
Abstract
Background:
The impact of near-infrared autofluorescence (NIRAF) imaging on postthyroidectomy hypocalcemia is controversial. As patients with Graves' disease are at increased risk, our aim was to compare postoperative parathyroid function in these patients undergoing total thyroidectomy (TT) with or without NIRAF imaging.
Methods:
This was a retrospective “before and after” study, comparing outcomes of patients who underwent TT without or with NIRAF imaging at a single center. Primary outcome was the incidence of temporary hypocalcemia and secondary outcomes, rates of incidental parathyroidectomy on final specimens and permanent hypocalcemia. Analyses were performed using Mann-Whitney U and chi-Square tests. Continuous data are expressed as median (interquartile range).
Results:
There were 85 patients in NIRAF and 100 patients in non-NIRAF group. Groups were comparable regarding age, gender, body-mass index, and thyroid weight. Number of parathyroid glands identified intraoperatively was 3 in both groups (p = 0.47). Intraoperative parathyroid implantation rate was 16.5% in NIRAF and 6% in non-NIRAF group (p = 0.02). Incidental parathyroidectomy rate on final pathology was 12.9% in NIRAF and 32% in non-NIRAF group (p = 0.002). The rates of temporary (11.7% vs. 16%) and permanent hypocalcemia (2.4% vs. 2%) were similar between the two groups, respectively (p = 0.66).
Conclusion:
To our knowledge, this is the first comparative study investigating the impact of NIRAF on postoperative parathyroid function after thyroidectomy for Graves' disease. The rate of incidental parathyroidectomy on final pathology was lower with use of NIRAF, without an impact on temporary or permanent hypocalcemia rates compared to conventional technique.
Introduction
Near-infrared autofluorescence (NIRAF) imaging, which was introduced in 2011, has given surgeons an adjunctive tool for parathyroid identification during thyroidectomy and parathyroidectomy procedures. 1 Since then, a significant research effort has started worldwide to identify best indications to use this technology in endocrine surgical procedures. 2,3 One of the first questions that has attracted significant interest is whether this technology could have a utility in preserving parathyroid function after total thyroidectomy (TT) by improving identification of parathyroid glands (PGs). Studies have shown that the use of this technology increased surgeon awareness to identify PGs, with 1/3 of PGs being detected earlier with this technology before they become apparent to the eye. 4
Nevertheless, the results of studies investigating whether incidence of hypoparathyroidism is lower with this technology compared to conventional practice have been discrepant. In two randomized studies, the incidence of temporary hypoparathyroidism in patients undergoing thyroidectomy with NIRAF was found to be lower compared to that in patients undergoing thyroidectomy without the use of this technology. 5,6 On the contrary, other studies have not demonstrated a similar benefit when using NIRAF imaging. 7,8
Among all indications, surgery for Graves' disease is particularly challenging due to the associated inflammation involved. Many studies have documented a higher incidence of temporary hypocalcemia after thyroidectomy for Graves' disease versus other pathologies (range 13.8–65% vs. 7.3–58%, respectively). 9 –14 While searching for the best indications to use NIRAF, it is important to know what the impact of NIRAF imaging could be in thyroidectomies performed for Graves' disease. At the time of this writing, our PubMed search for Graves' disease and autofluorescence did not reveal any entries.
Our objective was to determine whether the use of NIRAF during thyroidectomy for Graves' disease results in a lower incidence of postoperative hypoparathyroidism compared to conventional thyroidectomy, which does not utilize such an adjunctive technology. The primary outcome was the rate of temporary hypocalcemia and secondary outcomes were rates of permanent hypocalcemia and incidental parathyroidectomy detection on final pathology specimens.
Methods
This was a retrospective “before and after” study. An evaluation of NIRAF technology in thyroidectomy and parathyroidectomy procedures was started at the Cleveland Clinic, Department of Endocrine Surgery in August 2016. Patients enrolled in this registry had their procedures performed using a NIRAF camera (Fluobeam®, Fluoptics©, Grenoble, France) by holding it about 20 cm away from the surgical field with the room lights turned off. The technique has been described in detail before. 4 In brief, the NIRAF camera was used to identify PGs during the dissection and to detect those incidentally removed with the specimen for implantation before sending off the sterile field. Imaging was repeated at the discretion of the surgeon, taking about 30–60 seconds each time. Cleveland Clinic Institutional Review Board approval was obtained (IRB#16-460 and IRB#19-446). Patient consent was waived due to minimal risk to subjects.
For this study, patients who had TT using NIRAF between August 2016 and October 2023 (NIRAF group) were compared to a historical group of consecutive Graves' patients (n = 100) who underwent TT by the same surgeons without the use of this technology (non-NIRAF group) between April 2010 and August 2016, before this technology was available. Patient lists were obtained from a departmental database and an analysis was performed retrospectively. In both study groups, the procedures were performed by a mixture of senior (>5 years of experience) and junior (<5 years of experience) surgeons at the same department of endocrine surgery. All of the surgeons were members of the American Association of Endocrine Surgeons.
All patients were prepared for thyroidectomy with 10 days of potassium iodide oral solution. The procedures were done under general anesthesia using a Kocher incision. Surgical loupes were worn by the surgeons routinely. All patients were discharged home on postoperative day (POD) 1 with 500 mg Ca to be taken PO TID. In those patients with hypocalcemia, additional prn doses of oral Ca (500–1000 mg/h) were administered. Serum Vitamin D 25-OH and Vitamin D 1,25-OH levels were also checked in the presence of postoperative hypocalcemia and repleted if low.
None of the patients had an underlying kidney failure or had undergone bariatric surgery.
Data collected included demographic and clinical details; age, biologic sex, body-mass index (BMI), thyroid weight, biochemistry, thyroid scan results, previous treatments, operative time, number of PGs identified intraoperatively (including those on the specimen intraoperatively), number of PGs identified first with NIRAF, number of patients in whom intraoperatively PG implantation was done, incidental parathyroid tissue detected in final pathology report, POD 1 serum calcium, POD 1 serum parathyroid hormone (PTH), and six-month follow-up serum calcium and PTH levels. Hypocalcemia was accepted as serum calcium <8 mg/dL. Temporary hypocalcemia was defined as lasting less than six months and permanent hypocalcemia as persisting beyond six months. The groups were compared using Mann-Whitney U and chi-square analysis using JMP®, Version 17.1.0 (SAS Institute, Inc., Cary, NC, 1989–2023).
Continuous data are expressed as medians interquartile range (25th to 75th percentile). Statistical significance was accepted as p-value <0.05. A post hoc analysis was performed to study the correlation between the incidence of parathyroid tissue detection on final pathology and postoperative serum calcium levels and hypocalcemia rates. However, this post hoc analysis was not used to generate any hypothesis.
Temporary hypocalcemia was taken as the primary outcome of the study, as reported in a number of randomized studies investigating the impact of NIRAF on postthyroidectomy parathyroid function in the literature. 11,15 The rate of temporary hypocalcemia has been reported to range between 12% and 72% after thyroidectomy for Graves' disease in the literature. 9,14,16,17 A sample size calculation accepting a 30% incidence of temporary postoperative hypocalcemia after TT for Graves' disease, predicting a reduction to 10% with the use of NIRAF, using an α error of 0.05 and a β error of 0.20 revealed 72 patients in each group. Secondary outcomes included the rate of permanent hypocalcemia and incidental parathyroid tissue detection on final pathology specimens.
Results
There were 85 patients in the NIRAF and 100 patients in non-NIRAF group. Table 1 shows the demographic and clinical characteristics of the study patients. Between the NIRAF and non-NIRAF groups, respectively, patient age [46.0 (31.0–59.0) years vs. 41.5 (29.3–53.8) years, p = 0.17], biologic sex (male: 16 vs. 15, female: 69 vs. 85, p = 0.49), BMI [29.7 (25.0–34.2) kg/m2 vs. 29.3 (25.6–35.3) kg/m2, p = 0.81], and thyroid weight [34.0 (21.3–58.9) g vs. 31.7 (18.0–57.0) g, p = 0.93] were similar.
Demographic and Clinical Details of Study Patients
Continuous variables are given as medians interquartile range (25th to 75th percentile).
BMI, body mass index; NIRAF, near-infrared autofluorescence; TSH, thyrotropin.
The median number of PGs identified per operative report was the same in NIRAF (n = 3) and non-NIRAF groups (n = 3) (p = 0.47). In the NIRAF group, 18.3% (n = 44) of glands were identified first with their bright autofluorescence before they became apparent to the eye (Fig. 1).

Identification of PGs (arrows) with NIRAF during thyroidectomy before they become apparent to the eye. The first part of the figure (
Intraoperative parathyroid implantation rate was higher in the NIRAF versus the non-NIRAF group (16.5%, 6%, p = 0.02), with more incidental parathyroidectomy detected during the dissection and salvaged with implantation in the NIRAF group (Fig. 2). In the NIRAF group, 57.2% (n = 8) of the intraoperative implantations were performed for glands identified to be devascularized in situ and 42.8% (n = 6) for glands incidentally removed on the specimen; whereas, in the non-NIRAF group, 100% of the implantations were performed for the former scenario (Table 2). Incidental parathyroid tissue was detected less often on final pathology in the NIRAF (12.9%) versus non-NIRAF group (32%), (p = 0.002).
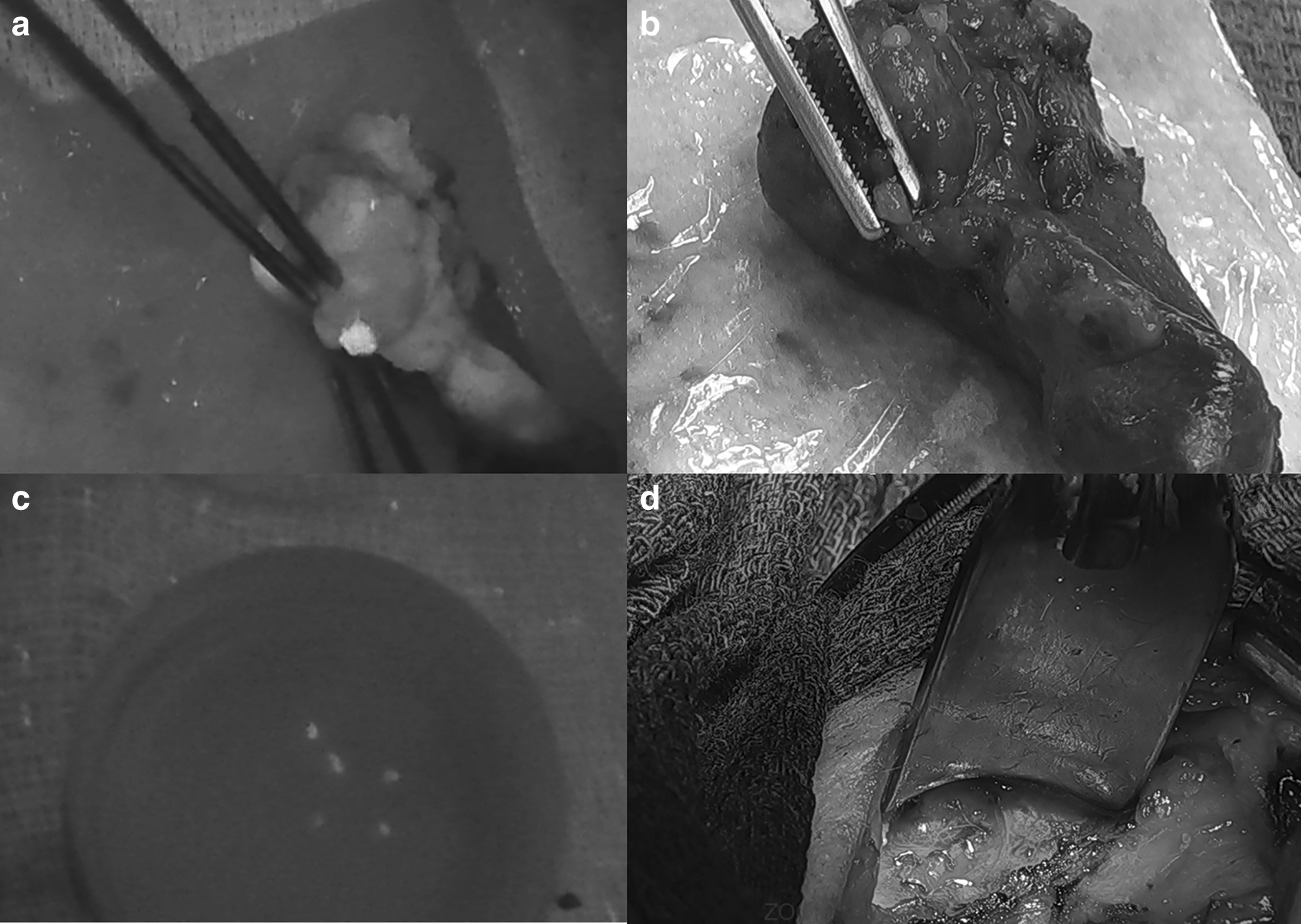
Identification of incidental parathyroid tissue on thyroidectomy specimen on the sterile field (
Perioperative Outcomes of Study Patients
Continuous variables are given as medians interquartile range (25th to 75th percentile).
POD, postoperative day; PTH, parathyroid hormone.
For the NIRAF versus non-NIRAF groups, the rate of neither temporary (11.7%, 16%, respectively, p = 0.66) nor permanent hypocalcemia rates (2.4%, 2%, respectively, p = 0.66) were different. Table 2 summarizes the study outcomes between the two groups. On POD 1, serum calcium and PTH levels were 9.0 (8.6–9.4) and 8.6 (8.1–9.1) mg/dL (p < 0.0001) and 21.0 (9.0–35.0) and 16.0 (10.0–28.3) pg/mL, respectively, (p = 0.31) for the same groups.
There was an inverse relationship between the presence of incidental parathyroid tissue on final pathology and POD 1 serum calcium levels (p = 0.001) (Supplementary Fig. S1). Furthermore, the rate of hypocalcemia was lower in patients in whom parathyroid tissue was present (30.2%) compared to those in whom parathyroid tissue was absent (12.6%) on final pathology (p = 0.01).
Discussion
To the best of our knowledge, this is the first dedicated study in the literature investigating the utility of NIRAF in thyroidectomy performed for Graves' disease. Our results show that in thyroidectomies performed with versus without NIRAF, there was an increased ability to avoid incidental removal of PGs in the specimen, although this did not translate into differences in temporary or permanent hypocalcemia rates. These results mirror our findings in patients undergoing thyroidectomy for all indications with or without NIRAF. 8
Graves' disease is known to increase the risk of complications after thyroidectomy. In a report of 17,906 patients who underwent thyroidectomy in the National Surgical Quality Program, 30-day incidence of both hematoma (3.1% vs. 1.9%, p = 0.01) and hypocalcemia (13.8% vs. 7.3%, p < 0.01) were increased in Graves' versus other patients. 17 Graves' disease has been reported to be associated with more bleeding during manipulation of the thyroid gland. 9 Furthermore, there are more adhesions between the PGs and the thyroid capsule in these patients. As a result, there is a higher risk of injury to the PGs and their vasculature during thyroidectomy.
In the current study, there was an increased ability to recognize PGs at risk for both devascularization and incidental removal with NIRAF compared to the conventional technique, as highlighted by the higher rate of intraoperative implantation (16.5% vs. 6%) and lower incidence of detection on final pathology specimens (12.9% vs. 32.0%). Previous studies have shown the presence of PGs in thyroid specimens to be predictive of postoperative hypocalcemia. Furthermore, a correlation between presence of parathyroid tissue on final thyroidectomy specimen and incidence of hypocalcemia on POD 1 was shown in Graves' patients undergoing thyroidectomy. 9 The findings of the current study are in parallel, with the incidence of postoperative hypocalcemia being 30.2% in those patients in whom parathyroid tissue was detected on final pathology versus 12.6% in those in whom parathyroid tissue was not detected.
As a result, despite not showing statistically significant differences in temporary or permanent hypocalcemia rates, thyroidectomy with versus without NIRAF seems to increase the ability to preserve PGs and minimize the risk of incidental removal in specimens.
As NIRAF use in thyroidectomy is generating a big interest in the surgical community, a few randomized studies have already been performed to assess the utility with regard to improving outcomes. 5,18,19 The first such study did not demonstrate any differences in postoperative temporary hypocalcemia rates between the NIRAF (8.2%) and non-NIRAF groups (16.5%, p = NS); 18 whereas the second study showed a lower incidence of temporary hypocalcemia (9.1% vs. 21.7%, p = 0.007) in the NIRAF versus non-NIRAF group. 5 Nevertheless, no difference in the rate of permanent hypocalcemia was demonstrated between the groups in either study that included patients with various thyroid pathologies. A most recent randomized study 19 also did not report a difference in the percentage of patients developing temporary hypocalcemia in patients undergoing TT with or without NIRAF.
It should be emphasized that a study to answer whether the rate of permanent hypocalcemia is different between NIRAF and non-NIRAF groups would need 70,000 patients for an adequate power. 8 Furthermore, NIRAF is an adjunctive tool for parathyroid identification, but does not show perfusion. Incidental parathyroidectomy rate on final pathology is an objective parameter that gives a hint about how well PGs were identified and preserved during thyroidectomies. We, as well as others have shown before that the rate of incidental parathyroid tissue detection rate on thyroid specimens is lower after thyroidectomies performed with versus without NIRAF for all pathologies. 8,19 This study further shows that the improvement in incidental parathyroid tissue detection rates on thyroid specimens with versus without NIRAF was more extensive for Graves' patients (down to 12.9% from 32.0%) versus for patients with all indications (down to 13% from 23%) in our previous report. 8
There are certain limitations of the current study. Despite being the largest study in the literature focusing on the use of NIRAF in Graves' patients, the sample size was still small to detect differences in permanent hypocalcemia rates between the groups. Furthermore, the results reflect the experience of high-volume surgeons who were skilled in identifying and managing PGs and therefore may not apply to lower volume practices. However, less experienced surgeons have been advocated to benefit most from NIRAF in previous studies done with both probe-based 20 and image-based systems. 8
Conclusion
In conclusion, we report the first dedicated study on the impact of NIRAF on parathyroid function after thyroidectomy performed for Graves' disease. There was an increased ability for intraoperative preservation of PGs and lesser incidence of incidental parathyroid tissue identification on final pathology with the use of NIRAF, without an impact on temporary or permanent hypocalcemia rates. We suggest the design of future multicenter studies focusing on less experienced surgeons to further investigate the impact of NIRAF imaging on parathyroid function in patients undergoing thyroidectomy for Graves' disease.
Footnotes
Authors' Contributions
E.B. and M.U. designed review of results and preparation of the article. E.A. and A.G.S. helped with the collection and analysis of data.
Author Disclosure Statement
E.B. has been a consultant for Fluoptics since April 2023. He also has unrelated consulting agreements with Ethicon, Medtronic, Aesculap, Progenics, and Intuitive, which he has received honoraria from. The other authors do not have any disclosures.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1