
Abstract
Background:
The current edition of the World Health Organization (WHO) classification of endocrine tumors introduced grading for follicular cell-derived thyroid cancer. Tumors with necrosis and/or high mitotic count but not fulfilling the Turin criteria for poorly differentiated carcinoma will be reclassified as differentiated high-grade thyroid carcinoma (DHGTC). However, the impact of this reclassification has not been evaluated. In this study, we performed a systematic review and meta-analysis to estimate the prevalence of this new entry across thyroid tumor subtypes.
Methods:
In this systematic review and meta-analysis, studies reporting data on necrosis and/or mitoses in well-differentiated thyroid carcinoma (WDTC) were used to estimate the prevalence of DHGTC. Heterogeneity and potential publication bias were also evaluated. Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were followed, and quality assessment was performed using a modification of the Newcastle–Ottawa scale. The study has been registered in the International Prospective Register of Systematic Reviews (PROSPERO, ID: CRD42022378716).
Results:
In clinically unselected patients, the prevalence of DHGTC in WDTC was 0.072 [95% confidence interval, CI, = 0.045–0.113]. The proportion of high-grade tumors greatly varied across growth patterns and subtypes. Overall, the prevalence of DHGTC was higher in follicular thyroid carcinoma (FTC; 0.146 [CI = 0.101–0.205]) than in papillary thyroid carcinoma (PTC; 0.059 [CI = 0.036–0.097]). Diffuse sclerosing, follicular, and classic subtype PTC had the lowest rates of high-grade features (i.e., 0.018 [CI = 0.004–0.084]; 0.036 [CI = 0.010–0.124]; and 0.042 [CI = 0.027–0.066], respectively), while a greater proportion of solid trabecular and histologically aggressive PTC could be reclassified as DHGTC (i.e., 0.154 [CI = 0.067–0.314] and 0.168 [CI = 0.108–0.252], respectively). Similar proportions were obtained for minimally and widely invasive FTC (i.e., 0.136 [CI = 0.058–0.287] and 0.152 [CI = 0.086–0.254], respectively). Finally, in a cohort of patients with poor prognosis (i.e., fatal cases, metastatic and radioiodine resistant tumors, cases with biochemical recurrence), the proportion of DHGTC was 0.287 [CI = 0.155–0.469].
Conclusions:
Following the current WHO indications, some tumors will be reclassified as DHGTC. The proportion of tumors with high-grade features is relevant in FTC, solid trabecular, and histologically aggressive PTC subtypes. A remarkable enrichment in DHGTC among patients with poor prognosis confirms the negative impact of high-grade features on outcome.
Introduction
The fifth edition of the World Health Organization (WHO) classification of endocrine tumors was released at the end of 2022. One of the major changes was the recognition of two groups of high-grade non-anaplastic follicular cell-derived carcinomas: poorly differentiated thyroid carcinoma (PDTC) and differentiated high-grade thyroid carcinoma (DHGTC). PDTC was already present in the previous editions, and the criteria for its diagnosis date back to 2007. 1 The Turin criteria establish that PDTC has a poorly differentiated growth pattern (i.e., solid, trabecular, insular, or a combination of them), absence of nuclear features of papillary carcinoma, and at least one of the following features: convoluted nuclei, mitotic count ≥3 per 10 high-power field (HPF; now defined as 2 mm2), and tumor necrosis.
DHGTC represents a new entry in the WHO classification scheme, introduced due to the prognostic relevance of grading for tumors that—while retaining architectural and cytological characteristics of well-differentiated tumors—have unfavorable prognosis. 2 DHGTC retains the architectural and cytological characteristics of well-differentiated tumors but present high-grade features defined by the presence of tumor necrosis or mitotic count ≥5 per 2 mm2. 3,4
The combined prevalence of PDTC and DHGTC ranges from 1% to 6.7% of all thyroid carcinoma. 3,5 Reports on necrosis and mitotic count in well-differentiated tumors have often been presented in aggregate with PDTC. Hence, the prevalence of high-grade features in well-differentiated carcinomas—and, consequently, the prevalence of DHGTC alone—is unclear. Similarly, the independent prognostic impact of necrosis and high mitotic count has been proven, but results were usually obtained in aggregate with PDTC defined according to the Turin consensus criteria. 6 Recently, Wong et al. observed a poorer disease-free and disease-specific survival in papillary thyroid carcinoma (PTC) with high-grade features compared with PDTC. 7
In this study, we performed a systematic review and meta-analysis to assess the prevalence of tumor necrosis and high mitotic count (i.e., ≥5 per 2 mm2/10 HPF) in well-differentiated thyroid carcinomas (WDTCs) to estimate the prevalence of this new entry in the current WHO classification scheme. We also performed a subgroup analysis by histological subtype.
Materials and Methods
Search strategy and selection criteria
A systematic search was performed on PubMed and Scopus databases following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
8
The strings used are provided in the Supplementary Data S1. The electronic search was performed on November 29, 2022, and updated on November 3, 2023. The following filters were applied: studies on humans, English-written articles, and publication date between January 1, 2003, and the day of search. Records identified from databases were merged and screened for duplicates using the automation tool available on Zotero 6 for Windows (
In particular, data on mitoses were used only when the cutoff was ≥5 mitoses per 2 mm2 (or per 10 HPF), or when the number of cases with mitotic count above the cutoff to determine differentiated high-grade thyroid tumor (i.e., ≥5 mitoses per 2 mm2) could be extracted. Studies reporting assessment of proliferative index by immunohistochemical markers (e.g., Ki-67, MIB-1) were not considered—since the use of immunohistochemistry markers is not explicitly recognized by the WHO scheme for diagnosing DHGTC of follicular cell origin—unless data on necrosis were provided. The complete Participants, Interventions, Comparisons, Outcomes, and Study design (PICOS) framework is reported in Table 1. The study was registered in the International Prospective Register of Systematic Reviews (PROSPERO, ID: CRD42022378716). The list of studies reviewed in full text and the reasons for exclusion are provided in Supplementary Table S1.
Eligibility Criteria Using Participants, Interventions, Comparisons, Outcomes, and Study Design Framework
IHC, immunohistochemistry.
Data extraction
Record screening and data extraction were carried out independently by two investigators (A.M.P. and E.M.) according to the above-mentioned framework. Disagreement was resolved by discussion with a third investigator (F.B.). For the studies that fulfilled the criteria but presented data in aggregate so that the prevalence of the features of interest could not be estimated, the corresponding author was contacted. In case of no reply, the study was excluded. The following parameters were extracted: first author and year of publication, country of the study cohort, period of data collection, total number of cases fulfilling the criteria described in the Population of the PICOS framework, total number of cases with tumor necrosis, total number of cases with mitotic count ≥5 mitoses per 2 mm2, type of study, type of tumors included in the study, and, when available, tumor subtypes.
The total number of cases fulfilling the criteria of DHGTC was obtained combining data on necrosis and mitosis. When overlapping cases could not be deducted, the number of DHGTC was defined as the minimum possible, thus with perfect overlapping between cases with necrosis and those with mitoses above the cutoff. When either data on necrosis or mitoses were provided, these were used to define the number of DHGTC. Data on the impact of necrosis and mitoses on prognosis were recorded when fulfilling the Population criteria of the PICOS. Quality of the studies included in the meta-analysis was assessed by a modification of the Newcastle–Ottawa scale for cohort and cross-sectional studies. 9 Although this tool consists of 3 categories (i.e., Selection, Comparability, and Outcome) with a maximum of 9 items, Comparability and Outcome were considered only when data on prognosis were available. Hence, studies used to assess the prevalence of DHGTC could be awarded with a maximum of 4 stars (i.e., 4 items of Selection). The complete criteria are available on the Supplementary Data S2.
Statistics
A meta-analysis was conducted using the raw numbers extracted in the previous phase. The metaprop function of the meta R package v.6.2-1 was applied to estimate the prevalence of DHGTC within WDTC and in the subtypes for which at least two studies were collected. The univariate meta-analysis was carried out with a random-effect model using the inverse variance method and logit transformation. Continuity correction of 0.5 was applied to studies with zero cell frequencies, and confidence intervals of individual studies were estimated by the Clopper–Pearson method. Heterogeneity was assessed via the I 2 and τ 2 statistics.
The latter was computed with the DerSimonian–Laird estimator, and confidence interval was estimated by the Jackson method. Substantial heterogeneity was defined when I
2 was above 50%, and p-value of Cochran's test was below 0.05,
10
and the causes of such heterogeneity were further explored whenever present. Publication bias and small study effects were evaluated by funnel plot and Egger's test. In the presence of significant bias (p ≤ 0.1) and in the absence of substantial heterogeneity, the trim-and-fill method was used for adjusting the number and outcomes of missing studies. All analyses and graphics were produced in R environment (v. 4.2.2;
Results
Literature search and quality assessment
Literature search identified 28 studies that met the criteria for inclusion; these were included in the systematic review and meta-analysis. The selection process is detailed in Figure 1. Twenty-four of the 28 studies included cases not selected nor enriched for patients' prognosis. These 24 studies (Table 2) were used to estimate the prevalence of DHGTC since the introduction of studies focusing on patients with poor prognosis might produce enrichment for aggressive pathological features, including necrosis and high mitotic count. Follicular thyroid carcinoma (FTC) represented about 6.1% of all cases. Four studies reported data on clinically selected patients (i.e., radioiodine-resistant tumors, metastatic PTC and FTC, fatal non-anaplastic tumors) and were used in a separate analysis (Table 3). Only four studies analyzed the prognostic impact of necrosis fulfilling the PICOS criteria. Sugitani et al. reported a significant association between necrosis and disease-specific survival, but the results were not confirmed on multivariate analysis. 11
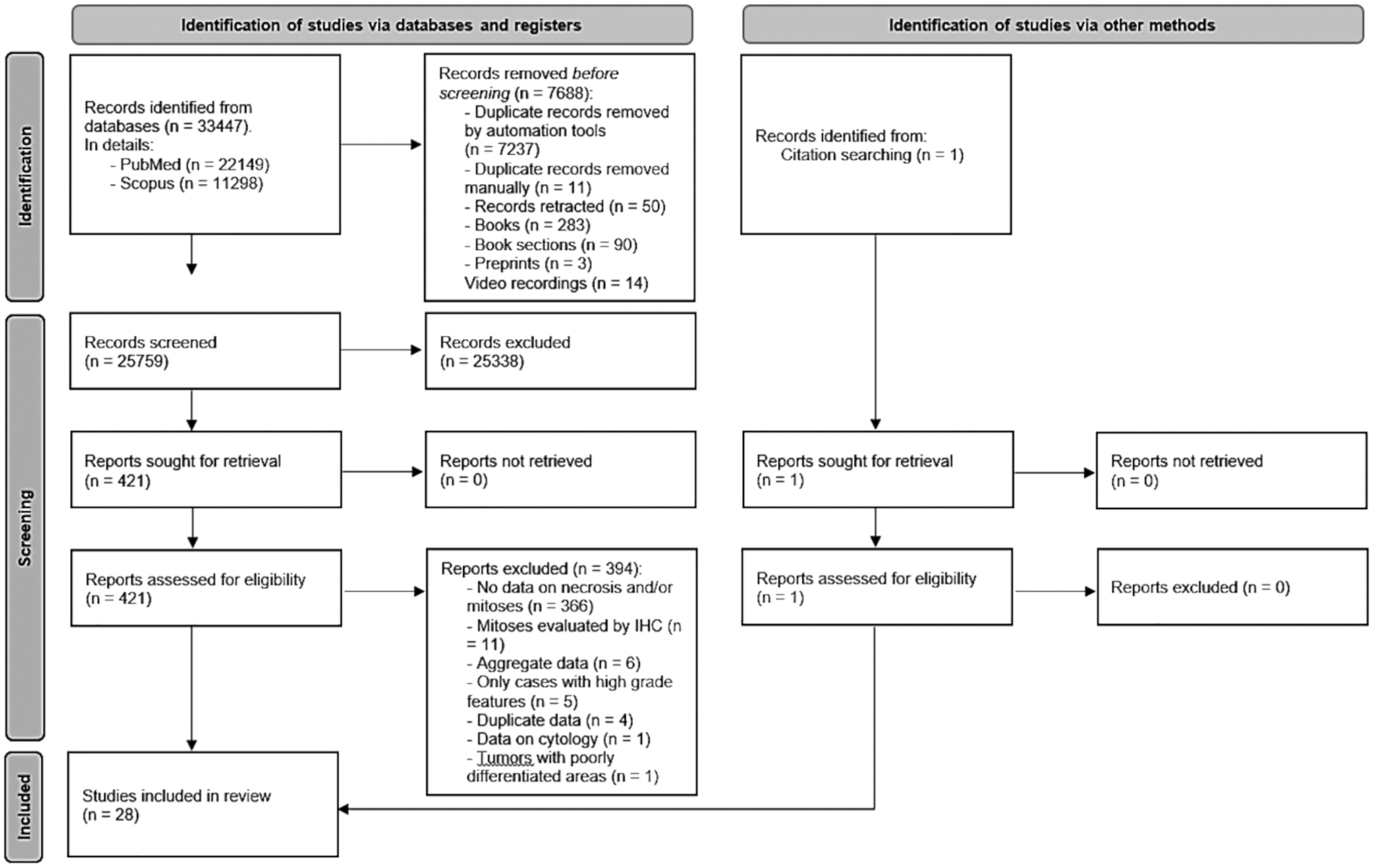
PRISMA flow diagram. The detailed process that led to the inclusion of 25 studies in the meta-analysis is shown. For each step, raw numbers and reasons of exclusion are reported. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Studies Reporting Data on High-Grade Features Without Clinical Selection of Patients and Included in the Meta-Analysis
Cases fulfilling the inclusion criteria and for which raw numbers were available.
Data on necrosis and mitosis provided in aggregate.
COLPTC, columnar subtype papillary thyroid carcinoma; DSPTC, diffuse sclerosing subtype papillary thyroid carcinoma; FTC, follicular thyroid carcinoma; HPTC, hobnail subtype papillary thyroid carcinoma; PTC, papillary thyroid carcinoma; SPTC, solid subtype papillary thyroid carcinoma.
Studies Reporting Data on High-Grade Features in Clinically Selected Patients
Cases fulfilling the inclusion criteria and for which raw numbers were available.
Data on necrosis and mitosis provided on aggregate.
Presence of metastases at diagnosis, development of distant metastases during follow-up, biochemical recurrence defined as >2 ng/mL levels of thyroglobulin after thyrotropin stimulation but in the absence of structural disease.
RAIR, radioiodine resistant.
Similar results were obtained by Póvoa et al., which observed the association between necrosis and recurrent or persistent disease only at univariate analysis. 12 In line with these findings, in the study by Metovic et al., 13 necrosis and mitotic count were associated with disease-free and overall survival at univariate analysis but were not independent predictors after adjusting for confounders. Finally, necrosis and high mitotic count were significant predictors of recurrence in the study by Jeong et al., 14 but only necrosis remained significant at multivariate analysis. These data could not be used for meta-analytic purposes due to the heterogeneity of endpoints.
In all studies, the data derive from secure records (i.e., surgical records or histological revision). The overall quality was superior for cohort studies in comparison with cross-sectional ones. The complete quality assessment of the studies is reported in Supplementary Table S2.
Meta-analysis of DHGTC prevalence in clinically unselected patients
The prevalence of DHGTC was assessed on 3095 WDTC from 24 studies without prior clinical selection. Raw numbers of tumor subtypes in this cohort are reported in Figure 2. Considering the entire WDTC cohort, 138 tumors could be reclassified as DHGTC. The random-effect model resulted in a pooled prevalence of 0.072 [95% confidence interval, CI, = 0.045–0.113] with a substantial heterogeneity among studies (I 2 = 84% [CI = 77–88%], p < 0.0001; Supplementary Fig. S1A). Hence, we began by stratifying cases by tumor growth pattern, which might account for such heterogeneity. The prevalence of DHGTC in all PTC (n = 2696) was 0.059 [CI = 0.036–0.097], again with substantial but lower heterogeneity (I 2 = 80% [CI = 69–87%], p < 0.0001; Supplementary Fig. S1B).
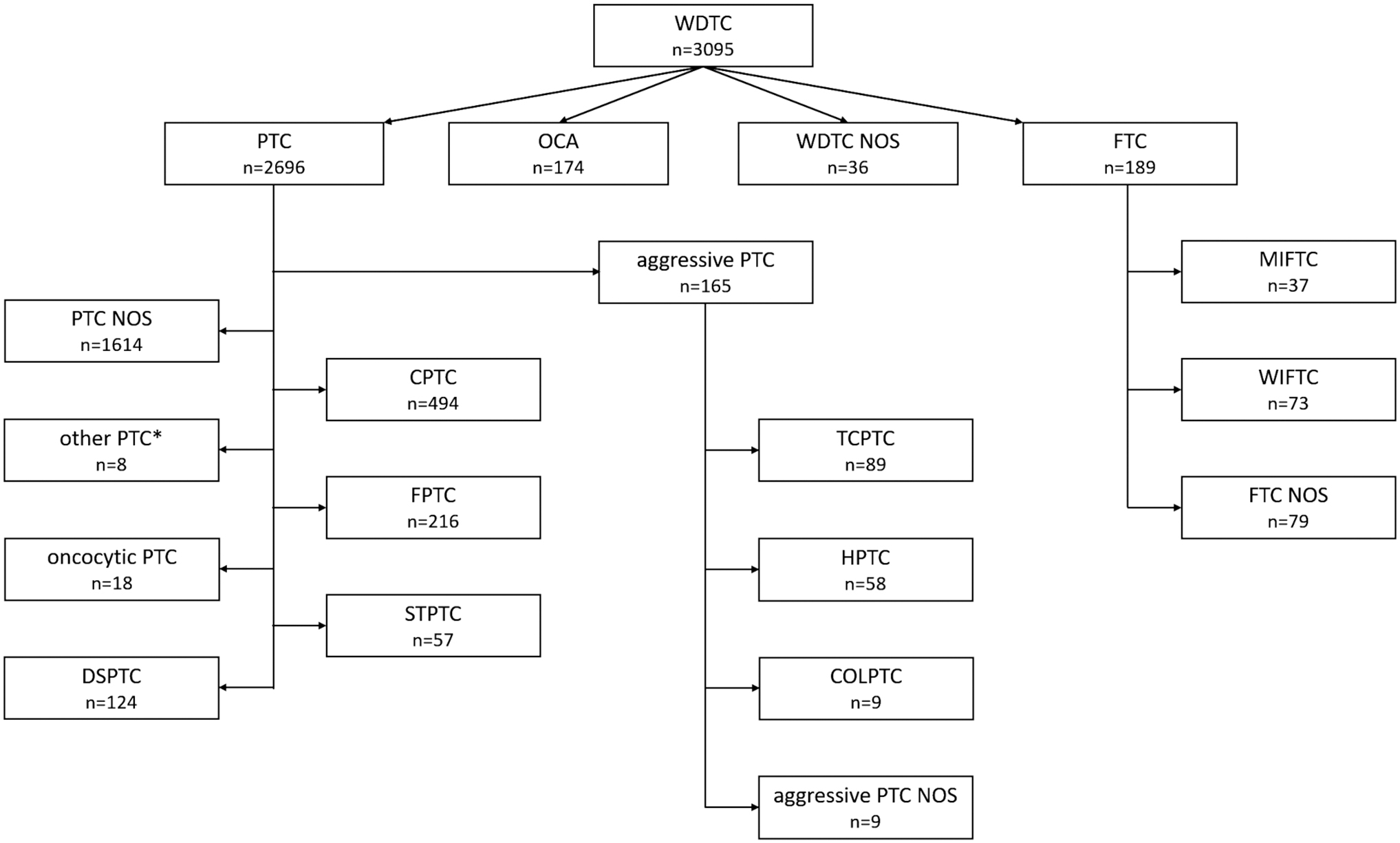
Cases without prior clinical selection included in the meta-analysis. The diagram details all the tumor subtypes. *Other PTC, not specified by the authors; other than CPTC, FPTC, TCPTC, and STPTC. COLPTC, columnar subtype papillary thyroid carcinoma; CPTC, classic subtype papillary thyroid carcinoma; DSPTC, diffuse sclerosing subtype papillary thyroid carcinoma; FPTC, follicular subtype papillary thyroid carcinoma; FTC, follicular thyroid carcinoma; HPTC, hobnail subtype papillary thyroid carcinoma; MIFTC, minimally invasive follicular thyroid carcinoma; NOS, not otherwise specified; OCA, oncocytic carcinoma; PTC, papillary thyroid carcinoma; STPTC, solid trabecular subtype papillary thyroid carcinoma; TCPTC, tall cell subtype papillary thyroid carcinoma; WDTC, well-differentiated thyroid carcinoma; WIFTC, widely invasive follicular thyroid carcinoma.
On the contrary, the estimated proportion of high-grade cases in FTC (n = 189) was greater than that in PTC: 0.146 [CI = 0.101–0.205] with I 2 = 0% ([CI = 0–75%], p = 0.74; Supplementary Fig. S1C). Then, a further stratification was performed based on PTC subtypes. The lowest proportion of tumors reclassified as high-grade was observed in diffuse sclerosing subtype papillary thyroid carcinoma (DSPTC, n = 82) after removing pediatric patients (i.e., the study by Saliba et al. 15 and 10 cases from the study by Chou et al. 16 ) that would have introduced significant heterogeneity: 0.018 [CI = 0.004–0.084], I 2 = 0% ([CI = 0–90%], p = 0.98; Supplementary Fig. S2A). The proportion of classic subtype papillary thyroid carcinoma (CPTC, n = 494) that could be reclassified as high-grade was 0.042 [CI = 0.027–0.066] with I 2 = 0% ([CI = 0–71%], p = 0.49; Supplementary Fig. S2B). In follicular subtype papillary thyroid carcinoma (FPTC, n = 216), the random-effect model resulted in a proportion of DHGTC of 0.076 [CI = 0.013–0.341], but the amount of heterogeneity was significant (I 2 = 79.1% [CI = 54.3–90.5%], p = 0.0002).
The major source of heterogeneity was attributed to the pediatric cohort from the study by Saliba et al. Hence, we removed this study and re-ran the analysis (n = 196) that resulted in a pooled proportion of 0.036 ([CI = 0.010–0.124]; I 2 = 31%, [CI = 0–73%], p = 0.22; Supplementary Fig. S2C). The proportion of high-grade tumors was higher in solid trabecular subtype papillary thyroid carcinoma (STPTC, n = 57): 0.154 [CI = 0.067–0.314], I 2 = 17% ([CI = 0–83%], p = 0.31; Supplementary Fig. S2D), as well as in tall cell subtype papillary thyroid carcinoma (TCPTC, n = 89): 0.187 [CI = 0.064–0.437], I 2 = 54% ([CI = 0–83%], p = 0.07; Supplementary Fig. S2E).
After adjusting for potential publication bias in the absence of significant heterogeneity, the estimated proportion of DHGTC in the hobnail subtype papillary thyroid carcinoma (HPTC, n = 58) raised to 0.202 [CI = 0.114–0.334], I 2 = 0% ([CI = 0–71%], p = 0.54; Supplementary Fig. S2F). Finally, we computed the cumulative proportion of high-grade tumors in those histological PTC subtypes considered to be clinically aggressive (i.e., TCPTC, HPTC, and columnar subtype papillary thyroid carcinoma 5 [COLPTC], n = 165): 0.168 [CI = 0.108–0.252], I 2 = 9% ([CI = 0–48%], p = 0.35; Supplementary Fig. S2G).
Similar to PTC, FTC was further stratified into minimally invasive follicular thyroid carcinoma (MIFTC) and widely invasive follicular thyroid carcinoma (WIFTC). In clinically unselected patients, the proportion of high-grade tumors was similar in MIFTC (n = 37, 0.136 [CI = 0.058–0.287], I 2 = 0% [CI = 0–0%], p = 0.81; Supplementary Fig. S3A) and WIFTC (n = 73, 0.152 [CI = 0.086–0.254], I 2 = 0% [CI = 0–0%], p = 0.60; Supplementary Fig. S3B). Significant publication bias was detected in HPTC only (p = 0.04), and estimates were adjusted as mentioned previously. All funnel plots are reported in Supplementary Figure S4A–I and L. The summary of the results in clinically unselected patients is reported in Figure 3.

Summary of results. The graph shows the prevalence (diamonds) and relative confidence interval (black lines) in clinically unselected cases and by tumor subtypes along with the total number of cases, the total number of studies, and heterogeneity.
Prevalence of high-grade tumors in clinically selected well-differentiated tumors
Since the impact of high-grade features on prognosis could not be estimated due to the lack of studies with common endpoints that met the inclusion criteria for the meta-analysis, we tried to assess it indirectly. In four studies 13,17 –19 (Table 3 and Supplementary Fig. S5), the presence of tumor necrosis and/or mitotic count were assessed in cohorts of patients with poor prognosis (i.e., radioiodine-resistant tumors, metastatic PTC and FTC, fatal non-anaplastic tumors, cases with biochemical recurrence). In these cases (n = 177), the pooled proportion of DHGTC was 0.287 [CI = 0.155–0.469], I 2 = 74% ([CI = 28–91%], p = 0.008; Supplementary Fig. S6). The main cause of such heterogeneity was attributed to the study by Metovic et al., in which cases with biochemical recurrence but no evidence of structural disease was included. Without this study, heterogeneity (I 2 ) dropped to 9% ([CI = 0–91%], p = 0.33). No significant publication bias was detected (p = 0.24; Supplementary Fig. S7).
Discussion
Grading of follicular cell-derived tumors, originally proposed in the year 2000, 2,20 has been introduced in the current fifth edition of the WHO classification of thyroid neoplasms. The current classification scheme distinguishes two types of high-grade tumors: PDTC and DHGTC. The latter represents a new entry, which is characterized by the presence of tumor necrosis and/or high mitotic count (i.e., ≥5 per 2 mm2) but not fulfilling the Turin criteria for PDTC. Since high-grade features have been often presented in aggregate data with PDTC and, sometimes, anaplastic tumors, the impact of this new DHGTC entry in the classification scheme is yet to be determined. In this study, we performed a systematic review and meta-analysis aimed at estimating the prevalence of high-grade tumors within WDTC and per tumor subtype. Pooled estimates were performed from studies reporting clinically unselected patients. Most of these studies presented consecutive cases series. The overall proportion of FTC (i.e., about 6.1%) is in line with previous literature reports. 3,21
Similarly, the cumulative rate (i.e., between 6.1% and 15.2%, computed on the total of PTC and without PTC not otherwise specified, respectively) of aggressive PTC subtypes (i.e., TCPTC, COLPTC, and HPTC) is consistent with that of consecutive series. 22 The aggregate prevalence of DHGTC in WDTC is about 7.2% of all cases. In accordance to the large clinical–pathological variability across tumor subtypes, heterogeneity among studies was high. To reduce heterogeneity, a first stratification was performed based on tumor growth pattern. The prevalence of high-grade features in FTC was more than double than that in PTC (14.6% vs. 5.9%). This result is in line with the poorer overall prognosis of FTC. 23 However, three considerations should be made. First, in this meta-analysis, WIFTC was more abundant than MIFTC (i.e., 73 vs. 37), which is not common in real-life series. Second, although the prevalence of high-grade tumors in MIFTC was only slightly lower than that in WIFTC (i.e., 13.6% vs. 15.2%), the former might encompass both true MIFTC and angioinvasive FTC.
Finally, in the case series described by Arif et al. and Cracolici et al., 24,25 some FTC show solid, trabecular, or insular areas; hence, the possibility that a part of them could be reclassified as PDTC cannot be excluded. As a consequence, the rate of high-grade FTC here reported might be overestimated, thus highlighting that, in FTC, the distinction between high grade and poorly differentiated might be subjected to interobserver variability. In regard to PTC subtypes, DSPTC showed the lowest rate of high-grade features (i.e., 1.8%) with the exception of tumors of pediatric age. Indeed, in the cohort described by Saliba et al., 15 10 of 32 (31%) pediatric DSPTC could be reclassified as DHGTC. As expected, a low proportion of FPTC presented high-grade features (i.e., 3.5%)—again with the exception of pediatric tumors 15 —followed by CPTC (4.2%). A remarkably higher prevalence of DHGTC was observed in STPTC (15.3%) and in those histological PTC subtypes considered to be clinically aggressive (i.e., TCPTC, COLPTC, and HPTC, 16.8%).
While these findings are consistent with the aggressive clinical–pathological behavior of TCPTC, COLPTC, and HPTC, 22 controversies exist around STPTC. In fact, in a meta-analysis, it was demonstrated that patients with solid PTC have a higher risk of recurrence and mortality than those with CPTC, 26 and some authors place STPTC among aggressive PTC subtypes. On the contrary, a recent study reported an excellent prognosis of patients with STPTC, especially those with encapsulated noninvasive tumors. 27 This controversy may be related to the lack of consensus around the proportion of tumor cells showing solid/trabecular growth pattern to define the tumor as STPTC as well as to the fact that at least 3 of the 11 publications reviewed in the meta-analysis of Vuong et al. 26 explicitly included cases with elevated mitotic count 28,29 or necrosis. 20 According to the current WHO indications, the diagnosis of solid PTC subtype requires that >50% of tumor show a solid, trabecular, or nested growth pattern. 3
Due to the lack of studies that met the inclusion criteria and with the same endpoint, to assess the prognostic impact of high-grade features on the prognosis of patients with WDTC, we estimated the proportion of cases that could be reclassified as DHGTC in four series of clinically selected patients (i.e., patients with biochemical recurrence, patients with radioiodine resistant tumors, patients with distant metastases, and patients who died of disease 17 –19 ). Almost one third (i.e., 28.7%) of these tumors presented high-grade features. It has to be acknowledged that, while the proportion of FTC in this cohort was similar to that of the clinically unselected one (7.9% vs. 6.1%), aggressive PTC accounted for about 30% of all PTC. Nevertheless, the pooled proportion of DHGTC in patients with poor prognosis was much higher than that in clinically unselected aggressive PTC (i.e., 16.8%), thus supporting a negative impact of high-grade features on the prognosis of patients with WDTC.
This study has some limitations. First, the estimates reported here derive from studies from various countries, different design, and with potential interobserver variability. Also, the estimates are mainly based on case series reporting the assessment of the features which define DHGTC (i.e., necrosis and mitotic count) and do not represent histological revisions specifically intended to assess DHGTC. The sample size of a few studies is small, thus suboptimal to estimate the prevalence of DHGTC. However, this is a common situation for reports of rare tumor types and subtypes. It has to be acknowledged that our estimates are conservative. In fact, a perfect overlap between the presence of necrosis and mitotic count above the cutoff was considered whenever this information was missing. Also, some studies did not evaluate mitotic counts, and the prevalence of DHGTC was solely based on the presence of necrosis. Due to the lack of assessment of mitotic counts in some studies, a higher prevalence of DHGTC especially among aggressive subtypes cannot be excluded.
Nevertheless, the estimates provided in this study were mostly generated using consecutive series and in controlled or absence of substantial heterogeneity; hence, the prevalence here provided can be considered representative of real-life data. The case of MIFTC may be an exception. Indeed, in this study, we could not distinguish angioinvasive tumors from true MIFTC (i.e., tumors with capsular invasion only). Regarding FPTC, the current edition of the WHO system has introduced several novelties, that is, the distinction between the invasive encapsulated FPTC and the infiltrative FPTC subtype; 3 in the present study, all FPTC were considered as a single group.
Also, the hobnail subtype was acknowledged in the WHO classification scheme only in 2017; hence, some cases might not have been diagnosed in earlier reports. Nevertheless, the criteria for the diagnosis of the hobnail subtypes were first outlined in 2004 30 and further refined in 2009. 31 Therefore, we do not expect substantial underestimation of the hobnail subtype. Finally, the association of high-grade features with poor prognosis could only be inferred indirectly, due to the lack of studies that met the inclusion criteria for the meta-analysis.
In conclusion, the introduction of DHGTC in the latest edition of the WHO may lead to the histological reclassification of a number of tumors of follicular cell derivation that is not negligible. The proportion of high-grade features is low in DSPTC, FPTC and CPTC, while in STPTC and histologically aggressive PTC subtypes, it can raise up to 20%. Significant differences could be observed in tumors of pediatric age, among which DSPTC and FPTC may frequently present with necrosis and/or high mitotic index. The reclassification of tumors as DHGTC will likely improve the prognostic stratification of patients with WDTC. This new scheme will identify patients who need aggressive therapeutic approach and more intensive follow-up. Also, this change will probably determine an enrichment of BRAF-like tumors (i.e., PTC, especially aggressive subtypes) within high-grade follicular cell-derived carcinomas. Dedicated studies should further assess the impact of high-grade features on prognosis of patients with specific WDTC subtypes.
Footnotes
Acknowledgments
We are grateful to Prof. Iwao Sugitani from the Nippon Medical School, Tokyo, Japan, Prof. Sofia Asioli from the University of Bologna, Italy, and Prof. Marco Volante from the University of Turin, Italy, for providing additional data and helpful information.
Authors' Contributions
Conceptualization: A.M.P. and F.B. Methodology: A.M.P., E.M., R.A.G., G.T., and F.B. Formal analysis: A.M.P. Writing—original draft: A.M.P. Writing—review and editing: all authors. Supervision: F.B.
Author Disclosure Statement
All authors have no disclosure to declare.
Funding Information
This study was supported in part by the Cancer Center Support Grant of the National Institutes of Health/National Cancer Institute under award number P30CA008748.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Figure S7
Supplementary Table S1
Supplementary Table S2
Supplementary Data S1
Supplementary Data S2