
Abstract
Background:
As thyroid cancer incidence rises, it is increasingly valuable to recognize disparities in treatment and diagnosis. Prior investigations into social determinants of health (SDoH) are limited to pediatric populations or studies looking at single factors such as race or environmental influences. Utilizing the CDC-social vulnerability index and SEER-patient database to assess the amalgamated, real-world influence of varied SDoH and their quantifiable impact on thyroid cancer disparities across the United States.
Methods:
In a retrospective cohort study, 199,340 adult thyroid cancer patients from 1975 to 2017 were assessed for significant regression trends in months of follow-up/surveillance, survival, late staging, and treatment receipt across thyroid cancer-subtypes with increasing overall social vulnerability, as well as in 15 SDoH variables regarding socioeconomic status, minority-language status, household composition, and housing-transportation across all the U.S. counties while accounting for sociodemographic regional differences.
Results:
With increasing overall social vulnerability, decreases in months of follow-up were observed with patients with papillary, follicular, medullary, oncocytic, and anaplastic thyroid cancer (p = 0.001). Comparing lowest with highest vulnerability cohorts, relative decreases in months of surveillance ranged from 55.6% (14.5–6.5 months) with anaplastic to 17% (108.6–90.2) with oncocytic. Socioeconomic status vulnerabilities, followed by vulnerabilities in household composition and housing-transportation type, contributed to these overall trends. Similar survival decreases occurred across all thyroid cancer patients, ranging from 55.9% (9.6–4.2) with anaplastic to 28.3% (97–69.5) with oncocytic. Minority-language status vulnerabilities and housing-transportation types largely contributed to these trends. Increasing overall vulnerability was associated with increased odds of advanced staging for papillary (odds ratio [OR] = 1.07 [confidence interval, CI 1.03–1.12]) and decreased odds of indicated treatment via surgery (lowest, medullary: 0.91 [CI 0.84–0.99]), radiation therapy (lowest, anaplastic: 0.88 [CI 0.82–0.93]), and chemotherapy (lowest, oncocytic: 0.81 [CI 0.67–0.98]) were observed. Vulnerabilities in minority-language status and housing-transportation, followed by socioeconomic status vulnerabilities, were differential contributors to these overall vulnerability trends.
Conclusions:
Our results show significant detriments in thyroid cancer care and prognosis in the United States with increasing overall social vulnerability while identifying which SDoH quantifiably contribute more to disparities in inter-relational, real-world-like contexts.
Introduction
The incidence of thyroid cancer continues to rise worldwide, increasing by 211% between 1975 and 2013 and comprising the seventh-most common cancer worldwide. 1 –5 Despite the increasing access to diagnostics, which is considered to be the main reason underlying increasing incidences of thyroid cancer worldwide, there continues to be an alarming disproportionate burden of illness among medically underserved populations and minority populations, 6,7 Social determinants of health (SDoH), defined as the conditions that impact health outcomes based on differing environmental factors of where people are born, live, and function, have been shown to play a role in cancer progression through chronic psychosocial stress, socioeconomic factors, or neighborhood disadvantage. 7 –9
In addition to SDoH, current studies show varying prognoses among histopathologic types. Disparities in survival outcomes have been investigated for patients who not only present with advanced-stage disease, but also with SDoH such as socioeconomic status, race/ethnicity, and others. 10 –14 For example, Garner et al. identified significant disparities in treatment among 9585 well-differentiated thyroid carcinoma (WDTC) patients based on if they were uninsured, on Medicaid, or private insurance. 15 Roche et al. also noted that, among 1647 medullary thyroid cancer patients, there was a >2-fold increase in the risk of overall mortality among black patients compared with non-Hispanic white and younger patients. 10 Moreover, in a study with 1317 WDTC patients, Swegal et al. identified that adults from a lower socioeconomic background are more likely to present with higher stage and worse overall survival. 16
Despite these prior investigations, SDoH inquiries are yet to be conducted on larger cohorts of patients diagnosed with thyroid carcinomas. Furthermore, they are yet to examine a wider range of SDoH and how they interact to influence thyroid cancer disparities in real-world, nationwide contexts.
The Center for Disease Control-social vulnerability index (CDC-SVI) is a U.S. census-based tool of four SDoH-related themes that are measured across all U.S. census tracts and counties (Supplementary Fig. S1). 17 These themes comprise 15 different SDoH-factors that are amalgamated into categories of socioeconomic status, minoritized race/ethnicity and language status, household composition, and housing-and transportation status, as well as a differentially weighted, total composite of these themes. As per the CDC, 17 these metrics are scored based on relative rankings across all U.S. census tracts and/or counties and differentially adjusted to the specific surrounding contexts of each geographical area. Thus, generalized associations of a higher SVI score, indicating increasing social vulnerability, can be characterized across national patient populations specifically contextualized to their sociodemographic environments.
Prior cancer studies using the SVI have only assessed pediatric head and neck malignancies and melanoma patient populations, as well as limited investigations of care setting and postoperative disparities for various gastrointestinal and lung malignant pathologies. 18 –21 Despite this robust utility, it is yet to be applied in understanding SDoH associations of adult thyroid cancer patients.
Therefore, our study aimed to utilize the SVI and its subthemes of socioeconomic status, minority-language status, household composition, and housing-transportation to characterize the real-world associations of SDoH with care and prognostic outcomes among adults with thyroid cancer subtypes across the United States.
Materials and Methods
Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines were followed during conduct of this study. Institutional review board approval was exempted as per the investigators' institutional policies regarding publicly available, deidentified databases.
Databases
The CDC-SVI was utilized for measures across 15 SDoH, census-level factors of 4 SDoH themes. These themes encompass the following categories: socioeconomic status (poverty, unemployment, income level, high school diploma status), minority-status language (minority status, proficiency with English), household composition (household members 65+ years, household members ≤17 years, disabilities, single-parent status), and housing-transportation (multiunit structure, mobile homes, crowding, no vehicle, group quarters). Proportionalized averages were calculated for each of the four SVI themes as per the dynamic characteristics of each census-tract area and then composited into the total SVI score for each respective area.
Of note, these averages are not considered of equal weight to form the total SVI score and contain specialized proportionalization in balancing population densities and sociodemographic differences. Scores comprised a scale from 0 to 1, which corresponds with their relative percentile ranking (i.e., 0 represents 0th percentile, 1 represents 100th percentile) in comparison with all census tracts and counties across the United States.
The NCI-SEER database comprises a national scope of patients diagnosed with malignancies while containing patient characteristic information related to prognosis and care. The length of active follow-up for a primary malignancy diagnosis up until the patient's last provider interaction was delineated as “months under surveillance.” The length of time for which a patient survives and suffers a mortal outcome (whether all-cause or disease-specific) upon last provider interaction was delineated as “months survival.” As per the SEER documentation, the starting time point of these values was designated at the time of primary malignancy diagnosis; the ending time point of these values was designated as the time of last record as per a confirmed death certificate. Within SEER, multiple staging standards were utilized and recoded into a SEER-designated combined staging variable.
Specifically, various values based on iterations of American Joint Committee on Cancer (AJCC) standards that comprised the SEER-specific combined staging variable of “advanced” or “late staging” comprised “Stage IV” (and “Stage III” for anaplastic histology types), “distant [expansion],” or “distal [expansion]” under a SEER-specific combined variable to indicate “advanced” or “late-staging,” with other values under these valuables being categorized as “nonadvanced” or “early-earlier staging (Stage I–III).” Primary surgery, chemotherapy, and radiation therapy occurrence represents whether patients received their respective indicated intervention (based on PDQ® NCI guidelines) for their primary malignancy. For indicated radiation therapy receipt, radioactive iodine (RAI) was the administered modality. Sample sizes listed excluded those without necessary variables for analyses.
SVI scores were matched to SEER-patient data based on county-of-residence at the time of diagnosis. County-assigned scores comprised population density-averaged sums of each census tract within the county. A workflow diagram of this process is provided in Supplementary Figure S4.
Population definitions
SAdult (20+ years) patients diagnosed with head-neck malignancies from 1975 to 2017 were extracted from the SEER database. Thyroid malignancies were extracted using the International Classification of Diseases for Oncology, Third Edition (ICD-O-3) topographic codes [C73.9] and SEER-designated histology codes based on labeled, recoded AJCC-TNM sixth edition schema standards. These standards, rather than AJCC seventh, were chosen based on their wider availability and consistency across the chronologies, given that AJCC seventh standards were only available for post-2012 patients in the utilized SEER data set.
Statistical methods
Linear regression trends with increasing total SVI score and SVI theme subscores, as represented by increasing relative quintiles of “<20,” “20–39.99,” “40–59.99,” “60–79.99,” “80–99.99,” were assessed. These trends consisted of measures of continuous metrics regarding months surveyed and survival as per the thyroid carcinoma subtype. Mean surveillance period differences between the lowest and highest SVI-scored quintiles were calculated among these. Violin plots were also used for assessing relative sample distribution for mean surveillance months within each relative SVI quintile, as well as measuring the median interquartile range (IQR), 1.5-times the IQR, and means. Patients who were alive/lost or dead upon last follow-up were proportionalized per quintile. Mean survival period differences were analyzed similarly as above, but patients who were alive/lost upon last follow-up were excluded to extract patients who were confirmed dead upon last follow-up.
Odds of having advanced staging and or receiving indicated surgical, radiation therapy, or chemotherapy treatment were analyzed with univariate logistic regression across relative SVI quintiles. Reference groups for odds ratios and confidence intervals [CI] calculated for each of the total and SVI theme score for advanced staging and indicated treatment receipt outcomes were represented by their respective lowest SVI relative quintiles (i.e., lowest social vulnerability group), with subsequent ordinal variable values sequentially matching each increasing level of relative quintile (i.e., “<20” quintile was set as the baseline value, with increasing levels of comparator values represented on the ordinal scale of “20–39.99,” “40–59.99,” “60–79.99,” and “80–99.99” in sequence). Binary outcome delineations for advanced staging were determined on SEER-combined staging variable designations of being “Late/Advanced Staging” in comparison with “Early-Earlier Staging” occurrence.
Statistical significance was set as p-value <0.05. Two-sided p-values were reported for analyses.
Results
Out of 205,696 total patients, 199,340 adult patients with primary thyroid carcinomas were extracted and analyzed based on the availability of geographical and other clinicodemographic data. The most represented demographic characteristics were those 45–64 years of age (n = 83,457, 41.9%), female sex (n = 159,468, 75.5%), and non-Hispanic white race (n = 134,272, 67.3%). The most represented histology types were papillary (n = 175,078, 87.8%), followed by follicular (n = 13,297, 6.67%), oncocytic (n = 5048, 2.53%), medullary (n = 3979, 2.0%), and anaplastic (n = 1938, 1.0%). Other detailed demographic information can be found in Supplementary Table S1.
Thyroid-specific trends in months under surveillance by relative SVI percentile
With increasing overall social vulnerability, decreases in months of surveillance/follow-up were observed across all five thyroid carcinoma subtypes: anaplastic (p = 0.011), medullary, follicular, papillary, and oncocytic (p < 0.001 for the remaining). Comparing the lowest (i.e., least socially vulnerable overall) with the highest total SVI (i.e., most socially vulnerable overall) quintiles, the decreases in surveillance period ranged from as high as 55.6% (14.5–6.5 months) with anaplastic to as low as 17% (108.6–90.2 months) with oncocytic. Socioeconomic status, minority-language status, household composition, and housing-transportation showed variable contributions (Fig. 1).
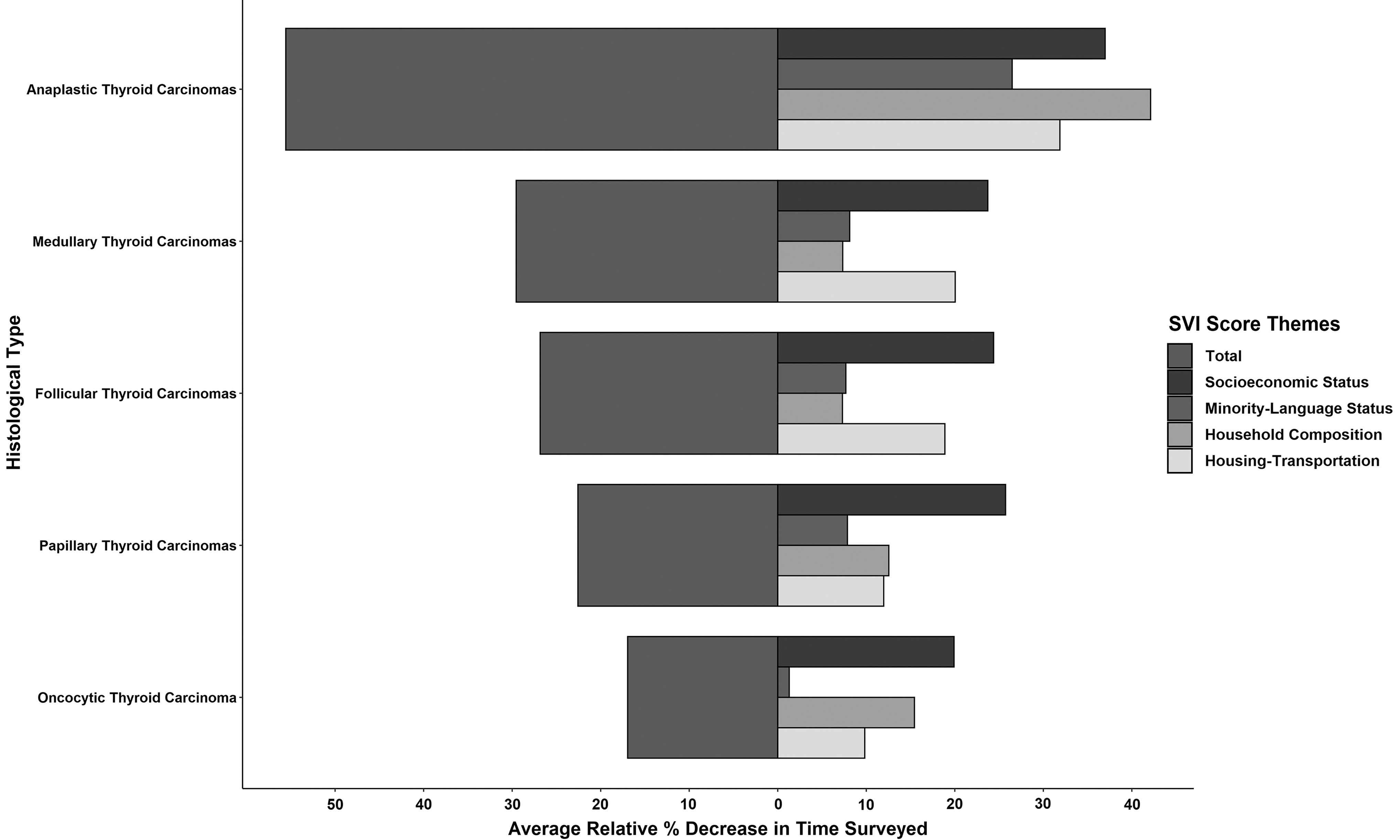
Relative decreases in months surveyed for thyroid histology types with increasing SVI scores. Percentage decreases from lowest to highest SVI quintiles based on mean months surveyed for total SVI score and subcomponent SVI theme subscores per class. SVI, social vulnerability index.
Contributing to these total SVI/overall vulnerability trends, increasing vulnerability in specific SVI themes of socioeconomic status demonstrated the highest magnitude contributions among medullary, follicular, papillary, and oncocytic carcinomas (p < 0.001 for all). In anaplastic carcinoma, household composition demonstrated the highest magnitude contribution to the total SVI score trend (p = 0.033). Minority-language status and housing-transportation showed variable magnitude contributions (Supplementary Fig. S2).
Thyroid-specific trends in months of survival by relative SVI percentile
With increasing total SVI score, significant decreases in total months survival were observed for prior mentioned thyroid carcinoma subtypes (p < 0.001 for all except p = 0.013 for anaplastic). Across thyroid carcinoma subtypes, substantial relative decrease in average months survival from the lowest to the highest total SVI quintiles ranged from as high as 55.9% (9.6–4.2 months) with anaplastic carcinoma to 28.3% (97–69.5 months) with oncocytic carcinoma. Socioeconomic status, minority-language status, household composition, and housing-transportation showed variable contributions (Fig. 2).
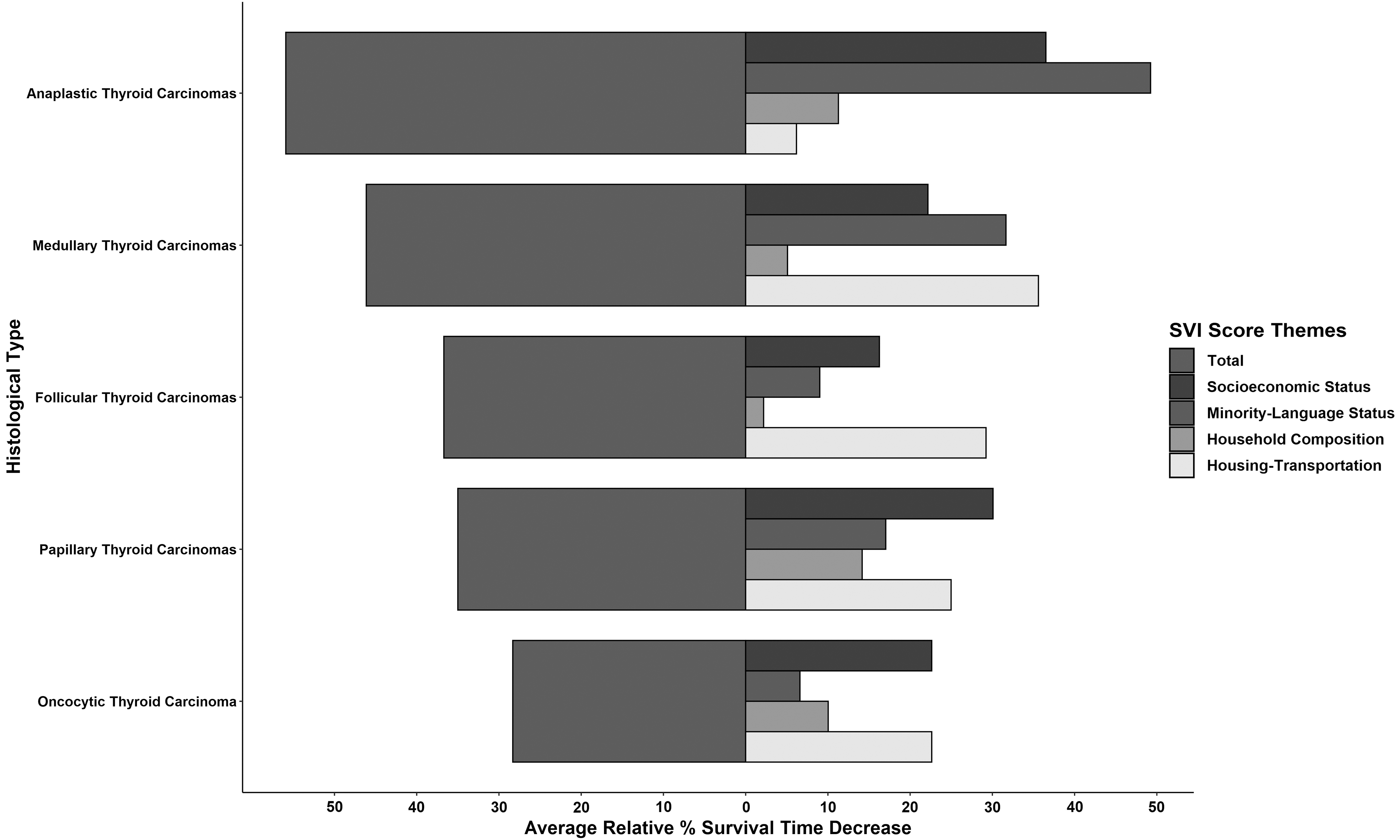
Relative decreases in months of survival for thyroid histology types with increasing SVI scores. Percentage decreases from lowest to highest SVI quintiles based on mean months of survival for total SVI score and subcomponent SVI theme subscores per class.
Contributing to the total SVI/overall vulnerability trends, increasing SVI-theme subscores in socioeconomic status demonstrated the highest magnitude contributions among papillary (p < 0.001) and oncocytic (p < 0.001) carcinomas, with housing-transportation closely following. In medullary (p < 0.001) and follicular (p < 0.001) carcinoma, housing-transportation composition demonstrated the highest magnitude contribution to the total SVI score trends. In anaplastic carcinoma (p = 0.034), minority-language status was the largest contributor to the disease's total SVI score (Supplementary Fig. S3).
Thyroid-specific analysis of advanced staging by relative SVI percentile
For patients diagnosed with various thyroid carcinoma histology types, significantly increased total odds (p < 0.001) of advanced-staging presentation were observed in patients diagnosed with papillary thyroid carcinoma with increased SVI vulnerability, with a total odds ratio of 1.07 [CI 1.03–1.12]. The total odds ratio encompassed the combined influence of socioeconomic status, minority-language status, household composition, and housing-transportation. In addition, patients with minority-language status and housing-transportation disparities had an increased incidence of those diagnosed with follicular thyroid carcinoma, with an odds ratio of 1.13 [CI 1.05–1.22] and 1.12 [CI 1.04–1.21] accordingly (Table 1).
Social Vulnerability Index-Based Analyses of Advanced Staging on Preliminary Presentation per Thyroid Histology Type
Univariate logistic regressions across SVI quintiles based on advanced staging on first presentation-occurrence for increasing total SVI score and subcomponent SVI theme subscores per histology type. Reference group for outcome combined “early-earlier staging (Stage I–III)” or “nonadvanced” to comparator group comprised “Stage IV” (and “Stage III” for anaplastic histology types), “distant [expansion],” or “distal [expansion].” Reference group for ordinal variates (total SVI and its themes), the lowest relative SVI quintile and ordinally increasing factors of sequentially more vulnerable quintiles as comparators.
By ICD-O-3.
[CI], confidence interval; ICD-O-3, International Classification of Diseases for Oncology, Third Edition; OR, odds ratio; SVI, social vulnerability index.
Across these overall social vulnerability trends of advanced staging, SVI-theme vulnerabilities in minority-language status followed by socioeconomic status and housing-transportation showed the highest magnitude, significant contributions to their respective total SVI trends (Table 1).
Thyroid-specific analysis of indicated treatment receipt by relative SVI percentile
Similarly, patients diagnosed with thyroid carcinomas with increasing total SVI vulnerability showed significantly decreased odds (at most p < 0.001) of receiving indicated primary surgical resection for those with medullary carcinoma, with a total odds ratio of 0.91 [CI 0.84–0.99], and papillary carcinoma, with a total odds ratio of 0.94 [CI 0.92–0.96] (Table 2).
Social Vulnerability Index-Based Analyses of Surgery Receipt per Thyroid Histology Type
Univariate logistic regressions across SVI quintiles based on primary tumor resection occurrence for increasing total SVI score and subcomponent SVI theme subscores per histology type. Reference group for ordinal variates (total SVI and its themes), the lowest relative SVI quintile and ordinally increasing factors of sequentially more vulnerable quintiles as comparators.
By ICD-O-3.
When analyzing indicated primary radiation therapy/RAI trends with increasing total SVI vulnerability, significantly decreased odds of receiving radiation intervention were observed with anaplastic (p < 0.001), with a total odds ratio of 0.88 [CI 0.82–0.93] (Table 3).
Social Vulnerability Index-Based Analyses of Radiation Therapy Receipt per Thyroid Histology Type
Univariate logistic regressions across SVI quintiles based on radiation therapy receipt occurrence for increasing total SVI score and subcomponent SVI theme subscores per histology type. Reference group for ordinal variates (total SVI and its themes), the lowest relative SVI quintile and ordinally increasing factors of sequentially more vulnerable quintiles as comparators.
By ICD-O-3.
When analyzing indicated chemotherapy receipt trends across thyroid carcinoma subtypes, significantly decreased odds of the intervention were observed with oncocytic carcinoma (p < 0.030), with a total odds ratio of 0.81 [CI 0.67–0.98] (Table 4).
Social Vulnerability Index-Based Analyses of Chemotherapy Receipt per Thyroid Histology Type
Univariate logistic regressions across SVI quintiles based on chemotherapy receipt occurrence for increasing total SVI score and subcomponent SVI theme subscores per histology type. Reference group for ordinal variates (total SVI and its themes), the lowest relative SVI quintile and ordinally increasing factors of sequentially more vulnerable quintiles as comparators.
By ICD-O-3.
For these overall vulnerability treatment differences, SVI theme vulnerabilities in minority-language status followed by socioeconomic status and housing-transportation featured the highest magnitude contributions to their respective total SVI trends (Tables 2 –4).
Discussion
To our knowledge, this is the first study to utilize the SVI as a comprehensive measure for evaluating SDoH across patients diagnosed with five thyroid carcinoma disease subtypes while assessing the interactions of diverse SDoH on thyroid carcinoma care and prognosis. Despite the improvements in surgical techniques, radiation modalities, and systemic therapies given to patients with thyroid carcinoma, increasing social vulnerability measured by SVI and SVI theme ranked scores showed significant detriments in overall survival and months of surveillance.
Similar to the subset analyses (Supplementary Fig. S2), our methodology allows specific diseases displaying significant overall-SDoH-disparities (measured by total SVI) to be assessed for not only which select SVI themes/SDoH categories significantly contribute to this overall disparity (i.e., socioeconomic status, housing-language status, and housing-transportation were significant contributors for patients with oncocytic thyroid carcinoma decreases in months surveilled) but also how much each SDoH contributes in the interactional context of other SDoH (i.e., socioeconomic status contributed the most to all thyroid carcinoma subtypes in months surveyed except anaplastic, as seen in Fig. 1).
Overall, many of the significant trends in months of surveillance across thyroid carcinoma diseases saw the highest magnitude decreases with an increasing socioeconomic status-SVI subscore. For months of surveillance, socioeconomic status-SVI subscore contributed substantially to the significant detriments observed with increasing total SVI score in all five thyroid carcinoma subtypes. Several retrospective studies demonstrated the influence of socioeconomic status on disease survival of thyroid carcinoma, noting that the time from diagnosis to commencing treatment was delayed in poorer populations, which may lead to prolonged treatment course, survival disadvantage, or increased therapy burden requirements. 5,15,16,22,23 Other lifestyle variables, such as increasing household composition, minority-language, and housing-transportation SVI subscores also showed varying contributions to overall vulnerability care and prognostic disparities.
Accordingly, these results correspond with prior literature regarding the influence of all four SDoH variable themes on general head and neck cancer disparities and lend credibility to our application of SVI in thyroid carcinoma disease types. 3,24,25
Unlike individual-level SDoH variables, the SVI and its community-level variables incorporate differential averages of each SVI theme subscore for calculating the composite SVI score by design. For instance, one area's total SVI could be derived from one set of particular weighted averages while another would have another set of differential “weighted” averages across SVI themes (e.g., 30% vs. 25% on socioeconomic status, 25% vs. 30% on minority-language). This feature provides the added nuance that individual-level SDoH alone cannot provide, given that patients with similar individual-level sociodemographics could have nonequivalent levels of health depending on their surrounding social environments. Such criticisms have long mired the landscape of SDoH literature, as the generalizability of past investigations focusing on a single or a small set of SDoH factors has seen equivocal utility in guiding actionable initiatives. 26,27
By capturing this sociodemographic, real-world variability, the SVI, and this analysis display dynamic, geospatial nuances for informing providers for which patient communities and their SDoH-related characteristics should equitable policy and initiatives strive to target for tackling thyroid carcinoma disparities.
Strengths and limitations
The major strengths of our study include the utilization of a novel comprehensive SDoH index that accounts for varied sociodemographic contexts to assess a variety of social vulnerabilities precisely measured by the U.S. census tracts while providing quantifiable measures that integrate the influences of varied SDoH; SVI themes highlighting which SDoH contribute the most toward total SVI trends while quantitatively accounting for sociodemographic contexts; our study encompasses five thyroid carcinoma disease types for important levels of care measurement and prognostic outcomes; lastly, being among the most comprehensive analyses to date on the national trends in SDoH for thyroid carcinoma.
However, this study has limitations. Although the SVI amalgamates measures from the U.S. census five-year summaries across a majority of the time, it does not extend across the full chronology of patients before the years of 1990, given the lacking documentation of certain variables and factors that were utilized to calculate the SVI iterations from 2000 to 2018. In addition, given that the SVI is constantly being updated both in its actual measures and formulation of categories/themes, future studies should continually provide updated associations assessed. The SEER database utilized in this study does not encompass the entirety of variables that would further characterize this study.
When analyzing thyroid carcinoma care, further clinical variables such as depth of primary invasion or therapies offered at the time of diagnosis, hospital policy variables such as use of telemedicine or interpreters for non-English-speaking patients, or individual variables such as a patient's body mass index or their racial, gender, and sexual intersectionality have been thought to affect disease progression. 23,24,28 Moreover, the database categorizes treatment modalities into overarching classifications of systemic therapies without clarifying specifications such as intravenous administration, antibody subtype, and dosage.
A major shortcoming in this analysis is the absence of such information due to the lack of data entries for the mentioned specific variables of interest or the variable itself being inaccessible, yet these variables could be influencers in driving SVI subscore trends in the overall survival and months of surveillance. These also include the restrictiveness of certain variables that prevented more nuanced analyses, including disease-specific mortality, delay of treatment, and other specific provider interactions during follow-up periods. Soliciting special authorization of other SEER databases would present future directions for addressing these gaps.
Conclusions
Through interactional analyses of the SVI, this study highlighted unique quantitative interpretations of how varied SDoH coalesce to dynamically influence aspects of care and prognostic differences among adult patients diagnosed with thyroid cancer. Beyond affirming prior SDoH thyroid carcinoma studies, this interactional approach to characterizing patients with varied SDoH accounts for the varying social contexts of all U.S. geographical regions. In doing so, it provides generalizable findings that allow actionable means of systematically initiating against SDoH vulnerabilities plaguing specific patients and their communities. Not only will such a nuance elucidate future investigation, it will also usher in the dialogue through which public policy and institutional outreach can begin to address the inequities that affect their surrounding social environments.
Footnotes
Authors' Contributions
D.J.F.-Z.: Conceptualization, data acquisition and analysis, data interpretation, and drafting and revision of article for significant scientific content. R.V.: Conceptualization, data interpretation, and drafting and revision of article for significant scientific content. R.A.: Revision of article for significant scientific content. A.S.L.: Revision of article for significant scientific content. D.C.C.: Conceptualization, data interpretation, revision of article for significant scientific content, and supervision. U.A.P.: Conceptualization, data interpretation, revision of article for significant scientific content, and supervision. S.S.S.: Conceptualization, data interpretation, revision of article for significant scientific content, and supervision. A.M.S.: Conceptualization, data interpretation, revision of article for significant scientific content, and supervision. J.C.R.: Conceptualization, data interpretation, revision of article for significant scientific content, and supervision.
Author Disclosure Statement
Dr. Chelius reported receiving a coordinator stipend from the American Academy of Otolaryngology outside the submitted work. No other disclosures were reported.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Table S1