
Abstract
Background:
Genomic profiling is now available for risk stratification of cytologically indeterminate thyroid nodules (ITNs). Mutations in RAS genes (HRAS, NRAS, KRAS) are found in both benign and malignant thyroid nodules, although isolated RAS mutations are rarely associated with aggressive tumors. Because the long-term behavior of RAS-mutant ITNs is not well understood, most undergo immediate surgery. In this multicenter retrospective cohort study, we characterize tumor growth kinetics of RAS-mutant ITNs followed with active surveillance (AS) using serial ultrasound (US) scans and examine the histopathologic diagnoses of those surgically resected.
Methods:
US and histopathologic data were analyzed retrospectively from two cohorts: (1) RAS-mutant ITNs managed with AS at three institutions (2010–2023) and (2) RAS-mutant ITNs managed with immediate surgery at two institutions (2016–2020). AS cohort subjects had ≥3 months of follow-up and two or more US scans. Cumulative incidence of nodule growth was determined by the Kaplan–Meier method and growth by ≥72% change in tumor volume. Pathological diagnoses for the immediate surgery cohort were analyzed separately.
Results:
Sixty-two patients with 63 RAS-mutated ITNs under AS had a median diameter of 1.7 cm (interquartile range [IQR] 1.2–2.6) at time of diagnosis. During a median AS period of 23 months (IQR 9.5–53.5 months), growth was observed in 12 of 63 nodules (19.0%), with a cumulative incidence of 1.9% (1 year), 23.0% (3 years), and 28.0% (5 years). Most nodules (81.0%) demonstrated stability. Surgery was ultimately performed in 6 nodules, of which 1 (16.7%) was malignant. In the cohort of 209 RAS-mutant ITNs triaged to immediate surgery, 33% were malignant (23.9% American Thyroid Association [ATA] low-risk cancers, 7.2% ATA intermediate-risk, and 1.9% ATA high-risk. During a median follow-up of 6.9 (IQR 4.4–7.1) years, there were no disease-specific deaths in these patients.
Conclusions:
We describe the behavior of RAS-mutant ITNs under AS and find that most demonstrate stability over time. Of the resected RAS-mutant nodules, most were benign; of the cancers, most were ATA low-risk. Immediate surgical resection of all RAS-mutant ITNs appears to be a low-value practice. Further research is needed to help define cases most appropriate for AS or immediate surgery.
Introduction
In recent years, the genetic alterations and molecular mechanisms underlying thyroid cancer development and progression have been more comprehensively defined. In parallel, genomic profiling of thyroid nodules has been introduced into clinical care, potentially helping clinicians risk stratify cytologically indeterminate thyroid nodules (ITNs) that cannot otherwise be categorized as benign or malignant without surgical resection. The most common genetic alterations identified in ITNs are mutations in RAS family genes—HRAS, NRAS, and KRAS. RAS mutations are observed in thyroid cancers and benign nodules: 30–45% of follicular thyroid cancer (FTC), 30–45% of follicular variant of papillary thyroid cancer (FVPTC), 20–40% of poorly differentiated thyroid cancer (PDTC), 10–20% of anaplastic thyroid cancer, 13% of classical papillary thyroid cancer (cPTC), and 25% of benign follicular adenomas (FA). 1 –5 Because benign nodules are much more common than cancers, most RAS-mutant thyroid nodules are benign. As such, the clinical significance of identifying a RAS mutation in an ITN remains poorly defined.
Current clinical practice guidelines of the National Comprehensive Cancer Network (NCCN) advise either surgery or observation as approaches for ITNs with molecular diagnostic testing “suggestive of malignancy.” 6 The American Thyroid Association (ATA, 2015) and the American Association of Clinical Endocrinology (AACE, 2016) guidelines do not provide specific recommendations for this scenario, acknowledging the uncertainty associated with molecular and genetic findings identified in ITNs. 7,8
For small, low-risk papillary thyroid carcinomas (PTCs), both ATA and NCCN guidelines offer active surveillance (AS) as a possible alternative to immediate surgery. This reflects growing evidence of the long-term stability of low-risk PTC, and the safety of delayed intervention, if needed. 9 –11 Emerging evidence demonstrates that ITNs may also be feasibly managed with AS. 12,13 Together, these guidelines and evidence base raise the question of whether observation would be a reasonable option for RAS-mutant ITNs.
Because of an evidence gap, most RAS-mutant ITNs are triaged to immediate surgical management, although most prove to be nonmalignant, and very few are high-risk cancers. A practice of immediate surgery for all RAS-mutant ITNs exposes many patients to the risks, potential morbidity, and financial toxicity of unnecessary surgery. 14 Therefore, defining management options for RAS-mutant ITNs is an unmet clinical need. Lack of consensus surrounding the management of these nodules stems from the absence of studies of their long-term clinical behavior.
In this study, we (1) characterize growth kinetics of RAS-mutant ITNs in patients offered AS as an alternative to immediate surgery and (2) examine histopathology of a separate contemporary cohort of RAS-mutant ITNs undergoing immediate surgical resection.
Methods
In this multicenter retrospective cohort study, we examined 63 RAS-mutant ITNs in 62 patients followed with AS (2010–2023) at Memorial Sloan Kettering Cancer Center (MSKCC; n = 56), New York University Langone Medical Center (NYU; n = 3), and Mount Sinai Health System (n = 4; all in New York, NY). This study was approved by the institutional review boards of each institution.
The decision to follow patients with AS, as opposed to proceeding directly to thyroid surgery, the frequency of serial ultrasound (US) and follow-up visits, and thresholds for surgery, was determined via shared decision-making and clinical judgment of treating physicians. Across all sites, AS was offered as an alternative to immediate surgery for ITNs with isolated RAS mutations, ≤4 cm in diameter, without suspicious sonographic characteristics (microcalcifications, irregular margins, extrathyroidal extension, or suspicious lymph nodes; Fig. 1). 15 Several patients were followed with AS despite not meeting all criteria: one patient with an ITN >4 cm in size (5.9 cm) and five patients with ITNs harboring co-mutations in other genes declined recommendations for surgery and were included in the AS cohort. Several patients had small (<2 cm) intrathyroidal nodules with either microcalcifications (n = 4) or irregular margins (n = 3) but without extrathyroidal extension or suspicious lymph nodes, strongly favored AS, and were included in the AS cohort.
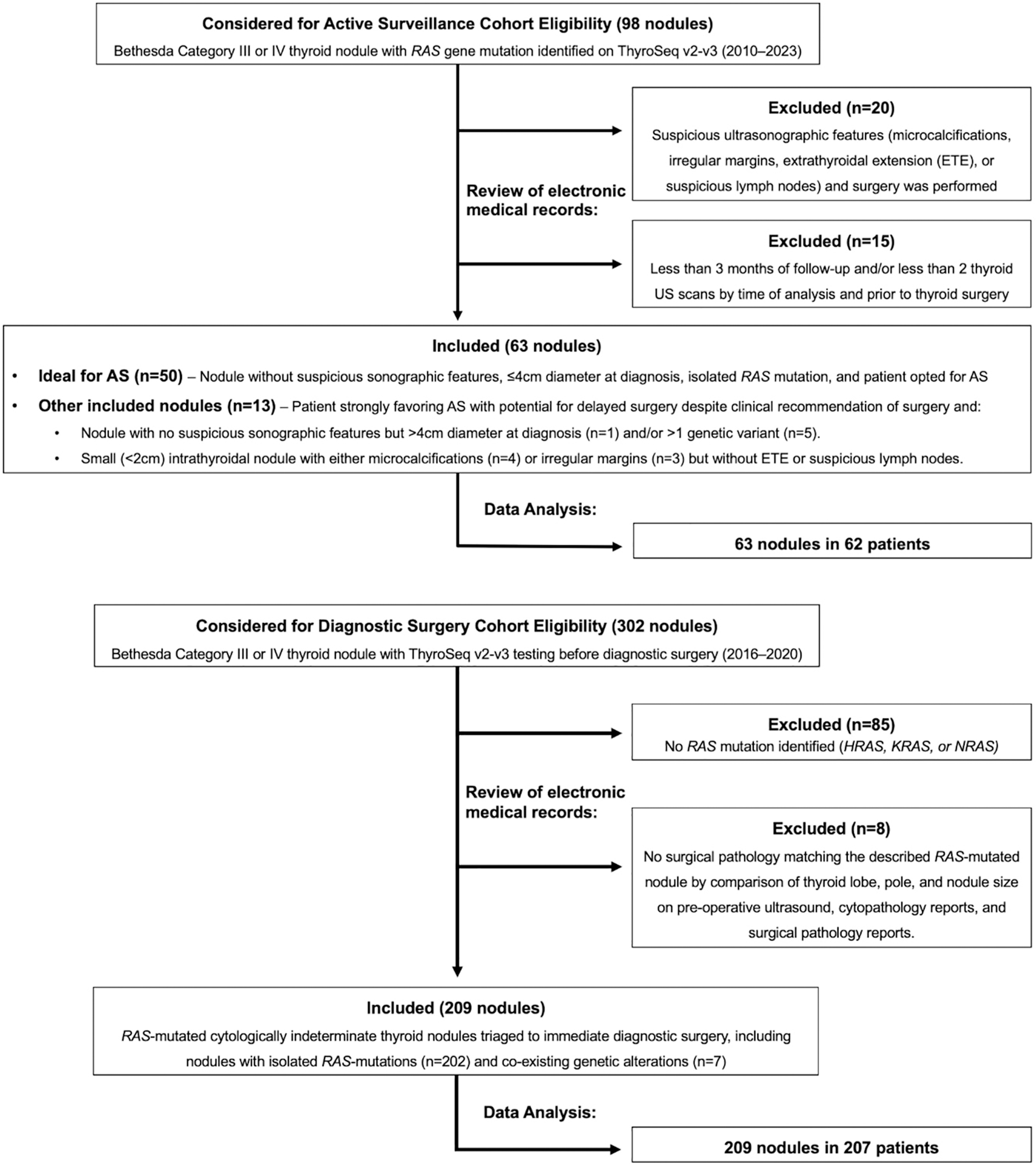
Patient selection process for active surveillance cohort and diagnostic surgery cohort.
All nodules underwent US-guided fine-needle aspiration (FNA) by a radiologist or cytopathologist using a 25- or 27-guage needle. One slide from each FNA was assessed for adequacy with modified Giemsa stain. Remaining slides were alcohol-fixed and stained with hematoxylin–eosin for cytopathologic assessment. ITNs were classified as Bethesda Category III (Atypia of Undetermined Significance) or Bethesda Category IV (Follicular Neoplasm) by fellowship-trained cytopathologists with >10 years of experience. 16 HRAS, NRAS, or KRAS gene mutations were identified with DNA-based sequencing assays (ThyroSeq v2-v3; CBL Path, Rye Brook, NY). Patients had two or more thyroid US scans measuring the targeted nodule and ≥3 months of follow-up between their first and most recent thyroid imaging. The minimum follow-up time of 3 months was chosen to ensure that any patients experiencing early nodule growth that led to surgery were captured.
Under AS, US assessments of the thyroid gland and cervical lymph nodes were performed every 6 months for 2 years and then annually. Nodule volume was calculated using the ellipsoid formula. To ensure that the same thyroid nodule was followed, the initial cytology report, molecular testing report, and subsequent US reports were reviewed to match nodule location within the lobe, size, and sonographic characteristics. For patients who ultimately had surgery (6 of 63), postoperative pathology reports were reviewed and correlated with preoperative US and FNA cytology reports to ensure correct matching to the index nodule.
As in previous literature, nodule growth was defined as an increase in tumor volume >72% from baseline. 17,18 Tumor volume doubling time was calculated for nodules exhibiting growth (not defined for stable nodules). Cumulative incidence of tumor volume growth was calculated using the Kaplan–Meier method and reported with confidence intervals (CIs).
We also retrospectively analyzed surgical pathology reports from 209 RAS-mutant ITNs undergoing immediate surgery (2016–2020) at MSKCC (n = 114) and NYU (n = 95; Fig. 1). ITNs were classified as Bethesda Category III or IV. All specimens were reviewed by surgical pathologists with >10 years of experience. Incidental carcinomas separated from the RAS-mutant nodules were considered separately.
The association between additional molecular alterations and malignancy was tested using the Fisher exact test. For all hypothesis testing, significance was set at α < 0.05.
Results
Growth kinetics of RAS-mutant thyroid nodules
Cohort characteristics are shown in Table 1 (n = 63). Most patients were female (n = 46, 73.0%), with median age at diagnosis of 46 (interquartile range [IQR] 40–67) years. NRAS was the most common RAS mutation (50.8%), followed by KRAS (22.2%), HRAS (22.2%), and RAS of unspecified subtype (4.8%). While 58 (92.1%) nodules had isolated RAS mutations, 5 (7.9%) also harbored another co-occurring variant (Table 1).
Cohort Characteristics of 63 Nodules in 62 Patients with RAS-Mutated Thyroid Nodules Followed with Active Surveillance
Previously known as nodular hyperplasia.
IQR, interquartile range; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features.
At diagnosis, nodules had a median diameter of 1.7 (IQR 1.2–2.6) cm and a median volume of 1.3 (IQR 0.4–4.7) cm3. The average time between US was 311 (IQR 151.8–350) days. During median AS period of 23 (IQR 9.5–53.5) months, in which 46% of nodules (n = 30) were followed for ≥2 years and 20% (n = 13) for ≥5 years, growth was observed in 12 of 63 nodules (19.0%), with cumulative incidences by the Kaplan–Meier method of 1.9% at 1 year [CI: 0.3–13], 15% at 2 years [CI: 7.3–33%], 23.0% at 3 years [CI: 12–44%], 28.0% at 4 years [CI: 16–51%], and 28.0% at 5 years [CI: 16–51%] (Fig. 2).
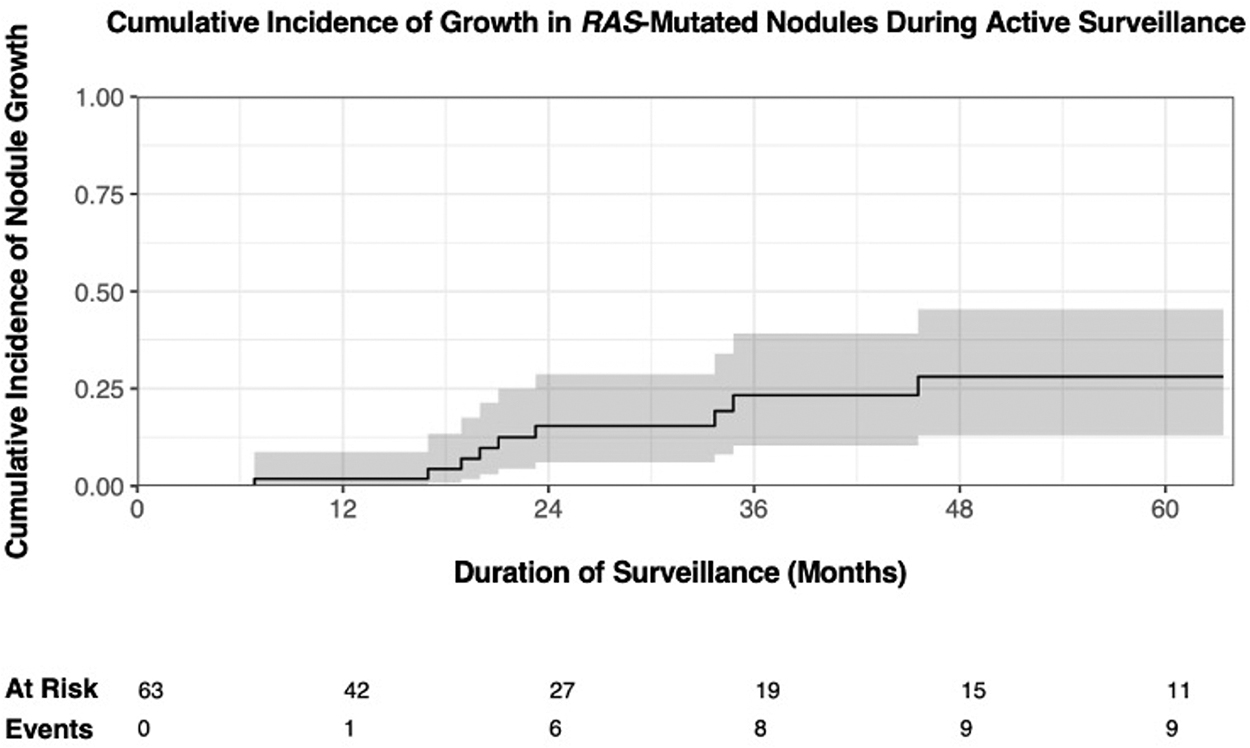
Cumulative incidence of nodule growth. In this figure, nodule growth was defined as >72% change in volume from baseline measurement.
Cumulative incidence of nodule growth was also calculated using an alternative threshold of >50% change in volume. 7,19 –21 Using this definition, growth was observed in 18 of 63 nodules (28.6%), with a cumulative incidence of 9.7% at 1 year [CI: 4.2–22%], 29% at 2 years [CI: 18–47%], 36% at 3 years [CI: 23–55%], 41% at 4 years [CI: 27–62%], and 47% at 5 years [CI: 31–70%].
Of the nodules that grew during AS, the median tumor doubling time was 39.0 (IQR 19.2–58.7) months (range, 6.7–174.6 months). However, most nodules (51; 81.0%) did not grow during observation. The greatest percent change observed for each nodule is shown in Figure 3, and the growth kinetics of individual nodules over time is shown in Figure 4, showing a range of growth kinetics including two nodules that immediately regressed and two that regressed after initial growth.
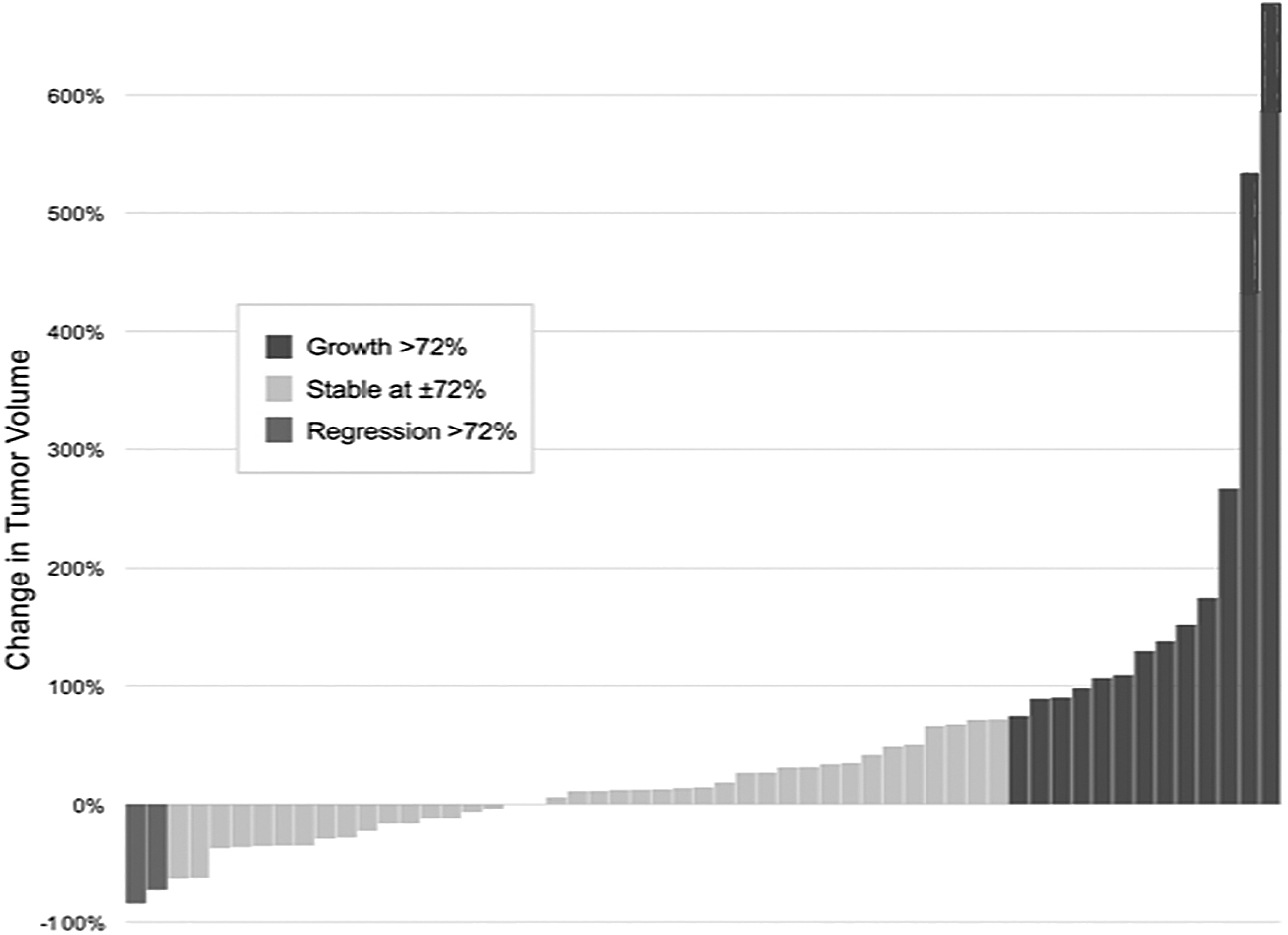
Percent change in tumor volume during active surveillance for each patient.

Percent change in volume of individual RAS-mutated nodules from baseline as determined by thyroid ultrasound scans (n = 63). Tumor growth was defined as >72% change in volume at any point during active surveillance (orange lines: n = 12) and included nodules that subsequently regressed (n = 2).
Clinical outcomes for observed RAS-mutant nodules
Of the 63 RAS-mutant ITNs followed with AS, 6 were ultimately resected after a median surveillance period of 6.5 (IQR 4.3–16.3) months. For one nodule, growth was the indication for surgery. Final pathology revealed a noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP). An additional five nodules were resected despite stable size for reasons including patient or physician preference (n = 4) or development of nodule microcalcifications (n = 1). The nodule that developed microcalcifications was the only resected nodule in this cohort with malignant pathology (encapsulated FVPTC), for an overall 16.7% incidence of malignancy. In five of six cases, surgery consisted of a lobectomy. There were no surgical complications, including no cases of vocal cord paresis or paralysis, hypoparathyroidism, hematoma, or infection.
In the one case of malignancy, the nodule was initially diagnosed with Bethesda III cytology, with coexisting RAS and TERT promoter mutations. Because of the coexisting mutations, the patient was initially advised to undergo surgery, but declined. On serial US imaging, the nodule remained stable at 3.7 cm in maximal diameter (11.9 cm3 volume), for 9.3 years (112 months). After increased microcalcifications were noted, surgery was recommended, and total thyroidectomy revealed a 3.7 × 2.0 × 2.1 cm FVPTC with 0 of 1 involved lymph nodes, focal capsular invasion, angioinvasion (>4 foci), but no extrathyroidal extension, tumor necrosis, or lymphatic invasion. There were no surgical complications. The patient was treated with 100 mCi of radioactive iodine postoperatively and remains without evidence of recurrent disease 3 years later.
Of the four other nodules harboring co-mutations that remain on AS, three remain stable in size, while one nodule (NRAS/EIF1AX mutated) has grown over 40 months but remains <1 cm3.
During AS, no regional or distant metastases were detected, and there have been no disease-specific deaths or deaths from any cause. All patients have been asymptomatic during AS, without associated compressive symptoms, pain, voice changes, or gross lymphadenopathy. At final follow-up, 57 (90.5%) patients are continuing AS.
Nodules continuing AS despite growth
There were three nodules that remain on AS despite growth >200% from baseline volume (Figs. 2 and 3). The Bethesda III nodule displaying 674% growth (doubling time 16.4 months) from a baseline volume of 1.63 cm3 and diameter of 2.0 cm had mixed cystic-solid components on US. At latest follow-up (volume 12.6 cm3; diameter 4.2 cm), surgery was advised. Because most growth has been in the nodule's cystic component in the absence of other suspicious sonographic characteristics, the patient elected to continue AS with plans for surgery in the event of continued growth.
The Bethesda III nodule displaying 533% growth (doubling time 24.5 months) had a baseline volume of 0.45 cm3 and diameter of 1.2 cm. At latest follow-up after 144 months (volume 2.7 cm3; diameter 1.9 cm), this patient elected to continue AS due to small nodule size and slow growth rate, with plans for surgery in the event of continued growth.
The Bethesda III nodule displaying 267% growth (doubling time 32.7 months) has a small nodule (baseline volume 0.1 cm3; diameter 0.7 cm) and after 78 months (volume 3.8 cm3; 1.0 cm diameter) has elected to continue AS, due to small size and slow growth.
Surgical pathology of operated RAS-mutant nodules
Of the 209 RAS-mutant ITNs undergoing immediate surgery (Table 2 and Fig. 5), the majority (67.0%, n = 140) were nonmalignant, of which 35.4% (n = 74) were NIFTP. Of the cancers (n = 69), 72.5% (n = 50) were ATA low-risk cancers; 21.7% (n = 15), ATA intermediate-risk cancers; 5.8% (n = 4), ATA high-risk cancers. Thus, of the complete cohort of 209 patients, 1.9% were ATA high-risk cancers.
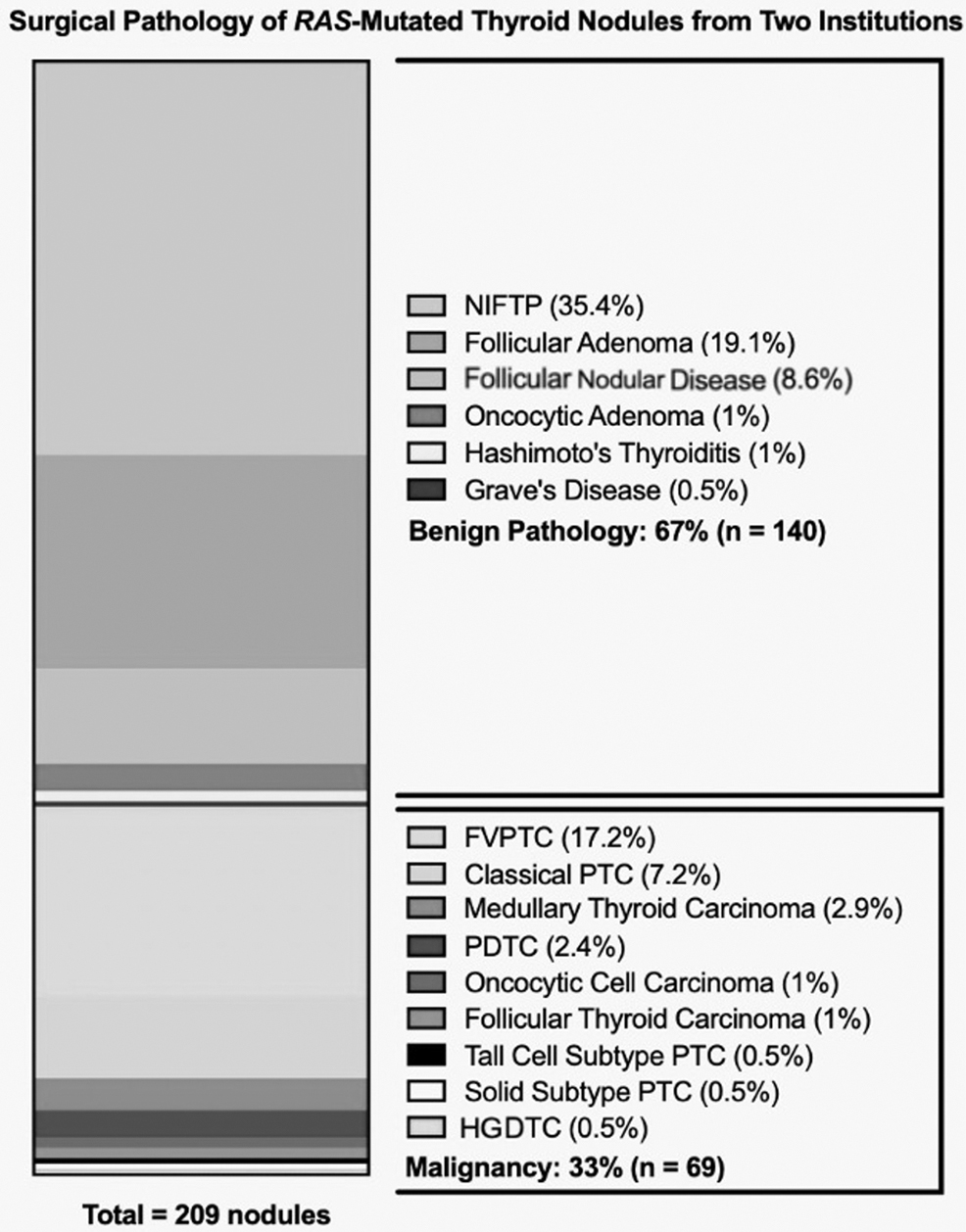
Surgical pathology of RAS-mutant thyroid nodules triaged to surgery. Benign or nonmalignant entities made up the majority (67.0%, n = 140) of the resected RAS-mutant indeterminate thyroid nodules, while cancer was found in 33.0% (n = 69). Of the carcinomas, 78% were ATA low-risk cancers. Follicular nodular disease, previously known as nodular hyperplasia; Oncocytic adenoma, previously known as Hürthle cell adenoma; Hashimoto's thyroiditis, described as chronic lymphocytic thyroiditis; Oncocytic cell carcinoma, previously known as Hürthle cell carcinoma. ATA, American Thyroid Association; FVPTC, follicular variant of papillary thyroid cancer; HGDTC, high-grade differentiated thyroid carcinoma; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; PDTC, poorly differentiated thyroid cancer; PTC, papillary thyroid carcinoma.
Cohort Characteristics of 209 RAS-Mutant Cytologically Indeterminate Thyroid Nodules in 207 Patients Managed with Diagnostic Surgery
Follicular nodular disease, previously known as nodular hyperplasia; Oncocytic adenoma, previously known as Hürthle cell adenoma; Oncocytic cell carcinoma, previously known as Hürthle cell carcinoma; Hashimoto's thyroiditis, described as chronic lymphocytic thyroiditis; PTC, papillary thyroid carcinoma; SD, standard deviation.
The most common malignant pathological diagnoses were FVPTC (17.2%, n = 36)—nearly all of which (n = 32, 94%) were low-risk tumors: intrathyroidal, <4 cm in size, without nodal or distant metastases. 7 Fifteen tumors (7.2%) were classical PTCs, followed by small numbers of medullary (n = 6), poorly differentiated (n = 5), oncocytic (n = 2), follicular (n = 2), tall cell subtype (n = 1), solid subtype (n = 1), and differentiated high-grade thyroid carcinoma (n = 1). FTC was uncommon in this cohort, consistent with prior reports indicating FTC prevalence among RAS-mutated ITNs between 0% and 10%. 5,22,23 Among patients with complete follow-up data available (n = 114), there have been no recurrences or disease-specific deaths during the median follow-up of 6.9 (IQR 4.4–7.1) years.
Most (94%) nodules in the surgical cohort harbored isolated RAS mutations. The presence of coexisting genetic alterations was associated with a numerically, but not statistically significantly, increased risk of malignancy compared with isolated RAS mutation: RAS+any co-mutation (odds ratio [OR] = 3.57; p = 0.12); RAS+TERT promoter (OR = 2.14; p = 0.54); RAS+EIF1AX (OR = 4.28; p = 0.09).
Discussion
Most ITNs harboring RAS mutations are benign; of those that are malignant, most are low-risk cancers. The ideal management for these nodules remains poorly understood, due to a lack of evidence describing the behavior of these nodules when not surgically resected. To address this knowledge gap, we present data on the growth kinetics of 63 RAS-mutant ITNs followed with AS, and surgical pathology data from 209 resected RAS-mutant ITNs.
When a RAS gene mutation is identified in an ITN, many physicians tend to recommend a thyroidectomy, reasoning that activating RAS mutations are indicative of either malignancy or a high risk of malignant transformation. 2 However, several recent studies have shown that these risks are, in fact, very low. In one prospective study, fewer than half of RAS-mutant ITNs were malignant; of the cancers, all were histopathologically low risk: encapsulated or partially encapsulated/well-circumscribed FVPTCs without lymphovascular invasion, extrathyroidal extension, lymph node metastases, or distant metastases—none of which resulted in disease-specific deaths. 24 Similarly, in our previous multi-institutional study of Bethesda III/IV ITNs, the rate of malignancy among 84 RAS-mutant nodules was low, ranging from 10% to 37% across four institutions. 22 In fact, RAS mutations are associated with a decreased risk of distant metastases compared with other alterations, leading isolated RAS mutations to be classified into a low-risk molecular risk group. 25
Because AS is now an accepted treatment option for clinically low-risk PTCs, and because most RAS-mutant nodules ultimately prove to be nonmalignant lesions or low-risk carcinomas with a lower risk of distant metastases, we have offered patients the approach of AS as an alternative to immediate surgery. 19 This approach is consistent with clinical practice guidelines of the NCCN, ATA, and AACE. 6 –8
We found that most (81%) RAS-mutant ITNs under AS have not demonstrated evidence of growth, during a median of 23 months of surveillance. The cumulative incidence of growth at 5 years was 28%. It is important to acknowledge that thyroid nodule growth is not a strong indicator of malignancy and that more accurate predictive features are needed. 26 –28 Ultimately, only one of six nodules in our cohort were resected due to growth, and only one resected nodule was malignant—a low-risk FVPTC, which was resected for the development of microcalcifications, not growth. Among the 209 RAS-mutant nodules that were immediately surgically resected, 33% of nodules were malignant. The vast majority (72.5%) of these were ATA low-risk cancers, similar to prior reports. 22 Therefore, more than 90% of RAS-mutant nodules were either benign or clinically low-risk carcinomas, and very few are high-risk carcinomas.
In this study, 35% of lesions were NIFTP—a non-malignant entity introduced in 2016. 29 –31 Cases diagnosed before 2016 were re-reviewed and recategorized with current nomenclature where applicable (Supplementary Table S1). The prevalence of NIFTP in RAS-mutated ITNs in this study is similar to prior reports. 32
There are several caveats to these findings. We caution that these results are not definitive, as this is the first report of the behavior of cytologically indeterminate RAS-mutant nodules under AS, to the best of our knowledge. Additional findings from other centers will enhance the generalizability of these results and allow for more precise assessment of the incidence of growth and/or metastasis over time.
We currently do not recommend AS for RAS-mutant ITNs when other genetic alterations are present. We found that coexisting alterations were associated with a numerically increased prevalence of malignancy in RAS-mutated ITNs, but this difference did not reach statistical significance, possibly owing to the limited number of nodules with each of these genetic profiles. Further data will help to delineate these risks.
It is unknown whether it is possible, over long periods of AS, for RAS-mutated thyroid nodules to develop additional mutations that may be associated with more aggressive behavior. For example, nodules that develop additional mutations—such as TP53—may be more prone to develop into aggressive tumors, which would not be suitable for AS. Further research will help to determine whether the development of additional mutations can be observed during AS. 29,33 Finally, we acknowledge that tumor growth or change in volume is only one marker of tumor behavior and that further follow-up will help to estimate if there is a measurable incidence of regional or distant metastases during AS, which we have not observed.
Conclusions
We have offered AS to patients with RAS-mutant ITNs (ideally, those with isolated mutations and without suspicious ultrasonographic features) based on prior data indicating that these nodules very rarely harbor high-risk cancers and that risks of distant metastases are lower than for other genetic variants in ITNs. In this study, our goal in assessing rates of tumor growth was to determine whether surgery can be safely delayed without the development of local invasion or a need for more extensive thyroidectomy. We report a low incidence of tumor growth under AS and conclude that surgical intervention, if ultimately necessary, can likely be safely delayed. We and others have also observed that the vast majority of resected RAS-mutated ITNs are benign or low-risk carcinomas.
Further prospective studies will improve our understanding of these tumors. 33 In light of the uncertainty surrounding the long-term behavior of RAS-mutant thyroid nodules, their very low risk of representing aggressive carcinomas, and these preliminary data suggesting most such nodules remain stable in size under observation, we conclude that the optimal management of RAS-mutant ITNs is not well defined. However, a universal practice of immediate surgery for all cases seems to be of low value. We therefore advise that physicians engage in honest conversation with patients about this uncertainty and decide on treatment using shared decision-making.
Footnotes
Acknowledgments
The authors thank members of the Memorial Sloan Kettering Cancer Center multidisciplinary thyroid cancer disease management team, and the Head and Neck Service, for helpful discussions.
Authors' Contributions
H.J.S.: Conceptualization (lead), methodology (supporting), data collection and analysis (lead), writing—original draft (lead), writing—review and editing (lead). E.S.K.: Data collection and analysis (lead), writing—original draft (supporting), writing—review and editing (supporting). K.Z.: Data collection and analysis (lead), writing—original draft (supporting), writing—review and editing (supporting). C.E.S.: Data collection and analysis (lead), writing—review and editing (equal). B.R.U.: Data collection (supporting), writing—review and editing (equal). J.L.M.: Data collection (supporting), writing—review and editing (equal). B.R.R.: Data collection (supporting), writing—review and editing (equal). J.D.: Data collection (supporting), writing—review and editing (equal).
R.S.W.: Data collection (supporting), writing—review and editing (equal). R.X.: Histopathology review (lead), writing—review and editing (equal). J.-M.C.: Histopathology review (lead), writing—review and editing (equal). B.X.: Histopathology review (lead), writing—review and editing (equal). R.G.: Histopathology review (lead), writing—review and editing (equal). B.G.: Data collection (supporting), writing—review and editing (equal). J.O.B.: Data collection (supporting), writing—review and editing (equal). R.M.T.: Methodology (equal), writing—review and editing (equal). J.A.F.: Writing—review and editing (equal). R.J.W.: Data collection (supporting), writing—review and editing (equal). L.G.T.M.: Conceptualization (lead), methodology (equal), data collection and analysis (supporting), writing—review and editing (lead).
Author Disclosure Statement
LGTM is listed as an inventor on intellectual property owned by Memorial Sloan Kettering Cancer Center and licensed to PGDx, unrelated to this study. All other authors declare no competing financial interests.
Funding Information
This project was supported by the following funds awarded to L.G.T.M.: National Institutes of Health (R01 DE027738); the U.S. Department of Defense (CA210784); the Geoffrey Beene Cancer Research Center; the Memorial Sloan Kettering Population Science Research Program; the Jayme and Peter Flowers Fund; the Sebastian Nativo Fund (to L.G.T.M.); and P30 CA008748 to Memorial Sloan Kettering Cancer Center.
Supplementary Material
Supplementary Table S1