
Abstract
Background:
It has often been reported that thyroid-specific autoimmune diseases (ADs), such as Hashimoto's thyroiditis and Graves' disease, could increase the risk of thyroid cancer, but the association between other ADs beyond thyroid and thyroid cancer has not been well investigated. This study aimed to examine the risk of thyroid cancer in patients with eight ADs compared with those without ADs.
Methods:
This nationwide retrospective matched cohort study was conducted to investigate the relationship of eight ADs (Hashimoto's thyroiditis, Graves' disease, type 1 diabetes mellitus, Sjogren's disease, inflammatory bowel disease [IBD], vitiligo, systemic lupus erythematosus, and rheumatoid arthritis [RA]) with the risk of incident thyroid cancer using the National Health Insurance Service-National Sample Cohort. The Cox-proportional hazard model was used to estimate the adjusted hazard ratio (HR) and confidence intervals (CI) for thyroid cancer in relation to each of AD compared with control group without AD.
Results:
During the average follow-up of 9.49 years, 138 thyroid cancer cases were newly developed in control group and 268 cases were occurred in group with 8 ADs. For all of study participants, the risk of thyroid cancer was significantly increased in patients with Hashimoto's thyroiditis (HR = 2.10 [1.57–2.81]), Graves' disease (HR = 2.67 [1.99–3.62]), IBD (HR = 2.06 [1.50–2.83]), vitiligo (HR = 1.71 [1.13–2.59]), RA (HR = 1.76 [1.07–2.90]), and total of 8 ADs (HR = 1.97 [1.60–2.42]) compared with control group without ADs. When ADs were divided into three types, thyroid-specific ADs (HR = 2.37 [1.85–3.03]) showed the strongest and significant association with thyroid cancer, followed by local ADs (HR = 1.83 [1.41–2.38]), and systemic ADs (HR = 1.77 [1.14–2.74]).
Conclusions:
Specific ADs—especially for thyroid-specific AD, vitiligo, IBD, and RA—were associated with increased risk for thyroid cancer.
Introduction
Autoimmune disease (AD) is a condition arising from abnormal immune response to own tissues of body due to dysregulation of immune system. Accumulating evidence has indicated that chronic inflammation is closely associated with ADs, including rheumatoid arthritis (RA), inflammatory bowel disease (IBD), systemic lupus erythematosus (SLE), and type 1 diabetes mellitus (T1DM). 1 –3 The causative relationship between chronic inflammation and cancer has been well delineated since 1863. 4 Thus, chronic inflammation subsequent to AD arouses the interest on the association between AD and cancer.
Thyroid cancer is the most common malignancy of endocrine system, presenting a gradual increase in incidence rate from high-income countries to some middle-income countries. 5 In particular, Korea is of the highest incidence rate of thyroid cancer (45/100,000) in world. 5 Thyroid gland is predisposed to ADs such as Graves' disease and Hashimoto thyroiditis, affecting 2–5% of population. 6 –8 Meta-analyses and observational studies have shown that the risk of thyroid cancer increased in patients with several ADs such as T1DM, 9 RA, 10 Hashimoto thyroiditis, 11 SLE, 12,13 Sjogren's disease, 14 IBD, 15 and vitiligo. 16 Therefore, it seems plausible that the presence of AD has a potential effect on the development of thyroid cancer.
However, epidemiological evidence is still controversial for the effect of AD on the risk of thyroid cancer. In a recent cohort study of 478,753 participants from UK Biobank, despite significant association between immune-mediated diseases and increased risk of organ-specific cancer, AD was not associated with the risk of thyroid cancer. 17 In addition, there is ongoing debate whether the presence of AD per se increases the risk of thyroid cancer. 18
To identify the effect of ADs on the risk of thyroid cancer, we comprehensively investigated the association between thyroid cancer and eight ADs. Therefore, using large-scale cohort database representing entire Korean population and over 40,000 AD patients, we matched general population to patients with ADs to examine the risk of thyroid cancer in patients with 8 ADs compared with those without 8 ADs.
Methods
Study population
A nationwide retrospective matched cohort study was constructed using the National Health Insurance Service-National Sample Cohort (NHIS-NSC) database. All Korean citizens are obligated to join the National Health Insurance, and if a Korean receives a prescription or treatment covered by medical insurance, all medical records will be recorded in the National Health Insurance database. The NHIS-NSC database includes information about health insurance qualifications, history of hospital visit, diagnosis, treatment, and health checkup examination results from 2002 to 2019 (for 18 years) for 1 million people, which were collected through stratified random sampling based on sex, age, income level, and area. 19,20
The NHIS-NSC database was provided data without personal identification to researchers who want to conduct medical research through a remote access system. The cause of death data from Statistics Korea are also linked to the NHIS-NSC database. The last follow-up date was December 31, 2019. This study was reviewed and approved by Institute review board of Kyung Hee University (IRB No. KHSIRB-22-168).
Classification and definition of AD
We could not cover all types of ADs in this study, because there are too many different types of ADs. Therefore, we selected eight ADs, which were reported to be closely associated with thyroid cancer or thyroid disease through a review of the previous studies. 9 –16 In addition, it has been reported that these eight ADs share genetic loci with similar functions as well as epidemiological relevance. 21
Thereafter, ADs are classified into thyroid-specific AD (Hashimoto's thyroiditis and Graves' disease), local AD (T1DM, Sjogren's disease, IBD, and vitiligo), systemic AD (SLE and RA) according to the anatomical location and distance.
ADs were defined using the main diagnosis code (ICD-10 code) among patients without cancer in the NHIS-NSC database (Supplementary Table S1). Especially, T1DM was defined as those who had been diagnosed with the main diagnosis (ICD-10 code: E10) more than twice, and RA was defined as patients who had been diagnosed with ICD-10 code “M05” and prescribed DMARDs for more than 30 days.
Definition for thyroid cancer
Among patients without previous thyroid cancer history, patients newly diagnosed with the ICD-10 code “C73” as main diagnosis code were defined as thyroid cancer patients. The main diagnosis for cancer in the NHIS-NSC database showed relatively good accuracy when compared with the patients confirmed as cancer in the cancer registration database. 22
Selection of the study participants
The index dates were defined as the first date of health examination between 2009 and 2010. The total number of source populations in 2009–2010 was 495,060 individuals. Of those, 354,155 people who participated in the health examination in 2009–2010 and had complete data for major covariates. In addition, 2856 patients were excluded because of known prevalence thyroid cancer before the index date, leaving 351,299 to develop the matched cohort.
The propensity score matching was used to match 1:1 (AD vs. control group) using age, sex, smoking, alcohol intake, fasting blood glucose, frequency of physical activity, body mass index (BMI), and income level based on the nearest neighbor matching algorithm, a maximum caliper distance was set to 0.1. Finally, 16,328 people with 8 ADs and 16,328 control group without 8 ADs were selected as final study population, respectively (Fig. 1).
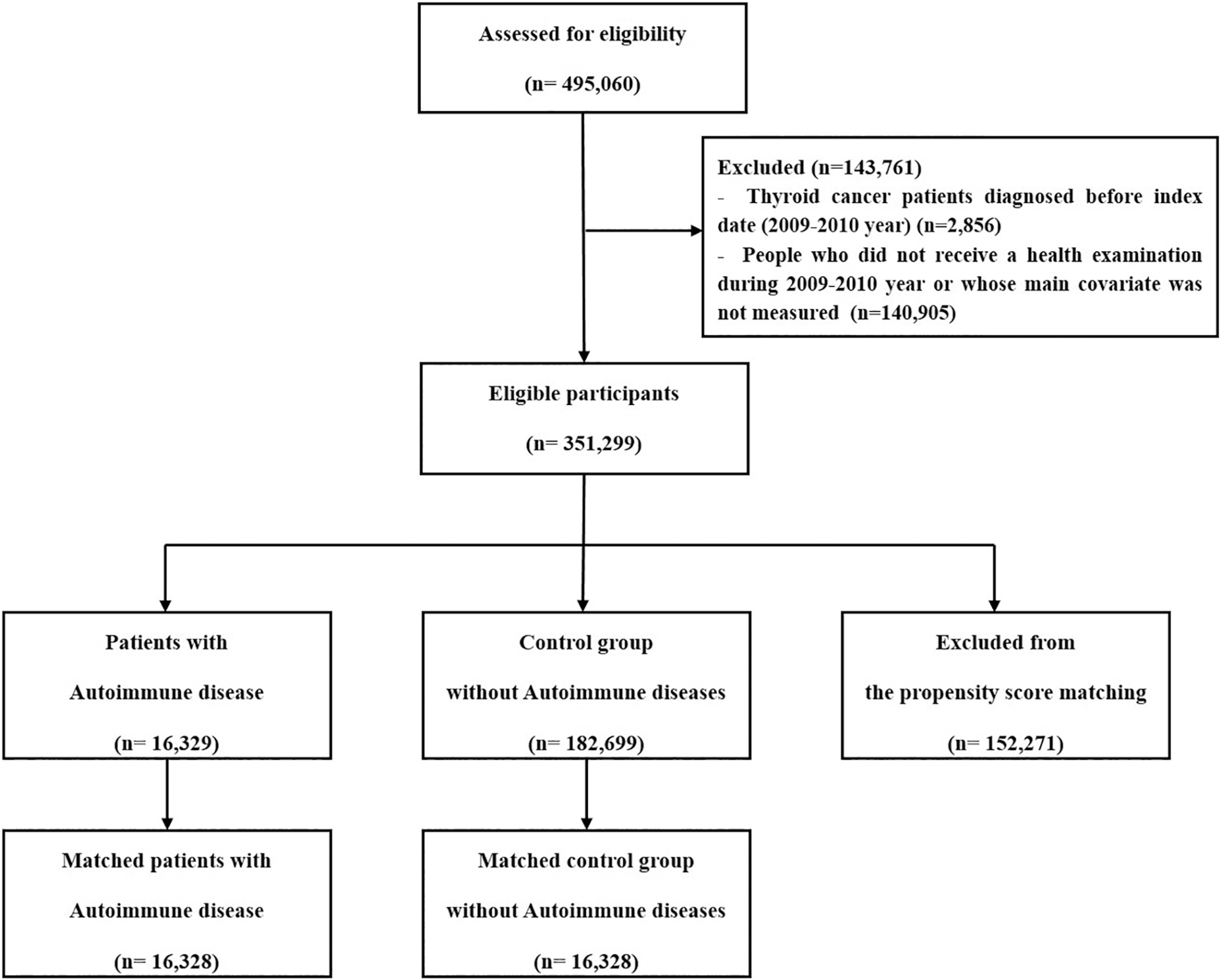
Flowchart for selection of study participants.
Follow-up of study participants
Study participants were followed from the index date (dates of health examination between 2009 and 2010) to December 31, 2019. People who withdrew from the study or died from any causes during the follow-up period or those who observed without any event until December 31, 2019 were considered as censoring cases. Person-year was calculated as the sum of the follow-up year from the index date to the occurrence of new thyroid cancer or censoring of the study.
Other covariates for thyroid cancer
Information on smoking status, alcohol intake and physical activity was obtained through questionnaires. Smoking status was classified into current smokers, former smokers, and never-smokers. Alcohol consumption was defined as those who drank alcohol three or more times a week.
The physical activity was classified into 0, 1–4, and 5 days or more per week using the number of days of moderate exercise of 30 minutes or more. BMI was calculated as weight (kg) divided by the square of height (meters). Fasting blood glucose level (mg/dL) was collected after 8 hours of fasting. Income level was divided into quintile groups and Medicaid based on insurance premiums.
Statistical analysis
The baseline characteristics of study participants were presented as number (percentage) for categorical variables and mean (standard deviation) for continuous variables. Incidence rates and confidence intervals (CIs) for each group of eight ADs were calculated as new thyroid cases divided by total person-years. The plots of cumulative incidence rate were illustrated to compare the difference in the incidence rates of thyroid cancer between each group of eight ADs and the control group without AD, and the differences between them was tested by the log-rank test.
After adjusting for age, sex, BMI, fasting blood glucose level, smoking status, alcohol intake, physical activity, and income level, the Cox proportional hazards models were used to calculate adjusted hazard ratios (HRs) and CIs for the risk of thyroid cancer (adjusted HR [CI]) in relation to each of eight ADs and total of eight ADs, compared with control group. It was checked whether the log–log survival function was parallel and satisfied the proportional hazard assumption, and if it was visually parallel, it was considered not to violate the proportional hazard assumption.
The significance level was set to 0.05. All statistical analyses were performed using SAS (version 9.4; SAS Institute, Cary, NC, USA) and R software (version 4.0.0; Vienna, Austria).
Results
Baseline characteristics of study participants
Table 1 shows baseline clinical and demographic characteristics of patients with eight ADs compared with control group without ADs. The overall proportions of total ADs were higher in females (60.2%) than males (39.8%), but the proportion of males were higher than females in patients with T1DM and IBD. The propensity score matched cohort showed no significant difference in age, BMI, fasting glucose, smoking status, alcohol intake, physical activity, and income levels between patients with eight ADs and control group. Regarding the incidence of thyroid cancer, each group of individual AD and group with total of ADs had the higher incidence of thyroid cancer than control group, except for T1DM.
Baseline Characteristics of the Study Participants
Students' t-test was used to examine the difference between patients with autoimmune diseases and control group, and chi-square test was used to examine the difference between patients with autoimmune diseases and control group.
ADs, autoimmune diseases; BMI, body mass index; IBD, inflammatory bowel disease; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; T1DM, type 1 diabetes mellitus.
When comparing the prevalence of comorbidities between the AD group and the control group, the AD group showed higher prevalence of gastric cancer, colorectal cancer, and liver cancer than control group, except for lung cancer. The prevalence of acute myocardial infarction, stroke, and hypertension was higher in the AD group than control group (Supplementary Table S2).
Incidence rates of thyroid cancer by specific types of ADs
Crude incidences of thyroid cancer according to types of ADs are presented in Table 2. In all of study participants, each group of individual AD except for T1DM had the higher incidence for thyroid cancer, compared with control group. Although the incidence rates of thyroid cancer were higher in females compared with those of males, the incidence rates of thyroid cancer were higher in both males and females with thyroid-specific ADs—Hashimoto's thyroiditis and Graves' disease—compared with control group. In addition, point estimates of crude incidence rates were higher in patients with IBD, SLE, and vitiligo of females.
Incidence Rates for Thyroid Cancer According to Autoimmune Diseases
The crude incidence rates are presented as number of thyroid cases per 100,000 person-years and Poisson method was used to estimate CIs.
CI, confidence interval.
HRs for risk of thyroid cancer by specific types of ADs
Table 3 presents adjusted HRs and CIs for the incident thyroid cancer of each types of AD, total of ADs, and control group. For all of study participants, the risk of thyroid cancer was significantly higher among patients with Hashimoto's thyroiditis (HR = 2.10 [1.57–2.81]), Graves' disease (HR = 2.67 [1.97–3.62]), IBD (HR = 2.06 [1.50–2.83]), vitiligo (HR = 1.71 [1.13–2.59]), RA (HR = 1.76 [1.07–2.90]), and total of 8 ADs (HR = 1.97 [1.60–2.42]) compared with control group. In males, Graves' disease (HR = 4.22 [1.95–9.13]), IBD (HR = 2.58 [1.35–4.93]), and total of 8 ADs (HR = 1.97 [1.61–2.43]) were significantly associated with increased risk of thyroid cancer, compared with control group.
Hazard Ratios and Confidence Intervals for Thyroid Cancer According to Autoimmune Diseases
The Cox-proportional hazard models were performed after adjusting for multiple covariates. Multivariable model 1 was adjusted for age, sex, BMI, and fasting blood glucose. Multivariable model 2 was adjusted for Multivariable model 1 and smoking status, alcohol intake, physical activity, and income level.
In females, the HRs for thyroid cancer were higher in patients with Hashimoto's thyroiditis (HR = 2.06 [1.52–2.80]), Graves' disease (HR = 2.46 [1.77–3.43]), IBD (HR = 1.92 [1.32–2.78]), vitiligo (HR = 1.69 [1.07–2.66]), and total of 8 ADs (HR = 1.97 [1.61–2.43]) than control group. Although the point estimate of adjusted HRs for thyroid cancer among patients with Sjogren's disease, T1DM, and SLE were higher than 1, it was not statistically significant. This was partially because Sjogren's disease and SLE are rare diseases and have low statistical power (Fig. 2).
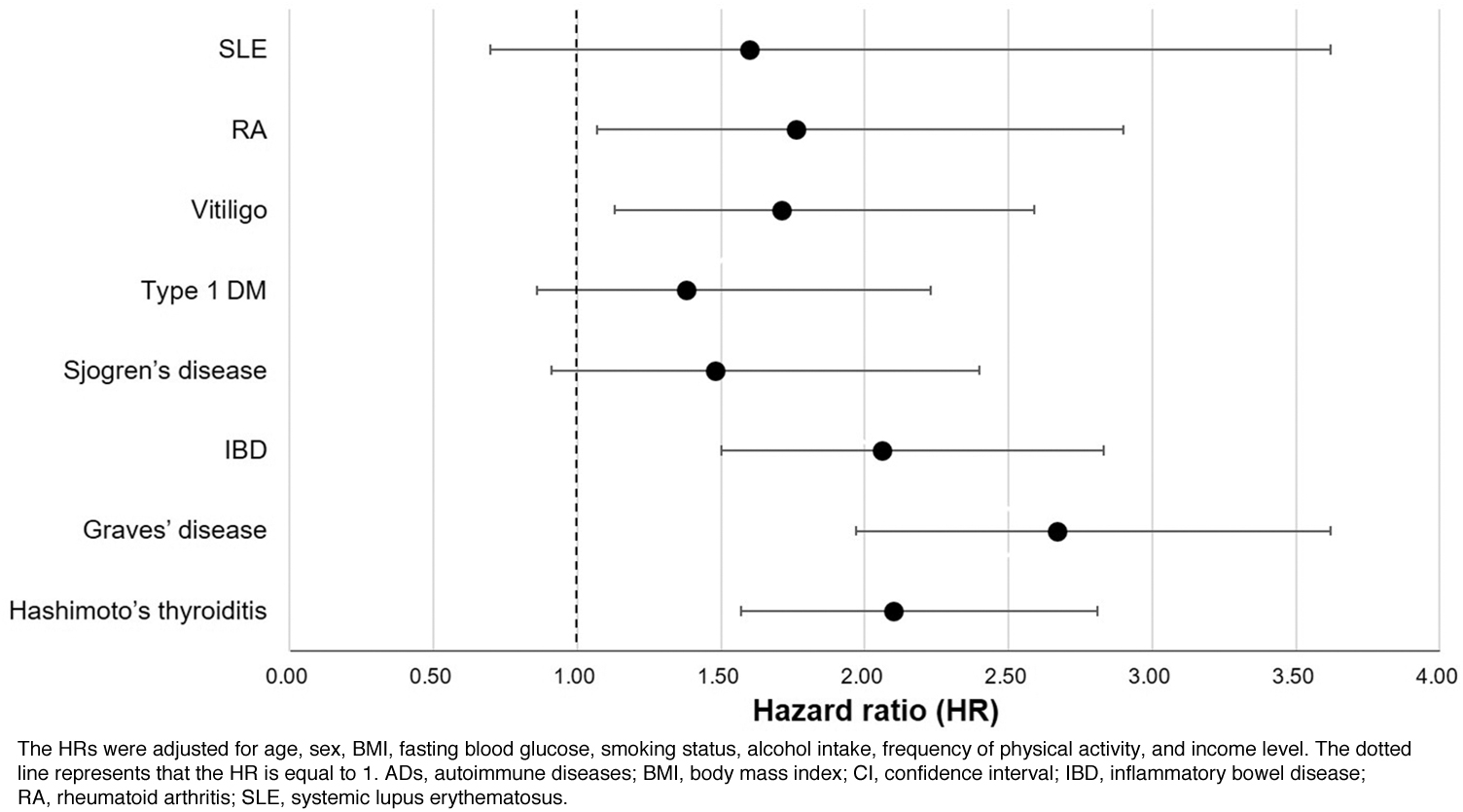
HRs and CIs for thyroid cancer according to types of ADs.
Risk of thyroid cancer for thyroid-specific, local, and systemic ADs
When ADs were classified into thyroid-specific, local, and systemic ADs, the crude incidence rate of thyroid cancer was highest in patients with thyroid-specific AD, followed by systemic AD and local AD (Supplementary Table S3). The Kaplan–Meier curve also showed that the risks of thyroid cancer in patients with thyroid-specific, local, and systemic ADs were higher than the control group (Supplementary Figs. S1–S3). However, after adjusting for all covariates, thyroid-specific ADs had the strongest and significant association with risk of thyroid cancer (HR = 2.37 [1.85–3.03]), followed by local AD (HR = 1.83 [1.41–2.38]), systemic AD (HR = 1.77 [1.14–2.74]), compared with control group (Table 4). Cases with two or more ADs were very rare, except for having both of Hashimoto's thyroiditis and Graves' disease (Supplementary Table S4).
Hazard Ratios and Confidence Intervals for Thyroid Cancer in Patients with Thyroid-Specific, Local, and Systemic Autoimmune Diseases
The Cox-proportional hazard models were performed after adjusting for multiple covariates. Multivariable model 1 was adjusted for age, sex, BMI, and fasting blood glucose. Multivariable model 2 was adjusted for Multivariable model 1 and smoking status, alcohol intake, physical activity, and income level.
ADs were classified into three groups: Thyroid-specific ADs = Hashimoto's thyroiditis, Graves' disease; local AD = T1DM, Sjogren's disease, IBD, vitiligo; systemic AD = systemic lupus erythematosus, rheumatoid arthritis.
Discussion
This large cohort study showed that thyroid-specific, local ADs (vitiligo and IBD), and RA were associated with increased risk of thyroid cancer. Especially, among many ADs, the Hashimoto's thyroiditis and Graves' diseases, which were limited to the thyroid tissue had the strong and significant association with thyroid cancer. In addition, each of seven ADs (except for T1DM) had the higher age-adjusted incidence rate of thyroid cancer than control group. Total patients of eight ADs also showed the increased incidence rate and higher risk for thyroid cancer, compared with control group. These results are in line with previous showing thyroid-specific AD is associated with the increased risk of thyroid cancer.
It is presumed that immune responses in ADs are involved in carcinogenesis. AD is characterized by pro-inflammatory low regulatory T cells, 23 which is frequently observed in the initiation of cancer. 3 Thus, we hypothesized that the presence of specific ADs may have a carcinogenic effect on the development of thyroid cancer. To verify this hypothesis, we analyzed the risk of thyroid cancer in relation to each of eight ADs, including Hashimoto's thyroiditis, Graves' disease, IBD, T1DM, Sjogren's disease, vitiligo, SLE, and RA, and total of eight ADs, compared with control group.
Hashimoto's thyroiditis is an autoimmune thyroid disease in which the immune system attacks the thyroid gland, leading to inflammation. Hashimoto's thyroiditis refers to chronic lymphocytic thyroiditis characterized by immune cells infiltration of the thyroid gland as a result of failure in immune tolerance. 3,8,11 Several meta-analysis studies showed that Hashimoto's thyroiditis was significantly associated with the increased risk for thyroid cancer. 24 –27
Mechanisms linking Hashimoto's thyroiditis to thyroid cancer may include inflammatory reaction causing DNA damage through formation of reactive oxygen species, and elevated levels of thyrotropin (TSH) stimulating follicular epithelial proliferation. 11,28,29 A review article also reported that the serum TSH level, even within normal range was associated with higher risk of thyroid cancer and more advanced stage of thyroid cancer. 30
A recent Mendelian randomization study also reported that elevated TSH level has causal role in thyroid cancer. 31 Pani et al. reported that inflammation and proliferation play an important role in autoimmune thyroiditis and thyroid cancer, and that these pathological changes are regulated by various components of the immune system. 32 Graves' disease is also another type of autoimmune thyroid disease, occupying most common cause of hyperthyroidism. 7,8
Graves' disease seemed to be associated with larger, multifocal, and more aggressive thyroid cancer than single hot nodules or multinodular toxic goiter. A nationwide representative cohort study in Taiwan also showed that patients with Graves' disease had almost 10 times increased risk of thyroid carcinoma than those without Graves' disease. 33 However, Rotondi et al. reported that there was no significant association between chronic autoimmune thyroiditis and thyroid cancer, when 510 patients with chronic autoimmune thyroiditis were observed for 10 years. 34
The association between IBD and thyroid cancer is still controversial. 35,36 In a study for Finnish patients with ulcerative colitis and Crohn's disease, patients with ulcerative colitis showed an increased standardized incidence ratio (SIR) for thyroid cancer compared with those expected in general population. 35 However, a study for 2621 Chinese patients with IBD failed to show the significant association between IBD and the risk of thyroid cancer. 36 Our result supports the hypothesis that IBD increases the risk of thyroid cancer. A recent large case–control study and meta-analysis also showed that IBD and ulcerative colitis were associated with elevated risk of thyroid cancer, similar to our findings. 15
Vitiligo was significantly associated with the increased risk of thyroid cancer in only females. There have been studies indicating the significant association of T1DM and vitiligo with thyroid cancer. A meta-analysis for 15 observation studies showed that T1DM was associated with an increased risk of thyroid cancer. 9 In a nationwide population-based Korean study, patients with vitiligo were at increased risk of thyroid cancer, compared with the controls. 16 There was rare study on the relationship between RA and thyroid cancer. A review article reported that RA and autoimmune thyroid disease have affected each other disease in a bidirectional manner. 37 A recent Korean study has reported that SIR of thyroid cancer was 1.75 (CI = 1.02–2.68) among women with RA. 10
Some limitations should be considered in this study. First, there is a possibility for the overestimation and detection bias in the incidence of thyroid cancer, especially for patients with thyroid ADs. Major explanation for this phenomenon is high accessibility to screening examinations using thyroid ultrasonography for thyroid cancer in Korea. 38 Patients with thyroid ADs may have more chance for screening for thyroid, which can be potential bias leading high detection rate of thyroid cancer.
Second, we could not evaluate the stage and pathological specific thyroid cancer risk and diagnostic method for thyroid cancer, because stage, pathological information, and diagnostic method on thyroid cancer were not available in the NHIS-NSC database. Third, we applied an operational definition for ADs using ICD-10 codes and drug prescriptions, but misclassification bias for ADs may occur. Our database is a secondary data source and is not collected for research purposes.
However, we referred carefully to the published literature to reduce the misclassification bias, and applied different operational definition for each AD. Fourth, there may be low statistical power especially for male ADs and rare ADs such as SLE and Sjogren's disease. This small number of thyroid cancer cases among subgroups may have lowered the statistical power, masking a significant association.
In conclusion, the risk of thyroid cancer was significantly increased in patients with Hashimoto's thyroiditis, Graves' disease, IBD, vitiligo, and RA. These results suggest that specific ADs potentiate the development of thyroid cancer. Further large-scale AD-specific study may be needed to clarify the association between local and systemic ADs and thyroid cancer.
Footnotes
Acknowledgments
We used the National Health Insurance Service-National Sample Cohort (NHIS-NSC) database (No. NHIS-2022-2-245) and the data set was obtained from the National Health Insurance Service. NHIS played no role in the study design, data curation, and interpretation of data.
Authors' Contributions
C.-M.O. made substantial contributions to the conception of the work, acquisition and interpretation of the data, and data analysis. S.K.P. and J.-H.R. wrote the article and contributed to the study design and interpretation of data. M.-H.K. conducted data analysis and illustrated the figures. M.-H.K., J.Y.J., Y.-S.J., K.-N.K., and S.S. made substantial contributions to the acquisition of the data and critical revision of the study protocol and article. All authors were involved in reviewing, editing, and final approval of the article. C.-M.O. is responsible for the overall content.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by grants from Kyung Hee University in 2023 (KHU-20230913 and KHU-20231514). The funding organization had no role in the design or conduct of this study.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4