
Abstract
Background:
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) are highly effective medications for the treatment of type 2 diabetes and obesity. Pharmacological studies in rodents support an association between the use of GLP-1 RAs and the development of medullary thyroid cancer (MTC) resulting in a black box warning for these agents in patients at risk for this condition. Yet, the association between GLP-1 RAs and non-MTC remains controversial. Excessive worry about unproven thyroid cancer risk might lead to underutilizing GLP-1 RAs in patients who could otherwise experience substantial benefits. Unwarranted concerns about thyroid cancer could lead to unnecessary thyroid cancer screening and harms from overdiagnosis.
Summary:
The body of evidence assessing the association between GLP-1 RA use and thyroid cancer spans a wide range of methodologies, including basic and translational research investigating biological plausibility; randomized trials assessing clinical efficacy and providing the strongest evidence for causality; observational studies providing real-life outcome evaluation in larger populations but with limited evaluation of covariates or dependable outcome definitions; and pharmacovigilance studies that provide postmarketing assessments of a safety signal but do not address causality. There is biological plausibility supporting an association between GLP-1 RA and MTC in rodents, which is less clear for non-MTC in humans. Clinical evidence from randomized trials and associated meta-analysis suggest thyroid cancer as a rare event making effect estimates imprecise but without conclusive and consistent evidence of increase risk in those receiving GLP-1 RA. Observational studies at higher risk of bias also show low event rates for thyroid cancer, with effect estimates that are inconsistent among different studies. Pharmacovigilance studies consistently show a signal of increased reporting of thyroid cancer in patients treated with GLP-1 RA.
Conclusions:
Evidence from randomized controlled trials indicates occurrence of thyroid cancer is infrequent in individuals exposed to GLP-1 RA. Observational studies at higher risk of bias yield inconsistent results. Overall there is no conclusive evidence of elevated thyroid cancer risk. These findings can help clinicians when addressing patient's concerns about a potential yet unproven link between GLP-1 RA therapy and thyroid cancer.
Introduction
The prevalence of people living with obesity and type 2 diabetes has increased substantially in the last decades. 1 –4 Approximately 770 million adults live with obesity and 500 million with diabetes worldwide. 3,4 Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have been approved by the U.S. Food and Drug Administration (FDA) since 2005 for the treatment of type 2 diabetes and have demonstrated cardiovascular, metabolic, and weight loss benefits. 5 –8 Two GLP-1 RAs are also approved for the management of obesity (liraglutide and semaglutide), with controlled trials (randomized controlled trials [RCTs]) of semaglutide showing a mean weight loss of 15% total body weight, higher than any other weight loss drug approved to date. 9 –12 Semaglutide has a secondary FDA-approved indication to reduce the risk of major adverse cardiovascular events in adults with type 2 diabetes and established cardiovascular disease. 13 Owing to the increasing trends of obesity and type 2 diabetes, the number of patients with clinical indications for treatment with GLP-1 RA will continue to increase in the upcoming years. 14 –16
Although the safety profile of GLP-1 RAs has generally been acceptable, concerns have arisen regarding a potentially increased risk of thyroid malignancy. 7,8,17 –21 Animal studies support an association between the use of GLP-1 RA and the development of medullary thyroid cancer (MTC), which depends on the dose and treatment duration. 22 –24 As a result, GLP-1 RAs are contraindicated for patients with a personal or family history of MTC or those with multiple endocrine neoplasia syndrome type 2. 8,17,22 In a recent case–control study, an increased risk of both MTC and non-MTC was reported in patients who were exposed to GLP-1 RA. 25 Concerns regarding the validity of outcomes have emerged, particularly owing to the reliance on indirect indicators such as the calcitonin test, carcinoembryonic antigen measurement, or vandetanib treatment to distinguish between MTC and non-MTC. This approach introduces the potential for misclassification. 21,25
A recent communication from the European Medicines Agency's Pharmacovigilance Risk Assessment Committee indicated that the current evidence does not support a causal link between GLP-1 RA and thyroid cancer, nor does it warrant alterations to the product information. Instead, they emphasize the importance of vigilant monitoring for the occurrence of these rare events and the ongoing evaluation of emerging evidence. 21 Concerns about thyroid malignancy may deter patients from being treated with GLP-1 RAs, yet this association is unproven when compared with known anticipated benefits secondary to weight loss, glycemic control, and reductions in cardiovascular and kidney disease risk. 7 Herein, we summarize the current evidence of GLP-1 RAs and thyroid cancer and discuss the potential implications for clinical practice and guide future research.
Search Strategy and Article Selection
References for this narrative review were identified through searches in PubMed and Scopus for articles published between January 1, 2000 and April 2023, using the following search strategy: “Neoplasms”[Mesh] OR (thyroid* AND (cancer* or carcino* OR neoplas* OR tumor* OR tumour*)) AND (albiglutide or beinaglutide or cotadutide or danuglipron or dulaglutide or ecnoglutide or efocipegtrutide or efpeglenatide or elsiglutide or exendin or liraglutide or lixisenatide or mazdutide or pegapamodutide or pegloxenatide or pemvidutide or semaglutide or taspoglutide or tirzepatide or utreglutide or vurolenatide or “glucagon-like-peptide” or GLP1* or GLP-1* OR “Glucagon-Like Peptide-1 Receptor”[Mesh]). Relevant articles resulting from these searches, references cited in these articles and provided by experts were reviewed.
Our goal was to summarize clinical evidence (although not exhaustively) obtained through various research methodologies that offer complementary insights when assessing both causal and noncausal associations between GLP-1 RA use and thyroid cancer. We aimed to examine the strengths and limitations of these methodologies to offer recommendations for clinical care, provide context for shared decision-making, and guide future research.
We classified the available evidence into four categories: (1) basic and translational research, (2) observational clinical studies, (3) RCTs and associated meta-analysis, and (4) pharmacovigilance studies. Meta-analysis of RCT was used to assess the quality of the evidence following the criteria included in the GRADE approach (risk of bias, inconsistency, imprecision, indirectness, and publication bias). 26 For observational studies we assessed the risk of bias following the Newcastle-Ottawa Scale that evaluates selection of participants, comparability of groups, and outcome assessment 27 (Fig. 1).
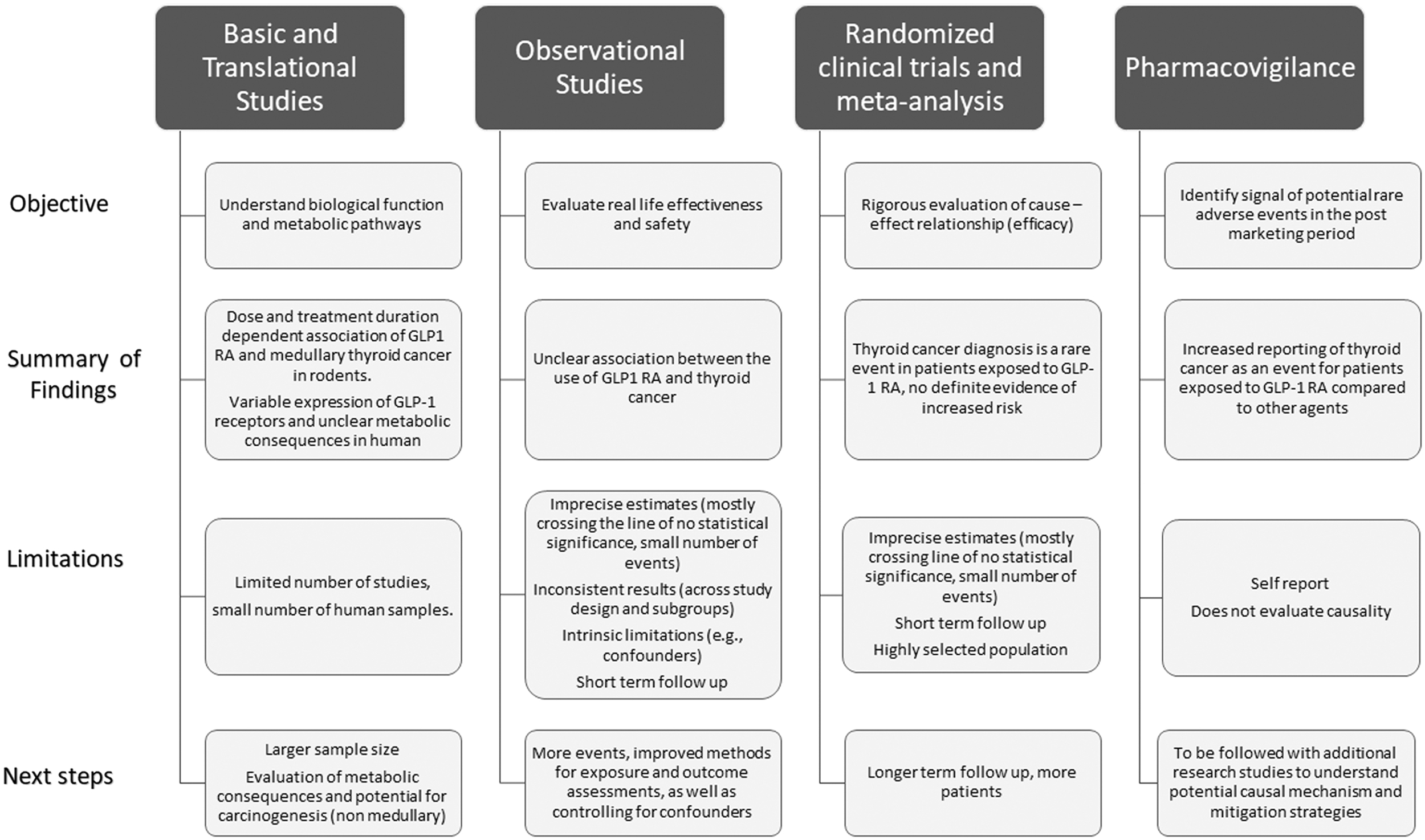
Glucagon-like peptide-1 receptor agonist and thyroid cancer across different research methodologies.
GLP-1 RAs: Clinical Primer
GLP-1 is a regulatory hormone derived from the proglucagon gene and secreted in response to food consumption. 6,28,29 The GLP-1 has a regulatory effect in multiple organs, including the liver, brain, pancreas, gastrointestinal tract, kidney, and muscle. 6,28,29 GLP-1 produces its direct biological effects through interaction with its receptor, a G protein–coupled receptor that increases cAMP levels. 6,28 Clinically, GLP-1 RAs are indicated for the treatment of type 2 diabetes (all) and obesity (liraglutide and semaglutide only) and have beneficial effects on patient-important outcomes such as weight loss, cardiovascular and kidney events, hepatic steatosis, and mortality. 5,7 –9,11,30
The most common adverse effects of GLP-1 RA are gastrointestinal, including nausea, vomiting, and diarrhea, affecting ∼15–30% of participants in RCT. 8,31 The potential role of GLP-1 RA as a risk factor for pancreatitis and biliary disease is still under investigation. 8,19,29,32 The potential trophic and carcinogenic effects of GLP-1 RA have been investigated across a series of primary sites, including thyroid and pancreatic cancer, with inconsistent results. 29,33,34
Complexities When Investigating the Causal Association Between GLP-1 RA Therapy and Thyroid Cancer
The investigation of the causal association between GLP-1 RA therapy and neoplasm is complex as it requires consideration of multiple factors such as biological interactions (e.g., the potential effects of type 2 diabetes and obesity, weight loss, and glucose reduction on cancer risk), direct biological effects (e.g., potential trophic effects and other direct effects of GLP-1 RA, personal susceptibility to thyroid cancer), and factors associated with the conduct of clinical studies (e.g., selection bias, detection bias, length of follow-up). 20,33 –36 Therefore, assessing a potential causal link between GLP-1 RA treatment and cancer necessitates a comprehensive examination of covariates that directly or indirectly influence pathways related to oncogenesis, as well as downstream effects of GLP-1 RA that can directly lead to oncogenesis. 37
Similarly, consideration of the clinical pathways leading to cancer diagnosis and subtypes of thyroid cancer is essential to inform clinical practice. For example, it is important to consider the difference between increased detection of thyroid cancer after exposure to GLP-1 RA versus de novo carcinogenesis and development of thyroid cancer in patients undergoing GLP-1 RA treatment. In fact, some studies exclude thyroid cases that are diagnosed too soon after drug exposure (e.g., <1 year). This consideration of a latency period can provide insight when distinguishing between a new diagnosis of preexisting thyroid cancer versus thyroid cancer carcinogenesis. 33,38 In addition, the distinction between MTC and non-MTC is important.
The incidence of non-MTC has tripled in the last three decades (from 5 to 15 per 100,000 persons), driven mainly by overdiagnosis and increased detection of low-risk thyroid cancer that will otherwise lead to no patient harm if it remained undiagnosed. 39,40 In other words, thyroid cancer diagnosis is an outcome that is prone to over-detection owing to medical surveillance, an important covariate to be assessed in clinical studies. 40,41
General Strengths and Limitations of Research Methodologies
The body of evidence assessing the potential association between GLP-1 RA use and thyroid cancer spans a wide range of methodologies that evaluate both causal and noncausal associations. As described in Figure 1, these methodologies have distinct goals, strengths, and limitations. 42,43 Considering the intricacies involved in understanding the potential clinical implications of GLP-1 RA therapy and thyroid cancer, they collectively offer complementary evidence that can inform practice and identify research gaps.
Basic and translational studies provide mechanistic and biological plausibility for the potential causal association between GLP-1 RA therapy and thyroid cancer. The meta-analysis of RCTs provides the strongest evidence for a causal association; however, given the rarity of the event and short duration of these studies the results are imprecise. Observational studies provide in general lower quality evidence of association, but complement findings of RCTs if their design allows for reliable classification of exposure and outcomes, and include large populations followed for clinically relevant periods of time. Yet, the observational studies discussed in this review suffer from shortcoming related to outcome definition (e.g., methods for assessing thyroid cancer and differentiating between MTC and non-MTC), lack of consideration of covariates of interest and similar to RCTs, limited number of events and follow-up time (Tables 1 and 2). Finally, pharmacovigilance studies are not meant to evaluate causality but are specifically conducted to identify potential safety signals postmarketing (Table 3).
Summary of Observational Studies (Cohort and Case–Control) Evaluating the Association Between Glucagon-Like Peptide-1 Receptor Agonists Therapy and Thyroid Cancer
CEA, carcinoembryonic antigen; CI, 95% confidence interval; DPP4i, dipeptidyl peptidase 4-inhibitors; GLP-1 RA, glucagon-like peptide-1 agonists; HR, hazard ratio; ICD-10, International Classification of Diseases, Tenth Revision; MTC, medullary thyroid cancer; RR, relative risk; SGLT2, sodium-glucose cotransporter-2 inhibitors.
Summary of Meta-Analysis of Randomized Controlled Trials Evaluating the Association Between Glucagon-Like Peptide-1 Receptor Agonist Therapy and Thyroid Cancer
Primary study also evaluated observational studies, not included in presented thyroid cancer analysis. Total number of patients on GLP-1 RA not reported.
Primary study also evaluated observational studies, not included in presented thyroid cancer analysis.
NR, not reported; OR, odds ratio; RCTs, randomized controlled trials.
Summary of Pharmacovigilance Studies Evaluating the Association Between Glucagon-Like Peptide-1 Receptor Agonist Therapy and Thyroid Cancer
FDA, Food and Drug Administration.
Basic and Translational Research
GLP-1 RAs have been observed to induce C cell proliferation, hyperplasia, and MTC in studies of rodents. 23,44,45 The association between GLP-1 RAs and MTC in humans has not been proven, and studies have shown interspecies differences regarding the density of GLP-1 receptors and responses to GLP-1 RA activation in the thyroid, limiting the predictive value of nonhuman preclinical studies on humans. 23,24,46 For example, studies including a small number of human samples (from patients) have confirmed expression of the GLP-1 receptor in human MTC samples, but also the expression of GLP-1 receptors in 18% of papillary thyroid cancer (PTC; 3/17) and 33% of control samples (5/15). 46 Similarly, GLP-1 receptor expression by immunostaining was found in 32% of PTC cases (18/56), all MTCs (4/4), and 29% of nodular hyperplasia cases (2/7), while negative expression was found in all normal thyroid follicular cells (56/56).
In addition, there was no association between demographic or clinical characteristics and GLP-1 receptor expression (age, sex, tumor size, lymph node metastasis, or extrathyroidal extension), except for an inverse correlation between tumor multifocality and GLP-1 receptor expression. 47 Furthermore, He et al. evaluated the effect of GLP-1 RA on cell proliferation and metabolism of thyroid cancer cells. 48 They evaluated 107 human thyroid tissues (52 PTC/55 normal) and found higher staining for the GLP-1 receptor in 49% of PTC tissues and none of the normal thyroid samples. In an analysis of primary cultured normal thyrocytes and PTC cell lines, PTC cell lines contained more GLP-1 receptors than primary cultured normal thyrocytes by Western blot. Yet, GLP-1 RA (liraglutide and exenatide) did not significantly affect these cell lines' proliferation, signaling pathways, mitochondrial respiration, or glycolysis. 48
Summary and limitations
Overall, based on preclinical nonhuman studies, there appears to be a strong association between GLP-1 RA and MTC in rodents. Small reports, including human samples, have shown variable expression of GLP-1 receptors in non-MTC cells. Yet, there is limited evaluation of the potential long-term effects of GLP-1 receptor activation as a carcinogenic factor. 22,23,48 Given the limitations of the current body of evidence and the emerging reports on the impact of GLP-1 RA on the risk of thyroid, prostate, and other cancers, there is a heightened interest in supporting research to enhance our understanding of the mechanisms that influence cancer risk associated with the use of these agents. 37
Observational Studies
General findings
Observational studies using data generated as part of clinical practice can provide real-world evidence of effectiveness and safety. Yet, they are prone to confounding and biases that hinder causal inference, in this case, supporting a causal association between GLP-1 RA use and development or diagnosis of thyroid cancer. 49,50 Table 1 provides a summary of six observational studies, comprising four cohort studies and two case–control studies that assess the association between GLP-1 RA and thyroid cancer. Among these, four studies utilized U.S.-based databases. These studies were categorized as having a moderate to high risk of bias owing to limited evaluation of covariates, reliability of thyroid cancer assessment, and restricted follow-up times (Supplementary Tables S1 and S2). All cohort studies incorporated propensity score matching in their methodologies.
Of note, there was considerable variability among the studies concerning exposure (e.g., evaluated a single GLP-1 RA vs. multiple GLP-1 RA), comparison groups (used specific agents as controls such as sodium-glucose cotransporter-2 [SGLT2] inhibitors vs. combined groups of antidiabetic agents or performed multiple comparisons), and timing of outcome evaluation (e.g., inclusion of thyroid cancer events during the first 12 months after therapy and length of follow-up). Two studies reported statistically significant findings of increased risk for thyroid cancer in those exposed to GLP-1 RA. 25,38 In addition, five studies included analyses considering different lag times for outcome assessment, while two studies provided distinct information differentiating between thyroid cancer in general and MTC. 25,38,51 –53
Specific studies
Dore et al. conducted a propensity score–matched study using administrative claims to evaluate the incidence of thyroid cancer among 32,894 initiators of exenatide between 2005 and 2009 in the Normative Health information database. 52 The overall follow-up time was <1 year and among the cohort of exenatide initiators, there were 37 thyroid malignancies, while in the metformin/glyburide initiators cohort, there were 26, resulting in a relative risk (RR) of 1.4 [95% confidence interval (CI) 0.8–2.4]; when only inpatient thyroid cancer claims were included the RR was 0.9 [CI 0.3–2.6]. 52
Liang et al. used two U.S. claims datasets (the Optum Research Database and the Impact National Benchmark Database) to conduct both a cohort and a nested case–control study comparing the incidence of thyroid cancer among patients with type 2 diabetes starting exenatide or other agents between 2005 and 2015. 53 The cohort study included 33,629 patients who started exenatide and 49,319 propensity score–matched initiators of other agents with a median follow-up time of 0.9 years, and identified 57 cases of thyroid cancer in the exenatide group and 43 cases in the comparator group. The hazard ratio (HR) for thyroid cancer was 1.46 [CI 0.98–2.19]. In the nested case–control study exenatide use was not associated with an increased for thyroid cancer (adjusted odds ratio [OR] = 0.89 [CI 0.64–1.24]). 53 For outcome assessment, authors developed and validated algorithms based on diagnosis and procedures codes, with a positive predictive value of 88% for thyroid cancer without distinction between non-MTC and MTC. 53
A nested case–control study used a large French national insurance database evaluated the risk for thyroid cancer in patients with type 2 diabetes treated with GLP-1 RA between 2006 and 2018. 25 Thyroid cancer was identified using diagnosis and procedure codes and 20 control cases were selected for each case matched by age, sex, and duration of diabetes. 25 They identified 3,746,672 patients with type 2 diabetes, of which 2562 patients met inclusion criteria as cases (new thyroid cancer) and were matched with 45,184 controls. GLP-1 RA use for 1–3 years was associated with increased risk for any thyroid cancer (adjusted HR = 1.58 [CI 1.27–1.95]) and MTC (adjusted HR = 1.78 [CI 1.04–3.05]). 25 Of all thyroid cancer cases identified, 15% were MTC, which is higher than expected and might be related to methods used for defining MTC (e.g., testing for calcitonin test/carcinoembryonic antigen or vandetanib treatment). 25
Funch et al. conducted a propensity score–matched study comparing the risk for thyroid cancer between new users of liraglutide and other diabetes medications (exenatide, metformin, pioglitazone, sulfonylureas, and dipeptidyl peptidase-4 inhibitors) using the Optum Research Database between 2010 and 2014. 38 The median follow-up time was 17 months and the RR for thyroid cancer for liraglutide was 1.66 [CI 1.00–2.75] against all comparators, 1.70 [1.03–2.81] against all comparators except exenatide and 1.66 [0.73–3.79] when compared with exenatide under the intention-to-treat analysis. Additional analysis including intention to treat with latency (exclusion of cases in the first year), time on drug, and cumulative exposure to the drug, failed to reach a statistically significant difference. 38
This study also included in their definition of thyroid cancer the need for a thyroid surgery procedure (positive predictive value of 0.91). 38 In addition, a subgroup of 72 confirmed thyroid cancer through record review served as the basis for additional analysis. Most represented PTC (85%) and no cases of MTC were reported. Micropapillary thyroid cancer represented 46% of the cases, with a proportion of 67% of the cases of liraglutide initiators (6/9), 50% of cases of exenatide initiators (1/2), and 43% of all comparators (27/63). Similarly, claims for thyroid-related tests, imaging, diagnostic procedures, or presence of goiters/nodules was similar between the liraglutide initiators and all other comparators groups (49.8% vs. 48.5%). 38
More recently, Bea et al. evaluated the risk for thyroid cancer associated with the use of GLP-1 RA (albiglutide, dulaglutide, exenatide, and lixisenatide) compared with SGLT2 inhibitors, in a population-based cohort study using claims data (Korean National Health Insurance Database) from 2014 to 2020. 51 Patients were followed from 1 year from cohort entry, for a median of 2.1 person-years of follow-up. In the new user of GLP-1 RA cohort 23 developed thyroid cancer (21,722) compared with 524 in the new user of SGLT2 inhibitor cohort (326,993), resulting in a weighted HR of 0.98 [CI 0.62–1.53]. The absolute rate difference between cohorts was −0.08 [95% CI −0.32 to 0.16]. 51 In the subgroup analysis, no statistically significant effect modifications were observed (age, sex, insulin use, autoimmune thyroiditis, treatment duration, body mass index), although the thyroid cancer risk increased in those with past insulin use. 51
Summary and limitations
These observational studies are at moderate to high risk of bias and have several limitations that hinder causal inference, including lack of randomization and reliance on medical claims and medical record documentation for the evaluation of exposure (e.g.,. GLP-1 RA use) and outcomes (e.g., thyroid cancer and subtypes). 50 Of note, there was a large variation in the percentage of cases reported as MTC between the two studies that included this distinction. 25,38 Similarly, the potential for residual confounding (e.g., limited evaluation of specific risk factors for thyroid cancer such as obesity, neck radiation, and family history of thyroid cancer) and the role of surveillance bias (e.g., clinicians might be more likely to do a thyroid exam or ultrasound on patients taking GLP-1 RA) are important considerations that have been not thoroughly assessed. 25,52 –54
Of note, the strength of the association of GLP-1 RA as a risk factor for the diagnosis of thyroid cancer is inconsistent in this body of evidence, as it varies according to study designs (e.g., case–control vs. cohort) and sensitivity and subgroup analyses (e.g., types of codes used for cancer diagnosis assessment, timing of cancer diagnosis) further decreasing our certainty in these results.
RCT
General description
RCT that evaluated the efficacy of GLP-1 RAs in individuals with diabetes or obesity have not shown a significantly increased risk of thyroid cancer. 33,55,56 Table 2 summarizes 5 meta-analyses of RCTs evaluating the association between GLP-1 RA and thyroid cancer. Overall, studies have low risk of bias and/or considered to have moderate–high quality, results are consistent, provide direct evidence and have limited evidence for publication bias. However, the main limitation of this body of evidence relates to imprecision owing to the small number of events and limited follow-up times.
Specific studies
Nauck et al. evaluated neoplasms as a prespecified exploratory outcome in participants of the LEADER Trial (randomized, double-blind study, including patients >50 years with type 2 diabetes and high cardiovascular risk assigned to receive liraglutide vs. placebo). 33 Overall, 10.1% of patients in the liraglutide group versus 9.0% in the placebo group had a neoplasm diagnosis (HR = 1.12 [CI 0.99–1.28]). Among ∼4660 patients randomized to each group and followed for a median of 3.8 years, 5 patients in the liraglutide group and 3 patients in the placebo group received a thyroid cancer diagnosis (HR = 1.66 [CI 0.4–6.95]). 33
Additional studies focused on evaluating calcitonin levels and diagnosing MTC in the LEADER study and EXSCEL study (randomized study, adults with type 2 diabetes, exenatide vs. placebo). 55,57 In the LEADER trial, at 36 months, there was no difference in the levels of calcitonin between participants in the placebo or liraglutide arm and no diagnoses of C-cell hyperplasia or MTC in those who received liraglutide and there was one event of MTC in the placebo arm. 57 Bethel et al. reported consistent findings of no increase in levels of calcitonin between patients in the placebo or exenatide arm of the EXSCEL trial. In their analysis, three patients were diagnosed with MTC as they were found to have elevated calcitonin at baseline as part of study procedures. They identified 70 patients who had elevated calcitonin levels during the study, of which ∼53% underwent additional diagnostic testing without any additional thyroid cancer diagnoses. These findings highlight the potential burden of diagnostic cascades, in this case stemming from routine monitoring of calcitonin levels in patients on GLP-1 RA. 55
At least 5 meta-analyses have summarized the risk of thyroid cancer diagnoses from randomized trials. 34,35,56,58,59 Alves et al. evaluated 25 RCTs and observational studies of GLP-1 RA in patients with type 2 diabetes up to 2012. Five RCTs evaluating liraglutide reported cases of thyroid cancer (9 liraglutide vs. 1 control group) resulting in an OR of 1.54 [CI 0.40–6.02]. 35 Cao et al. included 37 studies up to 2019, of which 22 reported no thyroid cancer events in the GLP-1 RA or control group. In 15 trials, at least one case of thyroid cancer was reported (34/22,276 active group vs. 17/20,525 control group), resulting in an OR = 1.49 [CI 0.83–2.66]. 34 Hu et al. included 35 studies, including patients with diabetes type 1 and 2, prediabetes, overweight, or obesity. 56 The RR for the diagnosis of thyroid cancer was 1.3 [CI 0.86–1.97] when including 32 studies (63/43,124 events in the GLP-1 RA group vs. 29/34,369 control). 56
A recent meta-analysis focused specifically on semaglutide and patients with diabetes, obesity, or hepatic steatosis from 11 RCTs that compared semaglutide with a passive control and 16 RCTs that compared semaglutide with an active control. When compared with placebo, the semaglutide OR for thyroid cancer was 2.04 [CI 0.33–12.61] with 4 cases/6046 participants in the semaglutide group and 0/5777 in the placebo group. Similarly, when comparing semaglutide to an active control group (diabetes medications), the OR for thyroid cancer was 1.19 [CI 0.15–9.66] with 2 cases/7556 in the semaglutide group and 1 case/5614 in the active control group. 58
Silverii et al. evaluated 64 trials of which 26 reported cases of thyroid cancer. Overall, they found an increased RR for thyroid cancer on the fixed-effect meta-analysis OR = 1.52 [CI 1.01–2.29], but the statistical significance was lost in the random effect analysis (OR = 1.41 [CI 0.91–2.17]), and in the leave one out sensitivity analysis of 5 studies. 59 Authors also evaluated a series of subgroups without detecting any significant difference in effects. Finally, their analysis focusing on specific diagnosis of PTC or MTC did not reach statistical significance. Using these findings, they estimated a 5-year number needed to harm, between 1349 and 1562 (Table 2). 59
Summary and limitations
RCT and meta-analysis of RCT trials in which thyroid cancer was not a primary outcome have infrequently reported thyroid cancer cases in participants treated with GLP-1 RA. Results from these meta-analysis suggest thyroid cancer as a rare event making effect estimates imprecise but without conclusive evidence of increase risk in those receiving GLP-1 RA.
Pharmacovigilance Studies
General description
Postmarketing surveillance is an important process by which medications that have completed clinical trials are monitored for signals of adverse events. 60 This methodology is of particular interest for rare adverse events that might be challenging to identify in RCT that usually have short follow-up periods and include highly selected populations. 60,61 Most of the available programs of pharmacovigilance are based on self-report of adverse events experienced by individuals reportedly taking the drug of interest and are designed to serve as hypothesis generating studies that trigger further evaluation to determine association or causality. 60,61 We summarize 4 pharmacovigilance studies assessing reporting of thyroid cancer in patients on GLP-1 RA (Table 3). Two studies used U.S.-based database, and the others the European or World Health database. 25,61 –63 These studies provide statistical assessment of the proportionality of reporting of thyroid cancer in GLP-1 RA users compared with users of other medications, as a way to identify potential safety signal that warrant further investigations.
Specific studies
Elashoff et al. evaluated the U.S. FDA database of reported adverse events for patients on GLP-1 RA (exenatide) from 2004 to 2009. In their analysis, they found an OR = 4.73 for a report of a thyroid cancer event for exenatide compared with comparators (rosiglitazone, nateglinide, repaglinide, and glipizide) (p = 0.004). 62 Wu et al. evaluated the U.S. FDA Adverse Event Reporting System from 2005 to 2021. They focused their analysis only on records that listed GLP-1 RA as monotherapy and reported important medical events, and included 16,350 reports. When classified by system organ classes, there was increased reporting of neoplasms (benign/malignant), including increased reporting of MTC and PTCs. 63
A similar analysis of the European Pharmacovigilance Database up to 2020 found 11,243 cases of thyroid cancer reported out of 6,664,794 reports, among which GLP-1 RA were listed in 236 (liraglutide 113, exenatide 76, dulaglutide 35, albiglutide 3, semaglutide 9). Most of the cases were reported in women aged 18–64 years and almost equally reported by health professionals and others. 61 The investigators calculated the proportional report ratio for GLP-1 RA and thyroid cancer and found the thresholds for reporting a new safety signal were fulfilled for exenatide, liraglutide, and dulaglutide as thyroid cancer was reported relatively more frequently with these drugs compared with all other drugs in the database. 61 Bezin et al. complemented the findings of their case–control study by evaluating the VigiBase a database that includes >23 million case safety reports from 150 countries from 2005 to 2021. 25 Consistent with previous studies, they also found a signal of disproportionate reporting of GLP-1 RA and overall thyroid cancer and MTC, including 606 reports (mostly from exenatide and liraglutide). 25
Summary and limitations
Findings from pharmacovigilance studies consistently show a signal of increased reporting of thyroid cancer in patients treated with GLP-1 RA. However, these databases reflect nonsubstantiated events reported by individuals and attributed—by those individuals—to a particular drug. 61 –63 They do not establish a causal or even an association relationship between a drug and the event, serving instead for hypothesis generation and prompt for future investigation of disproportional increased reporting of events.
Clinical and Research Implications
Basic science data support the association between GLP-1 RA and MTC in rodents and the expression of GLP-1 receptors in non-MTC cells in humans; yet the consequences of the expression of these receptors and comparisons with nonthyroid cancer cells in humans require further evaluation. RCT supports the rare occurrence of thyroid cancer diagnosis during relatively short follow-up periods, and without conclusive evidence of increased risk of thyroid cancer in GLP-1 RA users. Findings from observational data are at higher risk of bias and have less trustworthy results that are inconsistent across different study designs and subgroup analyses. Finally, while postmarketing studies support disproportional reporting of thyroid cancer among patients undergoing treatment with GLP-1 RA, pharmacovigilance data cannot establish causality.
The implications from this body of evidence are important as patients and clinicians consider the risk and benefits of GLP-1 RA. The benefits of GLP-1 RAs in patients with obesity and type 2 diabetes are large, and clinically significant, including weight loss, reduction in major cardiovascular events, improved kidney outcomes, decreased cardiovascular and all-cause mortality, improvement of glucose control and reduction of hepatic steatosis. These benefits need to be weighed against the unproven risk of harm from non-MTC. The benefits of therapy are likely to exceed the risk for most patients. Yet, patients and clinicians should consider this evidence when discussing potential risks and patients' values and preferences that might affect the risk/benefit balance. In particular, these conversations could help personalized treatment and help clinicians address patient fears related to thyroid cancer in general and the black box warning for MTC.
Based on the currently available evidence, GLP-1 RAs should not be used in patients with a family history of MTC or MEN2A, MEN2B. 8 However, there is no evidence supporting screening for thyroid nodules before initiating or during treatment with GLP-1 RA, nor for the inclusion of GLP-1 RA as a risk factor for thyroid cancer. Doing so is likely to lead to overdiagnosis of differentiated thyroid cancer, which has known harms to patients and the health care system without incurred benefit. 64,65 Therefore, thyroid nodules should be evaluated according to already published evidence-based recommendations until additional clinical evidence becomes available. 66
Studies evaluating effects of GLP-1 RA on normal and cancer human thyroid cells, and phase IV clinical trials, with large number of participants, standardized reporting of thyroid cancer as an outcome, including subtypes of cancer and longer follow-ups should help elucidate if there is a causal association between GLP-1 RAs and thyroid cancer. Similarly, large observational studies with robust methods for outcomes assessment (thyroid cancer and subtypes), analysis of confounders and comparisons between different agents in the GLP-1 RA class could help identify differences in associated risks for thyroid cancer.
Conclusion
There is biological plausibility supporting an association between GLP-1 RA and MTC in rodents, which is less clear for non-MTC in humans. Clinical evidence from randomized trials and associated meta-analysis suggest thyroid cancer as a rare event making effect estimates imprecise but without conclusive evidence of increase risk in those receiving GLP-1 RA when compared with control groups. Observational studies that are at higher risk of bias owing to lack of granularity for exposure and outcome assessment, also show low event rates for thyroid cancer, with effect estimates that are inconsistent among different studies. Pharmacovigilance studies consistently show a signal of increased reporting of thyroid cancer in patients treated with GLP-1 RA.
A comprehensive understanding of the different types of methodologies used to address the association between GLP-1 RA and thyroid cancer, their strengths, limitations, and results can assist clinicians when addressing concerns about the unproven risk for thyroid cancer when evaluating the potential benefits and harms of GLP-1 RA therapy.
Footnotes
Authors' Contributions
All authors contributed to conceptualize this narrative review. N.S.O. wrote the first draft. All authors edited and revised the article and approved of the final version.
Disclaimer
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Disclosure Statement
None of the authors have any conflict of interest related to the article.
Funding Information
In 2017, 2018 and 2019 A.E.E.D.Y. received compensation from Novo Nordisk, Servier, and Sanofi for consultancy or speakerships on topics not directly related to the research described in the article. Payment was limited to small, circumscribed engagements, and has not continued. The topics of the current research were not discussed.
N.S.O. was supported by the National Cancer Institute of the National Institutes of Health under Award No. K08CA248972.
In the last 36 months, R.G.M. has received support from the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institute of Health (NIH), National Institute on Aging of the NIH, and the National Center for Advancing Translational Sciences. She also serves as a consultant to Emmi® (Wolters Kluwer) on developing patient education materials related to diabetes.
Supplementary Material
Supplementary Table S1
Supplementary Table S2