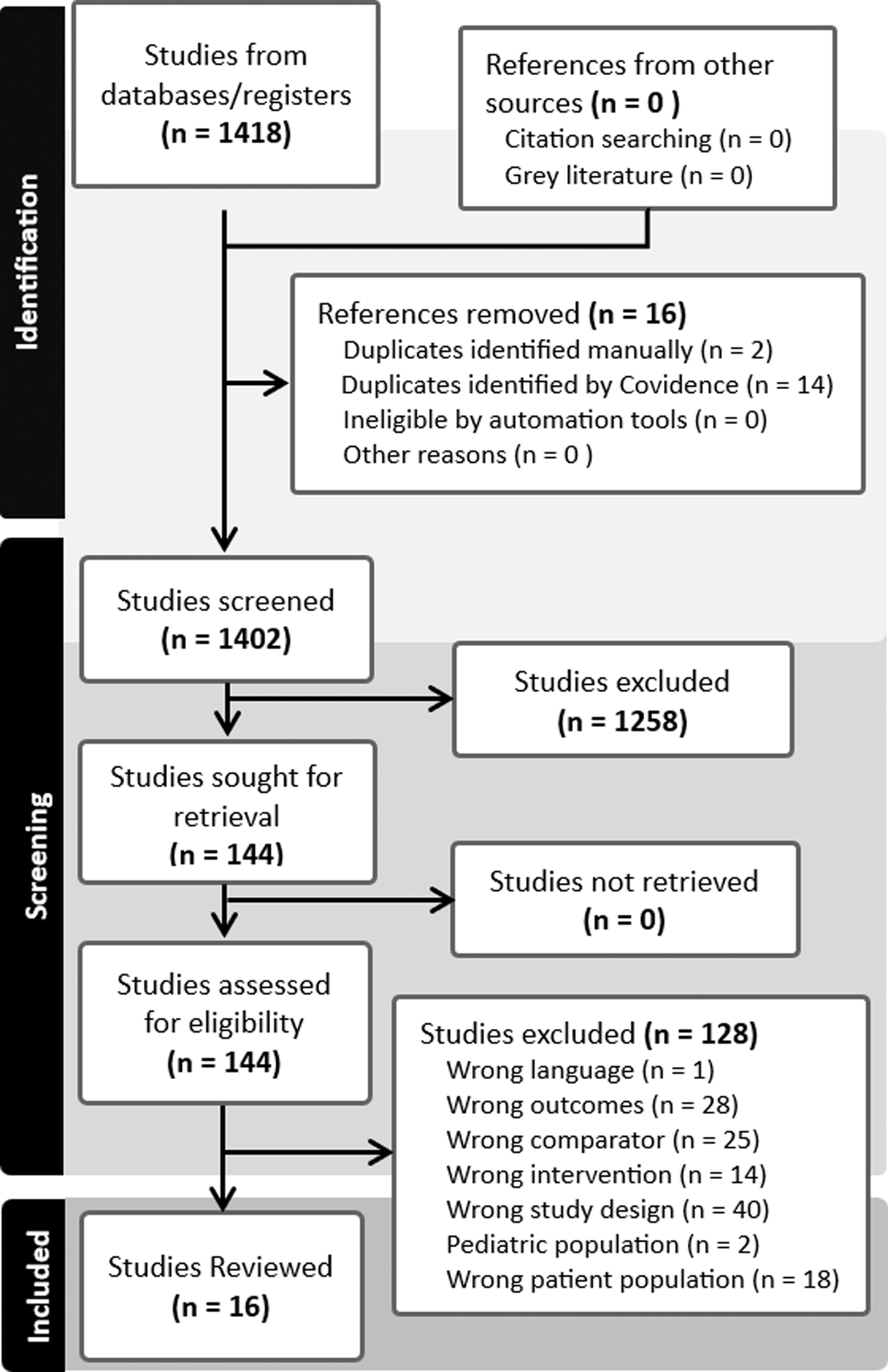
PRISMA flowchart of study search and selection pathway. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Studies Included in the Systematic Review Listed by Study Design and Year of Publication
(1) Patients diagnosed with non-DTC, intermediate or high-risk DTC, or patients undergoing active surveillance or remote access surgery as management were excluded from patient totals. (2) Study quality was determined with the NHLBI assessment tool.
Indicates studies where specific conclusions for patients with low-risk thyroid cancer were not available.
Studies have overlapping populations.
The bold refers to statistically significant findings overall for HT.
The italics refer to significant only is specific domains or procedure other than HT.
AJCC, American Joint Committee Cancer; CND, central neck dissection; DTC, differentiated thyroid cancer; EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire; EORTC QLQ-THY34, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire for Head and Neck cancer; f/u, follow-up; KT-QOL, Korean Thyroid-Specific Quality of Life Questionnaire for Thyroid Cancer Patients; LT4, levothyroxine; MI-FTC, minimally invasive follicular thyroid carcinoma; NHLBI, National Heart, Lung, and Blood Institute; PSM, propensity score matching; PTMC, papillary thyroid microcarcinoma; SF-36, 36-Item Short Form Health Survey questionnaire; THYCA-QOL, Thyroid Cancer-Specific Quality of Life questionnaire; TSH, thyrotropin.
Quality assessment
Utilization of the NHLBI assessment tool revealed that all but two studies included in this review had a good quality rating. 27,28 The article with the highest quality score concluded that HT had better quality of life compared only with TT with central neck dissection (CND) at a mean follow-up of ∼64 months. 20 A summary of the quality scores and ratings is located in Table 2. The details of the quality assessment of each study are provided in Supplementary Data S4.
Patient characteristics
A total of 4957 patients met the inclusion criteria; 77.6% (n = 3846) were female with an average age of 46.6 ± 4.5 years. Overall, 1306 patients (26.6%) underwent a TT without CND, 965 patients (19.5%) underwent a TT with CND, 626 patients (15.0%) underwent a TT without specifying CND, 948 patients (19.1%) underwent HT without CND, 367 patients (7.4%) underwent HT with CND, and 745 patients (12.6%) underwent HT without specifying CND.
HRQOL: comparison of TT versus HT
Six of 16 (37.5%) studies reported that HT led to better HRQOL than TT, 16 –21,23,25,29,31 while 2 (12.5%) reported that HT led to better HRQOL only compared with TT with CND, but not TT alone, 16,25 and 2 (12.5%) concluded that HT had better HRQOL in the short term, but no differences existed in HRQOL 6 months or greater postoperatively. 30 Two (12.5%) additional studies reported that HT led to better HRQOL only on certain domains or only before propensity score matching. 17,20 Four (25%) studies reported no difference in HRQOL between TT and HT. 22,24,26 –28 No study reported better HRQOL after TT.
Central neck dissection
Of the six studies where patients underwent CND, 16,17,22,24,26,28 two (33.3%) showed that TT with CND led to the worst HRQOL compared with TT alone and HT with or without CND. 18,20 One (16.7%) study concluded that TT with CND had worse HRQOL than HT with CND; 16 and one (16.7%) concluded that TT with CND had worse HRQOL compared with either TT or HT alone. 17 Two (33.3%) studies concluded that the increased extent of surgery needed for a CND did not impact HRQOL. 22,28
Study design
When considering study design, two of the five (40%) prospective cohort studies concluded that HT led to better HRQOL compared with TT, 19,23 while two (40%) reported better HRQOL with HT at 1 and/or 3 months postoperatively, but no differences in HRQOL were seen at 6–12 months. 16,30 Of the 11 retrospective cohort studies, 4 (36.4%) concluded that HT led to better HRQOL compared with TT. 18,21,25,31 Three (27.3%) studies concluded that there were no differences in HRQOL between TT and HT. 22,27,28
HRQOL measurement tools
The included studies measured HRQOL using both general instruments and thyroid-specific instruments, with mixed conclusions reflected in both categories of instruments. Among studies using general instruments such as the 36-Item Short Form Health Survey questionnaire (SF-36), four concluded better HRQOL with HT compared with TT, 17,21,25,29 while one study concluded no difference in HRQOL between the two procedures. 24 Among those that measured HRQOL with the EORTC QLQ-C30, two concluded better HRQOL after HT, 17,19 while four studies concluded no difference. 22,26,27,30
When examining the thyroid-specific instruments used to measure HRQOL, six studies that measured HRQOL using THYCA-QOL showed that three concluded better HRQOL after HT, 20,21,25 while three found no difference (Table 3). 26,28,30 Two prospective cohort studies using the Korean Thyroid-Specific Quality of Life Questionnaire for Thyroid Cancer Patients (KT-QOL) both concluded better HRQOL after HT (Table 3). 16,23 Two cross-sectional studies using the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire (QLQ) for thyroid cancer (THY34) 22 and EORTC QLQ for Head and Neck cancer (H&N43) 28 both concluded that there was no difference in HRQOL between the two surgeries. One study using a self-developed study-specific thyroid cancer questionnaire 18 and one study using ThyPRO 31 both reported better HRQOL with HT.
Differences in Health-Related Quality-of-Life Domains After Hemi- and Total Thyroidectomy for Three Instruments
 = better after HT (vs. TT), p < 0.05;
= better after HT (vs. TT), p < 0.05;  = better after HT (vs. TT), p ≥ 0.05 and p ≤ 0.10;
= better after HT (vs. TT), p ≥ 0.05 and p ≤ 0.10;  = better after TT (vs. HT), p < 0.05;
= better after TT (vs. HT), p < 0.05;  = no difference (HT vs. TT). (1) Luddy et al. reported no overall difference in HRQOL scores for patients who underwent HT vs. TT using the SF-36, but did not report individual domain scores; however, the PCS was reported to be significantly better for TT and the MCS significantly better for HT. (2) Table shows significant differences found at any point during a study. (3) The range of p-values was used because many of the studies were not powered to detect differences in domains.
= no difference (HT vs. TT). (1) Luddy et al. reported no overall difference in HRQOL scores for patients who underwent HT vs. TT using the SF-36, but did not report individual domain scores; however, the PCS was reported to be significantly better for TT and the MCS significantly better for HT. (2) Table shows significant differences found at any point during a study. (3) The range of p-values was used because many of the studies were not powered to detect differences in domains.
Indicates domain found to be significantly different across multiple studies and/or HRQOL measures comparing HT vs. TT.
MCS, mental component summary; PCS, physical component summary.
HRQOL domains
Several studies reported that specific HRQOL domains were better after either HT or TT, although more studies found HT to be superior when examining domains. 17,20 –22,24 –26,29,30 A summary of findings related to HRQOL domains is located in Tables 3 and 4. Of the five studies that used the EORTC QLQ-C30, one (20%) did not report domain-related information 24 and three (60%) found HT to be superior to TT in the global quality of life domain (two with p < 0.05 and one with p > 0.05, but <0.10) (Table 4). 17,26,30
Differences in EORTC-QLQ-C30 Domains After Hemi- and Total Thyroidectomy
 = better after HT (vs. TT), p < 0.05;
= better after HT (vs. TT), p < 0.05;  = better after HT (vs. TT), p ≥ 0.05 and p ≤ 0.10;
= better after HT (vs. TT), p ≥ 0.05 and p ≤ 0.10;  = better after TT (vs. HT), p < 0.05;
= better after TT (vs. HT), p < 0.05;  = no difference (HT vs. TT). (1) Li et al. also used the EORTC QLQ-C30 and reported overall better HRQOL scores for patients who underwent HT compared with TT but did not report differences by domain. (2) Table shows significant differences found at any point during a study. (3) The range of p-values was used because many of the studies were not powered to detect differences in domains.
= no difference (HT vs. TT). (1) Li et al. also used the EORTC QLQ-C30 and reported overall better HRQOL scores for patients who underwent HT compared with TT but did not report differences by domain. (2) Table shows significant differences found at any point during a study. (3) The range of p-values was used because many of the studies were not powered to detect differences in domains.
Indicates domain found to be significantly different across multiple studies and/or HRQOL measures comparing HT vs. TT; QOL, quality of life.
Chen et al. also reported better scores for HT in the domains of physical function, role function, emotional function, social function, fatigue, pain, appetite loss, and financial difficulties before 6 months postoperatively. 30 Two (40%) of these studies found less sleep disturbance after TT. 21,27 One (20%) study that used the EORTC QLQ-C30 also used the EORTC QLQ-THY34and found HT to have better HRQOL in the domains of fear, social support, body image, and impact on job or education. 22
Of the four studies that used the SF-36 to measure HRQOL, at least two (50%) studies found clinically moderate differences in the following domains favoring HT: role limits due to physical health, vitality, social-function, role limits due to emotional health, the physical component summary scores, and mental component summary (Table 3). 21,24,25,29
Overall, five studies used the THYCA-QOL. 20,21,25,26,30 At least two (33.3%) of these studies reported that the neuromuscular (leg cramps, physically slowed down, and pain in muscles/joint), voice (weak voice and hoarseness), and/or psychological (anxiety, restlessness, palpitations, and abrupt tiredness) domains were better after HT (Table 3). 21,30 Two (33.3%) studies used the KT-QOL, which was developed based on THYCA-QOL and reported better HRQOL scores following HT compared with TT overall as well as in the physical and social domains (Table 3). 16,23
Time from surgery
The studies included in this review varied widely with respect to the timing of HRQOL measurement, ranging from 2 weeks to 15 years postoperatively. In studies with a retrospective design, three of the three (100%) studies that predominantly measured outcomes <1 year postoperatively found that HT resulted in improved HRQOL. 22,23,30 Meanwhile, four of the seven (57.1%) retrospective studies that measured outcomes >1 year postoperatively found no difference between the two procedures, while two (28.6%) found that HT had better HRQOL only compared with TT with a CND, 16,25 and one (14.3%) found HT to have better HRQOL regardless of CND being performed. 26
In the five studies with a prospective design, none measured HRQOL >1 year after surgery. Of these, two (40%) reported that patients who underwent HT had better HRQOL scores throughout the study, 16,23 while two (40%) found better HRQOL after HT only in the early postoperative period measured at 1 and 3 months. 30 However, in the latter two studies, there were no differences in HRQOL seen at 6 months or later compared with patients who underwent TT. 30 Another study graphically showed similar results favoring HT with measurement of HRQOL at 2 weeks, but again reported no difference in HRQOL between HT and TT at 1 year. 31
Clinical factors affecting HRQOL
Several studies examined additional patient and clinical factors such as surgical complications that affected HRQOL (Table 2). While surgical complications were reported in 8 of the 16 (50%) studies included in this review, 19 –22,24,25,29,30 only 1 (12.5%) prospective cohort study examined the influence of complications on HRQOL. 19 In this study, recurrent laryngeal nerve injury was an independent risk factor for decreased HRQOL after TT. 19 Overall, transient and permanent nerve injury and hypoparathyroidism were found to be more prevalent after TT 24,25,29,30 and CND. 21 Seroma requiring repeat aspiration and wound infection were also more prevalent after TT. 29 Thyroid tumor size was examined and not found to affect HRQOL. 18
Discussion
This systematic review provides a critically needed update of the literature comparing HRQOL for survivors of predominantly low-risk DTC after TT compared with HT. Currently, no high-quality, prospective, randomized clinical trials comparing TT with HT have been performed and results are heterogenous across studies included in our analysis. Data from the 16 studies included suggest that increased extent of surgery with TT, particularly when performed with a CND, can result in reduced HRQOL compared with HT. One striking finding was the lack of data from the United States, South America, and other regions of the world. Notably, no study demonstrated worse quality of life for the patients who underwent HT compared with TT.
This systematic review differs from one of the most commonly cited large systematic reviews of HRQOL in thyroid cancer. 11 The current review focused specifically on differences in HRQOL for survivors of low-risk DTC after TT compared with HT. Husson et al. broadly examined HRQOL of patients with thyroid cancer and neither restricted to analyzing the low-risk, differentiated subtypes of thyroid cancer nor to the extent of surgery. 11 Nevertheless, the prior review did include three studies investigating HRQOL of patients with thyroid cancer that examined the effects of surgery. 11 In line with the findings of this systematic review, Husson et al. concluded that surgery for thyroid cancer leads to worse HRQOL compared with the general population, with the size of the effect of HRQOL depending on the type of surgery. 11
Examining HRQOL is important because TT offers no survival or locoregional control benefit for low-risk DTC compared with HT and yet is associated with increased risks such as recurrent laryngeal nerve injury leading to vocal fold paralysis, temporary or permanent hypoparathyroidism, and need for lifelong thyroid hormone supplementation. 6 These treatment- and follow-up-related effects of TT were found to adversely impact HRQOL in at least two studies in this review, although the interplay of such factors with a patient's fear of cancer recurrence and desire for “peace of mind” in determining HRQOL is unknown. 32
Cancer treatment should aim not only to increase survival but also to preserve HRQOL among survivors. As the incidence of thyroid cancer is increasing and the long-term survival—which approaches 100% in patients with low-risk DTC—remains stable, there will be a growing number of thyroid cancer survivors. 12 Optimizing HRQOL in this population is of great importance, especially when one considers the deleterious effects of negative HRQOL on one's emotional, physical, and social functioning. Chen et al. reported better quality of life after HT compared with TT for most of the functioning and symptom domains, while other studies that used the EORTC-QLQ-C30 reported no difference. 30 This finding was most likely related to sample size as Chen et al. had significantly more participants compared with the other studies. 30
While the findings of this review suggest that HT may offer better HRQOL compared with TT for patients with low-risk DTC, we observed significant heterogeneity in the study designs and HRQOL tools used. When comparing the results of both general instruments and thyroid-specific instruments, the SF-36 was the most likely general measure to show HRQOL difference, while there was no thyroid-specific measure that favored the others. This finding points to the critical need for a prospective randomized study comparing the effect of the extent of surgery on HRQOL in patients with low-risk DTC.
Limitations to this review that should be considered include the large variation in aims, study design, clinical characteristics, sample sizes, and instruments used to measure HRQOL, which prohibited our ability to perform a meta-analysis. Due to this known heterogeneity, a narrative review was planned from the beginning. In addition, despite many studies having a prospective design, the lack of a randomized design with respect to the extent of surgery means that selection bias may have affected the quality-of-life outcomes measured. Patients with less severe diseases may have received less aggressive treatment and, as a result, reported a higher quality of life. Another limitation is the inability to determine whether statistically significant differences in HRQOL were associated with clinically meaningful outcomes.
To narrow the focus of this review, studies that utilized other surgical and nonsurgical techniques such as active surveillance, transoral, robotic, and radiofrequency were excluded if they did not report outcomes of open TT compared with HT. As the search strategy did not include RAI, a conclusion could not be drawn about HRQOL related to RAI. Studies that only examined other patient-reported outcomes such as voice or swallow-related quality of life were also excluded.
Many studies included were also not powered to detect differences between two patient groups or surgical approaches, and so, their conclusions should be interpreted with this limitation in mind. In three studies, the authors did not report enough details to determine the risk level or report subanalyses based on risk level, 17,28,31 which made it difficult to draw conclusions only about patients with low-risk DTC. Data were also collected from patients who received treatment before and after the 2015 ATA guideline changes and at different time points postoperatively, which limits the ability to draw overarching conclusions. Finally, the surgeries were performed in multiple countries with differences in their patient populations and varying cultural conceptualizations of quality of life.
While the NHLBI quality assessment tool has been used to assess the quality of qualitative studies in several systematic reviews, it does not have prespecified parameters that allow for judgments of study quality. Therefore, the quality assessment criteria for “good,” “fair,” and “poor” vary between systematic reviews. This systematic review was not registered with PROSPERO.
In conclusion, many studies in this systematic review reported better HRQOL after HT compared with TT, particularly when measured early after surgery and when CND was performed. These findings are important because although oncologic outcomes are similar for both procedures, the quality of life among survivors may be different. While higher quality data in the form of large-scale, long-term randomized control trials are needed to draw firm conclusions, patients with low-risk DTC should be aware of potential differences in expected HRQOL outcomes. Future studies should strive to standardize measurement and utilize thyroid cancer-specific instruments to address the current diversity across the small patient populations as well as the heterogeneity of QOL measures.
Footnotes
Acknowledgment
The authors would like to thank Mary E. Hitchcock, MA, MLIS, for her assistance with the literature search and Covidence access.
Authors' Contributions
K.B.: methodology, screening, full-text review, extraction, analysis, and writing. P.A.: methodology, screening, full-text review, extraction, analysis, and editing. H.A.: methodology, screening, full-text review, extraction, and editing. N.M.M.: screening, full-text review, extraction, and editing. D.M.E.: screening and review. H.U.: review and editing. S.C.P.: conceptualization, methodology, screening, analysis, supervision, and writing.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Dr. Pitt receives funding from the National Institutes of Health/National Cancer Institute (K08CA230204; R03CA283105) and the Society of University Surgeons.
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3
Supplementary Data S4