
Abstract
Objective:
Redifferentiation therapy (RDT) can restore radioactive iodine (RAI) uptake in differentiated thyroid cancer (DTC) cells to enable salvage 131I therapy for previously RAI refractory (RAIR) disease. This study evaluated the clinical outcomes of patients who underwent RDT and identified clinicopathologic characteristics predictive of RAI restoration following RDT.
Methods:
This is a retrospective case series of 33 patients with response evaluation criteria in solid tumors (RECIST)-progressive metastatic RAIR-DTC who underwent RDT between 2017 and 2022 at the Mayo Clinic (Rochester, MN). All patients underwent genomic profiling and received MEK, RET or ALK inhibitors alone, or combination BRAF-MEK inhibitors for 4 weeks. At week 3, those with increased RAI avidity in metastatic foci received high-dose 131I therapy. Baseline and clinicopathologic outcomes were comprehensively reviewed.
Results:
Of the 33 patients, 57.6% had restored RAI uptake following RDT (Redifferentiated subgroup). 42.1% (8/19) with papillary thyroid cancers (PTC), 100% (4/4) with invasive encapsulated follicular variant PTCs (IEFV-PTCs), and 100% (7/7) with follicular thyroid cancers (FTC) redifferentiated. All (11/11) RAS mutant tumors redifferentiated compared with 38.9% (7/18) with BRAF mutant disease (6 PTC and 1 IEFV-PTC). 76.5% (13/17) of redifferentiated and 66.7% (8/12) of non-redifferentiated patients achieved a best overall RECIST response of stable disease (SD) or non-complete response/non-progressive disease. Both subgroups had a median 12% tumor shrinkage at 3 weeks on drug(s) alone. The redifferentiated subgroup, following high-dose 131I therapy, achieved an additional median 20% tumor reduction at 6 months after RDT. There were no statistically significant differences between both groups in progression free survival (PFS), time to initiation of systemic therapy, and time to any additional therapy. Of the entire cohort, 6.1% (2/33) experienced histologic transformation to anaplastic thyroid cancer, 15.1% (5/33) died, and all had redifferentiated following RDT and received 131I therapy.
Conclusion:
RDT has the potential to restore RAI avidity and induce RECIST responses following 131I therapy in select patients with RAIR-DTC, particularly those with RAS-driven “follicular” phenotypes. In patients with PTC, none of the evaluated clinical outcomes differed statistically between the redifferentiated and non-redifferentiated subgroups. Further studies are needed to better characterize the long-term survival and/or safety outcomes of high-dose RAI following RDT, particularly whether it could be associated with histologic anaplastic transformation.
Introduction
Patients with differentiated thyroid cancer (DTC) with persistence, recurrence, or progression of distant disease have a poor prognosis. 1 –6 With rare exceptions following 131I therapy, the majority of patients with advanced DTCs have no available curative therapies. Cytotoxic chemotherapy and external radiation therapies have limited efficacy and are associated with significant adverse effects. 7 –9
Multikinase inhibitors targeting angiogenic growth factor receptors and molecular oncogene targeted therapies have significantly improved progression free survival (PFS), 10 –12 but their benefits are limited by significant drug-induced toxicities as well as emergence of tumor resistance. 13 –15
In metastatic DTCs, high-dose 131I can be associated with complete responses (CR), although rarely. 16 Most tumor responses following radioactive iodine (RAI) therapy are transient, mixed, and/or completely refractory. 17 –19 Mechanistically, this is due in part to the genomic alterations that induce thyroid oncogenesis as well as inhibit thyroid cancer differentiation, leading to impaired expression of the sodium iodine symporter (NIS), decreased follicular iodine uptake, and poor response to 131I therapy. 13,20,21
In 2011, Chakravarty et al., using a mouse model of papillary thyroid cancers (PTC) driven by conditional activation of oncogenic BRAF in thyroids, demonstrated that genomic and pharmacologic inhibition of BRAF, or downstream MEK, led to re-expression of NIS and RAI incorporation in PTCs. 22 Subsequently, several pilot clinical trials have demonstrated mixed but promising results with the use of MAPK inhibitors to induce redifferentiation and facilitate treatment with 131I in patients with advanced DTCs. 23
Redifferentiation therapy (RDT) is a potential salvage therapeutic strategy for patients with advanced DTCs, but with limited efficacy data to date. Currently, much of RDT is off-label with outcome data that are limited to small cohorts with marked differences in patient selection and treatment protocols as well as a lack of comparison in clinical outcomes between patients with and without restored RAI avidity following RDT. 24
In this study, we aimed at characterizing the clinical patterns of RAI uptake restoration as well as non-RAI restoration in RAI refractory (RAIR) disease and importantly examining the long-term outcomes of patients re-treated with high-dose 131I following RDT. Our goal is to identify the ideal candidates for RDT and assess the long-term impact and safety of this approach in advanced DTCs.
Methods
Design and sample
This was a retrospective case-series study conducted at the Mayo Clinic (Rochester, MN). The electronic medical records of all patients with DTC who received care between 2018 and 2022 were screened. Adult patients (18 years or older) with progressive metastatic disease over the previous 6 months (defined by the response evaluation criteria in solid tumors [RECIST] as at least 20% increase in the sum of diameters of target lesions or unequivocal progression of non-target lesions), 25 who were RAIR (lack of any I123 uptake on their most recent whole body scan (WBS) or progression of disease within 6–12 months after 131I therapy), and underwent RDT protocol were included in the study (Supplementary Fig. S1).
All participants underwent genomic profiling and followed a 4-week RDT protocol (Fig. 1). At week 1, patients were started on MEK inhibitor monotherapy for RAS mutant disease, combination BRAF-MEK inhibitors for BRAF mutant disease, RET inhibitor for RET fusion, and ALK inhibitor for ALK mutant disease (Supplementary Table S1). Two weeks before imaging, all patients underwent low iodine diets.

Redifferentiation protocol. *Modified dosimetry protocol. RAI, radioactive iodine; RDT, redifferentiation therapy; WBS, whole body scan.
At the end of week 3, all patients underwent Thyrogen-stimulated I123 WBS with Single Photon Emission Computed Tomography/Computed Tomography. At week 4, those who redifferentiated (any uptake of at least one lesion based on qualitive assessment) were treated with high-dose 131I following a previously reported modified dosimetry protocol. 26 The latter allows for administration of only 70% of the calculated maximum tolerated activity of RAI and/or a maximum dose of 300 mCi. In some cases, RDT agents were continued beyond the RDT protocol at the discretion of the treating provider.
Baseline characteristics
In addition to demographic characteristics, a comprehensive description of the clinical, biochemical, and structural disease status at the time of RDT was performed, including staging (following the eight edition of the American Joint Committee on Cancer [AJCC]/TNM staging system), 27 histology, genetic profile, duration of cancer diagnosis, duration of metastatic disease, site and burden of distant metastatic disease, non-stimulated thyroglobulin (Tg) levels, prior therapies, and cumulative dose of 131I.
Clinical outcomes
Patients were categorized as redifferentiated if they expressed any RAI uptake following RDT. Patients with no RAI uptake following RDT were deemed non-redifferentiated. Structural responses were defined by RECIST criteria as (1) CR: disappearance of all target lesions or disappearance of all non-target lesions with normalization of tumor marker levels, (2) partial response (PR): at least 30% decrease in the sum of diameters of target lesions, (3) progressive disease (PD): at least 20% increase in the sum of diameters of target lesions, unequivocal progression of existing non-target lesions, or appearance of new non-target lesions, (4) stable disease (SD): target lesions without CR, PR, or PD, or (5) non-CR/Non-PD: persistence of non-target lesions without CR or PD. 25
A modified objective response definition was used to include those who achieved CR, PR, SD, or non-CR/non-PD following RDT and before initiation of any other treatment. In addition, we assessed overall survival (OS), PFS, variations in tumor burden and non-stimulated Tg levels, additional therapies after RDT, time to initiation of any additional therapy, and time to initiation of systemic therapy.
All variables were evaluated 6 months before RDT and every 6 months afterward for up to the available duration of follow-up. All RECIST measurements and comparisons were conducted by the same researcher, and the assessment was contrasted with the information available on the radiology reports and clinical documentations. Adverse events were extracted from providers' documentation and medication administration records.
Statistical analysis
Baseline characteristics and clinical outcomes were described separately for the redifferentiated and non-redifferentiated subgroups. Continuous variables were summarized using medians and interquartile ranges (IQRs), and categorical variables were described with counts and percentages. For the clinical outcomes, only those who had at least 6 months of follow-up were included in the analysis of RECIST response, PFS, OS, time to systemic therapy, time to any additional therapy, and improvement in tumor size and thyroglobulin levels at 6 months.
Comparisons between both subgroups were established using Fisher exact tests for categorical variables and t tests for continuous variables. Due to the small sample size, multivariate analysis could not be performed. A p-value <0.05 was used as the cutoff for statistical significance.
Given the observed differences in RDT response between different histology subgroups, we further performed a secondary analysis including only patients with PTC histology. In addition, we compared the clinical outcomes between BRAF mutant redifferentiated patients versus RAS mutant redifferentiated patients, and between BRAF mutant redifferentiated patients versus non-redifferentiated patients.
Ethical considerations
The study's protocol was reviewed by the Institutional Review Board at Mayo Clinic (19-010708), and the requirement for study-specific informed consent was waived. All participants had previously provided the required Minnesota Research Authorization. Participants' information, confidentiality, and integrity were respected throughout the duration of the study.
Results
Sample and demographic characteristics
A total of 33 patients who had progressive metastatic RAIR-DTC and underwent RDT were analyzed. Of those, 19 patients (57.6%) redifferentiated and 14 (42.4%) were non-redifferentiated. For the entire cohort, the median age was 65 years (IQR 55–69), there was balanced gender participation (57.6% male vs. 42.4% female), and white predominance (94%) (Table 1). There were no differences in demographic characteristics between redifferentiated and non-redifferentiated patients. The median follow-up for both subgroups was 24 months.
Demographic Characteristics
Redifferentiated: Increased RAI uptake after RDT. Non-redifferentiated: No RAI uptake after RDT.
IQR, interquartile range; RAI, radioactive iodine; RDT, redifferentiation therapy.
Clinical characteristics
The median durations of cancer diagnosis and metastatic disease at the time of RDT were 8 years (IQR 3–12) and 35 months (20.5–78.2), respectively (Table 2). At the time of initial surgical management, most patients were stage II (39.3%) followed by stage I (36.3%). The predominant histology was PTC (69.7%) (Table 3), followed by follicular thyroid cancer (FTC; 21.2%), which was reflected genomically by the presence of BRAF (54.5%), followed by RAS (36.4%), and TERT mutations (48.5%).
Baseline Clinical Characteristics
Redifferentiated: Increased RAI uptake after RDT. Non-redifferentiated: No RAI uptake after RDT.
Pazopanib (1), lenvatinib (6), axitinib (1), sorafenib (1), and dabrafenib (1).
Alectinib (1).
fT4, free thyroxine; FTC, follicular thyroid cancer; IEFV-PTC, invasive encapsulated follicular variant PTC; PTC, papillary thyroid cancer; RAIT, radioactive iodine therapy; TSH, thyrotropin.
Staging, Histology, and Genetic Characteristics
Redifferentiated: Increased RAI uptake after RDT. Non-redifferentiated: No RAI uptake after RDT. PI3K/AKT/mTOR pathway (includes PIK3CA, PTEN, PIK3C2G, PIK3CG, PIK3C3, PIK3R1, PIK3R2, AKT3, TSC1, TSC2, and MTOR). SWI/SNF chromatin remodeling complex (ARID1A, ARID1B, ARID2, ARID5B, SMARCB1, PBRM1, and ATRX). HMTs: Mutations of the histone methyltransferases (KMT2A, KMT2C, KMT2D, and SETD2). MMR: Mismatch excision repair (MSH2, MSH6, and MLH1).
At the time of initial surgical management.
AJCC, American Joint Committee on Cancer; TMB, tumor mutation burden.
The most common site of distant metastatic disease was the lungs (81.1%) followed by locoregional lymph node involvement (45.4%). The median non-stimulated Tg was 103 ng/mL (IQR 16–294). Most patients had received prior 131I therapy with a median cumulative dose of 203.5 mCi (IQR 150–305.7), 54.5% had prior surgical reintervention, 27.3% had prior localized therapy (such as ethanol ablation), 27.3% had prior radiotherapy, and 24.2% had prior systemic therapy.
Overall, there were 8 out of 19 (42.1%) patients with PTC, 4 out of 4 (100%) with invasive encapsulated follicular variant PTC (IEFV-PTC), and 7 out of 7 (100%) with FTC redifferentiated following RDT (Fig. 2). All 11 (100%) RAS mutant tumors (2 classical PTC [C-PTC], 3 IEFV-PTC, and 6 FTC) and only 7 (38.8%) with BRAF mutant tumors (6 PTC, and 1 IEFV-PTC) redifferentiated following RDT. Overall, patients with FTC (p = 0.01), RAS mutation (p < 0.001), non-stimulated Tg of 294 mIU/L or more (p = 0.03), largest tumor diameter of 1.7 cm or less (p = 0.05), and bone metastases (p = 0.007) were likely to redifferentiate following RDT.
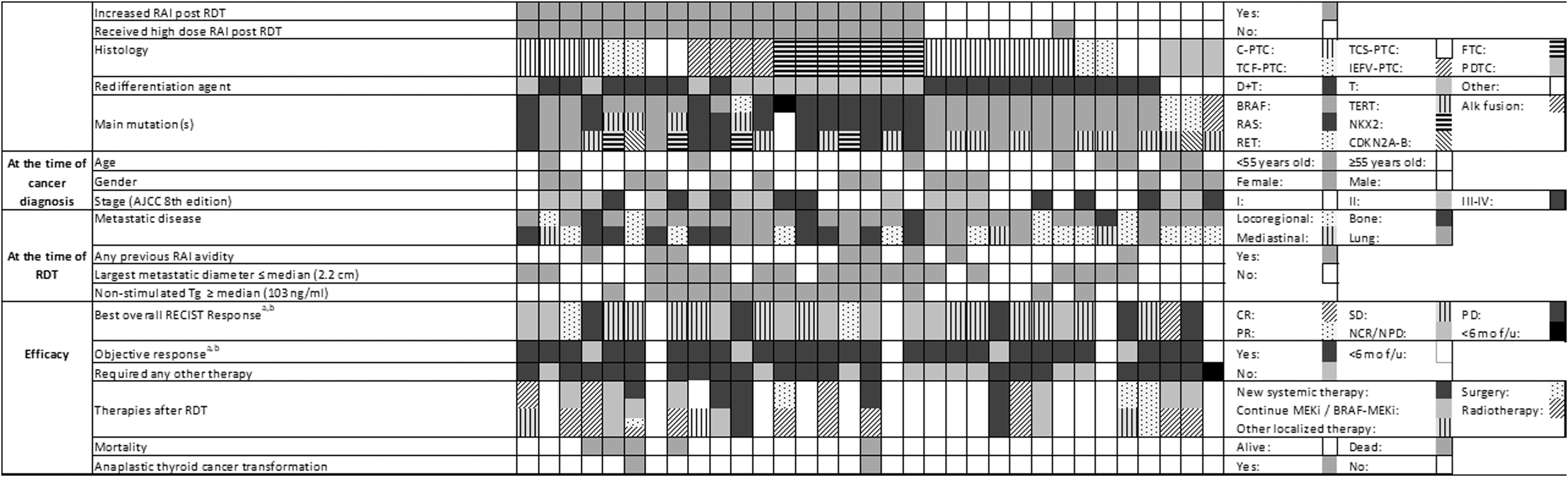
Onco print. aTwo patients were excluded on each subgroup since they had not completed 6 months from RDT. bBefore initiation of any other treatment. AJCC, American Joint Committee on Cancer; C-PTC, classical papillary thyroid cancer; CR, complete response; D+T, dabrafenib and trametinib; FTC, follicular thyroid cancer; f/u, follow up; IEFV-PTC, invasive encapsulated follicular variant papillary thyroid cancer; MEKi, MEK inhibitor; NCR/NPD, non-complete response/non-progressive disease; PD, progressive disease; PDTC, poorly differentiated thyroid cancer; PR, partial response; RECIST, Response Evaluation Criteria in Solid Tumors; SD, stable disease; T, trametinib; TCF-PTC, tall cell features papillary thyroid cancer; TCS-PTC, tall cell subtype papillary thyroid cancer.
In contrast, patients with poorly differentiated thyroid cancer (PDTC; p = 0.03), BRAF mutation (p = 0.01), and locoregional nodal disease at the time of initial surgical management (p < 0.001) or at the time of RDT (p = 0.001) were less likely to demonstrate restored RAI avidity following RDT.
Clinical outcomes
All 19 patients who redifferentiated received high-dose 131I with a median dose of 248 mCi (IQR 178.6–291.2) (Table 4). Of these patients, 15 (79%) expressed restored I123 avidity in lung metastases (including 4 FTC, 12 PTC, 8 RAS, and 5 BRAF mutant disease), and 13 (68.4%) did so in bone metastases (including 5 FTC, 6 PTC, 8 RAS, and 3 BRAF mutant disease).
Clinical Outcomes
Redifferentiated: Increased RAI uptake after RDT. Non-redifferentiated: No RAI uptake after RDT. Objective response: CR, partial response, stable disease, or non-CR/non-PD.
Two patients were excluded on each subgroup since they had not completed 6 months from RDT.
Before initiation of any other treatment.
CR, complete response; PD, progressive disease; RECIST, Response Evaluation Criteria in Solid Tumors; Tg, thyroglobulin; TKI, thyroid kinase inhibitors; TL, target lesion.
Figure 3 characterizes RECIST defined tumor responses and median changes in Tg levels following RDT. Of the 17 patients who redifferentiated and had at least 6 months of follow-up, 13 (76.5%) had SD or non-CR/non-PD as their best overall RECIST response before subsequent treatment (35.2% and 41.2%), 15 (87.2%) achieved objective response, and 13 (76.4%) required additional therapy after RDT (including 5 systemic therapy, and 8 radiotherapy).
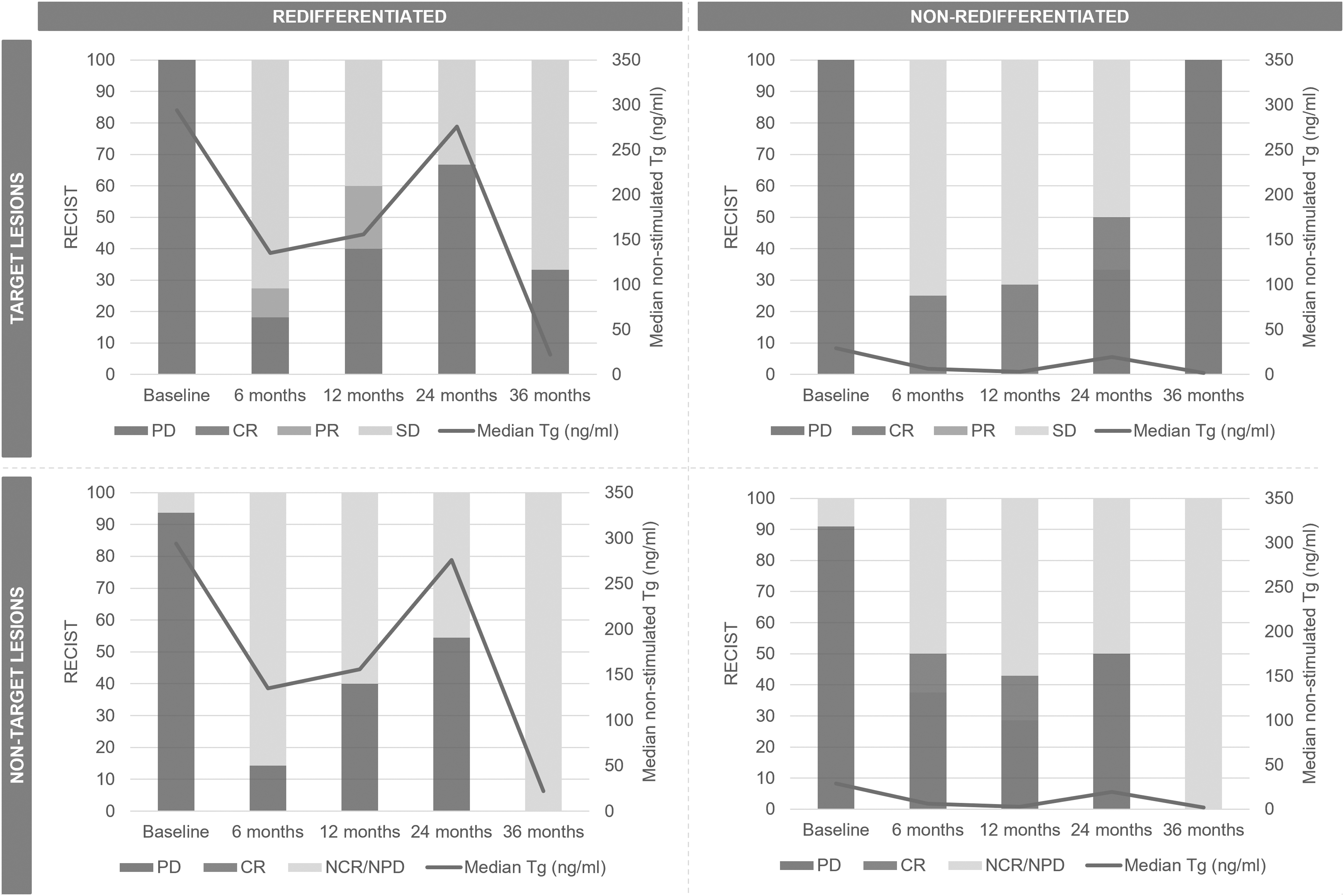
Progression of tumor burden and thyroglobulin levels before initiation of any other treatment. Two patients were excluded on each subgroup since they had not completed 6 months from RDT. Redifferentiated: Increased RAI uptake after RDT. Non-redifferentiated: No RAI uptake after RDT. Objective response: CR, PR, SD, or NCR/NPD.
In this group, the median PFS was 18 months, median time to initiation of systemic therapy was 18 months (Participants who were continued on thyroid kinase inhibitors [TKI] after RDT were excluded from this analysis), and median time to any additional therapy was 24 months (In participants who were continued on TKI after RDT, additional therapy was considered as the need for any additional intervention such as surgery, localized therapy, or radiotherapy) (Fig. 4).
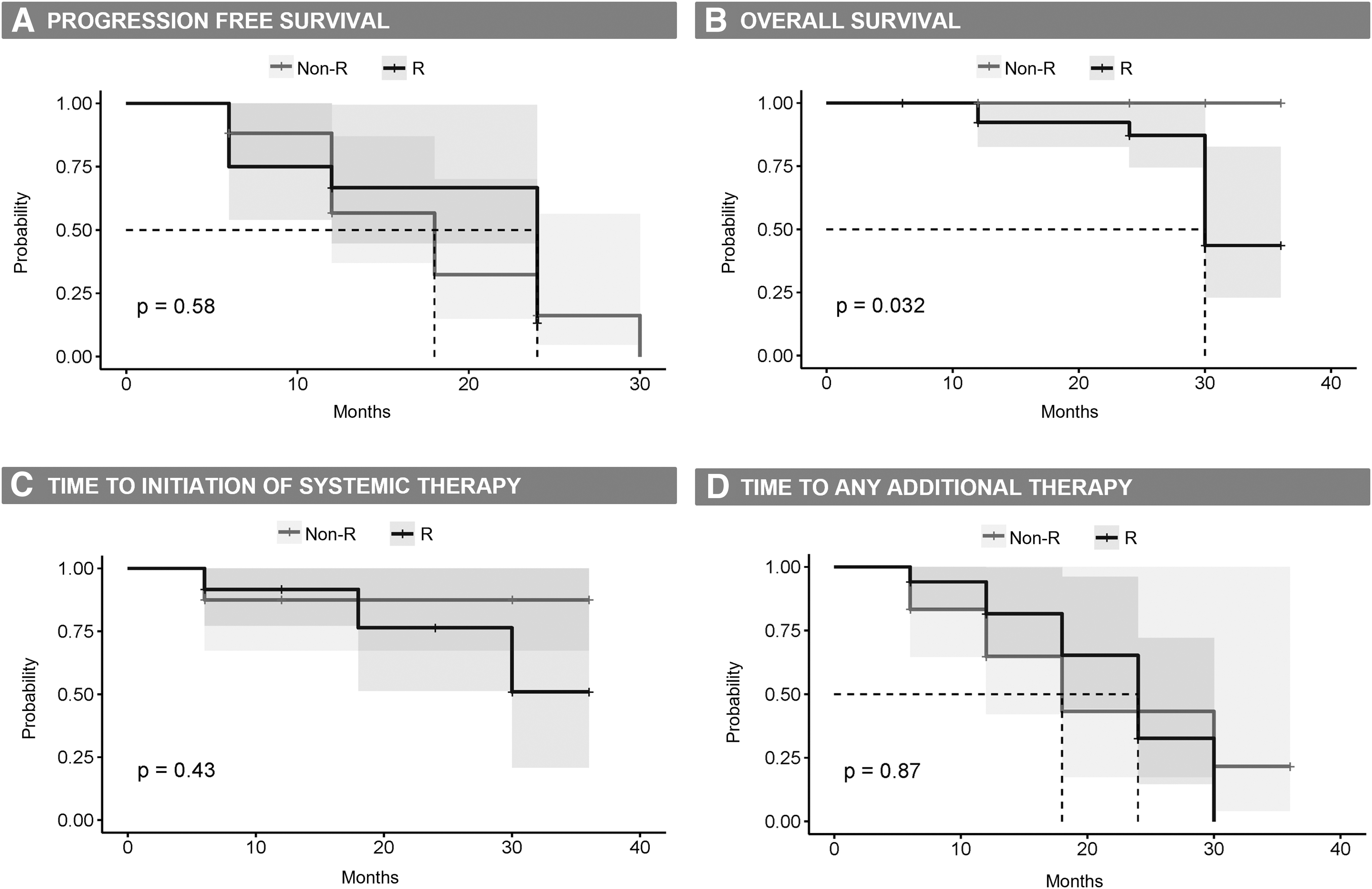
Clinical outcomes. Kaplan Meier curves for: (
The frequency and duration of these outcomes was comparable to that of the non-redifferentiated that did not receive 131I, with no statistically significant differences between both subgroups, even when stratifying the results by BRAF mutation status. Notably, the lack of control group for RAS mutant disease that did not receive RDT limits outcome data for this subpopulation.
Both redifferentiated and non-redifferentiated patients experienced a similar decrease in the median sum of the target lesions' diameters 3 weeks after treatment with MAPK inhibitor(s) (11% vs. 12.4%, p = 0.7). However, the redifferentiated subgroup developed additional tumor regression at 6 months following 131I therapy, while no further improvement was noted in the non-redifferentiated without 131I therapy (30% vs. 13%, p = 0.9). Despite this, both subgroups experienced comparable median percentual reduction of non-stimulated Tg levels 6 months after RDT (60.5% vs. 75.7%, p = 0.5).
Compared with the BRAF mutant non-redifferentiated patients, BRAF mutant redifferentiated patients experienced a similar decrease in the median sum of the target lesions' diameters 1 month after the initiation of the RDT agents (18% vs. 10.9%, p = 0.28) but with statistically greater decreases at 6 months (30% vs. 12%, p < 0.01). Overall, there were no statistically significant differences in median Tg levels nor overall clinical outcomes between these two subgroups on long-term follow-up.
Noteworthy, five out of the redifferentiated patients were continued on their TKI beyond the 4 weeks of the RDT protocol. Their RECIST responses over the first 6 months post-RDT were SD for four participants and non-CR/non-PD for one participant. Likewise, four of the non-redifferentiated patients were continued on TKI, out of which two achieved non-CR/non-PD, one SD, and one CR at 6 months from RDT initiation.
Mortality and safety
The most reported adverse effects were maculopapular rash (42.1% in redifferentiated vs. 28.6% in non-redifferentiated, p = 0.4) and fatigue (26.3 vs. 42.8%, p = 0.3) (Table 5). Of the entire cohort, 5 (15.1%) patients died. All of these had redifferentiated following RDT and received subsequent high-dose 131I treatment. Two out of these five had experienced non-CR/non-PD or SD following RDT but later experienced histologic transformation to anaplastic thyroid cancer (ATC; 18 and 24 months after RDT) and died within 6 months.
Safety
Redifferentiated: Increased RAI uptake after RDT. Non-redifferentiated: No RAI uptake after RDT.
Two initially experienced SD after RDT but died from complications associated with their tumor burden (24 and 30 months after RDT). One progressed despite RAI avidity restoration following RDT (12 months after RDT). Compared with the genetic profile of initial metastatic lesions, in the tall cell subtype PTC (TCS-PTC) that transformed to ATC, genomic interrogations demonstrated an underlying BRCA2 germline mutation and a newly acquired PTEN mutation. In the FTC that transformed to ATC, there were newly identified TERT, CDKN2A-B, EIF1AX, and NF2 mutations on subsequent genetic testing. None of these two patients had continued TKI or received any additional therapy after RDT and before anaplastic transformation.
Secondary analysis
Of the 19 patients with PTC, 4 out of 11 (36.4%) with C-PTC, 2 out of 4 (50%) with TCS-PTC, and 2 out of 4 (50%) tall cell features PTCs (TCF-PTC) redifferentiated following RDT. Both (100%) RAS mutant tumors (C-PTC) redifferentiated compared with only 6 (33.3%) of the BRAF mutant tumors (2 C-PTC, 2 TCS-PTC, and 2 TCF-PTC).
The median non-stimulated Tg level was higher in the redifferentiated subgroup (66.5 vs. 46 mIU/L, p = 0.18). Overall, patients with RAS mutation (p = 0.08), bone metastasis (p = 0.05), prior external radiotherapy (p = 0.03), or prior systemic therapy (p < 0.01) were more likely to respond to RDT. In contrast, patients with locoregional nodal disease or distant metastasis at the time of initial surgical management (p = 0.04 and p = 0.05), or with BRAF mutant disease (p = 0.08) were less likely to restore RAI avidity following RDT.
Regardless of redifferentiation status after RDT, both subgroups had similar outcomes in tumor burden as defined by RECIST criteria. Of the 7 redifferentiated patients who had at least 6 months of follow-up and received a median 131I dose of 226.7 mCi (IQR 191.8–250.5), 5 (71.4%) had SD or non-CR/non-PD as their best overall RECIST response before initiation of any other treatment (compared with 80% in non-redifferentiated, p = 0.6), and 6 (85.7%) achieved objective response (compared with 80% in non-redifferentiated, p = 0.7).
Redifferentiated patients had a non-statistically significant tendency toward higher median PFS (12 vs. 9 months, p = 0.5), and time to any additional therapy (18 vs. 12 months, p = 0.5) as compared with non-redifferentiated patients. The median time to systemic therapy was 12 months for the non-redifferentiated subgroup compared with no additional systemic therapy required in the redifferentiated subgroup (p = 0.12). Overall, the mortality incidence was higher in patients who redifferentiated compared with those who did not redifferentiate (50% vs. 0%, p = 0.01).
Discussion
RDT has emerged as a promising strategy for inducing RAI uptake in metastatic DTC to enable therapeutic benefit from 131I therapy. Published series with small sample sizes and heterogeneity in patient selection, RDT protocols, and outcome measures have demonstrated mixed responses in RAI avidity, RECIST responses, PFS, and other clinical outcomes. 24
The results of a randomized clinical trial of selumetinib versus placebo followed by 131I therapy in patients with advanced RAI avid disease (NCT02393690) are expected to be published this year. In the interim, off-label RDT in RAI avid and refractory disease is now common in advanced thyroid cancer practices. Our off-label series, which is currently the largest cohort, strengthens previous findings, demonstrating a strong phenotype-genotype correlation with clinical outcomes of RDT as well as unexpected durable partial tumor responses to short-term drug therapy alone.
Our data also raise important questions about the long-term benefits of RDT, particularly whether this therapy delays the need for systemic therapy with multikinase inhibitors and importantly, whether this therapy may select for and/or induce more aggressive tumor subclonal populations that may eventually progress to anaplastic transformation.
We identified that patients with FTC or IEFV-PTC histologies and RAS mutations were more likely to restore RAI avidity following RDT compared with BRAF mutations and/or PTC histologies. RAS mutation, high Tg levels, small tumor diameter, bone metastasis, and lack of locoregional nodal disease, all characteristic features of follicular histologies, demonstrated high likelihood of restored RAI avidity following RDT. Similar to Ho et al. and Jaber et al., all RAS mutant patients restored RAI avidity with RDT. 28,29
This finding is inconsistent with the results from Iravani et al. and Leboulleux et al. in which only around 30% of RAS mutant patients had restoration of RAI avidity with RDT. 30,31 In contrast, only 38% of our BRAF mutant patients restored RAI avidity despite the use of combination dabrafenib and trametinib as the RDT agents, and patients with PTC were less likely to restore RAI avidity if they had BRAF mutant disease.
We hypothesize that these mixed findings may be related to the diversity of disease definitions (i.e., criteria for RAI refractoriness or successful response to RDT), heterogeneity of tumor phenotypes (i.e., PDTC) and genomics (i.e., presence of additional mutations), and/or the predominance of PTC histologies in published series.
Additional studies are needed to better understand the discrepancies between the initial BRAF mutant animal data by Chakravarty et al. and our human data, indicating that PTCs with BRAF mutation are less likely to redifferentiate. This may be due to differences in the tumor microenvironment, host immunity, and/or genomic heterogeneity that may impair NIS re-expression.
The discordance between BRAF and RAS responses to RDT is consistent with TCGA multi-genomic profiling of nearly 500 PTCs, together with preclinical data demonstrating attenuated ERK-driven negative feedback in BRAF driven tumors, resulting in higher MAPK output signaling compared with RAS-driven tumors. 32
Despite potent combination BRAF-MEK inhibition in BRAF mutant PTCs, either incomplete MAPK inhibition or alternative signaling pathways likely facilitate resistance to NIS re-expression in most, but not all, advanced BRAF mutant PTCs. Conversely, RAS-driven tumors with lower MAPK output relative to BRAF-driven PTCs have robust re-expression of NIS following MEK inhibition; however, tumor heterogeneity results in mixed responses to RAI therapy following RDT.
Comprehensive genomic profiling of tumors before and following RDT will be important to better understand the pathways that may mediate resistance to RDT. For example, advanced oncocytic thyroid cancers (formerly called Hurthle cell thyroid cancers), well characterized by mitochondrial DNA alterations in the tricarboxylic acid cycle and most often lacking MAPK oncogenic drivers, are RAIR at baseline, despite high Tg levels. 33,34 This suggests that potentially altered mitochondrial metabolism may influence expression of NIS; whether this impacts PTC and FTC, and its reversibility has not been explored.
In our series, 88.2% of the patients who responded to RDT experienced RECIST defined SD, non-CR/non-PD, PR, or CR, which is consistent with the previously reported series.28–30,35–37 In addition, the median PFS of 18 months, and the median time to additional therapy of 24 months were shorter than those reported by Leboulleux et al. 37
However, in their series, RDT was given as first-line therapy for PD, the lesions' size was smaller, and the duration of advanced disease was shorter. This suggests that RDT used earlier in the course of metastatic disease may maximize its potential clinical benefits.
Similar to previous reports,29,35–37 short-term therapy with MAPK inhibitors alone appears to have durable tumor control, with 66.7% achieving SD, non-CR/non-PD or some degree of improvement in tumor burden. In our series, both redifferentiated and non-redifferentiated patients experienced a 12% reduction in tumor size 3 weeks after RDT. In patients who redifferentiated and received subsequent treatment with high-dose 131I, an additional 20% reduction in tumor size at 6 months after RDT was seen.
Leboulleux et al. also reported that RECIST responses at 6 months were independent of the initial improvement in tumor burden experienced at 1 month. 37 Altogether, the evidence suggests that, in patients with restored RAI avidity, retreatment with high-dose 131I could have added benefit as compared with drug therapy alone. Notably, for follicular phenotypes with RAS alterations of which 100% had successful RDT, the lack of “control” population (for example, non-RDT patients) may underestimate the therapeutic benefits of RDT in this particular population.
In general, RDT appeared to be a safe strategy with most patients experiencing only fatigue and maculopapular rash. However, in our series, mortality was higher in the patients who redifferentiated. Two of these patients experienced anaplastic transformation, with evolution of additional genetic alterations likely contributing to their tumor biology and rapidly fatal disease progression.
Other adverse events, such as myelodysplastic syndrome with progression to acute leukemia 28 and skin squamous cell carcinomas, 35 have been reported following RDT. While the causality between these events and RDT is not clear yet, future clinical trials and pooled data from off-label series may better examine the link between adverse events and cumulative 131I exposure, transformation to ATC, and/or molecular changes following RDT and RAI therapy. These safety concerns need to be weighed against the potential benefits when deciding whether to pursue RDT as a potential strategy in patients with advanced DTCs.
The results of this study should be considered in the context of its limitations. While our series is the largest published so far, it is still relatively small, which could lead to underestimation of the statistical significance of our outcomes. Although we used the redifferentiated and non-redifferentiated patients as the comparison subgroups for the statistical analysis, there is marked heterogeneity in histology types and genetic profiles that can influence the individual outcomes of each patient regardless of their response to RDT.
Thus, we stratified the results by type of histology and genetic profiles whenever possible and conducted a secondary analysis on PTC patients alone. Future research is needed to examine, in a genotype-phenotype specific manner and with control arms, the effects of RAI therapy following RDT on tumor genomic heterogeneity, time to salvage systemic therapies, and OS. Given the retrospective design of this study, the severity of adverse events could not be graded. The continuation of TKI beyond the RDT protocol could have overestimated the clinical outcomes in some patients.
Missing data may also impact the accuracy of the long-term follow-up findings. Finally, since the agents used for RDT are not FDA approved for this indication, there is a risk of selection bias that could affect the generalization of our findings. Despite these limitations, our results expand the current body of knowledge, do inform current clinical practices, and may guide the design of future randomized prospective studies.
In conclusion, RDT has the potential to restore RAI avidity and induce RECIST responses following 131I therapy in select patients with RAIR-DTC, particularly those with RAS mutations and “follicular” phenotypes. However, none of the evaluated clinical outcomes differed statistically between those who experienced restored RAI avidity and those who did not.
Importantly, however, there was a lack of “control” arm for RAS mutated disease, all that redifferentiated and received 131I. Responses in this group may underestimate the benefits for RDT for RAS-driven disease. RDT agents on their own appeared to have an impact in the burden of disease as evident by improvement in lesion's size and Tg levels during the first 6 months, regardless of the response to RDT or retreatment with high-dose 131I.
Further prospective, randomized, multicenter studies are needed to facilitate patient selection, evaluate the utility of alternative diagnostics like I-124 PET/CT to predict response to RAI therapy following RDT, and better characterize the long-term efficacy, survival, and/or safety outcomes of high-dose 131I following RDT, particularly whether it could be associated with histologic anaplastic transformation. International collaboration, and standardization of definitions and protocols would facilitate future research and improve the quality of data.
Footnotes
Acknowledgments
Authors' Contributions
D.T.-T.: conceptualization, methodology, data collection, statistical analysis, and manuscript preparation (initial draft, review, and editing). M.R.: conceptualization, methodology, and manuscript preparation (review and editing). J.C.M., C.H., C.P., and J.M.D.: manuscript preparation (review and editing).
Author Disclosure Statement
All authors have no relevant disclosures.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1