
Abstract
Background:
African American (AA) thyroid cancer patients have worse prognoses than European Americans (EA), which has been attributed to both health care disparities and possible genetic differences. We investigated the impact of both germ line and somatic variants on clinical outcome in a cohort of AA nonmedullary thyroid cancer (NMTC) patients who had received therapeutic intervention from cancer centers.
Methods:
Whole-exome sequencing was performed on DNA from available blood/normal tissues (N = 37) and paired tumor samples (N = 32) collected from 37 and 29 AA NMTC patients, respectively. Variants with Combined Annotation Depletion Dependent (CADD) score of ≥20 and VarSome Clinical classification of likely pathogenic or pathogenic were classified as presumed pathogenic germ line or somatic variants (PPGVs/PPSVs). PPGVs/PPSVs in cancer-related genes and PPGVs in cardiovascular risk genes were further investigated, and PPGVs/PPSVs associated with African (AFR) ancestry were identified.
Results:
Among 17 PPGVs identified in 16 cancer predisposition or known cancer-related genes, only WRN was previously known to associate with NMTC predisposition. Among PPSVs, BRAFV600E was most the prevalent and detected in 12 of the 29 (41%) tumors. Examining PPGVs/PPSVs among three patients who died from NMTC, one patient who died from papillary thyroid carcinoma/anaplastic thyroid carcinoma (PTC/ATC) led us to speculate that the PPGV ERCC4R799W may have increased the risk of PPSV TP53R273H acquisition. Among PPGVs identified in 18 cardiovascular risk genes, PPGVs in SC5NA, GYG1, CBS, CFTR, and SI are known to have causal and pathogenic implications in cardiovascular disease.
Conclusion:
In this cohort, most AA-NMTC patients exhibit favorable outcomes after therapeutic intervention given at cancer centers, suggesting that health care disparity is the major contributor for worse prognoses among AA-NMTC patients. Nevertheless, the clinical impact of PPGVs that might facilitate the acquisition of TP53 tumor mutations, and/or PPGVs that predispose individuals to adverse cardiovascular events, which could be exacerbated by therapy-induced cardiotoxicity, needs to be further explored. Integrated analysis of PPGV/PPSV profiles among NMTC patients with different stages of disease may help to identify NMTC patients who require close monitoring or proactive intervention.
Introduction
African Americans (AA) have higher death rates for many cancer types (
To date, however, these studies have mainly been conducted in tumors from individuals of European and Asian ancestry. 5,6 We previously reported that TG, BRCA1, and NSMCE2 haplotypes were uniquely found in four AA patients of >80% African (AFR) ancestry with radioiodine resistant disease via genome-wide association studies and that tumors available from three of these four AA patients were negative for BRAFV600E , NRASQ61R , and HRASQ61R tumor mutations. 7 In this study, we aimed to identify presumed pathogenic germ line and somatic variants (PPGVs and PPSVs) associated with progressive NMTC.
Among all the cancer survivors, cardiovascular disease (CVD) represents the second-most common cause of death after cancer. 8 The increased mortality among cancer survivors can, in part, be attributed to cardiotoxicity associated with cancer therapeutic agents. 9 Higher morbidity from CVD in AA individuals had been attributed to inequity in health care access and possibly AFR ancestry-specific genetic determinants of the disease, among other factors. 10 Recently, the American College of Cardiology reported that AA cancer patients are 71% more likely to experience heart damage following chemotherapy than EA patients. 11 Furthermore, AA cancer survivors are also at a higher risk of dying from CVD. 12 We propose that cancer treatment risk stratification can be further improved for individuals by considering genetic risk factors for adverse cardiovascular events, which could be exacerbated by therapy-induced cardiotoxicity. Thus, in addition to cancer-related genes, we also identified PPGVs known to be associated with CVD.
Materials and Methods
Subjects and whole-exome sequencing
All studies were conducted as per IRB 2018C0059 at The Ohio State University. Whole-exome sequencing (WES) was conducted on 37 DNA samples derived from blood (N = 33), normal thyroid tissue (N = 3), and normal lymph nodes (N = 1) of self-reported AA NMTC patients who consented to participate in both ORIEN/M2Gen and our IRB 2018C0059. Pertinent patient demographic and clinical information is shown in Table 1. Of these 37 patients, 32 paired tumor samples, primary tumor (N = 27) and/or lymph node metastases (N = 5), derived from 29 AA NMTC patients were available for WES, as multiple tumor samples were available from 3 patients (Fig. 1). As samples were ascertained over a multiyear time span, WES was performed by three different sequencing centers, including: Novogene, Inc. (Beijing, China), ORIEN/M2Gen, and the Institute for Genomic Medicine at Nationwide Children's Hospital (Columbus, OH).
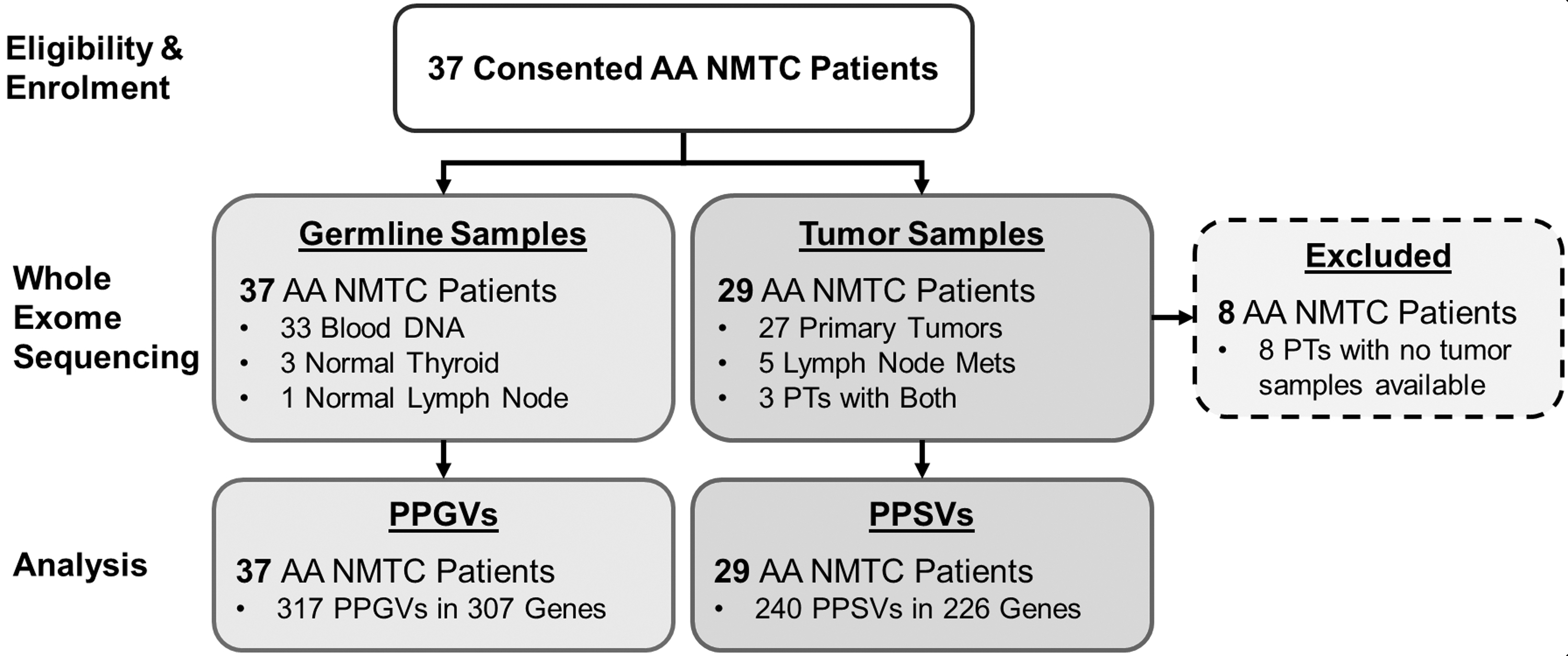
Patient enrollment and sample availability for WES. A total of 37 self-reported African American nonmedullary thyroid cancer patients consented to participate in ORIEN/M2Gen and/or in our IRB protocol. WES was performed on germ line DNA procured from 37 of 37 (100%) patients, and primary tumor and/or lymph node metastases from 29 of 37 (78%) patients, which were subsequently analyzed leading to the identification of 317 and 240 PPGVs and PPSVs, respectively. PPGV, presumed pathogenic germ line variant; PPSV, presumed pathogenic somatic variant; WES, whole-exome sequencing.
Patient Demographics and Clinical Information
A summarization of demographic and clinical information, including self-reported race, African ancestry (AdMIX), tumor histology, sex, TNM staging, ATA risk categorization, diagnosis age, years of follow-up, and disease status as of the most recent follow-up for the 37 African American nonmedullary thyroid cancer patients included in this study, is shown.
ATA, American Thyroid Association; ATC, anaplastic thyroid carcinoma; D, deceased; FTC, follicular thyroid carcinoma; FVPTC, follicular variant papillary thyroid carcinoma; ID, indeterminate response; mPTC, micro Papillary Thryoid Carcinoma; NED, no evidence of disease; PTC, papillary thyroid carcinoma; SD, standard deviation.
Variant effect prediction, filtering, and assessment of pathogenicity
The Baseplayer 13 program was used to consolidate all variant call files and to select variants with at least three altered reads. For PPGVs, a minimum read coverage of 10 and a minimum variant allele frequency (VAF) of 10% were selected. For PPSVs, a minimum read coverage of 20 and a minimum VAF of 5% were selected. Moreover, PPGVs were filtered to have Phred-scaled quality score for the assertion made in ALT allele (QUAL) over 100. PPGVs classified as long insertion-deletion (INDEL) variants with QUAL <300 were manually inspected and verified using IGV. 14
Variant Effect Predictor (VEP, Ensembl release 105, December 2021) 15 was applied to perform a comprehensive functional annotation of the variants and obtain population allele frequencies. To focus on rare potentially pathogenic variants, any variant with a combined population allele frequency of >0.01, >25 alleles observed for missense variants or >50 alleles observed for all other variants among the ∼20,000 AFR/AA samples in gnomAD, or >5 alleles observed with the 37 AA NMTC patients in this study were removed. Nonsynonymous variants were further evaluated for pathogenicity using functional prediction algorithms included in dbNSFP. 16 Moreover, VarSome Clinical (v11.2.4) was applied to obtain American College of Medical Genetics (ACMG) classification for all candidate variants. 17 To identify PPGVs and PPSVs, variants were excluded unless they had both a Combined Annotation Depletion Dependent (CADD) Phred-scaled score of ≥20 and VarSome Clinical (v11.2.4) ACMG classification of likely pathogenic or pathogenic.
Inference of genetic ancestry with admixture and assembly of gene panels
Ancestry analysis was performed by merging WES genotyping data for 37 normal tissues with 1000Genome samples in 5 super populations—Africans (AFR), Admixed Americans (AMR), East Asians (EAS), Europeans (EUR), and South Asians (SAS). Biallelic single nucleotide polymorphisms (SNPs) with minor allele frequency >0.05 were pruned by linkage disequilibrium with R-squared coefficient >0.1 in 50 bp windows advancing 10 SNPs at a time to select markers for the ancestry analysis. About 9400 independent common biallelic SNP markers were used in the ADMIXTURE v1.30 18 program to estimate AFR ancestry proportions for each sample using about 9400 independent common SNPs. PPGV/PPSVs enriched for AFR ancestry were identified by applying a Fisher's exact test when allele counts in the gnomAD African (AFR) are higher than those in non-Finish European (NFE) populations at a significance cutoff of p < 0.05.
Three gene panels assembled to characterize PPGVs and PPSVs occurring in genes with established roles in cancer and cardiovascular risk are shown in Supplementary Table S1.
Results
Analysis of PPGVs
After filtering, we identified 317 PPGVs in 307 genes in our cohort of 37 AA NMTC patients (Supplementary Table S2). PPGVs in genes known to be associated with hereditary cancer syndromes and NMTC predisposition, known cancer-related genes (KCRGs), and genes harboring polymorphisms associated with increased risk of CVD are shown in Figure 2. PPGVs with causal implication in disease via DisGeNET and genes causally associated with cancer via Qiagen Ingenuity Pathway Analysis (IPA) BioProfiler are indicated (Supplementary Table S2).

Presumed pathogenic germline variants identified in 37 African American non-medullary thyroid cancer patients. Pertinent clinical information is summarized in the top rows for each patient sequenced by NovoGene (NG) or M2Gen (M2G). Clinical features include pediatric patients (diagnosed at ≤20 years of age), patients with distant metastatic disease (M1), and patients who died from thyroid cancer (D). Disease status was evaluated by a physician at the most recent follow-up available and included no evidence of disease (NED), indeterminate response (ID), or deceased (D). Patient 1 died of complications unrelated to their thyroid cancer (D*). Presumed pathogenic germline variants (PPGVs) which occurred in the genes included in the Hereditary Cancer, Known Cancer-Related Genes (KCRGs), and Cardiovascular Risk gene panels are shown. Variant rsIDs are provided except when unavailable (“–”). Mutation type for each PPGV, total number of genes harboring PPGVs, and the name of each gene panel (numbered 1–7) is indicated in the bottom rows of the figure. AFR, African; ID, indeterminate response; KCRG, known cancer-related gene; M2G, M2Gen; NED, no evidence of disease; NG, NovoGene.
PPGVs in hereditary cancer genes or KCRGs
As shown in Figure 2, 11 PPGVs in 10 hereditary cancer genes—A2ML1, BMP1, ERCC4, ERCC6, LAMA5, PKD1, SLC19A2, TG, USB1, and WRN—were identified in 9/37 (24%) AA NMTC patients. PPGVs in TG and USB1 demonstrated AFR enrichment (p < 0.05, Fisher's exact test), PPGVs in A2ML1, ERCC6, and LAMA5 were not reported in gnomAD, and the remaining 6 PPGVs were not AFR enriched. PPGVs in 6 KCRGs—ARHGEF10L, COL2A1, LRP5, LRP6, MERTK, and SNX29—were identified in 5/37 (14%) AA NMTC patients. PPGV in MERTK demonstrated AFR enrichment, the PPGV in COL2A1 was unreported in gnomAD, and the remaining four PPGVs were not AFR enriched. There was no statistical difference in disease status between patients with or without PPGVs associated with cancer predisposition (p = 0.7023, Fisher's exact test).
PPGVs implicated in increased cardiovascular risk
As shown in Figure 2, 24 PPGVs in 18 genes associated with cardiovascular risk were identified in 18 of the 37 (49%) AA NMTC patients. PPGVs in DES and MYL3 were AFR enriched. Ten PPGVs in 7 genes—CFTR, CPS1, DPP4, GUG1, SCN5A, SI, and SYNE2—were not AFR enriched, and the remaining 13 PPGVs did not have allele frequencies available in gnomAD. Utilizing the DisGeNET database, seven PPGVs in five genes—SC5NA, GYG1, CBS, CFTR, and SI—are causally implicated in CVDs.
PPGVs in genes having causal association with cancer
Genes harboring PPGVs having causal association with cancer are shown in Supplementary Table S2. Among 11 PPGVs in 11 genes identified, PPGVs C11orf80E314* , ITGB3S471I , and PRNPG58W were AFR-enriched and PPGVs RAD54B *911X, DHCR7 (splice-acceptor variant), ALG8W353X , and ABCC2L809X did not have allele frequencies reported in gnomAD.
Analysis of PPSVs
Among 32 paired tumor samples from 29 AA NMTC patients, 240 PPSVs in 226 genes were identified (Supplementary Table S3). As shown in Figure 3, 52 PPSVs in 47 KCRG genes were identified in 25 of the 32 (78%) tumor samples derived from 24 of the 29 (83%) AA NMTC patients.
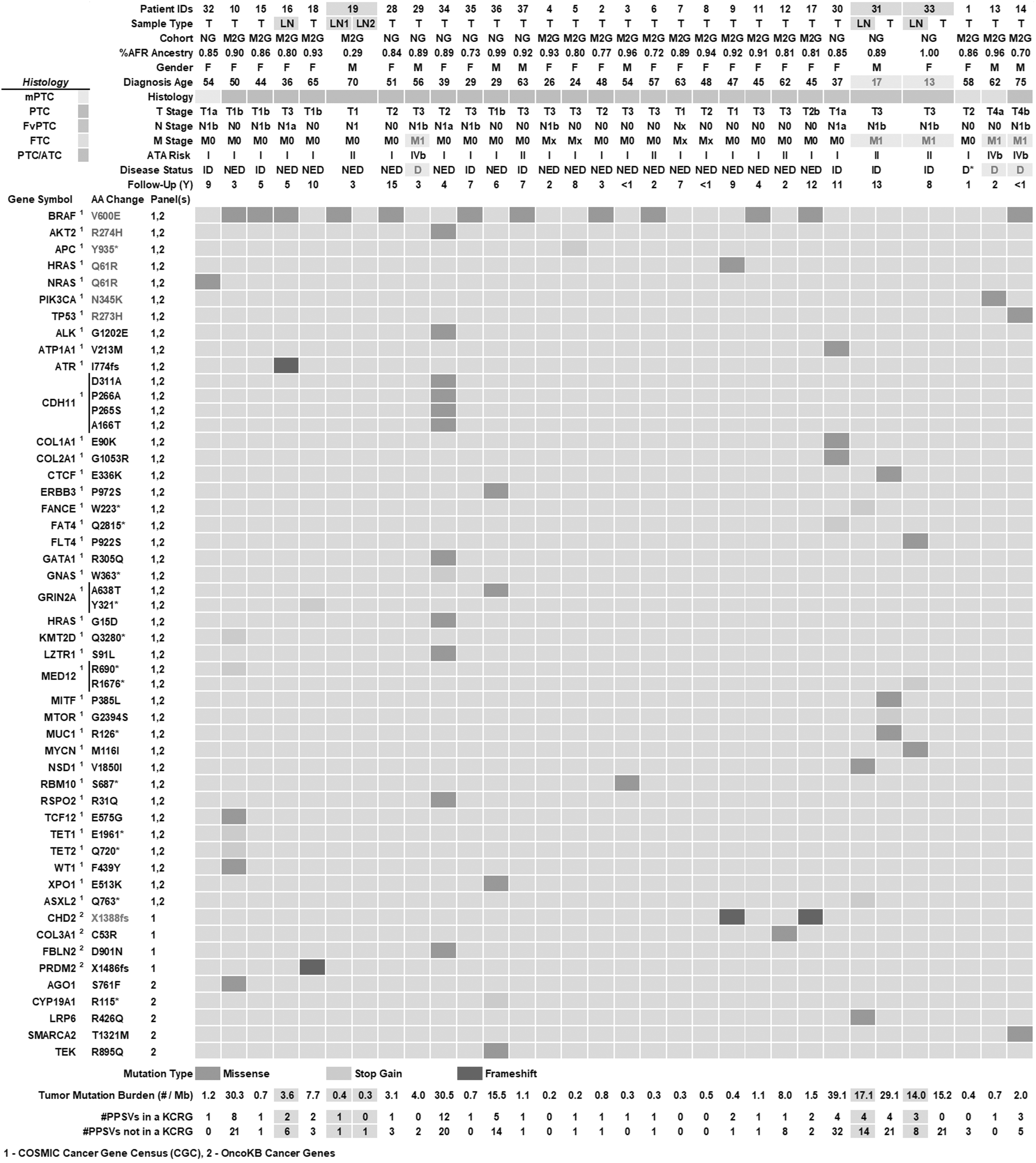
Presumed pathogenic somatic variants identified in 32 tumor samples derived from 29 African American non-medullary thyroid cancer patients. Pertinent clinical information is summarized in the top rows for each patient with DNA extracted from tumor (T) and/or lymph node metastases (LN) and sequenced by NovoGene (NG) or M2Gen (M2G). Clinical features include pediatric patients (diagnosed at ≤20 years of age), patients with distant metastatic disease (M1), and patients who died from thyroid cancer (D). Disease status was evaluated by physician as of the most recent follow-up available and included no evidence of disease (NED), indeterminate response (ID), or deceased (D). Patient 1 died of complications unrelated to their thyroid cancer (D*). Gene symbol, amino acid change, and inclusion of a gene in either COSMIC Cancer Gene Census (1) or OncoKB Cancer Genes (2) panel are shown for each PPSV. The census tier for genes in the COSMIC Cancer Gene Census are indicated by superscripts and are either Tier 1 ( 1 ) or Tier 2 ( 2 ). Mutation type for each PPSV, tumor mutation burden (TMB), calculated as the total number of candidate somatic mutations per megabase (Mb) of the coding tumor genome, and the total number of genes harboring PPSVs are shown in the bottom rows of the figure. LN, lymph node metastases; T, tumor; TMB, tumor mutation burden.
PPSVs known to contribute to cancer development and/or progression
As shown in Figure 3, PPSVs previously reported in NMTC such as BRAFV600E , AKT2R274H , APCY935*, HRASQ61R , NRASQ61R , PIK3CAN345K , and TP53R273H were detected in tumors from 17/29 (59%) AA NMTC patients. BRAFV600E was the most prevalent PPSV occurring in 12/29 (41%) AA NMTC patients. Among patients carrying PPSV BRAFV600E , patient 14 who had concurrent PTC/anaplastic thyroid carcinoma (ATC) also harbored PPSV TP53R273H . Tumor mutation burden (TMB) did not correlate with disease status, yet both pediatric patients had higher TMB than others (p = 0.0206, Welch's t-test).
AFR-enriched PPSVs or PPSVs with increased incidence among AA cancer patients
Among 19 PPSVs with allele frequencies reported in gnomAD, CHD2X1388fs (Fig. 3) and DCLRE1CR64Q (Supplementary Table S3) are AFR-enriched PPSVs. Among 35 PPSVs reported in the Genomic Data Commons (GDC) pan-cancer data set, 5 were reported exclusively in cancers from AA patients, including CA12P181L (N = 2 AA patients, oropharyngeal and colon cancers), GPAA1R484Q (N = 2 AA patients, cervical and ovarian cancers), COL1A1E90K (N = 1 AA patient, endometrial cancer), MED12R690 *(N = 1 AA patient, cervical cancer), and PCDH15R1120 * (N = 1 AA patient, stomach cancer).
Of interest, 140/240 PPSVs (58%) have neither been reported in gnomAD Exomes (v2.1.1) nor in the GDC pan-cancer data set. Gene set enrichment analysis of genes carrying unreported PPSVs indicate that these PPSVs may have an impact in heart development and morphogenesis (p = 4.36 × 10−8), thyroid hormone signaling (p = 1.01 × 10−3), and methylcytosine dioxygenase activity (p = 9.18 × 10−3).
Discussion
Clinical significance of PPGVs in hereditary cancer genes in NMTC predisposition
Among PPGVs identified in 10 hereditary cancer genes, only WRN has been previously associated with NMTC predisposition. 19 PPGVs in A2ML1, 20 BMP1, 21 ERCC4, 22 PKD1, 23 and USB1 24 have been reported to predispose for diseases or syndromes with increased risk of various cancers but have not been previously recognized in thyroid cancer predisposition. We previously reported a TG haplotype in AA-NMTC patients of >80% AFR ancestry that associated with radioiodine resistant disease via a genome-wide association study. 7 ERCC6 PPGVs are not thought to predispose to cancer. 25 Roles of PPGVs in LAMA5 and SLC19A2 on cancer predisposition are less defined. To this date, only few variants have been identified in familial NMTC cases, which completely cosegregate with cancer occurrence. 26
Furthermore, the majority of cancer predisposing germ line variants neither significantly contribute to nor have clearly defined roles in clinical outcomes in pan-cancer 27 or thyroid cancer. 28 Accordingly, the 6/9 patients carrying PPGVs in hereditary cancer genes and 5/5 patients carrying PPGVs in KCRGs have no evidence of disease following therapeutic intervention, suggesting that these PPGVs neither contribute to worse prognosis nor compromise treatment responsiveness. However, we urge caution in the interpretation of these findings, as our small sample size limits our ability to perform adequate statistical analyses to draw robust conclusions regarding these potential associations.
PPGVs facilitating acquisition of TP53 tumor mutations, if validated, could further improve risk stratification for early intervention
Most AA or EA NMTC patients with familial or sporadic thyroid cancer have favorable prognosis after surgical resection with or without subsequent radioiodine therapy. However, ATC arising from well-differentiated thyroid cancer through accumulation of additional genetic abnormalities 29 although rare is frequently lethal with an average survival rate of 5–6 months after diagnosis. ATC transformation is mainly facilitated by acquisition of TP53 somatic mutations, as the process has been recapitulated experimentally in mouse models 30 and supported by high prevalence of TP53 mutation in 73% of ATC. 29 Thus, it would be of clinical significance to identify PPGVs that promote acquisition of TP53 mutations in NMTC for early intervention.
The ERCC4R799W PPGV was detected in patient 14, whose PTC harbored both BRAFV600E and TP53R273H tumor mutations and died within 1 year of diagnosis with PTC/ATC. ERCC4R799W is causally implicated in the xeroderma pigmentosum (XP) group F 22,31 that is inherited in an autosomal recessive pattern. XP is strongly associated with the development of multiple cancers, particularly those of the skin, due to significantly increased sensitivity to ultraviolet (UV) radiation. 32,33 XP patients have a higher incidence of TP53 mutations, specifically C to T transitions at di-pyrimidine sites, which are hallmarks of UV-induced DNA damage. 34,35 XP patients are also sensitive to other forms of radiation due to their genetic inability to repair DNA damage. Accordingly, we speculate that the PPGV ERCC4R799W , through loss of heterozygosity in PTC, might increase the risk of PPSV TP53R273H acquisition leading to ATC transformation.
This notion is consistent with previous integrated analysis of germ line and somatic mutation profiles that implicate some germ line variants may dictate the acquisition of particular somatic mutations. 27,36,37 Nevertheless, our speculation necessitates further investigation on PPGVs associated with TP53 tumor mutations among NMTC patients at different stages of disease. To this date, our study is the first attempt to conduct integrated analysis of PPGVs/PPSVs for thyroid cancer patients. Identification of PPGVs that promote TP53 tumor mutations in thyroid cancer would hold high clinical significance, enabling strategic implementation of early intervention.
Patients who have PPGVs in cardiovascular risk genes require proactive strategies to prevent or manage cardiotoxicity induced by chemotherapy or tyrosine kinase inhibitor therapy
A recent study reported that AA cancer survivors were more likely to die from CVD versus EA cancer survivors across 18 cancer types. 12 Thus, we were interested in identifying potential CVD-risk genes in our cohort. We identified seven PPGVs with pathogenic implications in the cardiovascular risk genes SC5NA, GYG1, CBS, CFTR, and SI among six AA NMTC patients. Fortunately, these six patients did not require advance therapy after the initial therapeutic intervention. However, if these patients had progressive disease and receive thyroid hormone supplementation, they could be at higher risk of cardiovascular complications associated with advanced therapy. 9,38 Screening patients for existing cardiovascular abnormality before treatment and monitoring for treatment-related cardiotoxicity are routinely performed in patients treated with therapeutic agents known to have cardiovascular toxicity.
Thus, we propose that profiling of PPGVs in cardiovascular risk genes for patients who are to receive therapy associated with cardiovascular toxicity may help to identify patients at risk for preventive measures. Further study is warranted to investigate if patients carrying cardiovascular risk PPGVs have a higher incidence of cardiovascular adverse events associated with thyrotropin (TSH) suppression therapy with levothyroxine supplementation.
SC5NAR1626H , a gain-of-function variant, 39 has been reported in two individuals with prolonged QT syndrome 40,41 and one individual with atrial fibrillation. 39 GYG1D102H is associated with severe cardiomyopathy and causally implicated in glycogen storage disease. 42,43 CBSI278T represents the most frequently observed mutation in patients with cystathionine ß-synthase (CBS) deficiency, 44,45 a syndrome causing hyperhomocysteinemia, an established risk factor of CVD. 46 SIV577G has been casually implicated in the metabolic disorder congenital sucrase isomaltase deficiency (CSID). 47,48 Of the four PPGVs reported in CFTR, CFTRG480C , CFTRF508C , and CFTRR726fs have pathogenic implications in cystic fibrosis (CF). 49 Pulmonary hypertension is commonly observed in patients with CF and can result in associated cardiovascular dysfunction. 50 The CFTRG480C mutation was identified as a causal variant in an AA individual with CF and pancreatic insufficiency. 51 Of note, CF incidence is rare in AA and only represents 1 in 17,000 new cases (CF: MedlinePlus Genetics).
However, PPGV profiling in cardiovascular risk genes should be applied to both AA and EA NMTC patients who are to receive therapeutic agents associated with cardiovascular adverse events. It is notable that patient 31, a pediatric patient who had T3N1bM1disease diagnosed at age 17, carries both the CFTRF508C and CBSI278T PPGVs.
Clonal expansion of key PPSVs associated with progressive disease portends poor clinical outcome
In thyroid cancer, high TMB, and thus a higher incidence of PPSVs, was neither associated with more advanced stages of thyroid cancer nor poor clinical outcomes (see patients 10, 34, and 30 who had TMB of >30/Mb in Fig. 3). This is probably due to most subclones carrying distinct PPSVs failing to acquire growth advantage at the time of surgical resection. In contrast, distinct PPSVs such as those affecting the TERT promoter, TP53, PI3K/AKT/mTOR signaling, or chromatin remodeling complexes can confer a growth advantage, leading to clonal expansion of subclones harboring these PPSVs that drive cancer progression. 5 Similar to EA NMTC pediatric patients (REF), two pediatric patients 31 and 33 exhibit favorable outcomes during 8–13 years of follow up, despite having more advanced TNM staging (T3N1bM1) at diagnosis.
Among three male patients who died from thyroid cancer, patient 14 died from PTC/ATC carrying PPSVs TP53R273H and BRAFV600E ; patient 13 died from follicular thyroid carcinoma carrying PPSV PIK3CAN345K ; and patient 29 died from PTC likely carrying fusion oncogene and/or TERT promoter mutation, which could not be detected by WES analysis. Of interest, both TP53 and PIK3CA mutations have been reported to be significantly enriched in ATC with 73% and 18% incidence, respectively. 29 The APCY935* stop-gained mutation has been implicated as a causal variant in familial adenomatous polyposis (FAP), 52 and has been observed in multiple colorectal adenomas (MCRAs). 53 In addition, stop-gained mutations in APC have been observed in both breast 54 and colorectal 55 cancers. The spectrum of NMTC ranges from well-differentiated thyroid cancer to poorly differentiated thyroid cancer and then the ultimately lethal ATC through the accumulation of “key” additional PPSVs. 6,29
Thus, it would be of clinical significance to identify risk factors that facilitate acquisition of “key” PPSVs associated with high mortality. Consequently, risk-guided early intervention can be applied before the development of lethal ATC. Of note, male AA NMTC patients had a significant higher initial T staging (p = 0.0330, Mann–Whitney U test) and M staging (p = 0.0127, Mann–Whitney U test) than female patients, consistent with previous studies suggesting that male NMTC patients have worse outcomes. 56
The heterogeneity of PPSVs among tumors and metastases poses a challenge to achieve complete response to target therapy
Of note, PPSVs can differ significantly between the primary tumor and lymph node metastases as seen in patients 31 and 33, as well as among different lymph node metastases in patient 19. The heterogeneity in PPSVs across tumors and metastases would not have an impact on clinical outcome provided that tumors and metastases can be surgically resected and/or responsive to radioiodine therapy. Otherwise, it can pose a significant challenge to apply target therapy for patients who had progressive disease with multiple lesions carrying distinct PPSVs. This heterogeneity may, in part, explain why tyrosine kinase inhibitors (TKIs) have shown therapeutic efficacy in some patients with progressive thyroid cancers, 57 –59 but very few patients achieve complete responses to TKI targeted therapies. Recent spatial transcriptomic studies have further underscored the challenges, revealing extensive intratumor heterogeneity in thyroid cancer, 60,61 which adds an additional layer of complexity to achieving treatment efficacy.
Conclusion
This study is the first investigation on integrated analysis of both germ line and somatic variants in NMTC patients. A graphical summary of our key findings is shown in Figure 4. Our cohort comprised AA NMTC with high AFR ancestry (median AFR ancestry 89% ± 13%), who were treated at cancer hospitals. The fact that most AA NMTC patients in this cohort exhibit favorable outcomes with standard therapeutic intervention suggests that most of the AFR-enriched PPGV/PPSVs identified herein neither contributed to poor prognosis nor affected therapeutic responsiveness. Examining both PPGVs and PPSVs in patients with different stages of disease prompted us to speculate that PPGV ERCC4R799W may increase the risk of PPSV TP53R273H acquisition that resulted in anaplastic transformation, a novel finding that warrants further investigation.
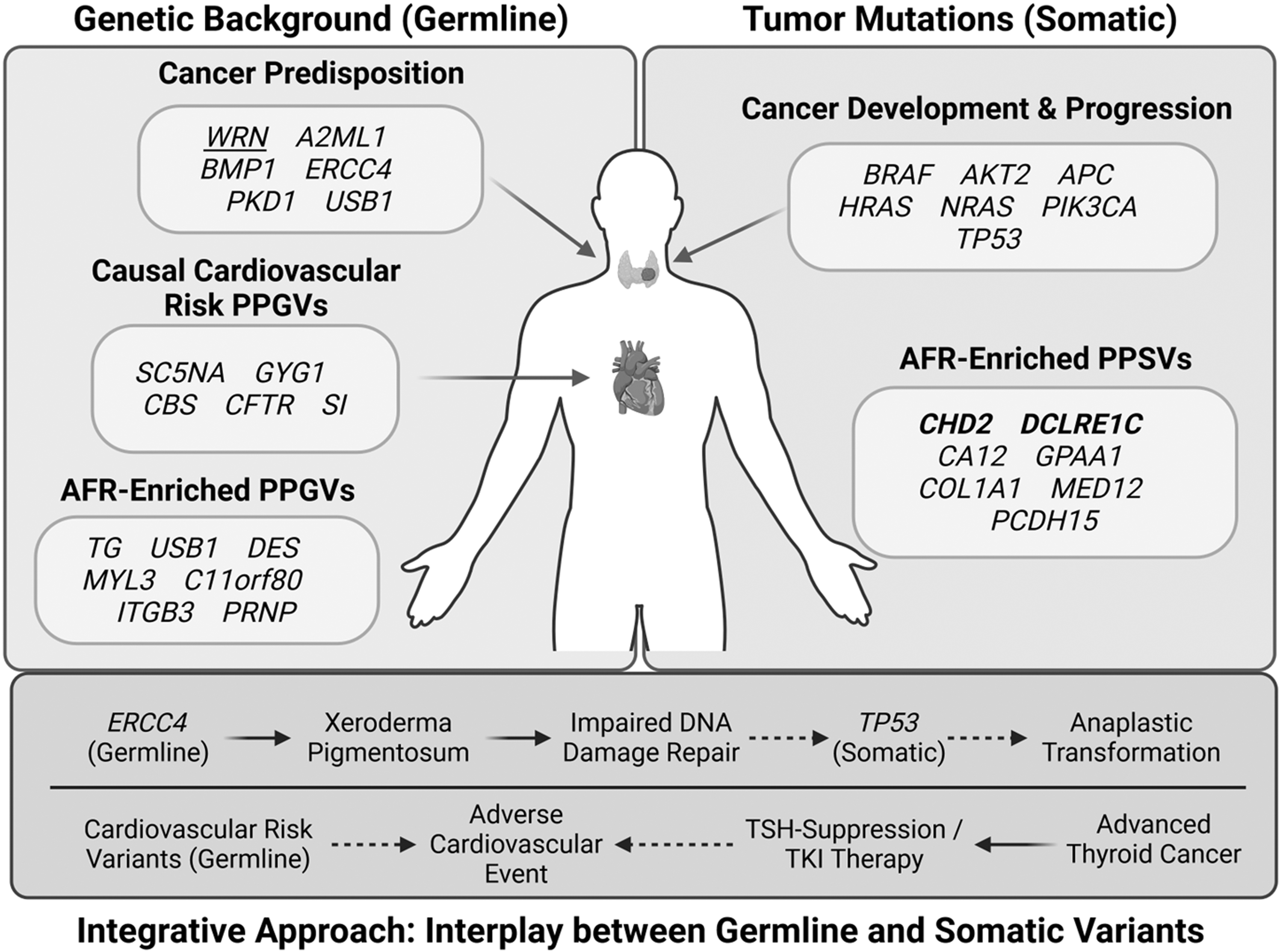
Graphical summarization of key study findings from PPGV and PPSV. Genes harboring PPGVs known to be associated with cancer predisposition, cardiovascular risk, or demonstrating AFR enrichment are shown in the left panel. WRN (underlined) has been previously shown to be associated with thyroid cancer predisposition. Genes harboring PPSVs implicated in cancer development and progression, AFR enrichment (bolded), or increased incidence in African American cancer patients are shown in the right panel. AFR-enriched PPSVs in CHD2 and DCLRE1C are highlighted in bold. Integrated analysis on both PPGVs and PPSVs led us to hypothesize that the ERCC4 PPGV may contribute to TP53 PPSV acquisition, and that CVD risk PPGVs can be used to improve thyroid cancer patient risk stratification (bottom panel). CVD, cardiovascular disease. Figure created with BioRender.
In addition, we reported seven PPGVs with causal implication in the cardiovascular risk genes SC5NA, GYG1, CBS, CFTR, and SI, which may help to identify patients who need preventive measures to minimize the impact of treatment-related cardiotoxicity.
Footnotes
Acknowledgments
ORIEN, M2Gen—Michael Hinton, Nancy Single, Laura Monovich, Jessica McCoy, and Michelle Churchman. The OSU Comprehensive Cancer Center Genomics Shared Resources with the Institute of Genomic Medicine at Nationwide Children's Hospital performed WES.
Authors' Contributions
Z.A.H.: conceptualization, methodology, formal analysis, investigation, data curation, writing original draft, review and editing, and visualization. S.L.: conceptualization, methodology, formal analysis, investigation, data curation, writing original draft, review and editing, and visualization. P.B.: investigation, data curation, and review and editing. H.H.: investigation and review and editing. F.N.: investigation. C.V.: investigation and review and editing. A.E.T.: methodology, review and editing, and supervision. M.D.R.: review and editing. S.M.J.: conceptualization, methodology, formal analysis, investigation, resources, writing original draft, review and editing, supervision, project administration, and funding acquisition.
Author Disclosure Statement
The authors of this study have nothing to disclose.
Funding Information
This work was supported, in part, by the OSU Comprehensive Cancer Center Bridge Fund and Seed Award (to S.M.J.) and National Cancer Institute P30 CA16058 (Genomics Shared Resource) R01 CA265975; P50CA168505 (to M.D.R.); and 1 R01 CA265975 and 1 R01 CA CA215151 (to A.E.T.).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3