
Abstract
Background:
Thermal ablation (TA) is an established therapeutic option alternative to surgery in patients with solid benign thyroid nodules causing local symptoms. However, a variable part of thyroid nodules remain viable after these nonsurgical treatments, and as many as 15% of nodules treated with TA may require a second treatment over time. This study aimed to evaluate the outcomes of TA re-treatment on symptomatic benign thyroid nodules where the volume decreased by <50% after the first procedure ( = technique inefficacy).
Methods:
We performed a multicenter retrospective cohort study including patients who underwent re-treatment with TA for benign thyroid nodules, whose volume decreased by <50% after initial treatment. The primary aim was to evaluate volume and volume reduction ratio (VRR) over time and compare the 6- and 12-month VRR after first versus second treatment. The secondary aim was to identify protective or risk factors for technique inefficacy, regrowth, and further treatments, expressed as adjusted hazard ratios (HRs) and confidence interval [CI], after adjustment for sex, age, nodule volume, structure and function, nodule regrowth or symptom relapse, technique used and if the same technique was used for the first and second TA and time between them.
Results:
We included 135 patients. Re-treatment led to VRR of 50% and 52.2% after 6 and 12 months. VRR after re-treatment was greater than after first treatment in small and medium size nodules (<30 mL), while there were no differences for large nodules (>30 mL). After re-treatment technique inefficacy rate was 51.9%, regrowth rate was 12.6%, and further treatment rate was 15.6%. Radiofrequency ablation (RFA) was protective toward technique inefficacy (HR = 0.40 [CI 0.24–0.65]) and need of further treatments (HR = 0.30 [CI 0.12–0.76]). Large nodule volume (>30 mL) was associated with increased risk of re-treatment (HR = 4.52 [CI 1.38–14.82]).
Conclusions:
This is the first study evaluating the outcomes of re-treatment on symptomatic benign thyroid nodules with a VRR <50% after the initial TA treatment. Best results were seen in small and medium nodules (<30 mL) and after RFA. Prospective confirmatory studies are needed.
Introduction
In 2022
TA is an outpatient procedure performed using different modalities. Technically, either an electrode-needle generating an alternating electric field (in case of radiofrequency ablation [RFA]) or one or more optical fibers conveying laser light (in case of laser ablation [LA]), are inserted into the nodule under local anesthesia and ultrasound (US) guidance, to induce rapid heating of the target zone. Heating is followed by coagulative necrosis, and, over time, by fibrotic changes and progressive nodule shrinkage. This is associated with symptom improvement or disappearance, as well as with improvement of health-related quality of life. 8 General principles for the safe performance, training, and adoption of ablation techniques for benign thyroid nodules have been recently published. 9
Although TA significantly decreases thyroid nodule volume, the thyroid nodule usually does not disappear. Follow-up studies have shown that technique efficacy (i.e., volume reduction ≥50% after one year from treatment) is not always achieved, and as many as 20% of nodules might regrow, such that 15% of nodules may require a second treatment. 10 Re-treatments are more likely in case of larger baseline nodule volume, lower energy delivered, unsatisfactory 12-month volume reduction (i.e., technique inefficacy) and nodule regrowth. 10 Several articles report the effects of multiple treatment sessions on the same nodules, 11 but the effects and outcomes of second treatments remain to be clarified.
The aim of this study was to evaluate the effect of re-treatment with TA on symptomatic benign thyroid nodules where the volume decreased by <50% after the first procedure (i.e., technique inefficacy). The primary aim of this study was to evaluate volume and volume reduction ratio (VRR) over time and compare the 6- and 12-month VRR after initial treatment versus re-treatment. The secondary aim was to evaluate the effects of re-treatment in terms of technique inefficacy, nodule volume regrowth, and the need for further interventions, as well as to identify protective or risk factors for these outcomes.
Materials and Methods
Study design
This is a multicenter retrospective cohort study on benign thyroid nodules that were retreated with TA due to technique inefficacy, as defined by VRR <50% after first treatment. The primary aim of this study was to evaluate volume and VRR over time and compare the 6- and 12-month VRR after initial treatment versus re-treatment. The secondary aim was to evaluate the effects of re-treatment in terms of technique inefficacy, nodule volume regrowth, and the need for further interventions, as well as to identify protective or risk factors for these outcomes.
The study protocol was presented during the conference “Minimally-invasive treatments of the thyroid (MITT) 2023. State of the art in Europe,” held in Milan in February 2023. The Italian Centers belonging to the MITT group were invited with an open call to contribute with patient data and 10 centers participated in the evaluation (1 Center in Lecce, 2 in Milano, 1 in Modena, 1 in Napoli, 1 in Perugia, 3 in Torino, and 1 in Trieste).
Patient inclusion criteria were (i) two separate benign fine-needle aspiration cytology reports before first treatment (i.e., Bethesda II) (10, 11); (ii) VRR <50% after first treatment; (iii) first and second TA performed by the same operator and in the same center; (iv) 6- and/or 12-month outcome data after re-treatment; and (v) consent to use patients' data for study purposes. Exclusion criteria were (i) VRR ≥50% and no regrowth after the initial treatment; (ii) very large volume thyroid nodules (volume >100 mL).
This study was conducted in accordance with the declaration of Helsinki, and the protocol was approved by the Institutional Review Board of the Comitato Etico Unico Regionale Friuli Venezia Giulia CEUR FVG (268_2019 FYTNAB). Patients provided informed consent for the use of their data for this study purposes.
Procedures
RFA was performed with 18-G needles and the moving shot technique, 12,13 median energy delivered was 1024 J/mL (190-9182). LA was performed with one to three optical fibers and a 1064 nm diode laser source. 6,14 The number of fibers depended on nodule volume and morphology, median energy delivered was 480 J/mL (165-3716).
Definitions
Nodules were classified as small, if their volume was <15 mL; medium, if their volume was between 15 and 30 mL, and large, if their volume was >30 mL and 100 mL. 15 Nodules with a volume >100 mL were considered as very large nodules, 16 and they were excluded from this study. Nodule structure was classified as solid if the fluid component was ≤10%, predominantly solid if the fluid component was between 11% and 50%, predominantly cystic if the fluid component was between 51% and 90%, and cystic if the fluid component was >90%. 17
Autonomously functioning thyroid nodules (AFTN) were defined based on thyrotropin <0.4 μU/mL and positive thyroid scintigraphy. Technique efficacy was defined as a volume reduction ≥50% after one year from the treatment. 17 Technique inefficacy was defined as any volume reduction <50% after at least six months from the treatment. Regrowth was defined as a ≥50% increase compared with the previous smallest volume at US examination. 17 Symptoms refer to local symptoms, such as neck discomfort or pain, cough, foreign body sensation, and cosmetic concerns, and their presence was assessed by clinical record review.
Timeline of patients' follow-up
The timeline of patients' follow-up is shown in Supplementary Figure S1. During the pre-re-treatment period, Tbaseline is the date of patient's first visit before any treatment was performed; T6 first treatment is the date of the visit performed 6 months after the first treatment; T12 first treatment is the date of the visit performed 12 months after the first treatment; Tlast visit is the date of the last visit performed after the first treatment and before re-treatment. During the re-treatment period, the follow-up visits started at T0 and ended at T n , the last visit done by each patient after re-treatment. The nodule volume was measured at each visit (Tx), and the VRR after the first procedure and after re-treatment were calculated compared with the measurements taken at Tbaseline and T0, respectively.
Statistical analyses
All the statistical analyses were performed using SAS (version 9.4; SAS Institute, Inc., Cary, NC). Categorical variables are reported as frequencies and percentages, and continuous variables as mean ± standard deviation (SD) and median stratified by each outcome. Variations over time of nodules' volume and VRR after re-treatment were evaluated applying the Friedman test for repeated measures in the whole cohort. Mean ± SD, median, first (Q1) and third quartiles (Q3) were reported.
The paired difference in volume of nodules (and VRR) between (i) T6 first treatment and T6 and (ii) T12 first treatment and T12 were evaluated with Wilcoxon signed-rank test, both in the entire cohort and stratified according to the nodule's volume category at Tbaseline and by technique (primary aim). Mean ± SD, median, first (Q1) and third quartiles (Q3) were reported.
Simple and multiple Cox proportional hazard models were performed to assess the association between re-treatment outcomes (technique inefficacy, nodule's volume regrowth, and further treatment), and different covariates, to identify protective or risk factors (secondary aim). In the Cox multiple proportional hazard analysis, the covariates were automatically selected using the backward selection with a p-value <0.20 according to Wald chi-square. The proportional hazard assumptions were verified for each model. Hazard ratio (HR) and confidence interval [CI] were reported.
In particular, in the Cox proportional hazard models, the following outcomes were examined: (i) technique inefficacy, defined as VRR <50% between Tx and T0, (ii) nodule's volume regrowth, defined as VRR ≥50% increase compared with the previous smallest volume at US examination, (iii) a further (third) treatment, defined as any treatment performed after T n . For each patient included in the study cohort, the period of follow-up started at T0 and ended with the occurrence of the first of the following event: the event of interest or the last visit T n . For each patient, person-time was appropriately computed according to each outcome.
In addition, in these models, the following covariates were considered: sex; age at Tbaseline; nodule's volume at Tbaseline in categories (small/medium/large); nodule's structure at Tbaseline (solid/predominantly solid); nodule's function at Tbaseline (non-AFTN/AFTN); nodule's volume regrowth at each Tx (yes/no); technique used at re-treatment (LA/RFA); a variable that specifies if the same technique was used as compared to the first treatment (yes/no); symptom relapse before re-treatment (yes/no); time (in month) elapsed between the first treatment and the last visit before re-treatment.
Results
Description of the patients and treatments
Data from 193 patients with symptomatic benign thyroid nodules that were retreated with TA were collected. We excluded 48 nodules with a satisfactory response to first treatment (VRR >50% and no regrowth), 3 patients whose data were incomplete, and 7 very large thyroid nodules (>100 mL). Our final cohort comprised 135 patients with symptomatic benign thyroid nodules where the volume decreased <50% after first procedure, and who underwent a re-treatment with TA (Fig. 1).
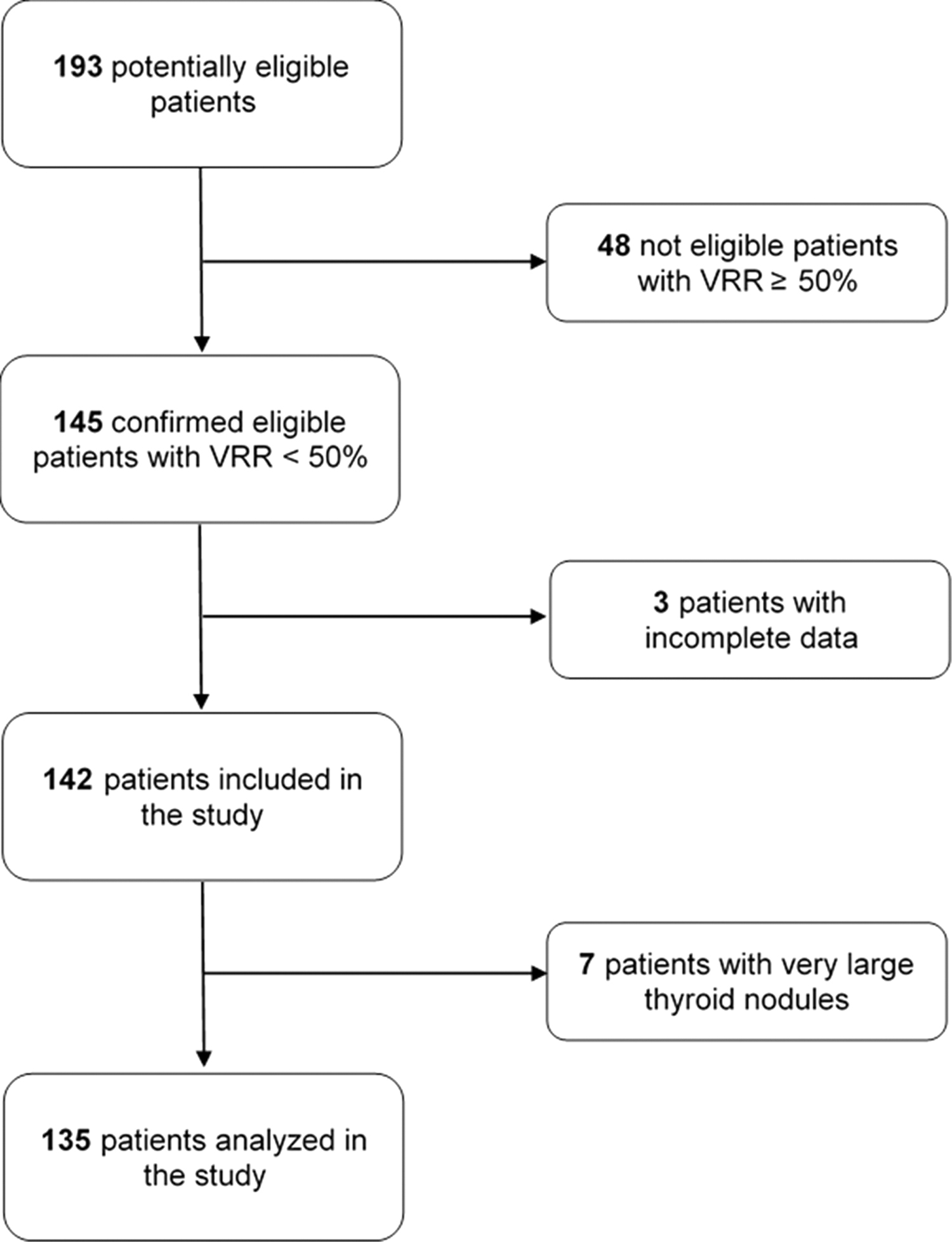
Flowchart of the criteria used for the selection of patients analyzed in the study.
As shown in Table 1, median age of patients was 54 years (interquartile range [IQR] 18) and 75.6% (102/135) were women. As for nodule characteristics, 28.2% (38/135) of patients had a small nodule, 31.9% (43/135) had a medium nodule, and 40% (54/135) had a large nodule. Nodules were solid in 62.2% (84/135) of patients, and the remaining 37.8% (51/135) were predominantly solid. Nodules were nonfunctioning in 91.1% (123/135) of patients.
Patient Characteristics
AFTN, autonomously functioning thyroid nodules; LA, laser ablation; RFA, radiofrequency ablation; SD, standard deviation.
The earliest time point at which re-treatment was considered was six months after the first treatment. The median time elapsed between the first treatment and the last visit before re-treatment was 24 months (IQR 36). Before re-treatment, nodule regrowth was recorded in 23% (31/135) of patients, presence or relapse of symptoms was recorded in 74.8% (101/135) of patients, thyrotoxicosis was recorded in 6.7% (9/135) of patients ( = 75% [9/12] of patients in the AFTN subgroup). In 50 patients (mostly those with nodule regrowth) a new cytological assessment was performed before re-treatment and the results were consistent with Bethesda II cytology in 92% of them (46/50), Bethesda I in 4% of them (2/50), and Bethesda III in 4% of them (2/50).
In 66.7% (90/135) of patients, the technique of re-treatment was RFA, while in 33.3% (45/135) of patients it was LA. In 92.6% (125/135) of patients, the technique used for re-treatment corresponded to the same technique used for the first procedure. In the remaining few cases, the technique was changed from LA to RFA, mostly because LA had been the first TA technique that was introduced in clinical practice, followed by RFA. After re-treatment, the number of patients for each time point of follow-up and length of follow-up are reported in Figure 2A and B.
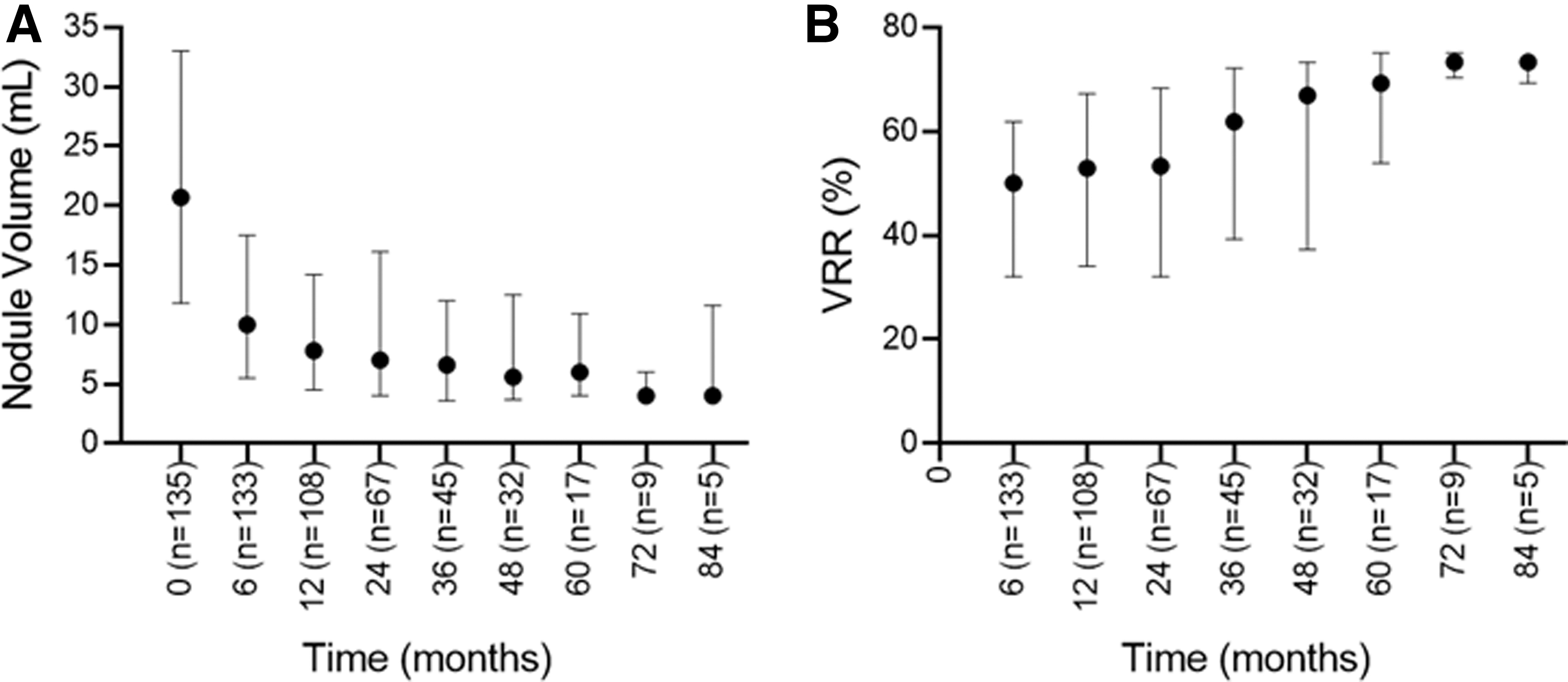
Distribution of nodule volume and VRR after re-treatment in the entire cohort. Length of follow-up after re-treatment and number of patients are specified for each time point. Data are expressed as first quartile (Q1), median and third quartile (Q3) of Friedman test. (
Nodule volume and VRR after 6 and 12 months from first procedure and re-treatment
After re-treatment, nodule volume and VRR changed over time (as shown in Fig. 2A, B). We compared the nodule volume and VRR measurements obtained at T6 first treatment and at T12 first treatment to those obtained at T6 and at T12 after re-treatment. Significant paired differences were found in the whole cohort (as shown in Fig. 3A, B and Supplementary Table S1). In particular, re-treatment was more successful than first treatment in terms of nodules' volume reduction. In the whole cohort, the VRR was 39.2% (25.0–50.4) at T6 first treatment as compared with 50% (32.0–61.8) at T6 after re-treatment, p < 0.001 for paired analysis. Likewise, the VRR was 36.7% (20.2–51.4) at T12 first treatment as compared with 52.2% (32.9–66.1) at T12 after re-treatment, p < 0.001 for paired analysis.

Distribution of 6- and 12-month nodule volume and VRR after first treatment and re-treatment. Data are expressed as first quartile (Q1), median and third quartile (Q3). Paired differences were evaluated with Wilcoxon signed-rank test. p < 0.05 are reported. (
After stratification for nodule volume at Tbaseline, re-treatment led to greater VRR than first treatment in small and medium nodules (<30 mL) at T6 and at T12, but not in large nodules (>30 mL) where the VRR did not differ between first treatment and re-treatment (Fig. 3B and Supplementary Table S1). In particular, in small nodules, the VRR was 32.9% (18.5–54.0) at T12 first treatment, as compared with 52.5% (36.4–67.2) at T12 after re-treatment, p < 0.001 for paired analysis. In medium nodules, the VRR was 34.7% (18.5–54.1) at T12 first treatment, as compared with 54.1% (46.4–69.2) at T12 after re-treatment, p < 0.001 for paired analysis. In large nodules, the VRR was 39.1% (24.3–47.1) at T12 first treatment, as compared with 41.8% (27.6–62.1) at T12 after re-treatment, p = 0.09 for paired analysis.
After technique stratification, re-treatment significantly reduced nodule volume in both LA+LA and RFA+RFA subgroups (Fig. 3C). Re-treatment led to greater VRR than first treatment at T6 in the RFA+RFA subgroup and at T12 in both LA+LA and RFA+RFA subgroups (Fig. 3D and Supplementary Table S2). In particular, in the LA+LA subgroup, the VRR was 30% (12.3–47.1) at T12 first treatment, as compared with 43.8% (26.4–53.3) at T12 after re-treatment, p < 0.037 for paired analysis. In the RFA+RFA subgroup, the VRR was 39.6% (23.8–54.1) at T12 first treatment, as compared with 58.4% (43.1–69.9) at T12 after re-treatment, p < 0.001 for paired analysis.
Technique inefficacy, regrowth, and further treatments
Technique inefficacy (VRR <50% after re-treatment) was observed in 70 patients (51.9%), as shown in Table 2. In a Cox proportional hazards model, RFA was independently inversely associated with technique inefficacy (HR = 0.4 [CI 0.24–0.65]). Regrowth was observed in 17 patients (12.6%) as shown in Table 3. There were no variables that were found to be independently associated with regrowth. Further treatments of thyroid nodules were observed in 21 patients (15.6%), as shown in Table 4. Large nodule volume at baseline was independently associated with further treatments over time (HR = 4.52 [CI 1.38–14.82]), and the use of RFA was inversely independently associated with requiring further treatments (HR = 0.3 [CI 0.12–0.76]).
Predictive Variables of “Technique Inefficacy” (Volume Reduction Ratio <50%) After Re-Treatment
A p-value <0.05 was considered significant.
[CI], confidence interval; HR, hazard ratio; VRR, volume reduction ratio.
Predictive Variables of “Nodule Regrowth” After Re-Treatment
A p-value <0.05 was considered significant.
Predictive Variable of Further Treatments After Re-Treatment
A p-value <0.05 was considered significant.
Histopathological findings
A total of 16/135 patients (11.8%) underwent thyroid surgery after re-treatment. The final histological diagnosis showed benign pathology in 10/16 patients (62.5%), malignant pathology in 3/16 patients (18.75%), while in 3 patients final pathology went missing (18.75%). Malignant pathology included the following: one classic papillary thyroid carcinoma, one follicular subtype of papillary thyroid carcinoma, and one follicular thyroid carcinoma.
Discussion
In this study, we report the effects of TA re-treatment on benign thyroid nodules after an initial unsatisfactory procedure, that is, nodule volume reduction <50% after the first procedure. Indications to TA re-treatment included nodule regrowth (23%), symptom relapse (75%), and persistence of thyrotoxicosis (6.7%). In our study, the earliest time point at which re-treatment was considered was six months after the first procedure, because the greatest volume reduction is usually observed after the first months from the procedure. 11,18 Nevertheless, based on the fact that the proper timing of re-treatment is presently unsettled, 1 and that re-treatment may address issues that arise during the follow-up (i.e., nodule regrowth and AFTN), the median time elapsed between the first treatment and the last visit before re-treatment was 24 months.
Re-treatment led to a median VRR of 50% and 52% after 6 and 12 months from the procedure, and it was more successful than first treatment in terms of nodules' volume reduction. Nevertheless, the effect of TA re-treatment appeared to be somewhat limited. For instance, we have previously reported that TA (either with LA or with RFA) was able to reduce nodules' volume by 63%, 67%, 68%, 69%, and 70% at one, two, three, four, and five years after the first treatment.
Therefore, our data suggest that in nodules with unsatisfactory responses to first treatment, the response to an additional TA might remain somewhat limited as compared with the average volume reduction that has been reported in the literature. Potential factors leading to suboptimal results may be nodule composition, vascularization, and/or the biological characteristics of thyroid benign tumors 19 that include not only thyroid follicular nodular diseases but also RAS-driven follicular adenomas and oncocytic adenomas. 20,21
In addition, re-treatment led to greater VRR than first treatment in small and medium nodules (<30 mL) but not in large nodules (>30 mL). These data are consistent with the established finding that the smaller is the nodule volume, the better is the response to the TA procedure. For instance, Deandrea et al. reported that nodules with a volume <15 mL were reduced by 77% as compared with nodules with a volume >15 mL that were reduced by 67% after RFA. 15
Likewise, also Valcavi et al. observed a trend toward larger effect in the smallest nodules after LA. 22 There are several factors underlying the different response of small and large nodules. The first is related to the amount of energy delivered 10,23 as in large nodules more efforts should be made to reach the required energy threshold to treat them entirely. 15 The second is anatomy. 24 The edges of large (>30 mL) thyroid nodules are usually close to critical surrounding structures, such as the esophagus, trachea, recurrent laryngeal or vagus nerve, and cervical ganglion, and it is cumbersome to perform a safe and complete target ablation. 24
After re-treatment, technique inefficacy (VRR <50% after re-treatment) was observed in 70 patients (51.9%), regrowth was observed in 17 patients (12.6%), and the need of further treatments was observed in 21 patients (15.6%). Cox multiple proportion hazard regression showed that RFA was protective toward technique inefficacy and the need of further treatments. This is consistent with our previous report that RFA was associated with a significantly lower risk of regrowth and re-treatment, 10 as well as with other studies. 25
These results may be ascribed to the amount of energy delivered, which is significantly higher in the RFA compared with LA. The energy delivered is associated with treatment outcomes and its amount should be always specified in the procedure report. 17 RFA and LA have specific modalities of production and distribution of thermal energy. In case of LA, energy delivered should be at least 500–600 J/mL, 9,26,27 while in case of RFA, the amount of energy delivered should be >1000 J/mL. 10,23 In line with these requirements, in our study we found that the average amount of energy delivered was 480 J/mL for LA and 1024 J/mL for RFA re-treatment.
A second technical aspect explaining why RFA was protective toward technique inefficacy and further treatments as compared with LA is the moving shot technique, whereby it is possible to move the tip of the electrode across the entire nodule area, which allows the tailoring of the procedure to the nodule variables features, maximizing the ablation of its marginal areas. 25,28 Consistent with this, previous studies have shown that the extent of tissue ablation, as assessed by the initial ablation ratio, 29 was associated with technique efficacy 29 and reduced likelihood of further treatments. 30 By contrast, LA induces a well-defined area of tissue ablation near the thermal source with rapid energy decay in the surrounding tissue, with the advantage of great precision but the disadvantage of the lack of total tissue ablation, unless multiple fibers are employed. 16,19 Nevertheless, caution should be taken when comparing the various TA techniques, because RFA, LA, and microwave ablation are strongly operator-dependent techniques and their outcomes are influenced not only by local expertise but also by continuous technical evolution. 31
Be it RFA or LA, the larger is the volume of the nodule the higher is the likelihood of the need of repeated treatments over time. 11 For instance, in a previous study we reported that baseline volume cutoffs associated with re-treatment after one procedure were 22.1 mL for RFA and 14.5 mL for LA. 10 In this study, we found that large nodule size (>30 mL) was associated with requiring further treatments.
It has been argued that TA may provide higher financial and quality of life values compared with surgery for appropriately selected patients. 32 For example, TA compares extremely favorably to surgery in terms of costs, as it costs roughly 2.6 times less than surgery, and sick-leave is significantly shorter, provided that patients are treated once. 18 On this basis, also from the cost-efficacy perspective, 18,32 our data suggest to consider that in thyroid nodules with unsatisfactory responses to first treatment (VRR <50%), the response to additional TA might remain somewhat limited, and that baseline volume >30 mL is associated with likelihood of further treatments. Second, RFA is protective toward technique inefficacy and likelihood of further treatments as compared with LA.
Third, based on the few patients who were operated on (16/135), 18.75% of the thyroid nodules that were surgically removed were found to be differentiated thyroid carcinomas. This rate of malignancy in benign nodules unresponsive to TA is consistent with other studies, indicating a malignancy rate of 19.4–20.8% in nodules whose volume did not decrease by 50% after one procedure or regrew during follow-up. 21,33 In particular, a VRR <20% after one year from the first TA should raise suspicion of an underlying malignancy 10 and prompt for repeat fine-needle biopsy/core-needle biopsy 33 or thyroid surgery. 10,33
The main limitations of this study are its retrospective design, the potential selection bias (as all consecutive patients were not screened for the study and the selection of patients was at the discretion of the investigators at each participating site), and the small number of patients with protracted (three-year) follow-up. In addition, being the first study on the outcomes of benign thyroid nodules that have undergone re-treatment with TA, it should be considered as a preliminary study.
Nevertheless, its strengths are (i) its innovative data, (ii) the inclusion of paired analyses (comparing VRR between first-treatment and re-treatment) as patients were treated by the same operators, and (iii) its multicenter design, providing a real-world assessment of TA outcomes (including both LA and RFA). Further studies are needed to determine whether 30 mL is the appropriate volume threshold for favoring surgical management, and to confirm the rate of malignancy in nodules unresponsive to TA.
In conclusion, this is the first study evaluating the effects of TA re-treatment on symptomatic benign thyroid nodules with unsatisfactory response to initial treatment. Re-treatment led to VRR of 50% at 6 months and VRR of 52.2% at 12 months. Best results were seen in small and medium nodules (<30 mL) and after RFA. Further prospective studies are needed to confirm our results.
Authors' Contributions
Conceptualization, data curation, investigation, visualization, and writing—original draft by
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Supplementary Table S2