
Abstract
Background:
The criteria for determining technical efficacy of thermal ablation for papillary thyroid carcinoma (PTC) are not clearly defined. We analyzed the involution process of the ablation zone with clear pathologic results on core-needle biopsy (CNB) to clarify the relationship between sonographic changes and pathologic findings.
Methods:
This retrospective cohort study included 382 patients with unifocal T1N0M0 PTC who underwent radiofrequency ablation (RFA) between May 2014 and August 2021. Patients with a single ablation zone biopsy (recommended at 3 or 6 months for T1a and 6 or 12 months for T1b) and regular neck ultrasound (US)/contrast-enhanced ultrasound imaging follow-up at 1, 3, 6, and 12 months and every 6–12 months thereafter after RFA were included. Patients also underwent yearly chest computed tomography. CNB was performed in the target lesion ablation zone's central, peripheral, and surrounding thyroid parenchyma to detect the presence of tumor cells. If the thyrotropin (TSH) was >2 mU/L, levothyroxine was prescribed with the intention of keeping the TSH 0.5–2 mU/L. Technical efficacy was defined as tumor disappearance by imaging follow-up together with the pathologically confirmed absence of tumor cells in the ablation zone.
Results:
During the mean follow-up period of 67.8 ± 18.2 months (22–110 months), the overall incidence of persistent disease and the technical efficacy rate were 3.9% (15/382; 2.9% of T1a, and 12.2% of T1b) and 96.1%, respectively. Tumor size (p = 0.03) and subcapsular location (p = 0.04) were risk factors associated with persistent disease. The technical success rate was 100%. Of the 367 ablation zones with benign CNB results, 336 (91.6%) showed tumor disappearance on US and no re-emergence of imaging-visible tumors during follow-up. Male sex (p = 0.006), age <40 years (p = 0.003), T1a tumor (p < 0.01), and energy per milliliter (p < 0.03) were significantly associated with tumor disappearance.
Conclusions:
US-guided RFA is an effective treatment for small low-risk PTC. Tumor disappearance on US after RFA may suggest an excellent prognosis and confirm complete ablation of the macroscopic tumor, but this sonographic finding is generally late and requires histological confirmation.
Introduction
Ultrasound (US)-guided thermal ablation is recommended as an alternative to surgery for benign thyroid nodules. 1,2 The treatment objective is to reduce nodule size, to relieve cosmetic problems or compressive symptoms. Importantly, papillary thyroid carcinoma (PTC) is the most common type of thyroid cancer, accounting for ∼80% of all cases. 3
Among these, small and low-risk PTCs are commonly associated with indolent behavior and excellent prognosis. 4 Moreover, with the increasing emphasis on de-escalation treatment strategies for low-risk PTC, minimally invasive interventions, such as US-guided thermal ablation, have gained increasing attention. 5,6
For the thermal ablation of benign nodules, technique efficacy is defined as a volumetric reduction ≥50% of the initial nodule volume. 7 Such an index could determine treatment outcomes after thermal ablation and guide follow-up management planning. Further, multiple studies have shown promising results for thermal ablation in the treatment of low-risk PTC. 8 –10
Nevertheless, the criteria for determining the efficacy of thermal ablation for PTC have not yet been clearly defined. In contrast to benign nodules, the treatment objective for malignant tumors is the complete eradication of the target tumor. Clear definitions of technique efficacy are necessary to ensure an objective and reliable interpretation of the complete tumor response after thermal ablation of PTC and to standardize the techniques and outcomes of thermal ablation as a treatment option.
Currently, the most commonly used method to evaluate the efficacy of the technique is US assessment of the size changes in the ablation zone after target tumor ablation to observe volume reduction, volume reduction ratio (VRR), and complete sonographic disappearance. 11 –13 A few studies have performed fine-needle aspiration (FNA) or core-needle biopsy (CNB) in the ablation zone to detect residual tumor cells. 14,15 However, no reliable evidence exists to confirm the parameters that can be used to predict therapeutic success after thermal ablation.
Therefore, we aimed at conducting an observational study of patients with PTC who underwent radiofrequency ablation (RFA), to analyze the involution process of the ablation zone during long-term follow-up. In addition, all ablated zones after RFA exhibited clear pathological results on CNB, clarifying the relationship between imaging and pathological findings.
Materials and Methods
Study population
This retrospective study reviewed the patients with unifocal low-risk PTC who underwent RFA at the Chinese People's Liberation Army General Hospital between May 2014 and August 2021. This study was approved by the Ethics Committee of the Chinese People's Liberation Army General Hospital (S2019-211-01 and S2020-237-01).
Written informed consent was obtained from all patients before RFA. The inclusion criteria were (1) PTC confirmed by FNA or CNB; (2) solitary tumor with maximum diameter ≤2 cm; (3) no imaging evidence of extrathyroidal extension, lymph node metastasis, distant metastasis on US, or computed tomography (CT); and (d) no history of neck radiation, and familial thyroid carcinoma. The exclusion criteria were as follows: (1) ablation zone without CNB, (2) multiple PTCs, and (3) follow-up period <12 months.
Pretreatment evaluation
All patients underwent US, CT, laboratory tests, and pathologic examination before RFA. US was performed to evaluate tumor size, location, US characteristics, and cervical lymph nodes. Tumor volume was calculated using the following equation: V = πabc/6 (V, volume; a, maximum diameter; b and c, two other perpendicular maximum diameters).
Further, a CT of the neck and chest was performed to detect cervical lymph node metastases and distant metastases. Laboratory tests included thyroid function, complete blood count, and blood coagulation tests. Pathologic examinations included US-guided FNA or CNB and BRAFV600E mutation tests.
RFA procedure
All RFA procedures were performed by a physician with >20 years of experience in thyroid US and tumor ablation. For guidance, a Siemens Acuson Sequoia 512 scanner (Siemens, Mountain View, CA) with a 6.0 MHz linear array transducer was used. In an outpatient clinic, patients were placed in the supine position with the neck extended. Local anesthesia with 1% lidocaine was administered at the subcutaneous tissue and perithyroidal area.
Moreover, a bipolar RFA generator (CelonLabPOWER; Olympus Surgical Technologies Europe) and an 18-gauge bipolar radiofrequency applicator with a 0.9-cm active tip (CelonProSurge micro100-T09; Olympus Surgical Technologies Europe) were used. The RFA procedure used a four-step approach 16 : (1) thorough examination by US, (2) proper use of the hydrodissection technique, (3) rigorous moving-shot ablation strategy, and (4) evaluation of the ablation zone by contrast-enhanced ultrasound (CEUS).
To prevent marginal residual tumors and recurrence, the ablation zone was ensured to exceed at least 2 mm from the original tumor margins. For the tumor with subcapsular location, the adjacent thyroid capsule was also ablated to ensure complete ablation. Complementary ablation was performed if a residual enhancement was observed.
Follow-up
Patients were evaluated using US at 1, 3, 6, and 12 months and every 6–12 months thereafter. US was used to assess the ablation zone and local tumor progression. Moreover, CEUS was performed at this follow-up interval to evaluate the ablation zone before its disappearance. US results for suspicious ablation zones were recorded according to the ACR Thyroid Imaging Reporting and Data System. 17 Volume reduction rate was calculated as follows: VRR = ([initial volume − final volume] × 100)/initial volume. Chest CT was performed annually monitoring for distant metastases.
Thyrotropin suppression
We recommended a goal serum thyrotropin (TSH) level in the range of 0.5–2 mU/L 18 for all patients. For patients whose TSH levels were above 2 mU/L, we recommended a starting dose of 25 μg/day levothyroxine. Thyroid function tests were performed every 2 months for the first year and every 6–12 months thereafter. Nine (2.4%) patients were treated with levothyroxine before RFA. At final follow-up, 24 patients (6.3%) were prescribed levothyroxine after RFA. Monitoring levothyroxine treatment and adjusting of levothyroxine dose was performed by study physicians with more than three years of experience in thyroid ablation.
Biopsy of the ablation zone
Based on the process of hyperthermic tumor injury, the ablation zone can be considered to have three zones, the central zone, peripheral zone, and normal surrounding tissue. 19,20 To confirm the efficacy of RFA in PTC, a single CNB was performed in the ablation zone's central, peripheral, and surrounding thyroid parenchyma of the target lesion to detect the presence of tumor cells (Fig. 1A).
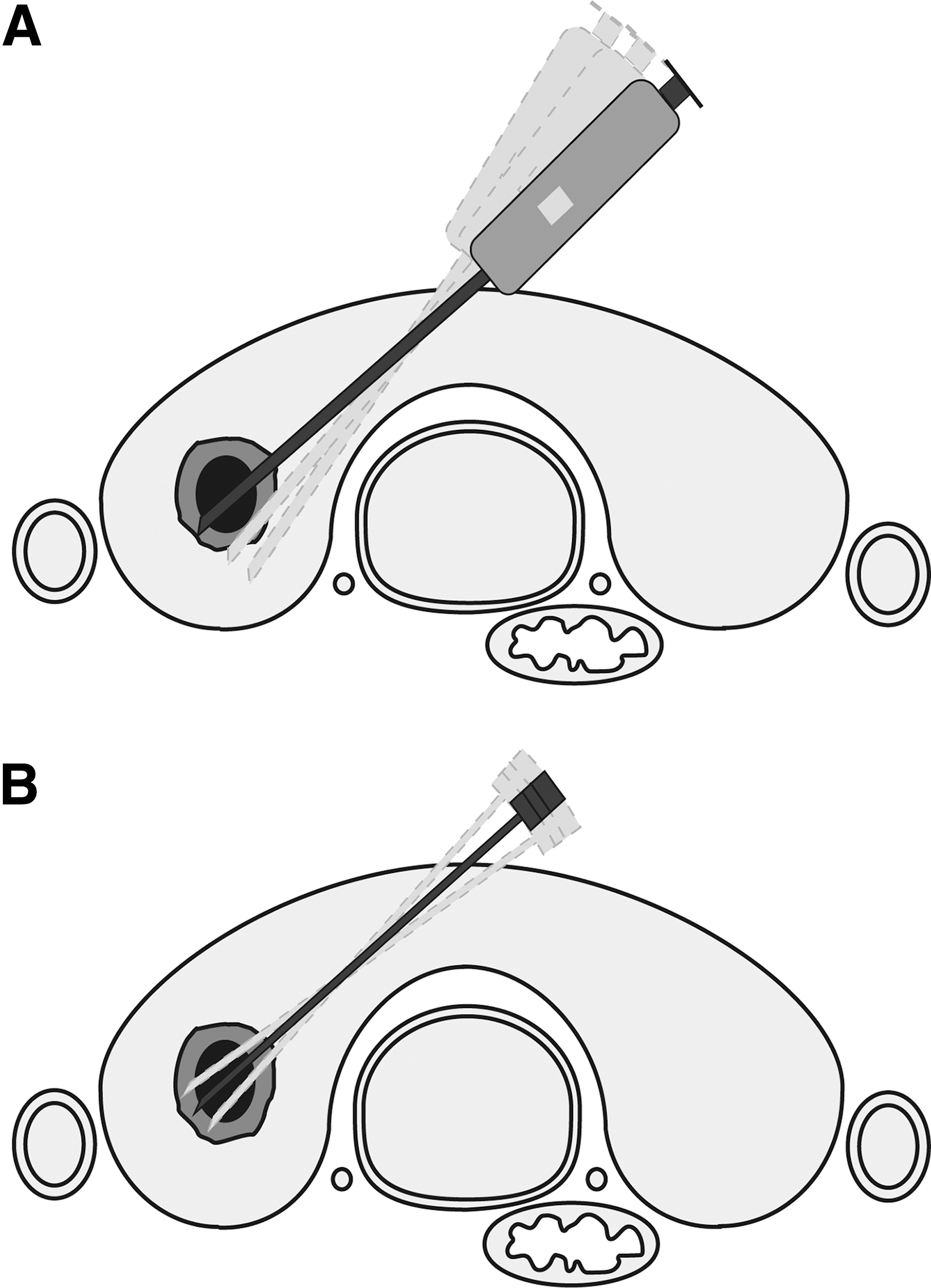
Schematic diagram of ablation zone biopsy. (
Routinely, for T1a tumors, it is recommended to be performed at three or six months after RFA. For T1b tumors, it is recommended at 6 or 12 months after RFA. The BRAFV600E mutation tests were performed at the same time as CNB was performed on the entire ablation zone using FNA to determine the BRAFV600E status (Fig. 1B).
The CNB and FNA procedures were performed by physicians with more than five years of experience in thyroid US. For CNB, biopsy procedures were performed using a disposable 1.5- or 2.2-cm excursion, 20-gauge spring-loaded needle (BARD double-action, Magnum; Bard Peripheral Vascular, Inc., Tempe). The FNA sampling for the BRAFV600E mutation tests was performed using a 25-gauge needle (Fine Aspiration Cytology Needle, Hakko, Japan), and BRAFV600E mutations were analyzed by quantitative polymerase chain reaction.
Clinical endpoints and definition
The primary endpoints were technique efficacy and persistent disease. The secondary endpoints were technical success, VRR, and tumor disappearance.
Technical success was defined as complete coverage of the target tumor by the ablation zone on CEUS at the end of each procedure. 21 Technique efficacy was defined as complete ablation of the target tumor, including tumor disappearance by imaging follow-up or the pathologically confirmed absence of tumor cells in the ablation zone. 21,22
Persistent disease was defined as persistently detected PTC in the ablated zone as confirmed by biopsy. The ablation zone with benign CNB results was defined as necrotic substances, inflammatory cells, granulation tissue, and fibrous proliferation, but no tumor cells were found. Tumor disappearance included: (1) complete disappearance, defined as the complete disappearance of the tumor on US, and (2) scarring, defined as the ablation zone observed as a linear scar. Incomplete disappearance was defined as an incompletely absorbed ablation zone on US. Subcapsular location was defined as the shortest distance of less than 2 mm between the tumor and the thyroid capsule or trachea.
Statistical methods
Categorical data are presented as numbers and percentages. Continuous data are described as means and standard deviations (SDs) or medians with interquartile ranges. Categorical comparisons were performed using the chi-square test or Fisher's exact test. Univariate and multivariable logistic regression analyses were conducted to identify the variables associated with persistent disease. Univariate and multivariable analyses of the Cox proportional hazards model were performed to identify the variables associated with tumor disappearance.
All p-values were two-sided, and statistical significance was set at p < 0.05. Statistical analyses were performed using the Statistical Package for the SPSS statistical software version 26.0.
Results
Patient characteristics
A total of 382 patients (297 females and 85 males) with solitary PTC were included in this study (Supplementary Fig. S1). Baseline patient characteristics are summarized in Table 1. The mean age, maximum tumor diameter, and median volume were 43.1 ± 9.7 (SD) years (range 18–74 years), 6.8 ± 2.9 mm (range 3–18 mm), and 78.8 mm3 (140.9 mm3), respectively. According to the AJCC/TNM cancer staging system, 23 341 (89.3%, 6.0 mm ±1.9, ≤5 mm comprised 44.3% of cases) patients were classified as stage T1a and 41 (10.7%, 13.0 ± 1.9 mm) patients were classified as stage T1b.
Baseline Patient Characteristics
Data are expressed as the n (%) or mean ± standard deviation (range) or median (interquartile range).
CEUS, contrast-enhanced ultrasound; TSH, thyrotropin.
The mean power, RFA time, energy for the RFA procedure, and median (interquartile range) energy per milliliter were 4.8 ± 1.5 W (range 3–9 W), 191.1 ± 127.4 seconds (range 26–1150 seconds), 888.3 ± 607.8 J (range 100–4520 J), and 8.94 J/mL (10.97 J/mL), respectively.
Technique efficacy
During a mean follow-up period of 67.8 ± 18.2 months (22–110 months), the technical efficacy rate and the overall incidence of persistent disease were 96.1% and 3.9% (15/382), respectively. The persistent disease rates in the T1a and T1b groups were 2.9% (10 of 341 patients) and 12.2% (5 of 41 patients), respectively. The persistent disease rates for T1a were 2.6% (4 of 151 patients) and 3.2% (6 of 190 patients) for lesions of less than 5 mm and more than 5 mm, respectively.
A statistically significant difference was found between the T1a and T1b groups (p = 0.015). Multivariable logistic regression analyses revealed that tumor size (p = 0.03) and subcapsular location (p = 0.04) were significant factors associated with persistent disease (Table 2). During the follow-up period, 1 patient (0.3%, 1 of 382 patients) was observed to have a metastatic lymph node in the ipsilateral neck at 21 months post-ablation. The patient elected re-ablation and had no disease progression after 68 months of follow-up. Of all patients, no distant metastases were detected.
Univariate and Multivariable Logistic Regression Analyses Identifying Variables Associated with Persistent Disease After Radiofrequency Ablation for Unifocal Small Low-Risk Papillary Thyroid Carcinoma
p < 0.05 was considered statistically significant.
CI, confidence interval.
We tested 345 tumors with the BRAFV600E mutation before ablation, and 87.2% (301/345) of them tested positive. After ablation, 316 tumors were tested for BRAFV600E mutations (Fig. 2), including 291 tumors that tested positive and 25 tumors that tested negative before ablation. In 84.9% (247/291) of the tumors that were BRAFV600E positive, the tumors were no longer present after RFA. Eleven of the 37 tumors that did not disappear were retested at three to six months and all were no longer present.
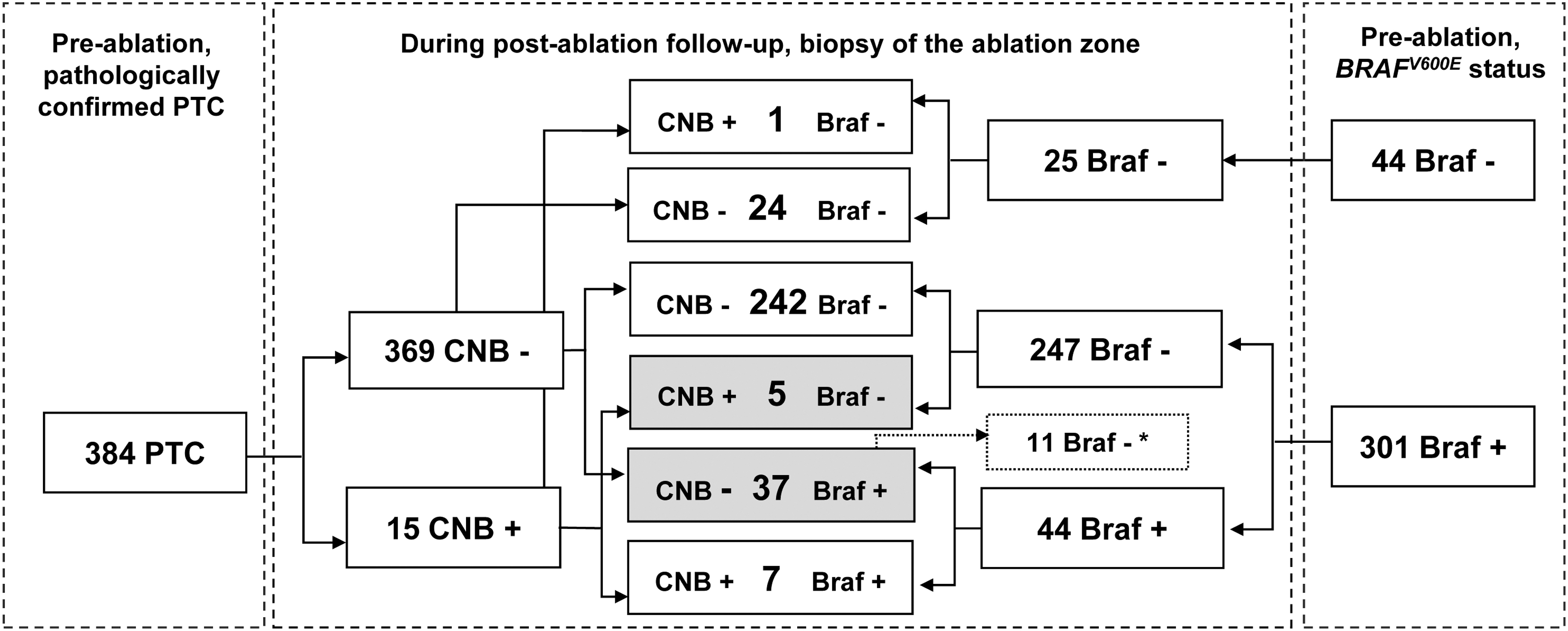
Changes in tumor pathology and genetic status before and after ablation. *Eleven of the 37 tumors that did not disappear were retested at three to six months and all were no longer present. PTC, papillary thyroid carcinoma.
Further, all patients who were BRAFV600E -negative before ablation remained BRAFV600E -negative after RFA. Using the post-ablation CNB results as the gold standard, the sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of the BRAFV600E mutation tests for the ablation zone were 58.3% (7/12), 86.4% (241/279), 85.6% (249/291), 15.9% (7/44), and 98.0% (242/247), respectively.
Changes in US performance
Fifteen patients with persistently detected PTC in the ablated zone had a positive CNB. The imaging appearances of all patients are shown in Table 3. On respective imaging modalities, 10 (66.7%), 7 (46.7%), and 14 (93.3%) ablation zones exhibited a suspicious US appearance, showed abnormal blood flow on color Doppler flow imaging (CDFI), and displayed abnormal contrast perfusion on CEUS.
Summary of the Post-Ablation Imaging Presentation of Different Pathological Conditions
Abnormal contrast perfusion is observed surrounding or within the ablated zone.
ACR TI-RADS, ACR Thyroid Imaging Reporting and Data System; CDFI, color Doppler flow imaging; CNB, core-needle biopsy; H, hypoechoic; hyper, hyperenhancement; hypo, hypoenhancement; I, ill-defined; iso, isoenhancement; P, punctate echogenic foci; T, taller-than-wide.
Moreover, CEUS allowed for a more sensitive identification of persistent diseases than did US and CDFI. Of the patients with persistent disease, four chose observation, with US showing the incomplete disappearance of stable hypoechoic areas (Fig. 3). The other 11 chose re-ablation; none showed abnormalities on US follow-up or pathologically confirmed benign results (Fig. 4).
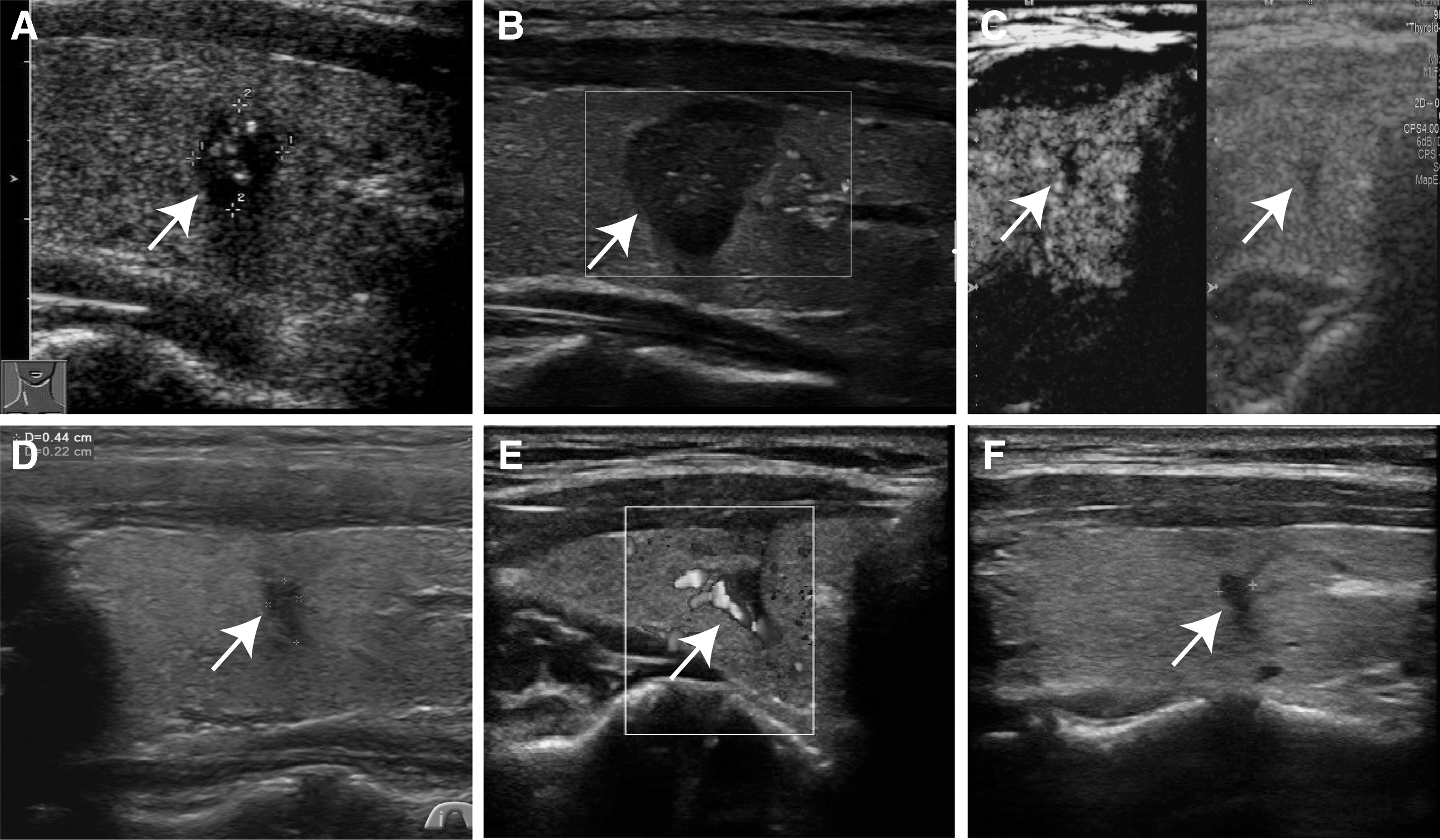
US image of a patient with the persistent disease chose observation. (
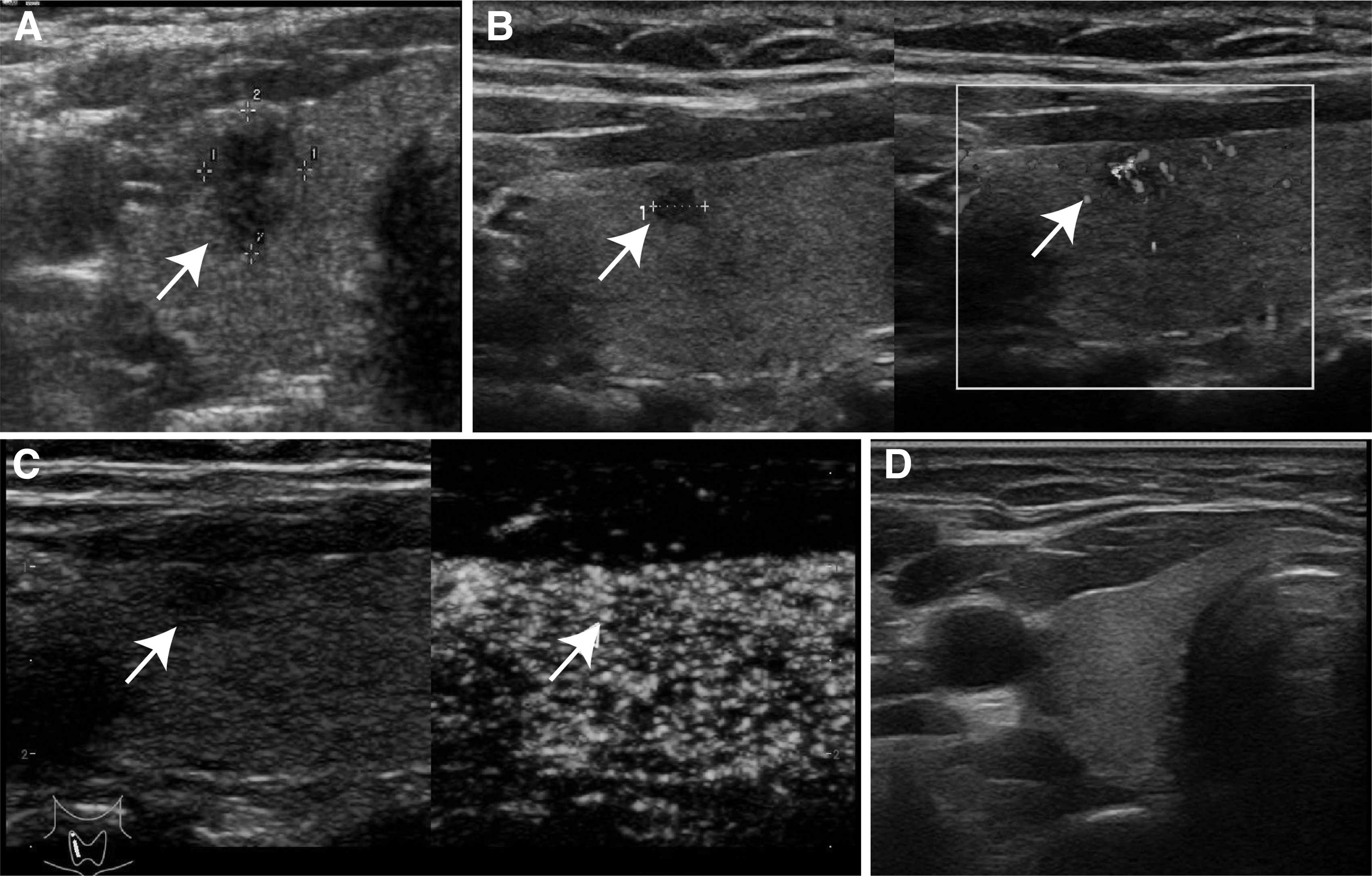
US image of a patient with the persistent disease chose re-RFA. (
Post-ablation tumor changes
None of the target tumors showed enhancement on CEUS at the end of ablation. The technical success rate was 100%. Due to the expanded ablation of the target tumor during ablation, the volume immediately after ablation and for the first three months was significantly larger than the initial volume before ablation (Supplementary Table S1).
Moreover, the volume of the ablation zone gradually decreased 3 months after ablation (p < 0.001 for all), while the median volume reduction rates were 62.1% and 98.0% at 6 and 12 months after ablation, respectively, and reached 100% at 18 months after ablation (Supplementary Table S1).
Of the 367 ablation zones with benign CNB results, 336 (91.6%) showed tumor disappearance on US during the follow-up period; of these, 57.7% (194 of 336 tumors) completely disappeared and 42.3% (142 of 336 tumors) were scars. The mean time for tumor disappearance was 15.4 ± 9.4 months. The tumor disappearance rates were 50.7% (186), 81.0% (111), 88.3% (27), 89.1% (9), 91.3% (2), and 91.6% (1) at 6, 12, 24, 36, 48, and 60 months, respectively.
At the final follow-up, 109 tumors (76.8%) scarring had completely disappeared (Fig. 5). Cox regression analysis revealed that male sex (p = 0.006), age <40 years (p = 0.003), T1a tumor size (p < 0.01), and energy per milliliter (p < 0.03) were significantly associated with tumor disappearance (Table 4). In addition, treated tumors that disappeared on US did not re-emerge as imaging-visible tumors during the mean follow-up period of 67.8 months.

US images of the involution process of the ablation zone in patients after RFA. (
Univariate and Multivariable Analyses Examining Tumor Disappearance
p < 0.05 was considered statistically significant.
HR, hazard ratio.
Discussion
As thermal ablation is increasingly used for PTC, an evidence-based definition of the efficacy of the technique is warranted. In this study, we analyzed the involution process of the ablation zone with clear pathologic results on CNB after RFA in 382 patients with solitary T1 PTC during five years. The tumor disappearance on US was the final result of the involution process of the ablation zone that has been effectively treated with thermal ablation.
Overall, the technical efficacy, persistent disease, technical success, and tumor disappearance rates were 96.1% (367 of 382 patients), 3.9% (15 of 382 patients), 100% (382 of 382 patients), and 91.6% (336 of 367 patients), respectively. For persistent disease, tumor size and subcapsular location were risk factors. Male sex, age <40 years, T1a tumor size, and energy per milliliter were significantly associated with tumor disappearance.
To our knowledge, this study is the first to examine the pathology of the post-ablation zone after RFA for PTC with a five-year follow-up period. Owing to the general lack of histological examination of the post-ablation zone, the true situation of complete tumor response after RFA is uncertain and the persistence of residual lesions cannot be excluded, potentially leading to the underestimation of the incidence of persistent disease.
Our study, although retrospective, defines the timing of the US changes and their correlation with the histological outcomes after RFA treatment of PTC. Our results showed that the incidence of persistent disease was 3.9%, which is higher than the range of 0–1% reported in previous studies. 8,13,24 –26 Notably, the incidence of T1b PTC (12.2%) with persistent disease was significantly higher than that of T1a PTC (2.9%).
Our results are consistent with those of previous studies in which the post-ablation zone showed pathological findings. 27,28 Larger tumors require more rigorous ablation procedures and adequate safety margins. Further, subcapsular location was associated with persistent disease, potentially due to inadequate safety margin. Therefore, we suggest ablation of the adjacent thyroid capsule along with adequate hydrodissection to ensure technical safety and complete ablation of the tumor.
The BRAFV600E mutation is the most common genetic alteration in PTC and has been reported in 30–67% of PTC cases. 18,29 Notably, its prevalence is significantly higher in Asia than in Western countries. 30 Here, the BRAFV600E mutation rate was 87.2%; specifically, we used FNA to test whether BRAFV600E -positive PTC was no longer present after thermal ablation to determine the technical efficacy. Notably, the test demonstrated low sensitivity (58.3%) yet high specificity (86.4%).
Consequently, while the test may overlook some instances of persistent disease, it remains highly reliable in confirming the success of thermal ablation. Further, we retested BRAFV600E status after three to six months in 11 tumors that did not disappear but were negative for CNB, and all were no longer present. We hypothesized that hyperthermic injury may induce coagulative necrosis in tumor cells; phagocytes' removal of this necrotic material is a dynamic process. 19
The optimal timing of BRAFV600E status is important to minimize false-positive results; early testing is not recommended and is suggested 6–12 months after ablation. However, future studies are warranted to verify this finding and explore applicable scenarios for testing the BRAFV600E state.
After ablation, the involution in the ablation zone gradually progressed. Male sex (p = 0.006), age <40 years (p = 0.003), T1a tumors (p < 0.01), and energy per milliliter (p < 0.03) were associated with earlier ablation zone disappearance. If the growth rate of residual tumor cells in persistent disease exceeds the absorption rate of the ablation zone, the ablation zone tends to increase in size, but PTC has an indolent disease process.
Therefore, the volume reduction and VRR parameters to assess the technical efficacy for PTC may not reflect the true tumor response in a timely manner. In our study, 91.6% of the tumors showed tumor disappearance on US examination after RFA, whereas the CNB results were all benign. In addition, the treated tumors that disappeared on US did not re-emerge as imaging-visible tumors, which was similarly observed in a 10-year follow-up study 8 and in a meta-analysis of a 5-year follow-up after thermal ablation of PTC. 31 Thus, tumor disappearance on US after RFA may indicate an excellent prognosis and confirm complete macroscopic tumor ablation, indicating the efficacy of the technique.
On US follow-up, ablation zones with persistent disease often appear hypoechoic, although suspicious features, such as taller-than-wide, ill-defined margins, punctate echogenic foci, and increased vascularity on CDFI, may appear. However, US findings are insensitive owing to the presence of necrotic or scar tissue, the appearance of which on US may closely mimic that of normal involution of the ablation zone.
Moreover, CEUS is a superior tool for detecting microvascular circulation compared with US and helps accurately define the gross extent of induced coagulation and microscopic foci of persistent disease. 32 Also, CEUS may be used to detect residual vital tissue after thermal ablation of benign nodules. 33,34 Notably, abnormal contrast perfusion is observed surrounding or within the ablated zone, indicating persistent disease. During involution of the ablation zone, the appropriate use of CEUS allows the early identification of persistent lesions and reduces unnecessary puncture biopsies.
Owing to the unique characteristics of ablation zone involution after thermal ablation of PTC, the tumor disappearance of the ablation zone can be used as an indicator of treatment efficacy. Importantly, most patients achieved tumor disappearance 12 months after thermal ablation. 35,36 For patients whose ablation zone has incompletely disappeared after 12 months or who have abnormal imaging findings, an appropriate biopsy is recommended (Fig. 6).
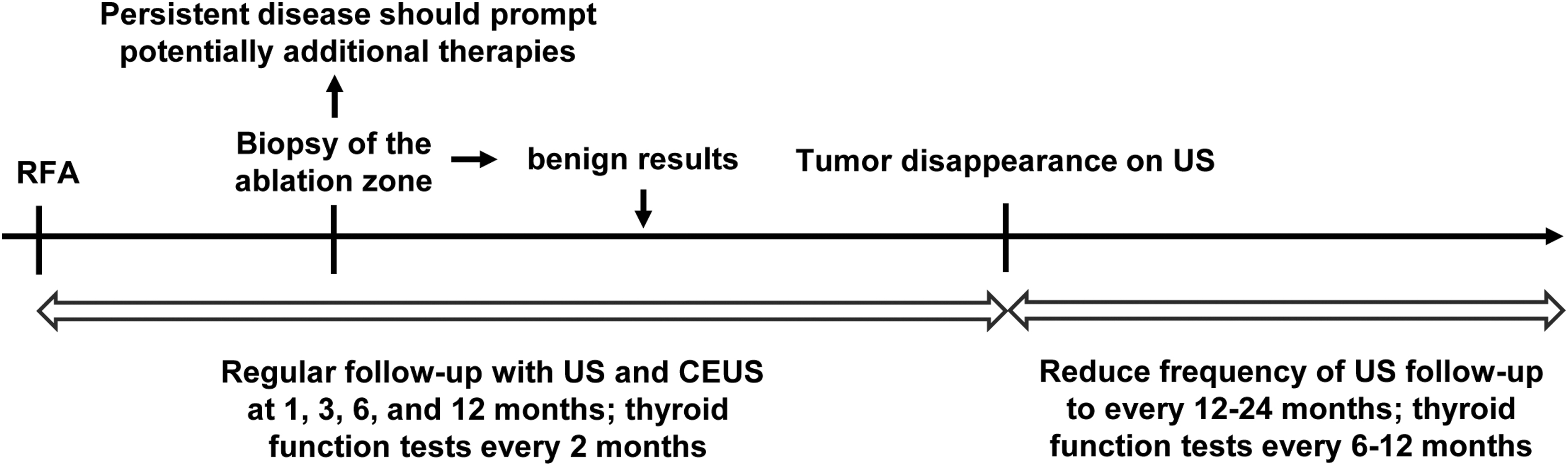
A schematic diagram of a suggested follow-up protocol for patients with PTC who have undergone RFA.
Routine follow-up with CEUS is not required once the tumor has disappeared from the ablation zone. This approach minimizes the use of unnecessary puncture biopsies and CEUS, without delaying retreatment for patients with persistent disease.
This study has several limitations. First, this was a single-center retrospective study; therefore, a selection bias may have affected our results and the multicenter reproducibility of the outcomes cannot be assessed. Second, because the timing of postablation CNB was recommended based on physician preference and patient circumstances, this study did not investigate the relationship between post-ablation CNB results and puncture time. Future prospective studies are warranted. Third, although the diagnostic accuracy of CNB after RFA is higher than that of FNA because more cellularity can be obtained in the ablation zone, pathological examination of the entire ablated zone cannot be performed.
Conclusions
Our findings show that US-guided RFA is effective for treating of small unifocal low-risk PTC, with 96.1% technical efficacy by CNB pathological examination and 91.6% tumor disappearance rate on US. Importantly, a complete ablation of low-risk PTC can be reliably obtained in tumors up to 10 mm (T1a), while persistent disease may be detected after treatment of tumors >10 mm (T1b) in 12.2% of cases.
Tumor disappearance on US after RFA may indicate an excellent prognosis and confirm complete ablation of the macroscopic tumor, but this sonographic finding is generally late and needs accurate histological confirmation with multiple passes. Technical efficacy should be defined as the complete ablation of the target tumor, including tumor disappearance by imaging follow-up together with the pathologically confirmed absence of tumor cells in the ablation zone.
This recommendation can ensure an objective and reliable interpretation of the complete tumor response after RFA of PTC and standardize the techniques and outcomes of RFA as a treatment option. Rigorous prospective studies at the multi-institutional level are necessary to confirm our findings. For BRAFV600E -positive PTC, testing the ablation zone after RFA for the absence of their mutations to confirm the technical efficacy has high specificity but low sensitivity and warrants future investigation.
Footnotes
Authors' Contributions
X.L.: Conceptualization (equal); formal analysis (lead); and writing—original draft (lead), review and editing (equal). Y. Li: review and editing (supporting); formal analysis (supporting). L.Y.: Software (lead); review and editing (supporting). J.X.: Methodology (equal); review and editing (supporting). Z.Y.: Methodology (equal); review and editing (supporting). H.J.: Methodology (equal); review and editing (supporting). M.Z.: Conceptualization (supporting); writing—original draft (supporting); and writing—review and editing (equal). Y. Luo: Conceptualization (equal); writing—original draft (supporting); and writing—review and editing (equal).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1