
Abstract
Background:
Nasolacrimal duct obstruction (NLDO) is an adverse effect of high dose radioactive iodine (RAI) therapy for thyroid carcinoma. There are currently no established preventive measures. This study assesses whether preservative free artificial tears (PFATs) can decrease the 131I sodium iodide (131I) activity in the tears of patients following RAI therapy for thyroid carcinoma, and potentially serve as a preventive measure for RAI-associated NLDO.
Methods:
This non-randomized prospective pilot clinical trial recruited contact-lens wearing patients undergoing RAI therapy for thyroid cancer to self-administer PFATs into the right eye for four days starting on the day of RAI ingestion. Left eyes were the controls. While wearing contacts, patients self-administered PFATs per the following—Day 1: every 15 minutes for 2 hours, then every 30 minutes until bedtime, day 2: every hour for at least 12 hours, day 3: four times a day, and day 4: two times a day. Contact lenses were changed daily, and all lenses were collected one week later. Levels of 131I activity were measured by a well counter, decay-corrected, and converted to units of becquerel. Statistical analyses were performed to compare the 131I activities of the experimental and control eyes.
Results:
Sixteen eyes of eight patients treated with an average of 145.7 mCi (range 108–159) of 131I for papillary thyroid cancer were included. On day 1, artificial tears decreased the geometric mean 131I activity by 26% in the experimental eyes (p = 0.008). Artificial tears also decreased the geometric mean area under the curve over four days by 23% (p = 0.002).
Conclusions:
131I is present in the tears following RAI therapy for thyroid carcinoma. Frequent PFATs starting on the day of RAI ingestion may decrease the level of 131I in the tears. This finding could have implications for lowering the risk of NLDO. Future multi-center clinical trials are needed to determine whether the use of artificial tears after RAI therapy may decrease the risk of NLDO.
Clinical Trial Registration:
NCT04327999
Introduction
Radioactive iodine (RAI) therapy with 131I sodium iodide (131I) is commonly administered for the treatment of thyroid carcinoma. 1 –6 A well-established adverse effect of RAI therapy is the development of nasolacrimal duct obstruction (NLDO), which has a higher incidence in patients treated with at least 150 mCi of 131I. 7 –13 The incidence of RAI-associated NLDO ranges from 2% to 7%. 8,9,13 –15
Symptoms include epiphora that can be visually impactful, mucoid discharge, and even dacryocystitis that can lead to orbital cellulitis. 10,11,14,16 Dacryocystorhinostomy surgery is the treatment for NLDO and consists of creating an ostomy from the lacrimal sac into the nose, thereby bypassing the obstruction.
The precise pathogenesis of RAI-associated NLDO is not entirely understood. It is unclear whether injury to the lacrimal drainage system is secondary to exposure from the tears or the direct uptake of RAI from the blood by sodium-iodide symporters (NIS) located in the epithelial cells of the nasolacrimal system. 13 Histopathologic studies have shown expression of NIS in the lacrimal sac and nasolacrimal duct of human tissue biopsies, corresponding to areas of obstruction. 17 Interestingly, two prior cases found RAI in the tears of patients following systemic therapy, as detected via Schirmer test strips and contact lenses. 18,19 If RAI is detectable in the tears, it is plausible that downstream exposure to the lacrimal sac and nasolacrimal duct can lead to fibrosis and obstruction.
There are currently no prophylactic measures or recommended guidelines to prevent RAI-associated NLDO. This study explores whether administration of preservative free artificial tears (PFATs) can decrease the 131I activity in the tears of patients following RAI therapy and thus potentially decrease the risk of NLDO.
Materials and Methods
This study is a prospective pilot clinical trial performed at Vanderbilt University Medical Center and registered under
Patients scheduled for at least 100 mCi of systemic 131I therapy for the treatment of thyroid cancer and who regularly wear bilateral disposable contact lenses were eligible for recruitment. The study's dose cutoff for systemic RAI therapy was initially 150 mCi, which was later lowered to 100 mCi in April 2021 to increase patient recruitment.
Patients were excluded if they had any of the following: use of eye drops other than artificial tears, history of tear duct or lacrimal gland injury, history of known lacrimal drainage diseases including canaliculitis or dacryocystitis, prior RAI therapy or chemotherapy, or history of sarcoidosis, granulomatosis with polyangiitis, or leukemia.
Patients who were scheduled for RAI therapy for thyroid carcinoma from October 1, 2020, to July 13, 2022 were contacted by telephone to screen for recruitment. Sample size was determined by the total number of eligible patients recruited during this period. The patients' electronic medical records were reviewed before their scheduled RAI treatment to ensure that at least 100 mCi of 131I was ordered by Nuclear Medicine. This dose was pre-determined by the Nuclear Medicine department. This study made no recommendations on the administered dose of RAI.
Recruited patients were provided with a gift card and at least four days-worth of bilateral contact lenses of their latest prescriptions. Patients were assessed in person by an attending oculoplastic physician before RAI therapy. Assessment of baseline vision, pupils, intraocular pressure, the anterior segment with fluorescein application, and irrigation of both nasolacrimal ducts were performed for each patient.
Due to radioactive risks to others, all patients were required by Nuclear Medicine to self-isolate for one week following RAI therapy. Recruited patients were instructed to wear bilateral contact lenses for at least 12 hours a day for 4 days, starting on the morning of their RAI administration GenTeal® brand PFATs were provided for the patients to be administered only into the right eye (OD) in the following regimen—Day 1 (the day of RAI ingestion): every 15 minutes for 2 hours, then every 30 minutes until bedtime, day 2: every 1 hour for at least 12 hours, day 3: four times a day (QID), and day 4: two times a day (BID).
Patients were instructed to not administer any eye drops into the left eye (OS) during this study period. Patients were thoroughly counseled on the importance of compliance and were given a document with checkboxes to track each time they instilled drops.
At the end of each night at home, patients stored the right and left contact lenses in separate wells of a provided plastic contact lens case. To prevent cross-contamination between the right and left contacts, patients were instructed to first remove and store the right contact lens, rinse the hands with water, pat dry, and then remove and store the left contact lens.
Patients were instructed to fill each of the contact lens wells with an entire vial of GenTeal PFATs to standardize the volume of fluid used for contact lens storage. This contact lens storage regimen was repeated for the three latter days in new separate contact lens cases.
At routine post-RAI week 1 appointment for nuclear medicine imaging, patients brought all contact lenses for collection and measurement of 131I activities by the study's nuclear medicine physicist. Each contact lens and its associated fluid were measured by a PerkinElmer Packard Cobra II (PerkinElmer, Akron, OH) automatic well counter. A counting window was set up for counting 131I at 260 to 470 keV. Each contact lens for each eye and day was placed in a vial and the associated solution was pipetted into the vials, then each vial was counted sequentially. The counts were then corrected for background and converted to becquerel using an established efficiency for the counting window and well counter used. Each measured activity was then decay corrected to the day each lens was removed.
The primary outcome measure was the measured 131I activity of each contact lens for each patient. The secondary outcome measure was the area under the curve (AUC) of all four days for each patient, which was calculated as the sum of the four trapezoid areas under the 131I exposure values. The primary and secondary outcome measures of the experimental and control groups were compared to see whether PFATs lowered the 131I activity in the tears.
To meet the normality assumption, 131I activities and AUCs were logarithmically transformed to obtain geometric mean 131I activities of each day and geometric mean AUCs. The Shapiro-Wilk test was used to evaluate the normal assumption for logarithmically transformed AUCs (log-AUCs). The confidence intervals [CI] of the AUCs were constructed for the right experimental eyes and left control eyes, assuming normality for log-AUCs, which were compared between the two groups using paired t-tests. Statistical analyses were conducted using R version 4.1.2 (R Project for Statistical Computing). Two-sided p < 0.05 was considered statistically significant.
Vanderbilt University Medical Center Institutional Review Board (IRB)/Ethics Committee approval was obtained (#NICHOC705032021103855). The study adhered to the ethical principles outlined in the Declaration of Helsinki and was HIPAA compliant. Written informed consent was obtained from all enrolled patients.
Results
Characteristics of the recruited patients
From October 1, 2020, to July 13, 2022, 108 patients receiving RAI therapy for thyroid cancer were contacted to see whether they wore bilateral contact lenses. Fifteen of these patients reported wearing contact lenses; 9 of these 15 patients agreed to participate in the study. One patient deviated from protocol and was excluded from the dataset. Thus, 16 eyes of 8 patients were included in this study (Fig. 1). Table 1 displays the characteristics of the included patients. All patients were female, except for patient 7.

Flow diagram displaying the study's recruitment process. One hundred eight potentially eligible patients receiving RAI therapy were contacted by phone. Of these patients, 15 were eligible for recruitment and reported contact lens use. Nine patients consented to the study. One patient was excluded from the study due to deviation from the study protocol. Thus, eight patients were included and analyzed in the study. RAI, radioactive iodine.
Demographic and Clinical Characteristics of the Recruited Patients
BMI, body mass index; DES, dry eye syndrome; L, left; N/A, not available; NLD, nasolacrimal duct; OD, right eye; OS, left eye; OU, both eyes; PEE, punctate epithelial erosions; R, right; RAI, radioactive iodine; RD, retinal detachment.
The average age of the patients was 47 years old (range 25–65). All patients wore disposable soft contact lenses either daily or monthly. The average administered dose of 131I was 145.7 mCi (range 108–159). Patient 7 had a history of a retinal detachment OD, and patient 9 had a history of dry eyes. No other patients reported prior ocular history. Other than thyroid carcinoma, diabetes, and hypertension, patients had no other medical history.
No patients had a history of receiving RAI therapy in the past. Before RAI therapy, all patients underwent a low iodine diet for one week. All patients received either two injections of recombinant human thyrotropin or thyroid hormone withdrawal. Thyroid hormone withdrawal was preferred when there was a suspicion for distant metastasis. Vision ranged from 20/20 to 20/30, with normal pupillary responses to light. Intraocular pressures ranged from 14 to 22. Patients 1, 2, 6, and 8 had mild dry eye on exam.
All patients had normal-sized and patent upper and lower puncta, except for patient 6 who had patent but small-sized puncta. All patients had patent lacrimal duct systems, except for patient 2 who had a fully obstructed right nasolacrimal duct and a partially obstructed left nasolacrimal duct. She reported no prior or current symptoms consistent with NLDO.
Each patient reported compliance to administering PFATs to the right eye. None of the patients administered any eye drops into the left eye. No adverse events occurred.
Levels of 131I activity measured from the tears collected from contact lenses
For each patient, maximal 131I activity was detected in the left control contact lens on day 1, with an average of 6096.7 Bq (range 1246.4–14475.5 Bq, Table 2). On day 1, experimental eyes had a significantly lower geometric mean 131I activity of 3437.4 Bq [CI 1774.4–6659] than controls, which had a geometric mean 131I activity of 4635.7 Bq [CI 2313.4–9289.1] (p = 0.008, Fig. 2).
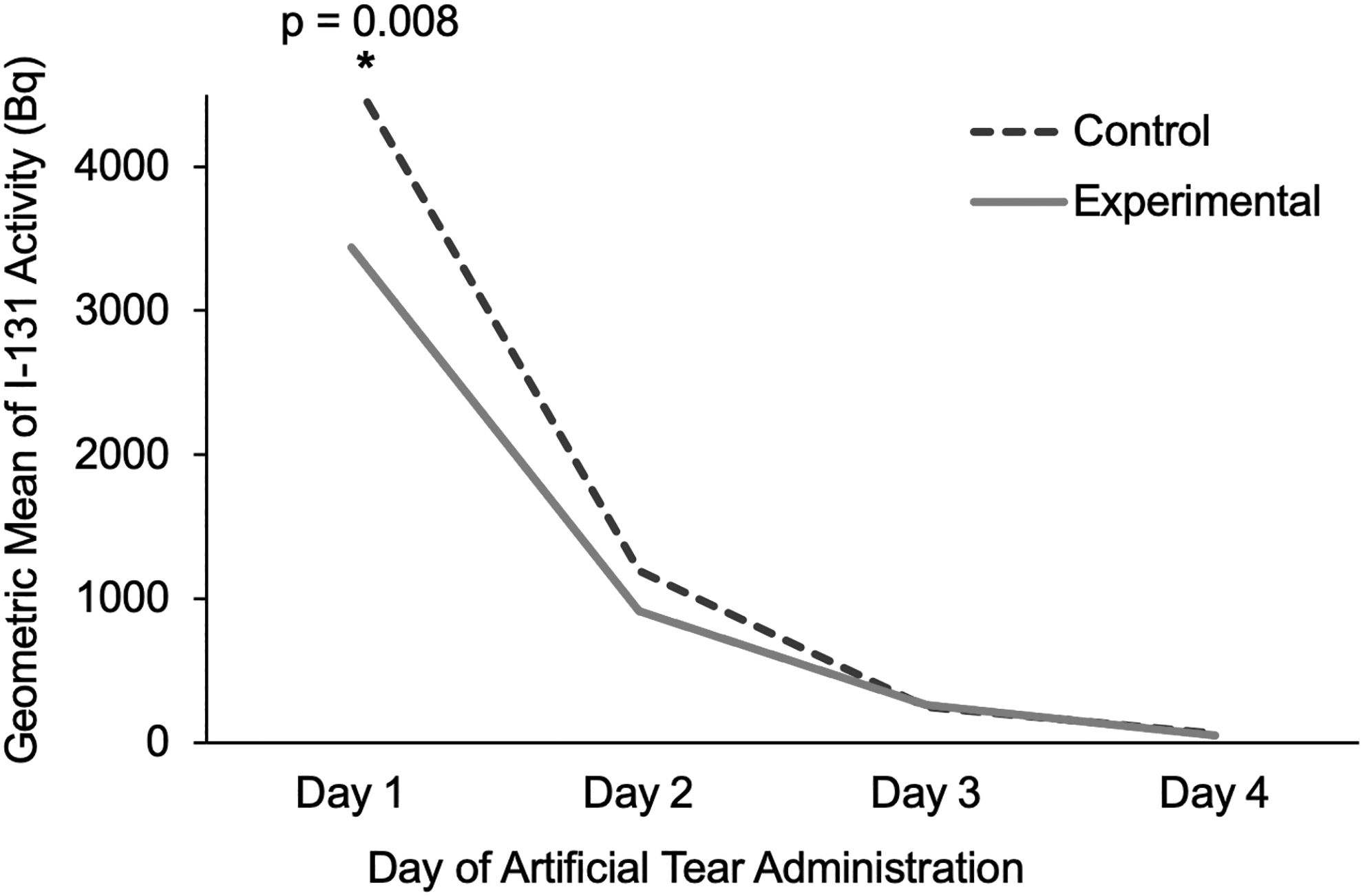
The geometric mean 131I sodium iodide (131I) activities of all patients' right experimental and left control contact lenses over days 1–4. Day 1 represents the day of RAI therapy ingestion. On day 1, the geometric mean 131I activity of experimental eyes (3437.4 Bq) was significantly lower by 26% than that of the control eyes (4635.7 Bq, p = 0.008).
131I Sodium Iodide (131I) Activities as Detected in the Left Experimental and Right Control Contact Lenses of the Recruited Patients
Percentage in parentheses represents the percentage of the maximal 131I activity for each patient. A percentage of the maximal activity of 131I for each patient was calculated for all the contact lenses of each patient. The maximal 131I activity for each patient was the left control contact lens on day 1. Day 1 represents the day of RAI therapy ingestion.
Based on these values, artificial tears decreased the geometric mean 131I activity on day 1 by 26%. On days 2–4, there were no differences in geometric mean 131I activities between the experimental and control eyes (p > 0.1). Finally, the geometric mean AUCs for the experimental lenses were significantly lower at 2975.7 Bq-days [CI 1579–5609] compared with the controls with 3860.8 Bq-days [CI 1957–7618] (p = 0.002). Artificial tears decreased the geometric mean AUC by 23% in experimental eyes.
Discussion
The pathophysiology of RAI is not entirely understood and may involve the active uptake of RAI from the blood via the NIS located in the epithelium of the lacrimal sac and nasolacrimal duct. Another possibility is that prolonged RAI exposure from the tears to the epithelial cells of the lacrimal sac and nasolacrimal duct may lead to inflammation, fibrosis, and ultimately obstruction.
The presence of RAI in the tears has previously only been documented in two patients treated with RAI therapy; tears were collected via Schirmer test strips in one report and via contact lenses in the other. 18,19 Our study corroborates the presence of 131I activity in the tears of all eight patients following RAI ingestion, as collected via contact lenses.
Instillation of PFATs may not only dilute the amount of RAI in the tears, but may also encourage more frequent drainage of tears from the lacrimal sac and nasolacrimal duct, thus preventing stasis of RAI-containing tears within the nasolacrimal duct system. This benefit could occur whether the exposure comes from the patient's tears or from uptake directly from the blood into the lacrimal system.
While it would be challenging to decrease 131I concentration in the blood without compromising thyroid ablation, decreasing the level of RAI in the tears locally can potentially be done with PFATs without systemic consequences. PFATs have minimal adverse effects and do not contain iodide and thus should not be contributing to increased retention of RAI in the lacrimal drainage system.
In our study, artificial tears significantly decreased the geometric mean 131I activity on day 1 by 26% (p = 0.008). When comparing the raw data before logarithmic transformation, all experimental eyes had lower 131I activities compared with those of controls on day 1 (Table 2). Given that 131I activities in the tears are at their maximal on the day of RAI therapy, it is probable that the majority of RAI uptake by the nasolacrimal duct occurs on day 1.
Thus, a decrease in 131I activity on the day of systemic therapy via PFATs may be especially impactful. There were no differences in geometric mean 131I activities between the left and right eyes on days 2–4 (p > 0.1). This finding may be secondary to the less rigorous PFAT schedule during these days, especially on days 3 and 4 when tears were being given QID and BID, respectively.
In addition, there may have been small differences in 131I activity during days 2–4 that were difficult to show due to the low amounts of activity remaining and thus larger statistical uncertainty at those time points. Despite the non-significant differences in 131I activities between the experimental and control eyes on days 2–4, artificial tears still significantly decreased the overall geometric mean AUC over 4 days (p = 0.002). This finding is likely secondary to the significant difference in geometric mean 131I activity on day 1.
Meaningful decreases of 131I activity in the tears may require frequent PFAT administration of at least every 15–30 minutes as performed on day 1 in this study. Patients being treated with high-dose RAI therapy for thyroid carcinoma may consider self-administering PFATs every 15–30 minutes in both eyes starting on the day of RAI therapy for at least 24 hours to potentially decrease the level of 131I in the tears. As patients are required to self-isolate for one week following RAI therapy (to reduce the risk of radioactive exposure to others), such high frequency of PFAT administration may be achievable.
Strengths of this study include its prospective clinical trial design with an optimal control group—the fellow eye of the same patient. While the number of recruited patients was small, the study was intended to be a pilot clinical trial that demonstrated a proof of principle and could be used as a model for future clinical trials of larger scale.
Given that eight of the nine initially recruited patients adhered to the study protocol, it is feasible to apply this study design to future larger scale studies involving multi-center institutions. The study had inherent limitations. Compliance was one issue, but measures were taken to maximize it. Each patient was thoroughly counseled and given a document with checkboxes for each time they administered a drop of PFATs.
The use of contact lenses, while an imperfect modality of measuring 131I levels in the tear film, was the most practical way to minimize trips to clinic during the mandatory isolation period. Contact lenses may serve as an absorptive reservoir for RAI in the tears. Thus, it is possible that the use of contact lenses in our study underestimates the true dilutional effect of artificial tears on 131I in the tears.
Some of the patient characteristics varied. In terms of nasolacrimal patency, Patient 2 had a fully obstructed right nasolacrimal duct and partially obstructed left nasolacrimal duct. Interestingly, she was asymptomatic on both sides. As the focus of the paper was regarding 131I activity in the tear film, rather than clinical correlation to NLDO, we did not exclude patient 2 in the data. It is possible that a fully obstructed nasolacrimal duct may decrease the effect of PFAT dilution of 131I in the tear film, because the tears are stagnant and not draining through the nasolacrimal duct.
However, the patient's experimental right eye still demonstrated a decreased level of 131I activity compared with that of her control, especially on day 1 (Table 2). Lastly, the levels of maximal 131I activities varied per patient, ranging from 1246.4 to 14475.5 mCi (Table 2).
Such variation may be related to the administered dose of systemic therapy, variation in tear production and volume per patient, or amount of 131I uptake by residual thyroid tissue and/or sites of metastases. However, the impact of such variation in 131I levels is minimized due to each patient's contralateral eye serving as an optimal control.
Correlation of our findings to the lack of or development of NLDO is beyond the scope of this study. Given the reported low incidence of RAI-associated NLDO ranging from 2% to 7%, 8,9,13 –15 it may be difficult to compare the incidence of NLDO in the experimental versus control eyes of our eight patients. Future multi-center clinical trials are needed to determine whether the use of artificial tears after RAI therapy may reduce the risk of associated NLDO.
Footnotes
Acknowledgments
The contents of this manuscript have been presented at the American Society of Ophthalmic Plastic & Reconstructive Surgery (ASOPRS) Fall Meeting in 2022.
Authors' Contributions
I.T.L., J.V.G., L.A.B., A.C.J., B.B., F.C., L.A.M., and R.K.S.: Conceptualization, Methodology, Validation, Investigation, and Writing. X.J. and Q.C.: Formal analysis, Data curation.
Author Disclosure Statement
L.A.M. is an advisor for Horizon Therapeutics. No other conflicting relationship exists for other authors.
Funding Information
ASOPRS Foundation Grant, St Paul, MN; Vanderbilt Eye Institute Lefkovitz Award for Vision Research, Nashville, TN.