
Abstract
Objective:
Rurality is associated with higher incidence and higher disease-specific mortality for most cancers. Outcomes for rural and ultrarural (“frontier”) patients with thyroid cancer are poorly understood. This study aimed to identify actionable deficits in thyroid cancer outcomes for rural patients.
Methods:
We queried linked California Cancer Registry and California Office of Statewide Health Planning and Development databases for patients diagnosed with thyroid cancer (1999–2017). We analyzed time from disease stage at diagnosis, time from diagnosis to surgery, receipt of appropriate radioactive iodine ablation, surveillance status, and overall and disease-specific mortality for urban, rural, and frontier patients. Cox and logistic regression models controlled for clinical and demographic covariates a stepwise manner. All incidence figures are expressed as a proportion of newly diagnosed cases.
Results:
Our cohort comprised 92,794 subjects: (65,475 women [70.6%]; mean age 50.0 years). Compared to urban patients, rural and frontier patients were more likely to be American Indian, White, uninsured, and from lower quintiles of socioeconomic status (p < 0.01). Distant disease at diagnosis was more common in rural (56.0 vs. 50.4 cases per 1000 new cases, p < 0.01) and frontier patients (80.9 vs. 50.4 per 1000, p < 0.01) compared to urban patients. The incidence of medullary thyroid cancer was greater in rural patients (17.9 vs. 13.6 cases per 1000, p < 0.01) and frontier patients (31.0 vs. 13.6 per 1000, p < 0.01) compared to urban patients. The incidence of anaplastic thyroid cancer was higher in frontier versus urban patients (15.5 vs. 7.1 per 1000, p < 0.01). When compared to urban patients, rural and frontier patients were more often lost to follow-up (odds ratio [OR] 1.69 [confidence interval, CI 1.54–1.85], and OR 3.03 [CI 1.89–5.26], respectively) and had higher disease-specific mortality (OR 1.18 [CI 1.07–1.30], and OR 1.92 [CI 1.22–2.77], respectively). Rural and frontier residence was independently associated with being lost to follow-up, suggesting that it is a key driver of disparities.
Conclusion:
Compared to their urban counterparts, rural and frontier patients with thyroid cancer present with later-stage disease and experience higher disease-specific mortality. They also are more often lost to follow-up, which presents an opportunity for targeted outreach to reduce the observed disparities in outcomes.
Introduction
In the United States, around 57 million people live in census tract rural-designated areas, representing 17% of the population. Rural-urban cancer disparities are well-documented and worsening, with major impacts on rural patients' morbidity and mortality. 1,2 Overall incidence of cancer and mortality rates, including lung, oropharyngeal, and colorectal cancer are higher in rural areas. 3 The higher incidence of cancer has been variously attributed to rural-urban differences in tobacco use, 4 HPV vaccination, 5 obesity, 6 degree of physical inactivity, 7 sun exposure, 8 and agricultural carcinogen exposure. 9 However, these attributions are likely only partial, as they do not account for the social and structural determinants of health, including the impact of access to specialists on rural morbidity and mortality. 10
While existing work has demonstrated and provided plausible partial causes for the rural-urban cancer disparities observed in breast, cervical, lung, colorectal, prostate, and hematologic cancers, there is a paucity of data on the impact of rurality on thyroid cancer outcomes. 11 –17 Inequitable access to guideline-concordant treatment, and especially to high-quality curative-intent surgery, is thought to be a key driver in worsening disparities. 11
The incidence of thyroid cancer in the United States is 13.7 per 100,000 with about 54,000 new cases being diagnosed annually. 18 Thyroid cancers are more likely to be diagnosed in urban patients, among those with higher socioeconomic status (SES) and among the privately insured. 19,20 A close eye has yet to be turned on the degree to which rural residence impacts the diagnosis, treatment course, and outcomes for thyroid cancer patients.
The present study examined the thyroid cancer continuum of care for rural and ultrarural (“frontier”) patients with thyroid cancer by performing a retrospective cohort study of all thyroid cancer cases diagnosed in California over a 19-year period. We conceptualized the thyroid cancer continuum of care to be a multidisciplinary and dynamic process, marked by several outcomes reported in cancer databases: stage at time of diagnosis, receipt of surgery, time from diagnosis to curative-intent surgery, appropriate use of adjuvant radioactive iodine (RAI) treatment, loss to follow-up, and overall and disease-specific mortality by degree of rurality (Fig. 1). We hypothesized that thyroid cancer patients in rural and frontier areas experience worse cancer outcomes compared to their urban counterparts. We also aimed to provide the first known evaluation of the demographic and clinical key-drivers of worse thyroid cancer outcomes by rurality.
Study population.
Methods
Patient selection
Approvals from the California Committee for the Protection of Human Subjects (IRB 14-10-1768 “Impact of Surgery and Adjuvant Treatment on Thyroid, Parathyroid, Adrenal, and Neuroendocrine Tumors”) and the UCLA Office of the Human Research Protection Program (IRB No. 14-001553-CR-00005 “Endocrine Disorders in California”) were obtained. We obtained the linked California Cancer Registry (CCR) and California Office of Statewide Health Planning and Development Patient Discharge Data (OSHPD-PDD) and California Office of Statewide Health Planning and Development Ambulatory Surgery Center (OSHPD-ASC) databases for thyroid cancer patients diagnosed between 1999 and 2017. The CCR is a comprehensive central cancer registry that mandates cancer reporting by law and should therefore capture all cases of thyroid cancer diagnosed in the state. The OSHPD-PDD and OSHPD-ASC databases include admissions and procedure details from all nonfederal licensed hospitals and ambulatory surgery centers in California.
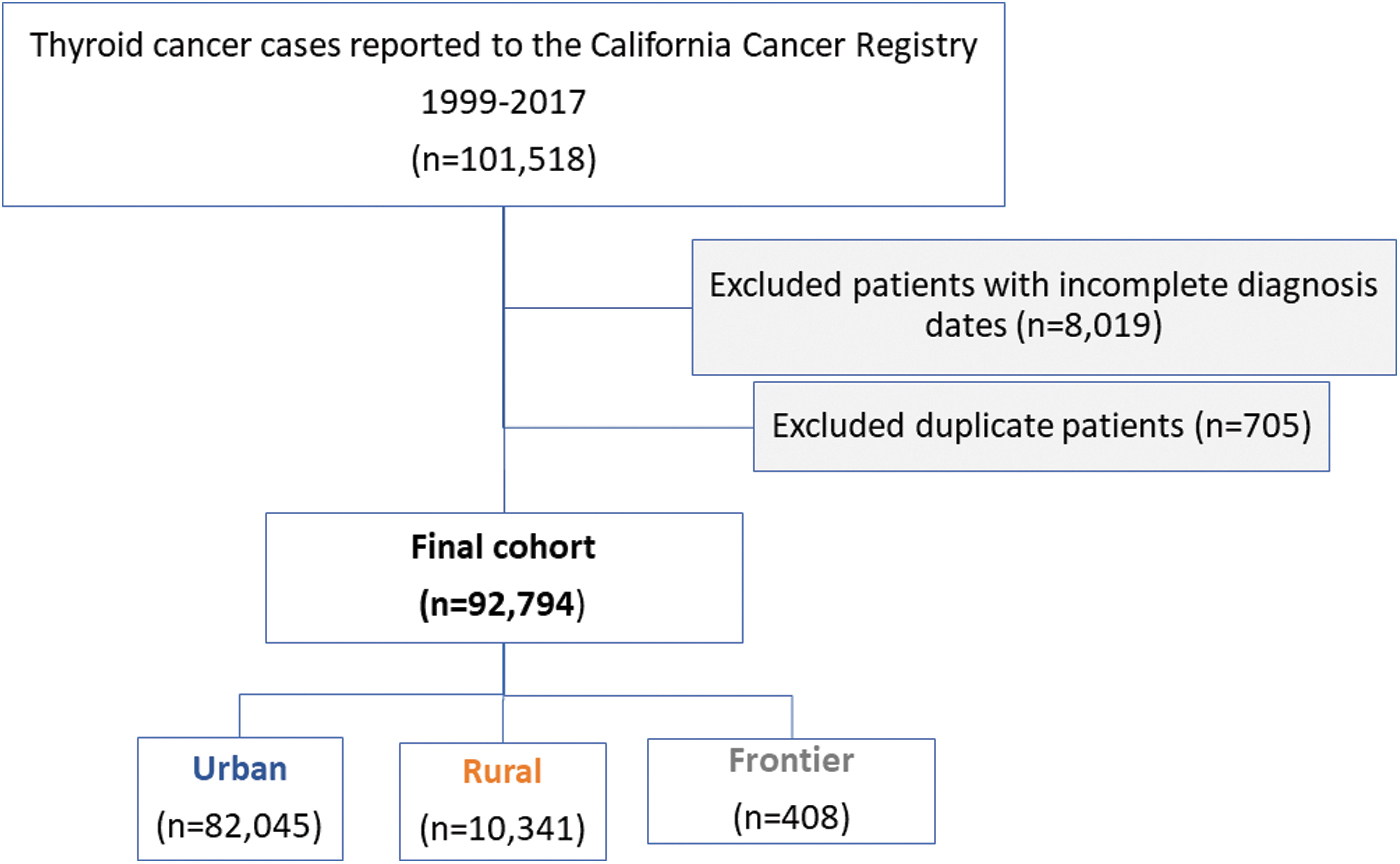
All cases of thyroid cancer from 1999 to 2017 were reviewed; duplicate patient IDs were excluded. Patients with multiple tumors were used as a single record with the largest tumor used analysis of tumor characteristics and clinical covariates. Complete patient data, including follow-up, was available for the study cohort through the end of 2021. Given that many of the outcomes designated for the thyroid cancer continuum of care were measures of timeliness, patients with incomplete dates of diagnosis—for example, year only with no month or date—were excluded from the study (Fig. 1).
Independent variables
Rurality
The independent variable of interest was Medical Service Study Area (MSSA) categorization: rural, urban, or frontier. MSSA categories were created by the California Office of Statewide Health Planning and Development. These are census-tract informed subcounty geographic units that assign degrees of rurality to all California regions with the aim of determining medically underserved areas. 21 The distinction between rural and ultrarural or “frontier” spaces is a well-recognized and meaningful indicator across multiple government agencies. 22 Although the MSSAs were designed to be relatively stable over time, we used MSSA codes from 2000 for patients in the study period 1999–2005 and MSSA codes from 2010 for patients in the study period 2006–2017. Urban MSSAs have a population range from 75,000 to 125,000; rural MSSAs have a population density of <250 persons per square mile. Frontier regions, comprising the most rural areas, have a population density of <11 person per square mile.
Dependent variables of interest
The thyroid cancer continuum of care
We conceptualized the thyroid cancer continuum of care to be a multidisciplinary and dynamic process. The continuum begins with recognition, diagnosis, and evaluation of cervical nodes of a new thyroid cancer. The patient may then be referred to a surgeon for shared decision-making regarding treatment options, with a focus on a pathway to guideline-concordant surgery, where appropriate. Postoperatively, in the appropriate patient, RAI may be offered. Thereafter, patients are followed with surveillance ultrasound and thyroglobulin and thyroglobulin antibody levels for varying degrees of time, depending on the patient's risk of recurrence. These waypoints on the continuum were correlated with reported outcomes in our cancer databases: time from diagnosis to curative-intent surgery, receipt of surgery, rates of completion thyroidectomy, appropriate use of adjuvant RAI, active follow-up, and overall and disease-specific mortality by degree of rurality (Fig. 2).
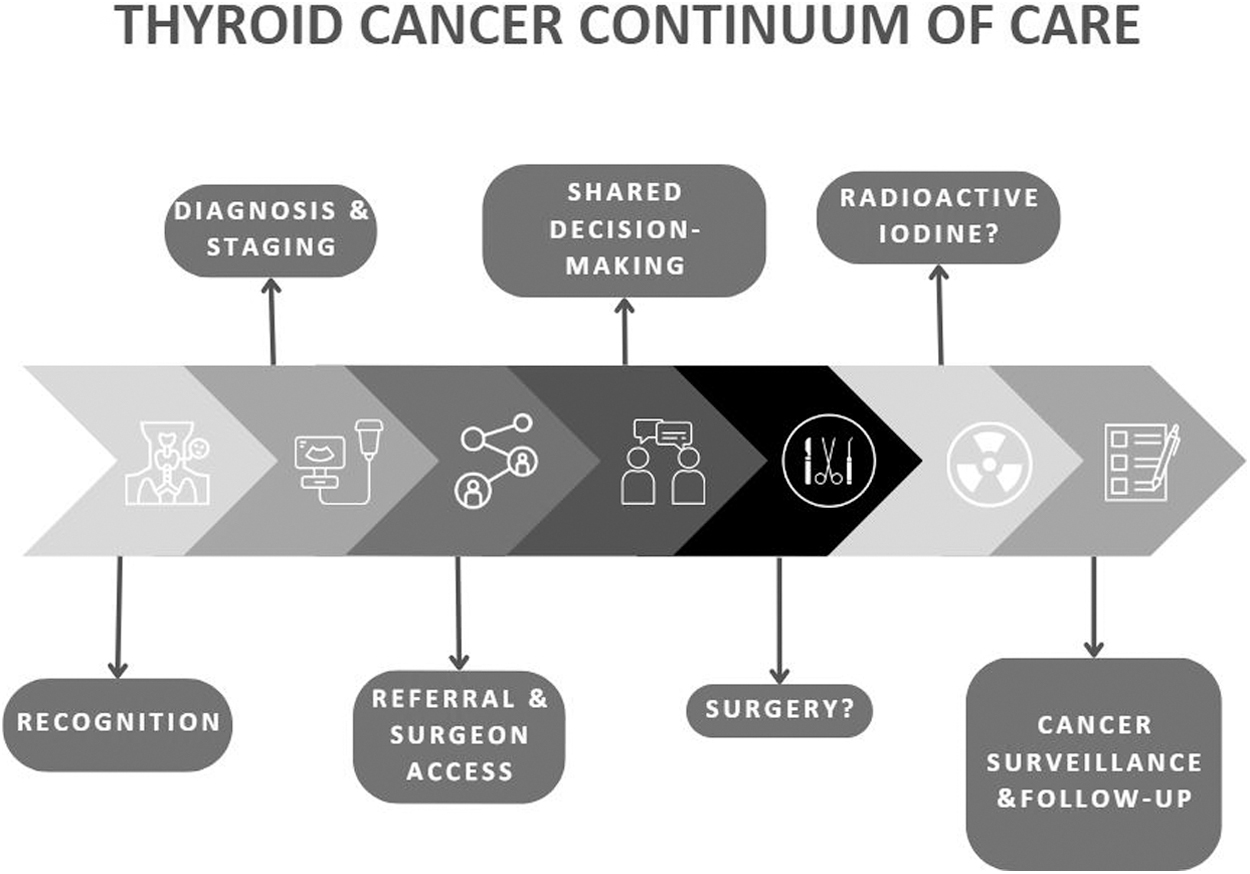
Conceptual model of the thyroid cancer continuum of care: high-quality and guideline concordant thyroid cancer care is situated along a continuum of multidisciplinary health care.
Time from diagnosis to curative-intent surgery defined by the difference between the date of diagnosis to date of either thyroid lobectomy (TL) or total thyroidectomy (TT). Receipt of surgery was binarily indicated by receipt of either TL, TT, or TT with lymph node dissection.
We performed a subset analysis of patients who received surgery to assess whether there was a higher proportion of patients undergoing completion thyroidectomies in rural and frontier areas, as this could suggest that diagnostic lobectomies were being performed more frequently, possibly due to difficulty in facilitating fine-needle aspiration (FNA) or molecular testing and requiring far more invasive means for definitive cancer diagnosis. Completion thyroidectomy was defined as receipt of two TLs, or a TL and a TT, within 6 months (90 days) of each other. Given the limited information around thyroid cancer initial management in our cancer database, including lack of information on FNA results or molecular testing, completion thyroidectomy was analyzed as a binary outcome without qualifications regarding appropriateness.
Next, we evaluated use of adjuvant RAI treatment for patients with regional disease. Based off of existing guidelines for use, 23,24 patients with well-differentiated thyroid cancer (WDTC) who had Surveillance, Epidemiology, and End Results (SEER) regional stage disease who underwent TT or two TLs within 90 days were assessed by a binary indicator of whether they received RAI therapy or not.
There are no consensus guidelines for follow-up surveillance after thyroid cancer diagnosis, 25 and prolonged intervals or no further follow-up may be appropriate for low-risk cancers after a period of time. Patients were deemed lost to follow-up if the patient was alive and there was more than 1 year since their last visit, and they were within 5 years of their thyroid cancer diagnosis. In California, hospital and facility reporting of cancer-related inpatient and outpatient visits to the CCR is required, regardless of whether it took place at the original site of diagnosis or a Commission on Cancer (CoC)-accredited facility.
Finally, overall and SEER disease-specific mortality were evaluated.
Covariates
Demographic characteristics
Patient characteristics, including age, sex, race, ethnicity, and insurance status, were analyzed. For a measure of patient SES, Yang quintiles of SES, which are area-based socioeconomic measures from American Community Survey data, were used. 26
Clinical characteristics
Clinical characteristics that lead to worse thyroid cancer outcomes were selected as covariates. These included the SEER tumor stage at diagnosis, provided by the CCR as local, regional, or distant disease and originates from the SEER site-specific guideline for staging of thyroid cancers. As a proxy for patient's overall health status, we used the Charlson Comorbidity Score, which we formed into a dichotomous variable for patients with a score of 0 versus patients with a score >1. Thyroid cancer tumor features that contribute to recurrence and mortality risk were then analyzed. These features included tumor size >4 cm, high-risk tumor histology (anaplastic, poorly differentiated, high-risk variants of papillary and follicular cancer, and medullary thyroid cancer), extrathyroidal extension and lymphovascular invasion.
Finally, we utilized treatment at a CoC registered facility as a clinical covariate because of mixed evidence that this may improve cancer outcomes for rural cancer patients. 27 Notably, CoC accreditation standards do not include standards for thyroid cancer.
Statistical analysis
To evaluate the variations in the thyroid cancer continuum of care for patients by rurality, demographic and clinical characteristics were summarized using descriptive statistics to characterize the study population, with the results stratified by rurality (urban, rural, and frontier). The outcomes comprising the thyroid cancer continuum of care were analyzed separately. The unadjusted outcomes for urban, rural, and frontier patients were reviewed, and then we used three separate regression modeling steps to assess if demographic factors, clinical factors, or a combination of the two were driving any observed disparities along the thyroid cancer continuum of care. Logistic regression models were used to evaluate the association between rurality and binary thyroid cancer care outcomes such as completion thyroidectomy, adjuvant RAI treatment in the appropriate patient, and active follow-up.
To analyze the time to surgery, death, and thyroid cancer-specific mortality, we used Cox proportional hazards models. Adjusted rates of odds ratio (OR) and hazard ratio (HR) between different rurality levels and their corresponding confidence intervals (CIs) were presented. p-Values <0.05 were considered statistically significant.
Results
Demographics characteristics
We studied 92,794 patients with thyroid cancer (65,475 women [70.6%]; mean age 50.0 years). Our sample comprised 82,045 urban patients (88.4%), 10,341 rural patients (11.1%), and 408 frontier patients (0.4%) (Fig. 1). Compared to urban patients, patients in rural and frontier areas were more likely to be American Indian, slightly older, uninsured, and from lower quintiles of socioeconomic status (p < 0.01) (Table 1). There was no statistically significant difference in lead-times between the urban, rural, and frontier cohorts followed by the CCR.
Demographic and Clinical Characteristics of Study Population, by Rurality
CoC, Commission on Cancer; ETE, extrathyroidal extension; FTC, follicular thyroid cancer; HMO, Health Maintenance Organization; LVI, lymphovascular invasion; NOS, not otherwise specified; PPO, Preferred Provider Organization; PTC, papillary thyroid cancer; SD, standard deviation; SEER, Surveillance, Epidemiology, and End Results; WDTC, well-differentiated thyroid cancer.
Clinical characteristics
There was no statistically significant difference in baseline health between the cohorts, as indicated by the Charlson Comorbidity Index (Table 1). Distant disease at diagnosis was more common in rural (56.0 vs. 50.4 cases per 1000 new cases) and frontier patients (80.9 vs. 50.4 per 1000) compared to urban patients. The incidence of medullary thyroid cancer was greater in rural patients (17.9 vs. 13.6 cases per 1000) and frontier patients (31.0 vs. 13.6 per 1000) compared to urban patients. The incidence of anaplastic thyroid cancer was higher in frontier versus urban patients (15.5 vs. 7.1 per 1000). Rural and frontier patients were more likely to be diagnosed and treated at CoC-registered facilities (p < 0.01) (Table 1).
Thyroid cancer continuum of care and adjustment for demographic and clinical covariates
Time to surgery
On both adjusted and unadjusted analysis, patients in rural and frontier areas had different but likely clinically insignificant mean times from diagnosis to surgery when compared to their urban counterparts (Table 2).
Unadjusted Outcomes Along the Thyroid Cancer Continuum of Care by Rurality
Patient received a thyroid lobectomy, total thyroidectomy, or total thyroidectomy with lymph node procedure.
Indicated patients who received either two thyroid lobectomies, or a lobectomy and a total thyroidectomy, within 90 days of each other.
Patients who had either a total thyroidectomy or completion thyroidectomy and had SEER regional-stage disease were considered to have an indication.
Patients diagnosed in the last 5 years of the study with any follow-up visit in the last 1 year of the study were considered to have active follow-up.
IQR, interquartile range; RAI, radioactive iodine.
Receipt of surgery
On unadjusted analysis, patients in rural, but not frontier areas were more likely to receive surgery for any diagnosis of thyroid cancer (HR 1.13 [CI 1.10–1.15]). After adjustment for clinical and demographic characteristics, this trend remained (Figs. 3 and 4).

Unadjusted and adjusted odds ratios and hazards ratios of the thyroid cancer continuum of care outcomes, comparing rural versus urban: modeling steps account for clinical and demographic characteristics in isolation (Model 1 and Model 2), followed by a multivariable regression for both clinical and demographic characteristics (Model 3). aAdjusted odds ratios; badjusted hazards ratios; csocioeconomic status quintile; dCommission on Cancer; eSurveillance, Epidemiology, and End Results; fCharlson Comorbidity Index; gextrathyroidal extension; hlymphovascular invasion; ianaplastic, poorly differentiated, high-risk variants of papillary and follicular thyroid cancer, and medullary thyroid.
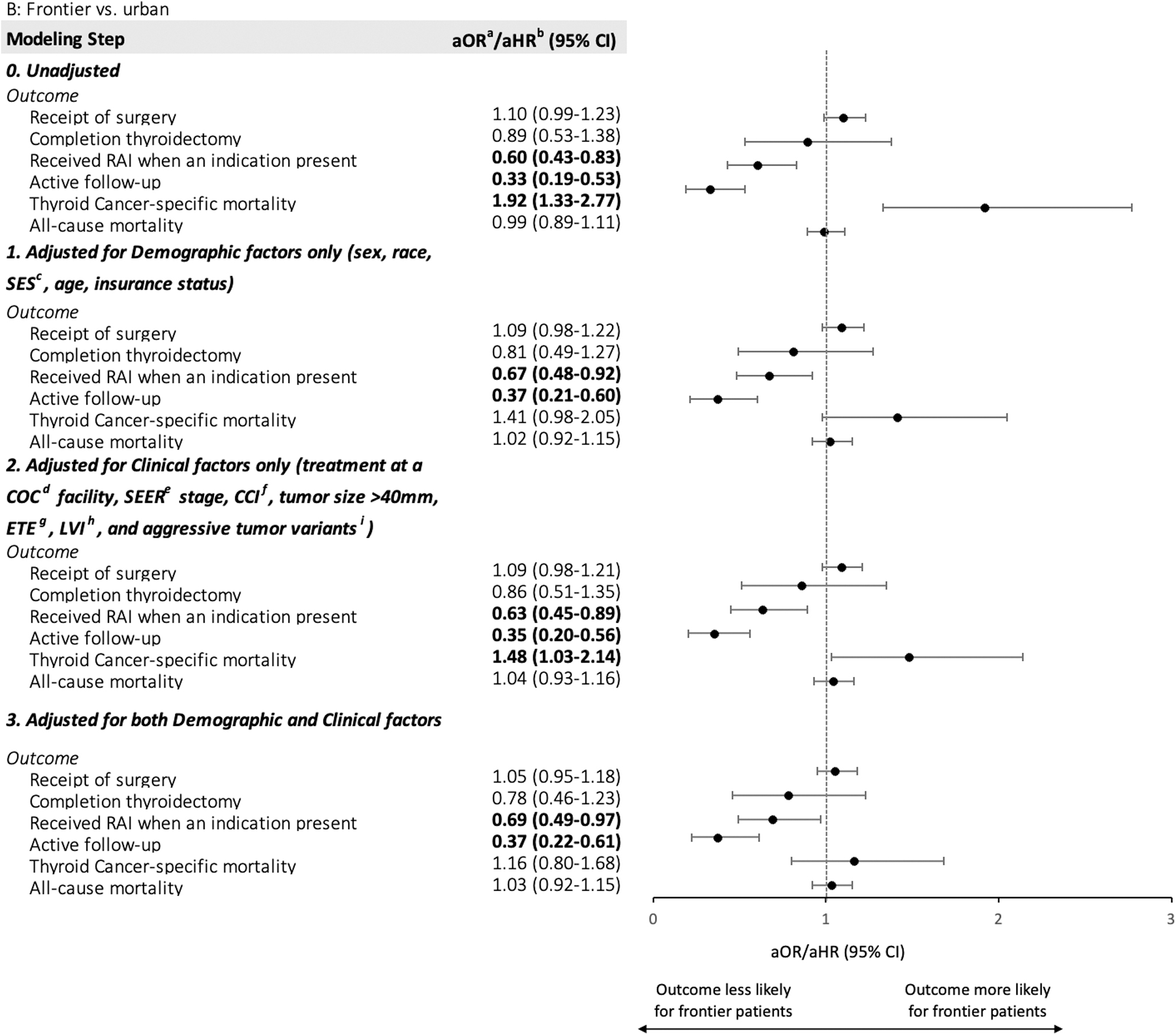
Unadjusted and adjusted odds ratios and hazards ratios of the thyroid cancer continuum of care outcomes, comparing frontier versus urban: modeling steps account for clinical and demographic characteristics in isolation (Model 1 and Model 2), followed by a multivariable regression for both clinical and demographic characteristics (Model 3). aAdjusted odds ratios; badjusted hazards ratios; csocioeconomic status quintile; dCommission on Cancer; eSurveillance, Epidemiology, and End Results; fCharlson Comorbidity Index; gextrathyroidal extension; hlymphovascular invasion; iAnaplastic, poorly differentiated, high-risk variants of papillary and follicular thyroid cancer, and medullary thyroid.
Rates of completion thyroidectomy
On unadjusted analysis, there was a small increased likelihood of receiving a completion thyroidectomy in rural areas versus urban (OR 1.13 [CI 1.03–1.23]); after adjusting for clinical and demographic characteristics, there was no observed difference (Figs. 3 and 4).
Appropriate use of RAI ablation
On unadjusted analysis, when compared to urban patients, rural patients who underwent TT with regional disease had similar odds of receiving adjuvant RAI treatment. Meanwhile, compared to urban patients, frontier patients who underwent TT with regional disease were less likely to receive adjuvant RAI treatment (OR 0.60 [CI 0.43–0.83]). After adjusting for both demographic and clinical covariates, frontier patients still had significantly lower odds of receiving adjuvant RAI treatment (Figs. 3 and 4).
Appropriate follow-up
On unadjusted analysis, among patients with thyroid cancer diagnosed in the last 5 years of the study (11,316 urban patients, 1650 rural patients, and 85 frontier patients), patients in rural and frontier areas were much less likely to receive active follow-up (OR 0.59 [CI 0.54–0.65], and OR 0.33 [CI 0.19–0.53], respectively). These findings did not appear attributed to either the demographic or clinical covariates of rural and frontier residence and appeared to be strongly determined by rurality on adjusted analysis (Figs. 3 and 4).
Thyroid cancer specific- and all-cause mortality
Rural, frontier, and urban patients with thyroid cancer had similar rates of all-cause mortality (Table 2). However, disease-specific mortality was significantly higher for rural and frontier patients (HR 1.18 [CI 1.07–1.30], and HR 1.92 [1.22–2.77], respectively) (Figs. 3 and 4). On adjusted analysis, this finding appeared to be attributed most significantly to the demographic characteristics of rural and frontier residence and less to the previously noted clinical characteristics such as higher stage disease at presentation and higher rates of aggressive tumor variants (Figs. 3 and 4). On analysis of patients with only WDTC, excluding aggressive histologic variants, this mortality disparity remained (Fig. 5).
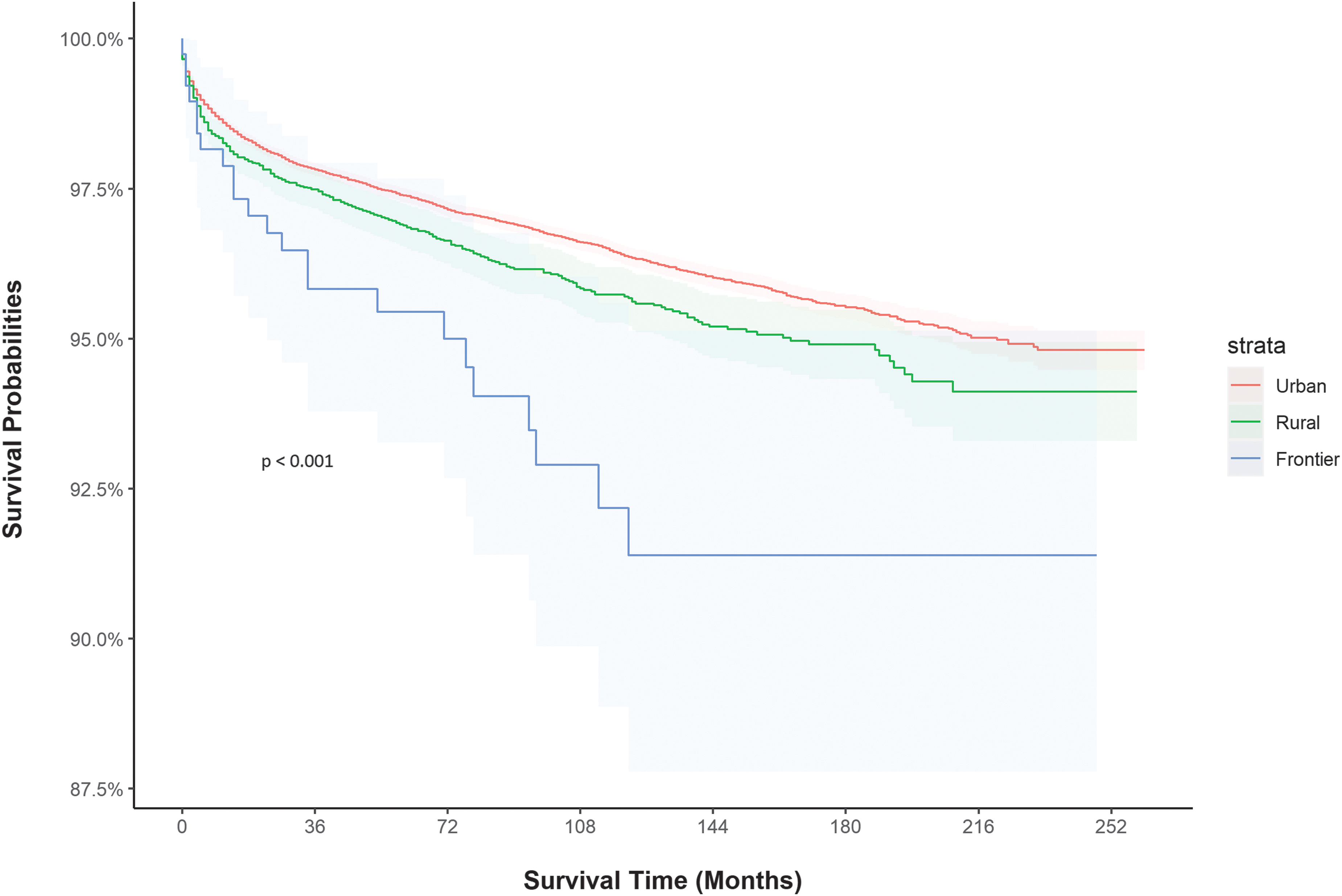
Kaplan-Meier curve for thyroid cancer-specific morality for patients with well-differentiated thyroid cancer over the study period (1999–2021) by rurality.
Discussion
In our patient cohort, rural and frontier patients with thyroid cancer were more likely to have a subset of high-risk tumor features, be diagnosed with distant disease, be lost to follow-up, and have significantly higher disease-specific mortality.
These findings contribute to the literature in important ways. Studies have reported isolated findings regarding rural-urban differences in the continuum of thyroid cancer care, but none to our knowledge has conceptualized the treatment course as a continuum along which rural patients experience disparate outcomes. Prior work has shown that rural patients are less likely to be diagnosed with thyroid cancer than their urban counterparts. 19 A recent retrospective cohort study showed differences in rates of TL and TT by geographic location. 28 Thyroid cancer patients residing in low SES neighborhoods and nonmetropolitan areas have lower cancer-specific survival after adjusting for stage at time of diagnosis. 29 A Canadian study of patients across two institutions showed that patients with lower SES are more likely to present with later-stage disease at diagnosis. 30 There are well-known cancer inequities faced by American Indian people, but these have not been described for thyroid cancer. 31
Rural populations sit at the nexus of social marginalization and economic deprivation in the United States. Overall health of rural residents is poorer: compared to people living in nonmetro areas, they have a shorter life expectancy and higher prevalence of chronic diseases like obesity and diabetes. 32 They are more likely to be uninsured and experience poverty. 32 This study was the first of its kind to attempt to disentangle the clinical and demographic characteristics of the rural thyroid cancer patient to assess their contributions to disparities in the thyroid cancer continuum of care.
Rural and frontier patients are more likely to present with distant disease and a subset of aggressive tumor variants. Since there is no recommended population-level screening for thyroid cancer, early detection of thyroid cancer is contingent on a patient's timely access to care, including to diagnostic imaging through ultrasound, and diagnosis with FNA. Therefore, it is reasonable to conclude that rural patients, more commonly uninsured and with poorer access to specialist services, are likely to be underdiagnosed with WDTC when compared to their urban counterparts. 19 The supply of and access to primary care physicians is also more limited in rural settings, leading to the delayed detection of early WDTC on physical examination and ultrasound.
We found that patients in rural areas were receiving surgery for thyroid cancer more frequently. Prior literature on breast cancer has demonstrated that rural patients undergo more aggressive surgical treatment the longer the distance traveled for treatment. 33 Additional qualitative research needs to be done with both rural thyroid cancer patients and the multidisciplinary teams that treat them to assess the key drivers of this trend.
Our study found that frontier patients with WDTC and regional disease were receiving adjuvant RAI treatment at significantly lower rates. Referral to and receipt of RAI requires specialty nuclear medicine services and the patient's ability to isolate. Further work may seek to understand how frontier patients may better access this important step in their care, particularly with the geographic and socioeconomic constraints they face. There are inherent constraints in the use of cancer databases, including the inability to factor in shared decision-making models where therapies are omitted.
In addition, rural and frontier patients are more frequently lost to follow-up. Geographic isolation may pose a significant barrier to regular follow-up. Patients who do not follow-up and develop recurrent disease may lose their window of opportunity for treatment, resulting in worse mortality rates. Lack of access to specialists, including surgeons and endocrinologists, may be a key driver of this trend. 34
Rural and frontier patients with WDTC had significantly higher rates of thyroid cancer-specific mortality. Despite being treated at CoC-registered facilities more commonly than their urban counterparts, rural and frontier patients had worse disease-specific mortality. Unnecessary referral out of the community, and subsequent travel to CoC-registered facilities may require further travel for these patients, which may discourage follow-up and result in higher mortality. Indeed, care fragmentation is a recognized contributor to thyroid cancer mortality. 35 This highlights the importance of targeted interventions, through local health systems and affiliate networks, to address the unique needs of rural thyroid cancer patients. 36 Recent work suggests that at centers treating more than five cases of thyroid cancer a year, there is no difference in surgical complications, reoperation for recurrent disease, or guideline-concordant use of RAI. 37 This indicates that excellent thyroid cancer outcomes can often be achieved locally, even in rural areas.
We acknowledge several limitations to our study. Thyroid cancer presents an epidemiologic conundrum for the health services researcher. Routine screening is not recommended by the United States Preventive Services Taskforce, and 5-year survival for WDTC approaches 100%. 38 For these reasons, many undiagnosed cancers remain indolent, and may only be diagnosed at much later stages. Accurate incidence and prevalence figures are also confounded by trends of overdiagnosis of thyroid cancer. 18,39,40 Although some of the study's findings regarding the prevalence of distant disease and aggressive tumor variants may be driven by a denominator with fewer WDTCs in rural and frontier areas, our modeling demonstrates that these clinically more aggressive cancers are not fully accounting for the observed disparities in outcomes. In addition, we cannot exclude the possibility that environmental exposures in rural and frontier areas are leading to more aggressive cancers. 41 –44
Conclusion
Despite high 5-year survival for patients with WDTC, patients in rural and frontier areas with thyroid cancer have higher disease-specific mortality. Disparities may be attributed to various inequities and disparities throughout the thyroid cancer continuum of care, including later disease stage at diagnosis and high rates of loss to follow-up. Rural patients with thyroid cancer should be considered a unique patient population: there is room for improvement in earlier detection of disease as well as in ensuring appropriate follow-up to mitigate some of these observed disparities.
Footnotes
Acknowledgments
To Dr. Utibe Essien for input on disparities methodology. This work was presented as an oral presentation in the Disparities and Health Equity Session on September 2, 2023 at the 2023 American Thyroid Association Annual Meeting.
Authors' Contributions
H.H.H.-P.: conceptualization, methodology, and writing—original draft. Y.M.: writing—original draft, review, and editing. C.-H.T.: methodology and formal analysis. J.K.: methodology and formal analysis. I.B.: writing—review and editing. J.X.W.: methodology and writing—review and editing. M.W.Y.: supervision, methodology, and writing—review and editing.
Disclaimer
The contents do not represent the views of the U.S. Department of Veterans Affairs or the United States Government.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
H.H.H.-P. was supported by the VA Office of Academic Affiliations through the National Clinician Scholars Program.