
Abstract
Background:
Despite the excellent disease-specific survival associated with low-risk differentiated thyroid cancer (DTC), its diagnosis and management have been linked to patient concerns about cancer recurrence, treatment-related health risks, and mortality. Lack of information regarding long-term health outcomes can perpetuate these concerns. Therefore, we assessed all-cause and cause-specific mortality in a large cohort of individuals diagnosed with low-risk DTC.
Methods:
From the U.S. Surveillance, Epidemiology, and End Results–12 cancer registry database (1992–2019), we identified 51,854 individuals (81.8% female) diagnosed with first primary DTC at low risk of recurrence (≤4 cm, localized). We estimated cause-specific cumulative mortality by time since diagnosis, accounting for competing risks. Standardized mortality ratios (SMRs) and CIs were used to compare observed mortality rates in DTC patients with expected rates in the matched U.S. general population, overall and by time since DTC diagnosis. We used Cox proportional hazards models to examine associations between radioactive iodine (RAI) treatment and cause-specific mortality.
Results:
During follow-up (median = 8.8, range 0–28 years), 3467 (6.7%) deaths were recorded. Thyroid cancer accounted for only 4.3% of deaths (n = 148). The most common causes of death were malignancies (other than thyroid cancer) (n = 1031, 29.7%) and cardiovascular disease (CVD; n = 912, 26.3%). The 20-year cumulative mortality rate from thyroid cancer, malignancies (other than thyroid or nonmelanoma skin cancer), and CVD was 0.6%, 4.6%, and 3.9%, respectively. Lower than expected mortality was observed for all causes excluding thyroid cancer (SMR = 0.69 [CI 0.67–0.71]) and most specific causes, including all malignancies combined (other than thyroid cancer; SMR = 0.80 [CI 0.75–0.85]) and CVD (SMR = 0.64 [CI 0.60–0.69]). However, mortality rates were elevated for specific cancers, including pancreas (SMR = 1.58 [CI 1.18–2.06]), kidney and renal pelvis (SMR = 1.85 [CI 1.10–2.93]), and brain and other nervous system (SMR = 1.62 [CI 0.99–2.51]), and myeloma (SMR = 2.35 [CI 1.46–3.60]) and leukemia (SMR = 1.62 [CI 1.07–2.36]); these associations were stronger ≥10 years after diagnosis. RAI was not associated with risk of cause-specific death, but numbers of events were small and the range of administered activities was likely narrow.
Conclusions:
Overall, our findings provide reassurance regarding low overall and cause-specific mortality rates in individuals with low-risk DTC. Additional research is necessary to confirm and understand the increased mortality from certain subsequent cancers.
Introduction
Differentiated thyroid cancer (DTC) is characterized by an excellent prognosis as most cases present as small tumors localized to the thyroid gland and are considered at low risk for recurrence according to the American Thyroid Association (ATA) risk classification scheme. 1 –5 From the early 1980s to mid-2010s, the incidence of DTC rapidly increased in the United States, largely owing to improvements in the detection and diagnosis of increasingly small tumors. 6,7
DTC is also diagnosed at relatively young ages compared with other adulthood cancers. 8 As a result, DTC survivors now make up the fifth largest cancer survivor population in the United States. 9 This population often faces significant worry and anxiety related to cancer recurrence, treatment-related health risks, and mortality. 10 Coupled with unmet information needs 11,12 and increased financial burden, 13 these concerns contribute to the poorer quality of life experienced by DTC survivors compared with the general population and even other cancer survivorship groups. 14,15
Therefore, it is essential to provide accurate prognostic information and timely and comprehensive data on health outcomes affecting this population and to identify potential short- and long-term complications of treatment. Previous large-scale population-based studies on mortality after diagnosis of DTC focused mainly on all-cause and thyroid cancer mortality. 3,4 There has been some, although conflicting, evidence of increased risk of second malignancies 16 and cardiovascular disease (CVD) in this population, 17 –20 although whether, or to what extent, these risks may be treatment related remains unclear.
In the current study, we assessed cumulative all-cause and cause-specific mortality in a large U.S. cohort of individuals diagnosed with low-risk DTC with up to 28 years of follow-up. Since it is well established that low-risk thyroid cancer survivors experience excellent disease-specific survival, our study was primarily focused on understanding patterns of mortality from causes of death other than thyroid cancer and whether treatment with radioactive iodine (RAI) may modify risk of death from these causes.
Materials and Methods
Data source
The current study used data from 11 population-based cancer registries of the Surveillance, Epidemiology, and End Results (SEER) Program (SEER-12 excluding Alaska Natives), representing ∼12.2% of the 2020 U.S. census population (Connecticut, Hawaii, Iowa, New Mexico, Utah, California [San Francisco–Oakland, San Jose–Monterey, and Los Angeles], Georgia (Atlanta and rural Georgia], and Washington [Seattle–Puget Sound]). 21
SEER collects information on demographics, cancer diagnosis, and first-course therapy received before recurrence or cancer progression from individual participating registries. 22 SEER registries collect data on vital status and cause of death from the National Center for Health Statistics. The study was considered nonhuman subjects research by the Institutional Review Board at the National Institutes of Health because it used publicly available deidentified data. 23
Identification of thyroid cancer cases and first-course treatment
Using SEER*Stat, version 8.4.0.1 (National Cancer Institute), we identified patients who were diagnosed with DTC (papillary and follicular carcinomas; Supplementary Table S1) as their first primary cancer between 1992 and 2019 (Fig. 1). We included only microscopically confirmed cases diagnosed before the age of 85 due to concerns of misclassification of the cause of death among older adult patients.
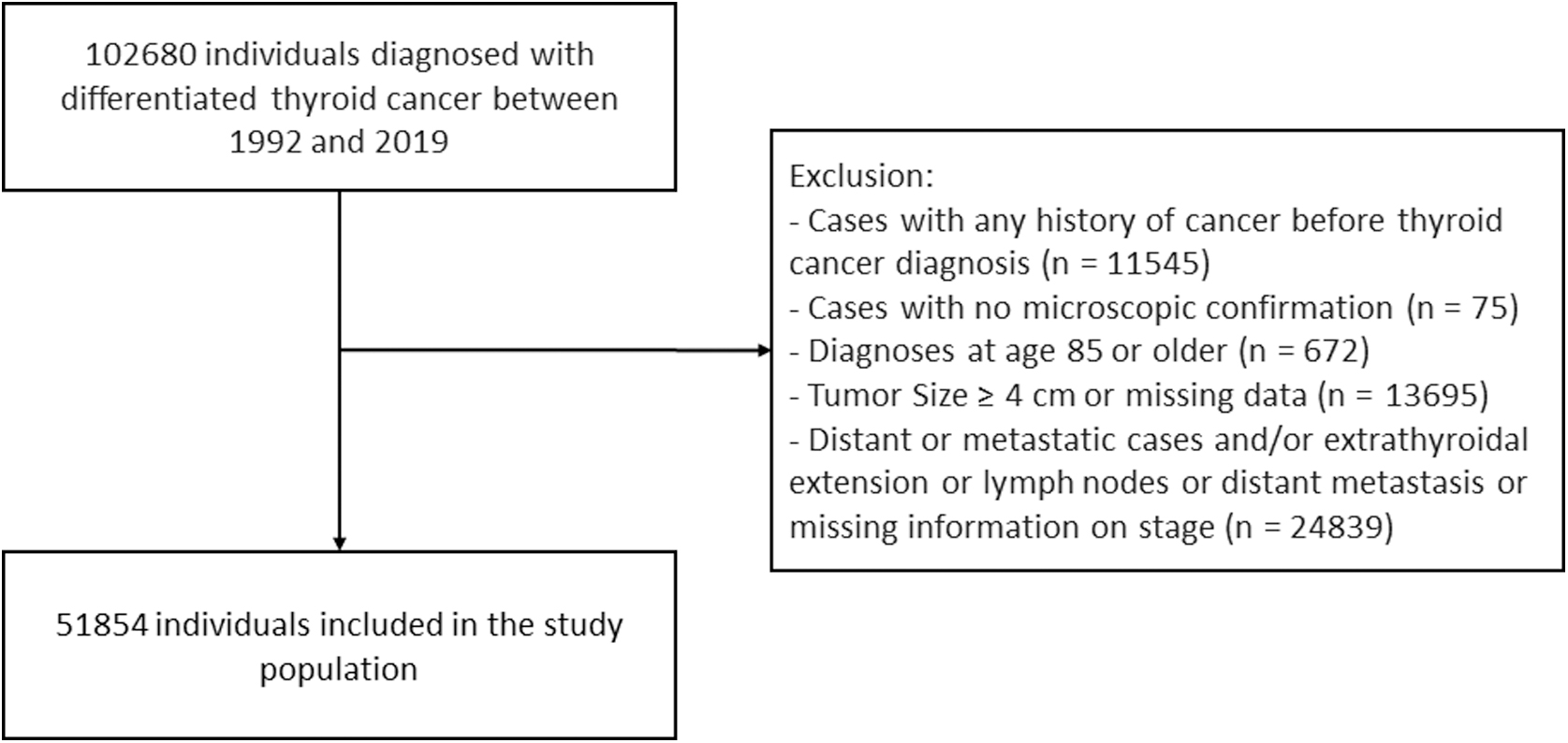
Flowchart of the study population.
Our study focused on DTC cases classified as localized, without extrathyroidal extension or lymph nodes or distant metastasis, following the ATA initial risk of recurrence classification. 5 Localized cases were identified using the “Localized” category from the following variables: SEER historic stage A (1973–2015) for the period before 1997, summary stage 2000 (1998–2017) for 1998–2003, and combined summary stage (2004+) for 2004 onward.
We excluded cases with tumors larger than 4 cm and those with missing information on stage or size. Cases were further categorized according to tumor size at diagnosis: ≤1, 1–2, and 2–4 cm. We classified patients into the following RAI treatment categories: no/unknown radiation, radioactive iodine, and other types of radiation (e.g., external beam radiation) (Supplementary Table S1).
We defined surgery procedures as total thyroidectomy, lobectomy, no surgery, and other/unspecified type of surgery. Subsequently, we classified patients into the following mutually exclusive groups according to their first-course treatment: total thyroidectomy followed by RAI, total thyroidectomy alone (no/unknown radiation), lobectomy alone (no/unknown radiation), no surgery with no/unknown radiation, and other/unspecified treatment.
The other/unspecified treatment group included patients who received any radiation treatment other than RAI, any surgical procedures other than total thyroidectomy and lobectomy, and RAI alone (no surgery) or after lobectomy.
Outcome
The SEER Program collects data on the underlying cause of death from death certificates provided by the National Death Index, which is maintained by the National Center for Health Statistics, 24 and deaths are coded according to the 10th revision of the International Classification of Diseases. Since the National Death Index is a national database, if a patient relocates from the SEER catchment area and dies elsewhere, the corresponding cause of death information can still be captured. Mortality groupings were based on the leading causes of death in the United States in 2019. 25
Statistical analyses
Unless stated otherwise, follow-up started at the date of DTC diagnosis and ended at the date of death, last contact, or December 31, 2019, whichever came first. We estimated cumulative all-cause mortality and cause-specific mortality by time since DTC diagnosis, considering death from other causes as competing risks.
External cohort comparisons
To compare mortality rates in low-risk DTC survivors with those in the general population, we calculated standardized mortality ratios (SMRs, the ratio of observed to expected number of deaths) and 95% confidence intervals [CIs], assuming a Poisson distribution for the observed deaths. Expected deaths were calculated by multiplying sex- (female/male), age- (5-year groups), calendar period-, and race-specific (White/Black/other) mortality rates of the U.S. general population by the person-years at risk.
The absolute excess mortality risk per 10,000 person-years was calculated as follows: [(number of observed events – number of expected events)/person-years of follow-up] × 10,000. Secondary analyses evaluated SMRs stratified by time since DTC diagnosis (<10 years/≥10 years), age at DTC diagnosis (<55 years of age/55+ years of age), and sex (males/females).
In a sensitivity analysis, we excluded cases classified as stage II/III/IV based on the 8th edition of the American Joint Committee on Cancer/TNM staging system from 2004 onward (n = 113), when information on TNM staging became available in SEER. 26 We also performed sensitivity analyses using data from the SEER-8 cancer registry database, which captured the most available calendar years (1975–2019), but had the smallest geographic coverage (∼8.3% of the U.S. population compared with 12.2% in SEER-12). 27
Internal cohort comparisons
Since RAI treatment has been associated with increased risk of second cancer after a thyroid cancer diagnosis, 28,29 we examined the association between RAI treatment and cause-specific mortality using multivariable Cox proportional hazards models with attained age as the timescale (to efficiently control for the confounding effects of age). We excluded the first 2 and 5 years of follow-up in analyses of deaths from hematologic and solid malignancies (other than thyroid or nonmelanoma skin cancer [NMSC]), respectively, to account for the minimal latency period for radiation-induced cancer. 30
For other causes of death, we excluded the first 2 years of follow-up to minimize confounding by prebaseline comorbidities. Proportional hazards assumptions were graphically evaluated based on plots of scaled Schoenfeld residuals against time and formally tested by introducing an interaction term between covariates and attained age during follow-up. Models were mutually adjusted for sex, race, and calendar period at DTC diagnosis.
In a sensitivity analysis, we used Fine–Gray models, 31 accounting for causes other than the outcome of interest as competing risks.
Results
In the cohort of 51,854 low-risk DTC patients, most subjects were female (n = 42,420, 81.8%), most were diagnosed with papillary thyroid cancer (n = 48,182, 92.9%), and most diagnoses were made before the age of 55 years (n = 35,379, 68.4%) (Table 1). Most patients received total thyroidectomy either with (n = 16,417, 31.7%) or without (n = 22,840, 44.0%) RAI as the first-course treatment.
Baseline Characteristics of Low-Risk Differentiated Thyroid Cancer Survivors in Surveillance, Epidemiology, and End Results–12 (1992–2019)
Patients who received any radiation treatment other than RAI, any surgical procedures other than total thyroidectomy and lobectomy, and RAI alone (no surgery) or after lobectomy.
RAI, radioactive iodine.
During follow-up (median = 8.8 years, range = 0–28 years), 3467 deaths (6.7%) were recorded. The leading causes of death were malignancies (other than thyroid or NMSC) (n = 1031, 29.7%), CVD (n = 912, 26.3%), thyroid cancer (n = 148, 4.3%), and accidents and adverse effects (n = 148, 4.3%).
Cumulative mortality
Cumulative mortality by time since DTC diagnosis is summarized in Figure 2 and Supplementary Table S2. At 5, 10, 15, and 20 years postdiagnosis, all-cause cumulative mortality was 2.2% [CI 2.0–2.3], 5.4% [CI 5.2–5.7], 9.7% [CI 9.3–10.1], and 14.9% [CI 14.3–15.5], respectively. Cumulative mortality from thyroid cancer reached 0.6% [CI 0.5–0.8] at 20 years of follow-up.
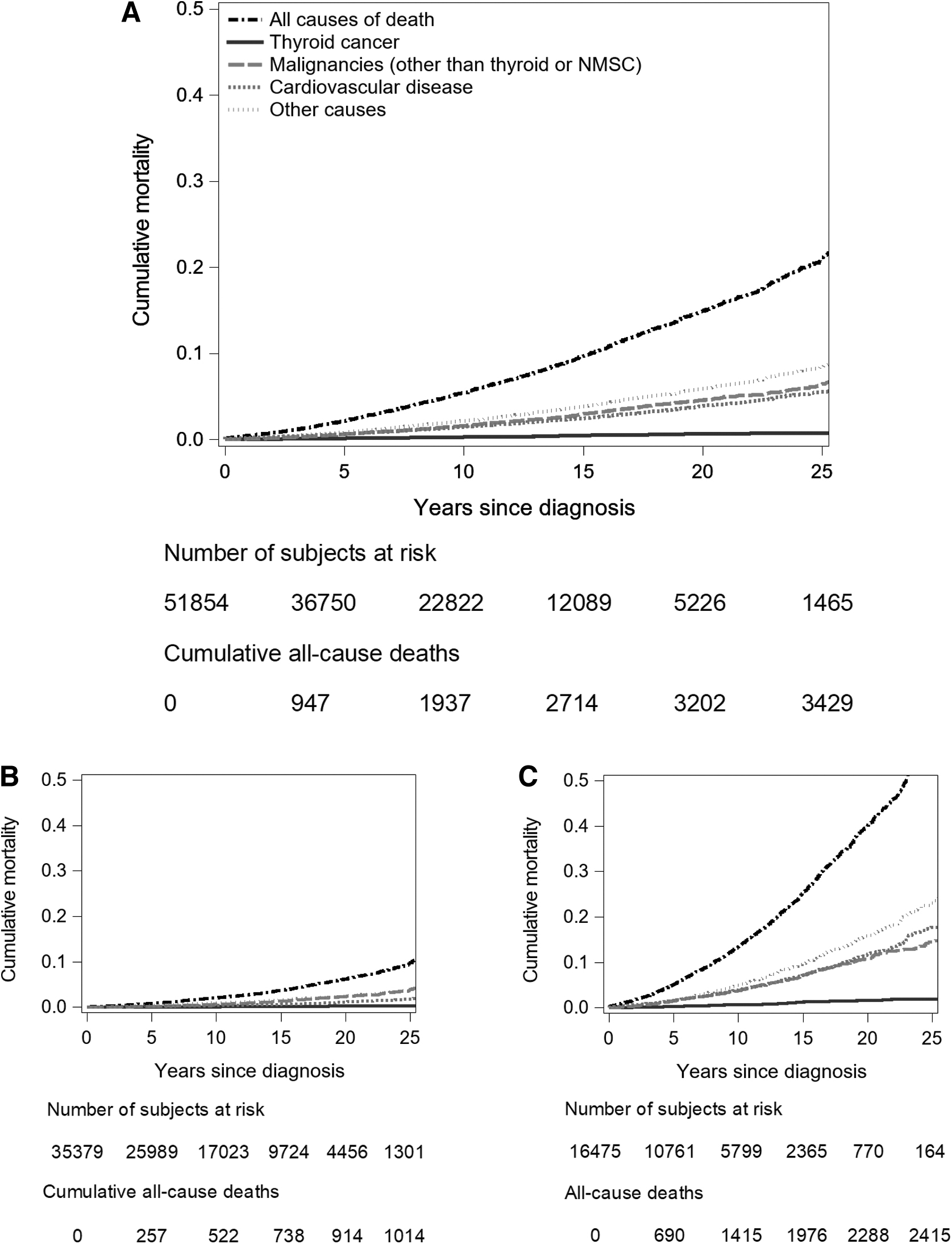
Cumulative mortality among low-risk differentiated thyroid cancer survivors in SEER-12 (1992–2019).
Cumulative mortality from malignancies (other than thyroid or NMSC), CVD, and other causes increased with time since diagnosis and reached 4.6% [CI 4.2–4.9], 3.9% [CI 3.6–4.2], and 5.9% [CI 5.5–6.2], respectively, at 20 years. Cumulative mortality from thyroid cancer, malignancies (other than thyroid or NMSC), and CVD was lower in DTC patients diagnosed before versus after age 55 years, irrespective of time since diagnosis.
External comparisons (SMRs)
Compared with the matched U.S. general population, individuals diagnosed with low-risk DTC had lower mortality overall (SMR = 0.69 [CI 0.67–0.71]) and from all malignancies combined (other than thyroid cancer and NMSC) (SMR = 0.80 [CI 0.75–0.85]), all solid malignancies combined (other than thyroid cancer and NMSC) (SMR = 0.76 [CI 0.71–0.81]), CVD (SMR = 0.64 [CI 0.60–0.69]), and other causes of death (SMR = 0.66 [CI 0.62–0.69]) (Fig. 3).
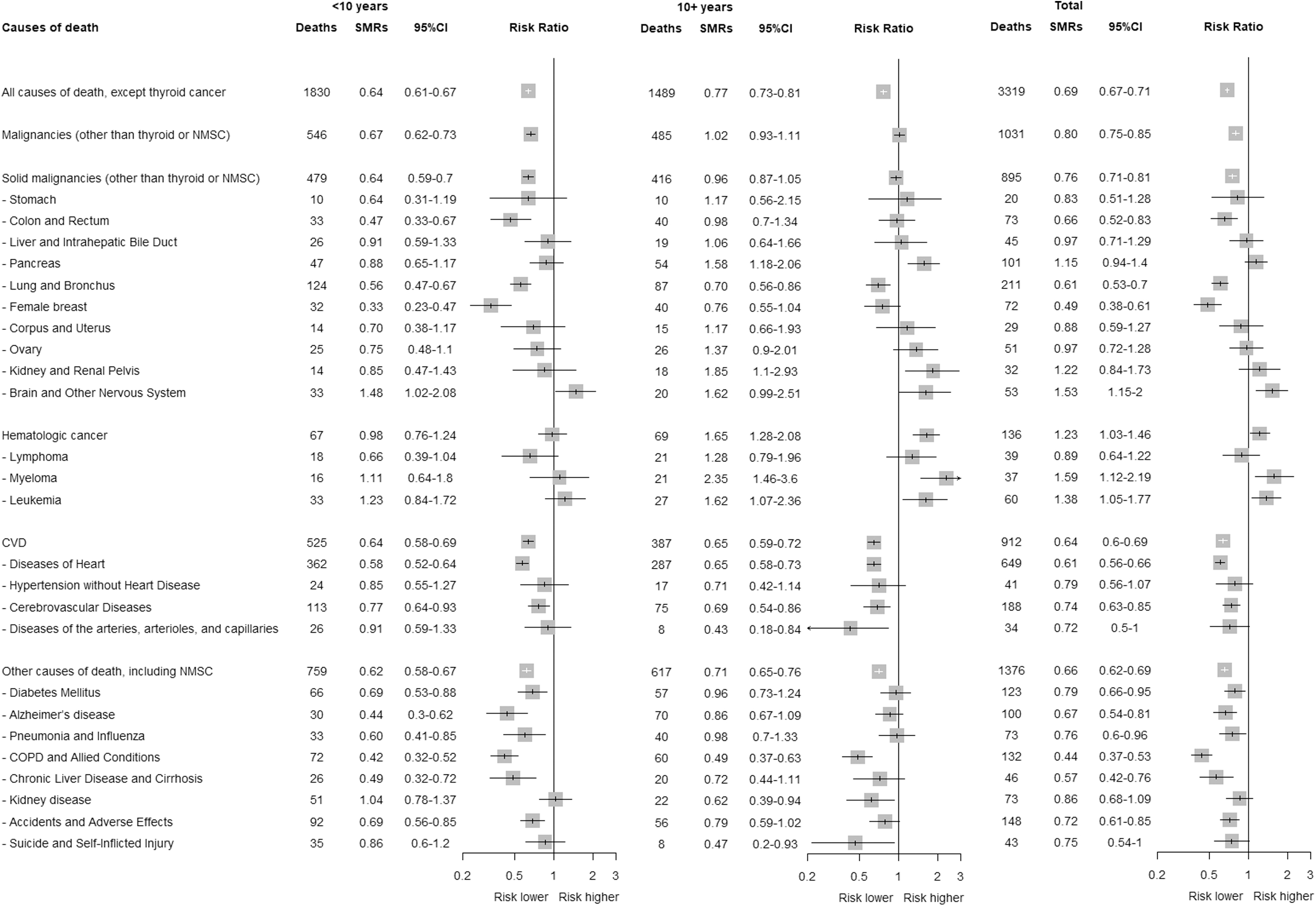
Frequency of deaths by different causes and the corresponding standardized mortality ratios in low-risk differentiated thyroid cancer survivors in SEER-12 (1992–2019), overall and by time since thyroid cancer diagnosis. The SMR estimates are not shown if the total number of cases is fewer than 20. Excess risk is per 10,000 person-years. Analyses of sex-specific cancers were conducted in a sex-specific population (i.e., either male or female population). COPD, chronic obstructive pulmonary disease; CVD, cardiovascular disease; NMSC, non-melanoma skin cancer; SMRs, standardized mortality ratios.
However, mortality was elevated from brain and other nervous system cancers (SMR = 1.53 [CI 1.15–2.00]), all hematologic cancers combined (SMR = 1.23 [CI 1.03–1.46]), myeloma (SMR = 1.59 [CI 1.12–2.19]), and leukemia (SMR = 1.38 [CI 1.05–1.77]). For solid malignancies (other than thyroid or NMSC), statistically significantly reduced SMRs were only observed in the first 10 years after DTC diagnosis (SMR<10 years = 0.64 [CI 0.59–0.70]; and SMR10+ years = 0.96 [CI 0.87–1.05]).
Starting 10 years after DTC diagnosis, we observed borderline elevated mortality from brain and other nervous system cancers (SMR = 1.62 [CI 0.99–2.51]) and significantly higher risk of cancers of the pancreas (SMR = 1.58 [CI 1.18–2.06]) and kidney and renal pelvis (SMR = 1.85 [CI 1.10–2.93]), as well as all hematologic cancers combined (SMR = 1.65 [CI 1.28–2.08]), myeloma (SMR = 2.35 [CI 1.46–3.60]), and leukemia (SMR = 1.62 [CI 1.07–2.36]). Similar findings were observed for SMRs stratified by age at diagnosis and sex (Supplementary Table S3).
Excluding cases classified as stage II/III/IV yielded virtually identical results (Supplementary Table S4). Similarly, when we conducted the analyses using the SEER-8 database (n = 37,966, median follow-up: 11 years, maximum of follow-up: 45 years), the cumulative mortality rates showed consistent trends (Supplementary Fig. S1) and SMRs were largely similar in magnitude (Supplementary Table S5).
Internal comparisons
RAI treatment was not associated with risk of specific causes of death, except for diseases of the heart (relative risk = 0.81 [CI 0.66–0.99]) (Fig. 4). However, numbers of cause-specific deaths among the RAI-treated and non-RAI-treated individuals were small (≤20 cases). The interpretation of findings did not change when restricting to 10-year DTC survivors (Supplementary Fig. S2), using Fine–Gray models (Supplementary Fig. S3) or when using the SEER-8 database (Supplementary Fig. S4).

Cause-specific mortality associated with first-course treatment of low-risk differentiated thyroid cancer survivors in SEER-12 (1992–2019). The first 5 years of follow-up were excluded in analyses of deaths from solid nonthyroid cancer, and the first 2 years of follow-up were included in analyses of deaths from hematologic cancer, CVD, and other causes. Models were adjusted for sex, race, year at diagnosis, histology, and tumor size. Attained age was considered as the timescale. Cumulative person-years for total thyroidectomy with and without RAI in the analyses, excluding the first 5 years of follow-up, are 115,309 (with RAI) and 109,275 (without RAI). For females, the person-years are 92,185 (with RAI) and 94,017 (without RAI). Excluding the first 2 years of follow-up, the person-years are 159,202 (with RAI) and 160,911 (without RAI). HR, hazard ratio; TT, total thyroidectomy.
Discussion
To inform the short- and long-term clinical management of patients diagnosed with low-risk DTC, which is characterized by excellent disease-specific survival, we evaluated all-cause and cause-specific mortality in a large U.S. population-based cohort with up to 28 years of follow-up (median follow-up = 8.8 years). In brief, we observed that these patients experienced lower rates of mortality overall and from most other causes compared with the general population, consistent with previous studies. 3,4,32 –35
Importantly, the proportion of low-risk thyroid cancer survivors who died from any cause or from the top three causes (CVD, malignancies [excluding thyroid cancer and NMSC], and thyroid cancer) remained low during the follow-up period. Our study is unique, in that it was restricted to survivors of low-risk DTC and included all ages at diagnosis, a longer duration of follow-up compared with previous studies, 3,4,17,18 and a comprehensive investigation of specific causes of death.
Our observations of lower than expected rates of mortality from CVD and noncancer causes were reassuring, as prior studies have found that thyroid cancer survivors exhibited a 1.29- to 2.47-fold higher incidence of atrial fibrillation 18,20 as well as higher incidence of other common CVD subtypes (e.g., heart failure, coronary artery disease, cerebrovascular accidents). 18,20,36 These prior findings were considered to be potentially attributable to the low levels of thyrotropin (TSH) induced by TSH suppression therapy. 18,20,36
Yet, of the few studies investigating CVD mortality, findings for CVD subtypes have been mixed, 17,18,37 which may be explained by limitations of these prior studies, including short follow-up duration, 37 hospital-based population, 16,17 and small population sizes. 17,18,37 The reduced rates of CVD and noncancer mortality in our cohort compared with the general population may be explained by differences in lifestyle. For instance, individuals with DTC may be less likely to smoke cigarettes or drink alcohol, two major factors contributing to various causes of death. 38 –40
Consistent with previous studies, 16,41,42 we found reduced mortality from lung and respiratory diseases, such as COPD, which supports a lower prevalence of smoking in our cohort. As most low-risk DTCs are identified through thyroid cancer screening or diagnostic imaging performed for reasons unrelated to the thyroid, 7 it is possible that our study population had more frequent interactions with the health care system or exhibited more health care-seeking behaviors. It is also possible that healthier behaviors are adopted after a thyroid cancer diagnosis, 43 which would contribute to a reduction in all-cause mortality. 44
Prior reports showed that compared with the general population, thyroid cancer survivors experience higher incidence of certain second primary malignancies, regardless of stage at DTC diagnosis, 42 including cancers of the salivary gland, colon/rectum, breast, prostate, kidney, bone, and brain and central nervous system, as well as soft tissue sarcoma, and hematologic malignancies. 16,41,42
In the current study, we did not observe increased risk of death from cancers of the salivary gland (3 deaths), bone (2 deaths), and prostate (17 deaths), or soft tissue sarcoma (13 deaths), likely due to the limited number of events, nor increased mortality risk from female breast cancer, which may be partly explained by high disease-specific survival.
On the other hand, consistent with previous findings, we found increased risk of death from certain types of cancers (e.g., pancreas, kidney and renal pelvis, and brain and other nervous system cancers, myeloma, and leukemia), which emerged in the longer-term follow-up period (≥10 years after DTC diagnosis). These increased risks are unlikely to be explained by surveillance bias as these cancers are typically not identified through screening. The co-occurrence of kidney and thyroid cancers has been shown in previous studies, 45 irrespective of RAI treatment, 45,46 suggesting a possible influence of genetic susceptibility or shared environmental risk factors.
As suggested by several studies, the late effects of radiation exposure from RAI treatment could at least partly explain an increased risk of cancer-related death in DTC survivors. 28,29,47 For instance, a recent SEER-based study of individuals diagnosed with either localized or regional stage thyroid cancer at younger ages (<45 years) found that those who were treated with RAI experienced higher incidence of certain second solid and hematologic malignancies than those not treated with RAI; moreover, the risk of solid malignancies was most pronounced for those diagnosed with thyroid cancer at younger ages and starting 20 or more years after thyroid cancer diagnosis. 28
Although we did not find associations of RAI treatment (yes vs. no/unknown) with cancer-specific mortality, our findings do not rule out an association between postsurgical RAI treatment and risk of subsequent cancer. In contrast to the study by Pasqual et al., our cohort included low-risk DTC diagnosed mostly in middle- to older-aged adults, who were likely treated with a lower dose of RAI.
Additionally, numbers of cancer-specific deaths were small, and the duration of follow-up may not have been sufficient to capture the long latency period between radiation exposure and cancer incidence and potentially long time frame from cancer diagnosis to death. Reliance on follow-up for cancer mortality rather than cancer incidence was a major limitation, specifically for cancers having a relatively high disease-specific survival rate (e.g., breast cancer), because multiple factors influence survival after subsequent cancer diagnosis.
SEER only captures information on the initial treatment, not treatments received for a recurrence or subsequent cancer. However, considering the length of mortality follow-up, it is unlikely that treatments related to recurrence or subsequent cancers had a major effect on our results. Incorrectly classifying exposure to RAI would most likely bias the risk estimates for RAI and cause-specific mortality toward the null. In addition, SEER registries do not collect information on RAI-administered activity, which prevented us from examining the dose–response relationship.
Finally, we had insufficient statistical power to investigate RAI treatment in relation to mortality from lymphoma and leukemia subtypes, which are etiologically heterogeneous, or RAI-associated risks among individuals diagnosed with DTC in childhood or young adulthood.
Our study also had some limitations, in addition to those described above. Our study was designed to capture mortality risks only during the follow-up period (median 8.8 years), not over the entire lifetime. The median age at the end of the follow-up was 58, while the median life expectancy is 76.4 years in the U.S. general population. These data should be reanalyzed after additional follow-up has accrued to understand the long-term mortality patterns among individuals diagnosed with low-risk DTC.
Some misclassification of the primary causes of death was possible due to reliance on death certificates. The lack of information on potential confounding factors in our Cox analyses, such as lifestyle factors (e.g., obesity, physical activity, cigarette smoking, alcohol consumption) as well as socioeconomic indicators, may have biased our results either toward or away from the null.
Our study also had several strengths. The large number of subjects and wide range of ages at diagnosis allowed us to perform a broad-based assessment of total and cause-specific mortality in patients with low-risk DTC. The choice to restrict to patients diagnosed with low-risk DTC likely reduced the potential for confounding by indication as first-course therapy options and long-term care differ substantially from high-risk DTC patients. Findings from studies using SEER cancer registry data are considered broadly generalizable and include diverse patient representation. 48
In conclusion, we found that low-risk DTC patients experienced low rates of mortality overall and from the top three causes of death in this population (CVD, solid malignancies [other than thyroid or NMSC], and thyroid cancer). Although further follow-up is necessary to confirm and understand the elevated risk of mortality from certain cancers beginning 10 or more years after DTC diagnosis, our findings are generally reassuring and may help to guide short- and long-term management of low-risk DTC.
Footnotes
Acknowledgment
This work was presented as an abstract at the 2023 American Thyroid Association Annual Meeting in Washington, DC, USA.
Authors' Contributions
T.-V.-T.T. was involved in conceptualization, data acquisition, methodology, formal analysis, visualization, writing—original draft, and writing—review and editing. S.J.S. was involved in conceptualization, methodology, formal analysis, and writing—review and editing. E.P., M.R.H., and L.M.M. were involved in conceptualization, methodology, and writing—review and editing. C.M.K. was involved in conceptualization, methodology, writing—review and editing, and supervision.
All the authors reviewed the work critically for important intellectual content, approved the final version of the article to be published, and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Author Disclosure Statement
E.P. is affiliated with the International Agency for Research on Cancer/World Health Organization and holds exclusive responsibility for the views expressed in this article. These viewpoints do not necessarily reflect the official decisions, policies, or stances of the International Agency for Research on Cancer/World Health Organization. M.R.H. holds the position of Associate Editor at Thyroid journal and was not involved in peer review of this article and was blinded to the review. The remaining authors have no disclosures to report.
Funding Information
T.-V.-T.T. and C.M.K. are funded by the Intramural Research Program of the National Cancer Institute, National Institutes of Health (ZIA-CP010131).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4